
The Mediating Role of School and Sibling Bullying in the Relationship between Subjective Well-Being and Mental Health Symptoms


Abstract
:1. Introduction
1.1. Well-Being and Mental Health
1.2. The Relationships of Sibling and School Bullying with MH and Well-being
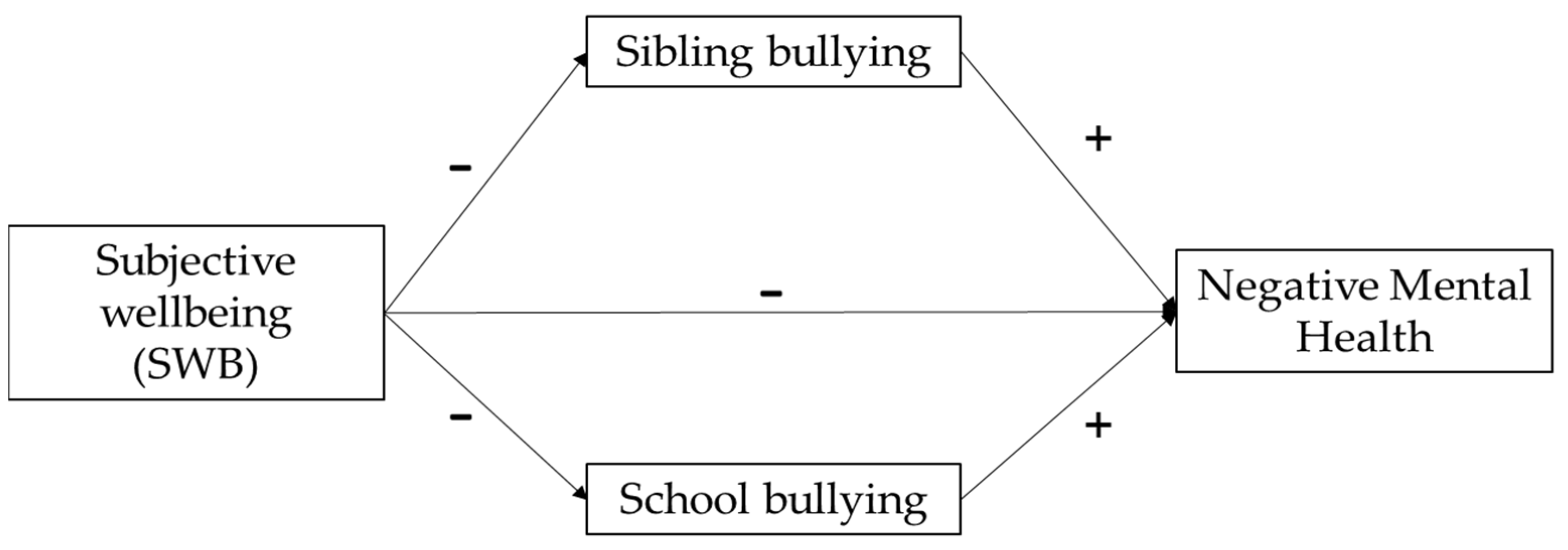
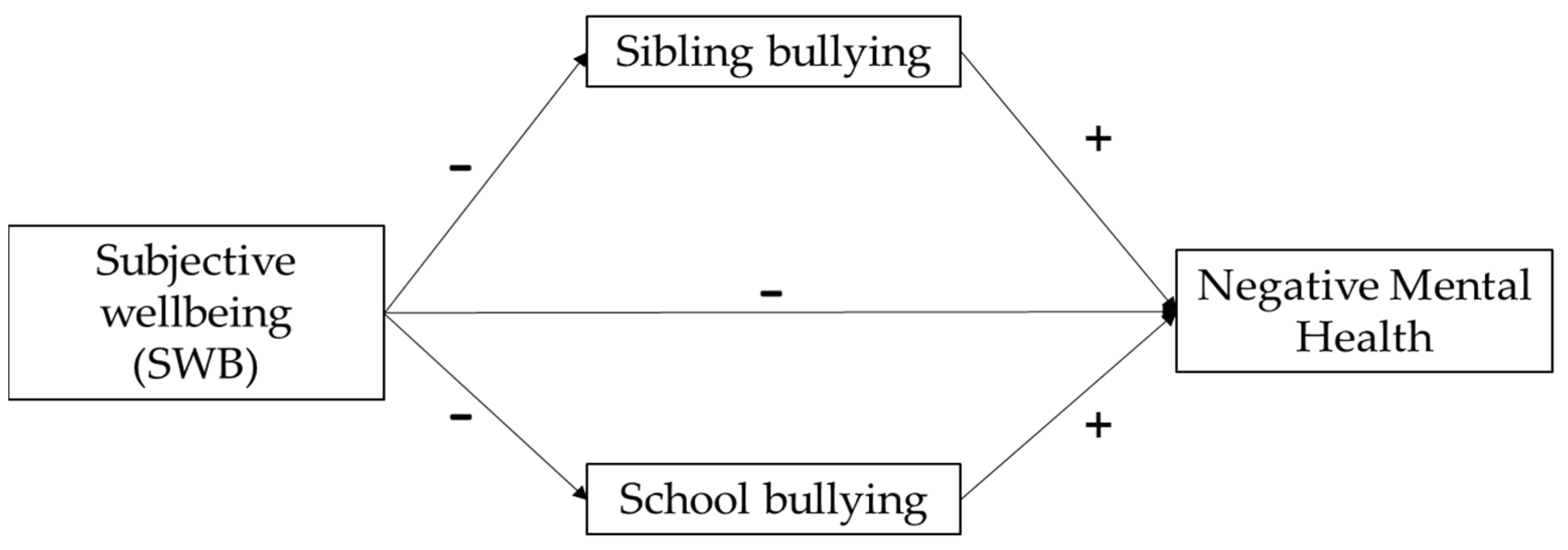
1.3. The Present Study
2. Materials and Methods
2.1. Dataset and Sample
2.2. Measures
2.2.1. Subjective Well-being
2.2.2. Mental Health Symptoms
2.2.3. School Bullying
2.2.4. Sibling Bullying
2.3. Data Analysis
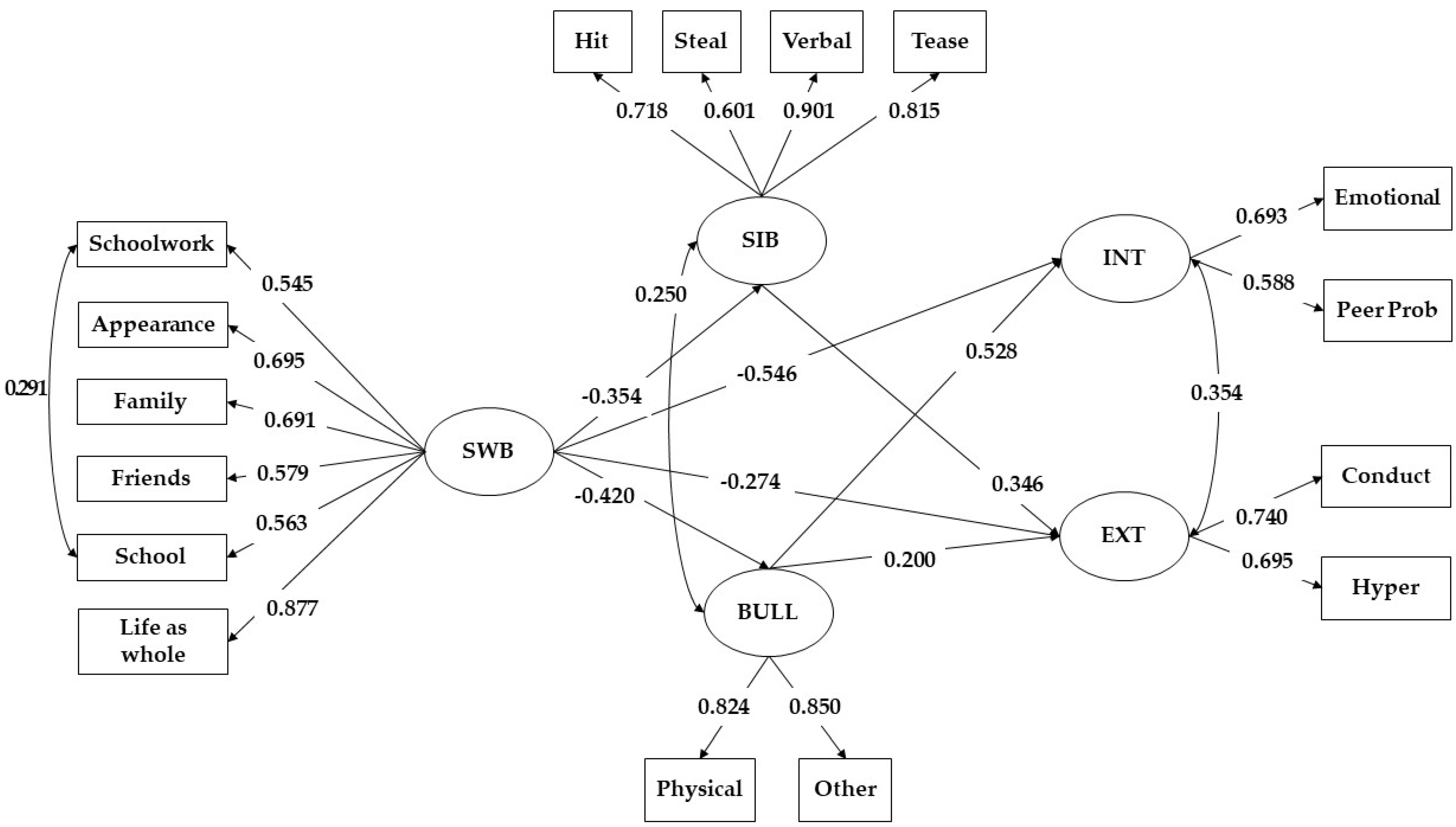
3. Results
4. Discussion
4.1. Implications for Policy and Practice
4.2. Limitations and Future Directions for Research
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Mental Health: Strengthening Our Response. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response (accessed on 23 April 2022).
- Keyes, C.L.M. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Cons. Clin. Psych. 2005, 73, 539–548. [Google Scholar] [CrossRef] [Green Version]
- Rose, T.; Joe, S.; Williams, A.; Harris, R.; Betz, G.; Stewart-Brown, S. Measuring Mental Wellbeing Among Adolescents: A Systematic Review of Instruments. J. Child Fam. Stud. 2017, 26, 2349–2362. [Google Scholar] [CrossRef]
- Vega, W.A.; Rumbaut, R.G. Ethnic Minorities and Mental Health. Ann. Rev. Soc. 1991, 17, 351–383. [Google Scholar] [CrossRef]
- Toseeb, U.; Wolke, D. Sibling bullying: A prospective longitudinal study of associations with positive and negative mental health during adolescence. J. Youth Adolesc. 2021, 51, 940–955. [Google Scholar] [CrossRef]
- Arslan, G. School Bullying and Youth Internalizing and Externalizing Behaviors: Do School Belonging and School Achievement Matter? Int. J. Ment. Health Add. 2021, 1–18. [Google Scholar] [CrossRef]
- Eastman, M.; Foshee, V.; Ennett, S.; Sotres-Alvarez, D.; Reyes, H.L.M.; Faris, R.; North, K. Profiles of internalizing and externalizing symptoms associated with bullying victimization. J. Adolesc. 2018, 65, 101–110. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. On Happiness and Human Potentials: A Review of Research on Hedonic and Eudaimonic Well-Being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef]
- McLellan, R.; Steward, S. Measuring children and young people’s wellbeing in the school context. Camb. J. Educ. 2015, 45, 307–332. [Google Scholar] [CrossRef] [Green Version]
- Keyes, C.L.M.; Shmotkin, D.; Ryff, C.D. Optimizing Well-Being: The Empirical Encounter of Two Traditions. J. Personal. Soc. Psychol. 2002, 82, 1007–1022. [Google Scholar]
- Huta, V.; Waterman, A.S. Eudaimonia and Its Distinction from Hedonia: Developing a Classification and Terminology for Understanding Conceptual and Operational Definitions. J. Happiness Stud. 2014, 15, 1425–1456. [Google Scholar] [CrossRef]
- Ryff, C.D. Happiness Is Everything, or Is It? Explorations on the Meaning of Psychological Well-Being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Waterman, A.S. Two conceptions of happiness: Contrasts of personal expressiveness (eudaimonia) and hedonic enjoyment. J. Personal. Soc. Psychol. 1993, 64, 678–691. [Google Scholar] [CrossRef]
- Stewart-Brown, S. Population Level: Wellbeing in the General Population. In Wellbeing, Recovery and Mental Health; Slade, M., Oades, L., Jarden, A., Eds.; Cambridge University Press: New York, NY, USA, 2017; pp. 215–230. ISBN 978-1-316-33927-5. [Google Scholar]
- Goodman, A.; Goodman, R. Strengths and Difficulties Questionnaire as a Dimensional Measure of Child Mental Health. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 400–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patalay, P.; Fitzsimons, E. Correlates of Mental Illness and Wellbeing in Children: Are They the Same? Results From the UK Millennium Cohort Study. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 771–783. [Google Scholar] [CrossRef] [Green Version]
- Patalay, P.; Fitzsimons, E. Development and Predictors of Mental Ill-Health and Wellbeing from Childhood to Adolescence. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 1311–1323. [Google Scholar] [CrossRef]
- Merikangas, K.R.; Nakamura, E.F.; Kessler, R.C. Epidemiology of Mental Disorders in Children and Adolescents. Dialogues Clin. Neurosci. 2009, 11, 7–20. [Google Scholar] [CrossRef]
- Collishaw, S. Annual Research Review: Secular Trends in Child and Adolescent Mental Health. J. Child Psychol. Psychiatry 2015, 56, 370–393. [Google Scholar] [CrossRef]
- Kessler, R.C.; Zhao, S. Overview of Descriptive Epidemiology of Mental Disorders. In Handbook of the Sociology of Mental Health; Handbooks of Sociology and Social Research; Aneshensel, C.S., Phelan, J.C., Eds.; Springer: Boston, MA, USA, 1999; pp. 127–150. ISBN 978-0-387-32516-3. [Google Scholar]
- Dawson, D.L.; Golijani-Moghaddam, N. COVID-19: Psychological Flexibility, Coping, Mental Health, and Wellbeing in the UK during the Pandemic. J. Context. Behav. Sci. 2020, 17, 126–134. [Google Scholar] [CrossRef]
- Brown, B.B.; Larson, J. Peer Relationships in Adolescence. In Handbook of Adolescent Psychology: Contextual Influences on Adolescent Development, 3rd ed.; Lerner, R., Steinberg, L., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2009; Volume 2, pp. 74–103. ISBN 978-0-470-14922-5. [Google Scholar]
- Salmela-Aro, K. Stages of Adolescence. In Encyclopedia of Adolescence; Brown, B.B., Prinstein, M.J., Eds.; Academic Press: San Diego, CA, USA, 2011; pp. 360–368. ISBN 978-0-12-373951-3. [Google Scholar]
- Proctor, C.L.; Linley, P.A.; Maltby, J. Youth Life Satisfaction: A Review of the Literature. J Happiness Stud 2009, 10, 583–630. [Google Scholar] [CrossRef] [Green Version]
- Katsantonis, I. Cultural Variation in Aggressive Behavior: A Cross-Cultural Comparison of Students’ Exposure to Bullying Across 32 Countries. Electron. J. Res. Educ. Psychol. 2021, 19, 465–490. [Google Scholar] [CrossRef]
- Katsantonis, I.; Asimakopoulou, E.; Frounta, M. The role of the supportive environment in the development of school bullying: An ecosystemic approach. Hell. J. Res.Educ. 2021, 10, 52–64. [Google Scholar] [CrossRef]
- Olweus, D.; Breivik, K. Plight of Victims of School Bullying: The Opposite of Well-Being. In Handbook of Child Well-Being; Ben-Arieh, A., Casas, F., Frønes, I., Korbin, J.E., Eds.; Springer: Dordrecht, The Netherlands, 2014; pp. 2593–2616. [Google Scholar] [CrossRef]
- Olweus, D.; Limber, S.P. Bullying in School: Evaluation and Dissemination of the Olweus Bullying Prevention Program. Am. J. Orthopsychiatry 2010, 80, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Skinner, J.A.; Kowalski, R.M. Profiles of Sibling Bullying. J. Interpers. Violence 2013, 28, 1726–1736. [Google Scholar] [CrossRef] [PubMed]
- Wolke, D.; Tippett, N.; Dantchev, S. Bullying in the Family: Sibling Bullying. Lancet Psychiatry 2015, 2, 917–929. [Google Scholar] [CrossRef] [Green Version]
- Rivers, I.; Smith, P.K. Types of bullying behaviour and their correlates. Aggress. Voilotent Behav. 1994, 20, 359–368. [Google Scholar] [CrossRef]
- OECD. PISA 2018 Results (Volume III): What School Life Means for Students’ Lives; OECD: Paris, France, 2019. [Google Scholar]
- Bowes, L.; Wolke, D.; Joinson, C.; Lereya, S.T.; Lewis, G. Sibling Bullying and Risk of Depression, Anxiety, and Self-Harm: A Prospective Cohort Study. Pediatrics 2014, 134, e1032–e1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dantchev, S.; Hickman, M.; Heron, J.; Zammit, S.; Wolke, D. The Independent and Cumulative Effects of Sibling and Peer Bullying in Childhood on Depression, Anxiety, Suicidal Ideation, and Self-Harm in Adulthood. Front. Psychiatry 2019, 10, 651. [Google Scholar] [CrossRef] [Green Version]
- Borualogo, I.S.; Casas, F. The Relationship between Frequent Bullying and Subjective Well-Being in Indonesian Children. Pop Rev 2021, 60, 26–50. [Google Scholar] [CrossRef]
- Bradshaw, J.; Crous, G.; Rees, G.; Turner, N. Comparing Children’s Experiences of Schools-Based Bullying across Countries. Child. Youth Serv. Rev. 2017, 80, 171–180. [Google Scholar] [CrossRef] [Green Version]
- Frison, E.; Subrahmanyam, K.; Eggermont, S. The Short-Term Longitudinal and Reciprocal Relations Between Peer Victimization on Facebook and Adolescents’ Well-Being. J. Youth Adolesc. 2016, 45, 1755–1771. [Google Scholar] [CrossRef]
- Martin, K.; Huebner, E.S.; Valois, R.F. Does Life Satisfaction Predict Victimization Experiences in Adolescence? Psychol. Sch. 2008, 45, 705–714. [Google Scholar] [CrossRef]
- Hanniball, K.B.; Viljoen, J.L.; Shaffer, C.S.; Bhatt, G.; Tweed, R.; Aknin, L.B.; Gagnon, N.; Douglas, K.S.; Dooley, S. The Role of Life Satisfaction in Predicting Youth Violence and Offending: A Prospective Examination. J. Interpers. Violence 2021, 36, 5501–5529. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, H.; Fink, E.; Duffy, F.; Patalay, P. Changes in Peer and Sibling Victimization in Early Adolescence: Longitudinal Associations with Multiple Indices of Mental Health in a Prospective Birth Cohort Study. Eur. Child Adolesc. Psychiatry 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- University of Essex, Institute for Social and Economic Research. Understanding Society: Waves 1–11, 2009–2020 and Harmonised BHPS: Waves 1-18, 1991-2009, 15th ed.; UK Data Service; University of Essex: Colchester, UK, 2022. [Google Scholar]
- Institute for Social and Economic Research. Understanding Society: Waves 1-11, 2009-2020 and Harmonised BHPS: Waves 1–18, 1991–2009, User Guide, 30 October 2021; University of Essex: Colchester, UK, 2021; SN: 6614. [Google Scholar]
- Bollen, K. Structural Equations with Latent Variables; Wiley: New York, NY, USA, 1989. [Google Scholar]
- Li, C.-H. The Performance of ML, DWLS, and ULS Estimation with Robust Corrections in Structural Equation Models with Ordinal Variables. Psychol. Methods 2016, 21, 369–387. [Google Scholar] [CrossRef] [PubMed]
- Rhemtulla, M.; Brosseau-Liard, P.É.; Savalei, V. When Can Categorical Variables Be Treated as Continuous? A Comparison of Robust Continuous and Categorical SEM Estimation Methods under Suboptimal Conditions. Psychol. Methods 2012, 17, 354–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Anderson, J.C.; Gerbing, D.W. Structural Equation Modeling in Practice: A Review and Recommended Two-Step Approach. Psychol. Bull. 1989, 103, 411–423. [Google Scholar] [CrossRef]
- Understanding Society Ethics. Available online: https://www.understandingsociety.ac.uk/documentation/mainstage/user-guides/main-survey-user-guide/ethics (accessed on 20 March 2022).
- UK Data Archive. Available online: https://www.data-archive.ac.uk/find/ (accessed on 23 April 2022).

{kind=link}
{kind=link}
| Items | Males | Females | Min | Max |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| Internalising- emotional symptoms | 2.732 (2.285) | 3.876 (2.433) | 0 | 10 |
| Internalising- peer problems | 1.961 (1.813) | 1.893 (1.614) | 0 | 10 |
| Externalising- conduct problems | 2.181 (1.783) | 1.942 (1.657) | 0 | 9 |
| Externalising- hyperactivity/inattention | 4.227 (2.492) | 4.063 (2.318) | 0 | 10 |
| Sibling bullying- being hit, kicked or pushed | 2.162 (1.043) | 2.040 (0.967) | 1 | 4 |
| Sibling bullying- siblings take your belongings | 1.635 (0.848) | 1.765 (0.828) | 1 | 4 |
| Sibling bullying- called nasty names | 2.037 (1.10) | 2.007 (1.00) | 1 | 4 |
| Sibling bullying- made fun of (teasing) | 1.946 (1.051) | 1.942 (0.991) | 1 | 4 |
| School bullying- being physically bullied | 1.231 (0.550) | 1.166 (0.504) | 1 | 4 |
| School bullying- being bullied in other ways (e.g., called names, getting left out of games, etc.) | 1.407 (0.722) | 1.509 (0.806) | 1 | 4 |
| SWB- happiness with schoolwork | 5.264 (1.390) | 5.294 (1.299) | 1 | 7 |
| SWB- happiness with appearance | 5.495 (1.398) | 4.989 (1.555) | 1 | 7 |
| SWB- happiness with family | 6.482 (0.854) | 6.350 (0.998) | 1 | 7 |
| SWB- happiness with friends | 6.228 (1.079) | 6.189 (1.045) | 1 | 7 |
| SWB- happiness with school | 5.515 (1.537) | 5.444 (1.515) | 1 | 7 |
| SWB- happiness with life as whole | 5.855 (1.141) | 5.522 (1.289) | 1 | 7 |
| 1 | 2 | 3 | 4 | |
|---|---|---|---|---|
| 1. Internalising MH Symptoms | 1 | |||
| 2. Externalising MH Symptoms | 0.606 | 1 | ||
| 3. SWB | −0.761 | −0.481 | 1 | |
| 4. School bullying | 0.750 | 0.440 | −0.420 | 1 |
| 5. Sibling bullying | 0.362 | 0.515 | −0.354 | 0.361 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsantonis, I. The Mediating Role of School and Sibling Bullying in the Relationship between Subjective Well-Being and Mental Health Symptoms. Psych 2022, 4, 258-268. https://doi.org/10.3390/psych4020022
Katsantonis I. The Mediating Role of School and Sibling Bullying in the Relationship between Subjective Well-Being and Mental Health Symptoms. Psych. 2022; 4(2):258-268. https://doi.org/10.3390/psych4020022
Chicago/Turabian StyleKatsantonis, Ioannis. 2022. "The Mediating Role of School and Sibling Bullying in the Relationship between Subjective Well-Being and Mental Health Symptoms" Psych 4, no. 2: 258-268. https://doi.org/10.3390/psych4020022
APA StyleKatsantonis, I. (2022). The Mediating Role of School and Sibling Bullying in the Relationship between Subjective Well-Being and Mental Health Symptoms. Psych, 4(2), 258-268. https://doi.org/10.3390/psych4020022