Improved Modeling of Temperature Evolution during Lung Cancer Tumor Thermal Ablation


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
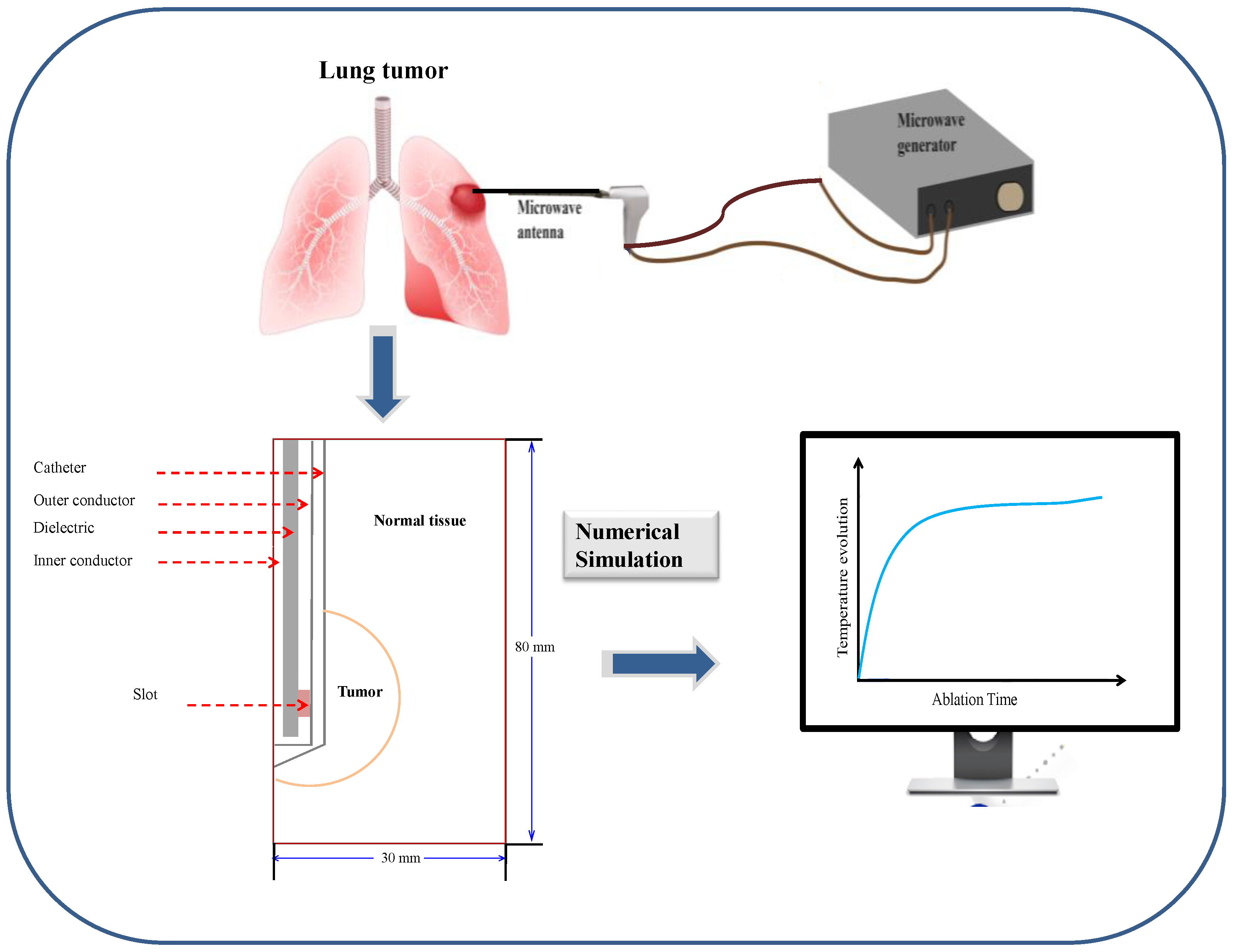
2. Model and Methods
2.1. Model Geometry
2.2. Mathematical Model
2.2.1. Heat Transfer Field
2.2.2. Electromagnetic Field
2.2.3. Thermal Damage Equation
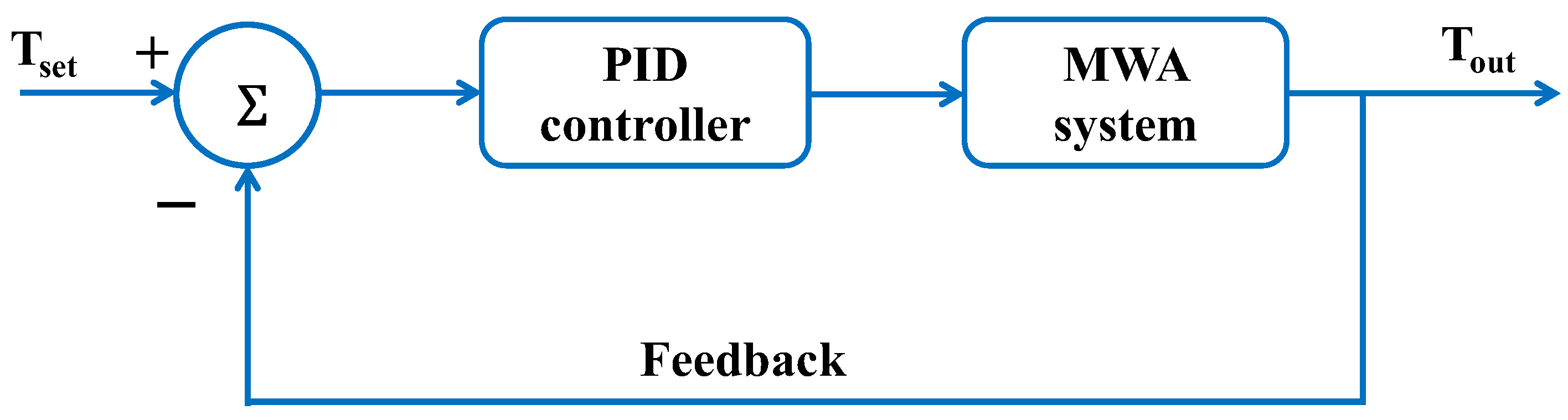
2.2.4. Temperature-Controlled MWA
2.3. Boundary Conditions
2.3.1. Boundary Conditions for Heat Transfer Field Analysis
- i
- The surrounding healthy lung tissue is considered as an insulation condition .
- ii
- An axial symmetry boundary condition at is adopted.
- iii
- The presence of continuous heat flux through the cancer and the lung tissue is assumed, which can be expressed by .
2.3.2. Boundary Conditions for Electromagnetic Field Analysis
- i
- In this model, it is assumed that the z-axis represents a symmetry axis:and .
- ii
- The scattering boundary condition is applied along the outer side of the lung or or .
- iii
- The walls of the antenna with the values or or are computed as perfect metal conductors: .
- iv
- At the tumor–lung interface, the continuity behavior of the tangential component of the electric field is imposed by .
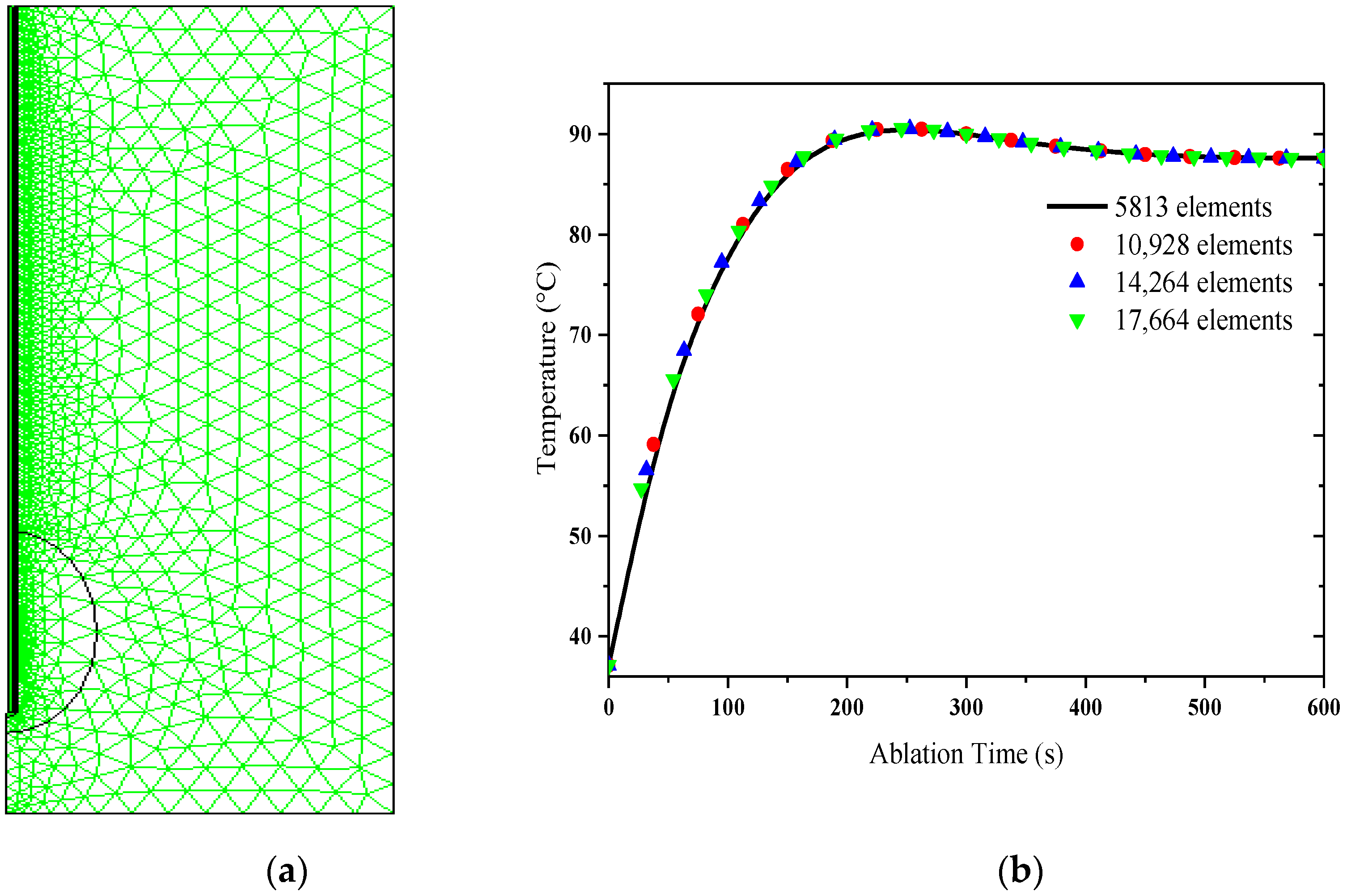
2.4. Numerical Method and Verification of Simulation Model
3. Results and Discussion
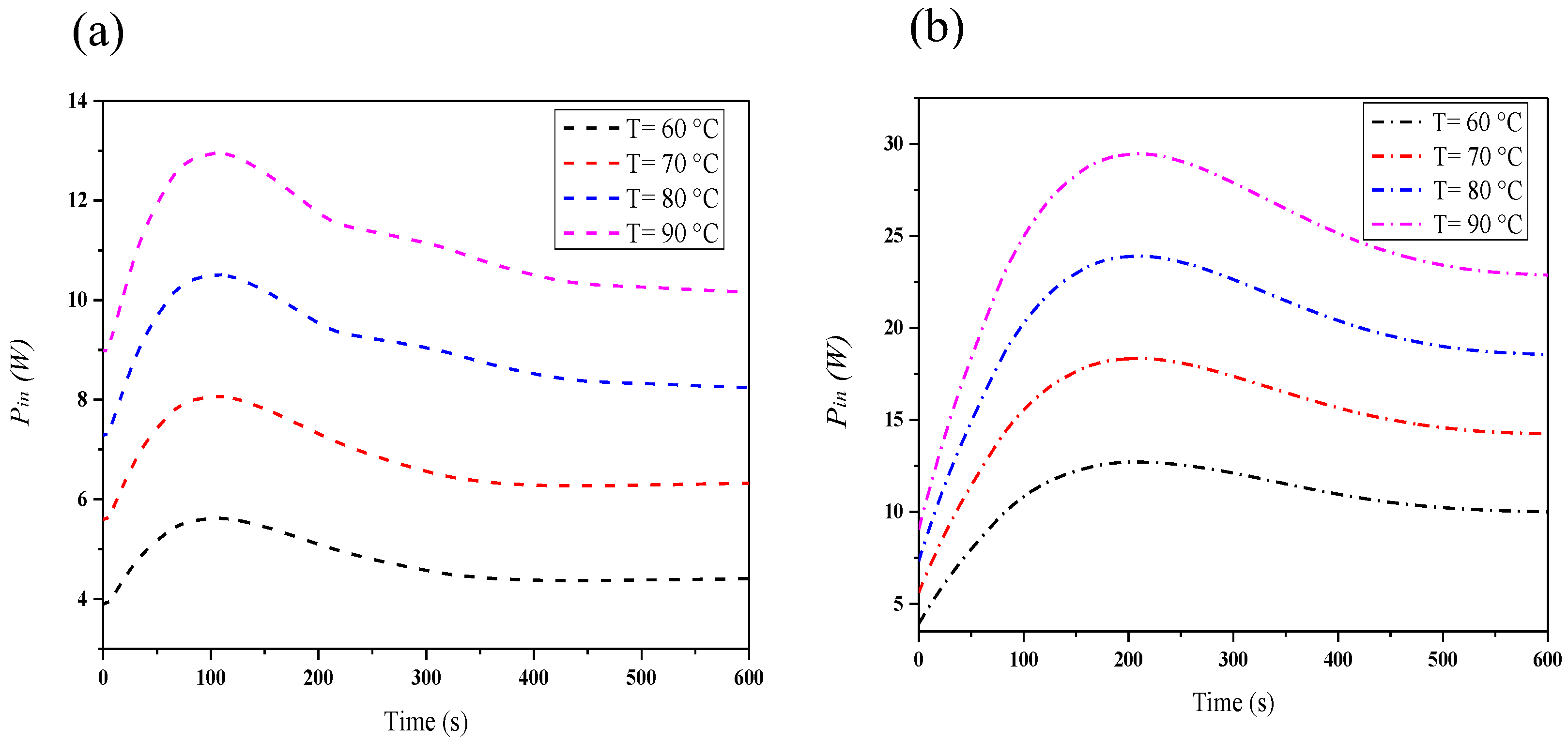
3.1. Effect of Target Tip Temperature on the Applied Input Power during MWA
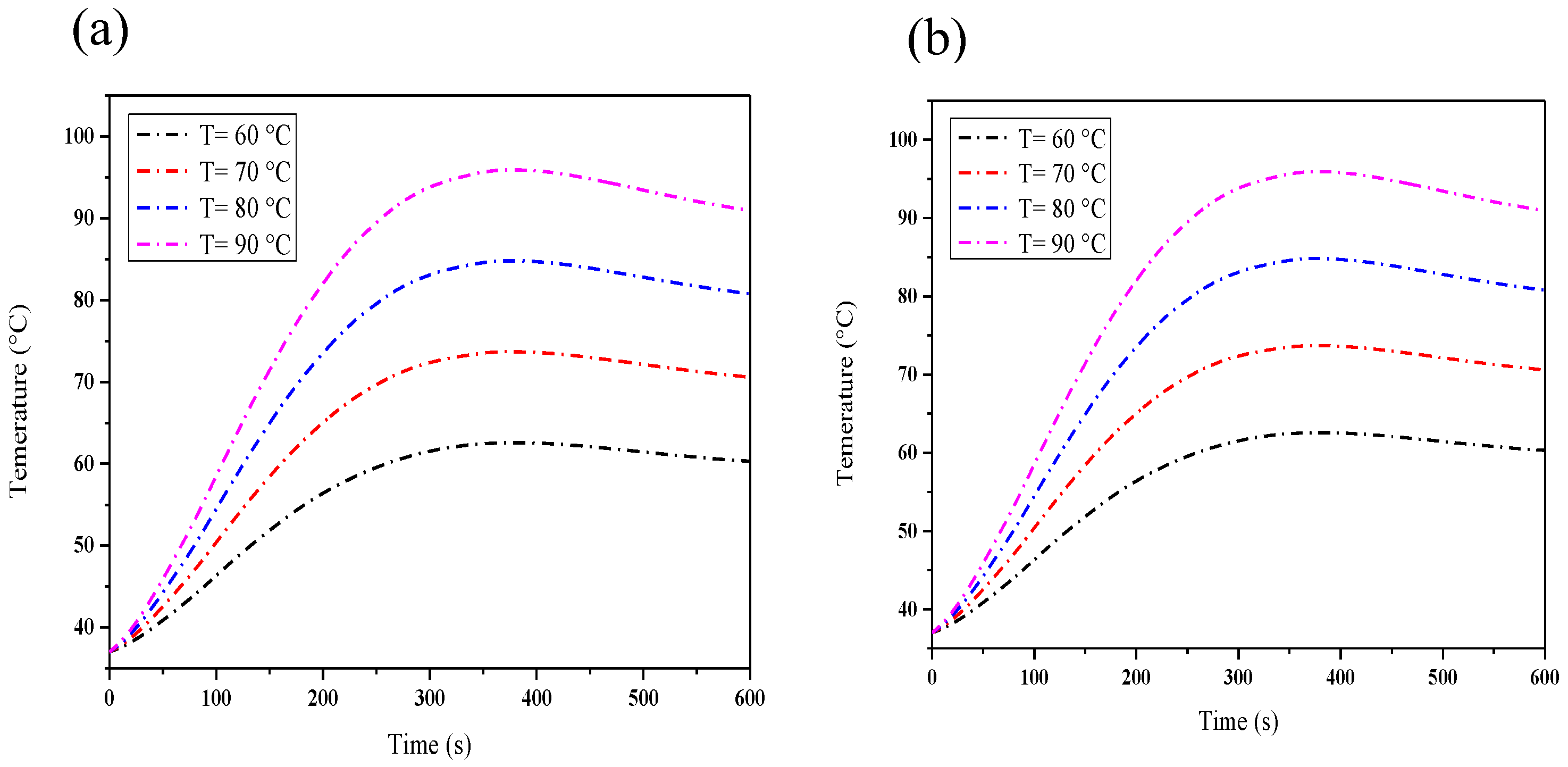
3.2. Effect of Target Tip Temperature on Temperature during MWA
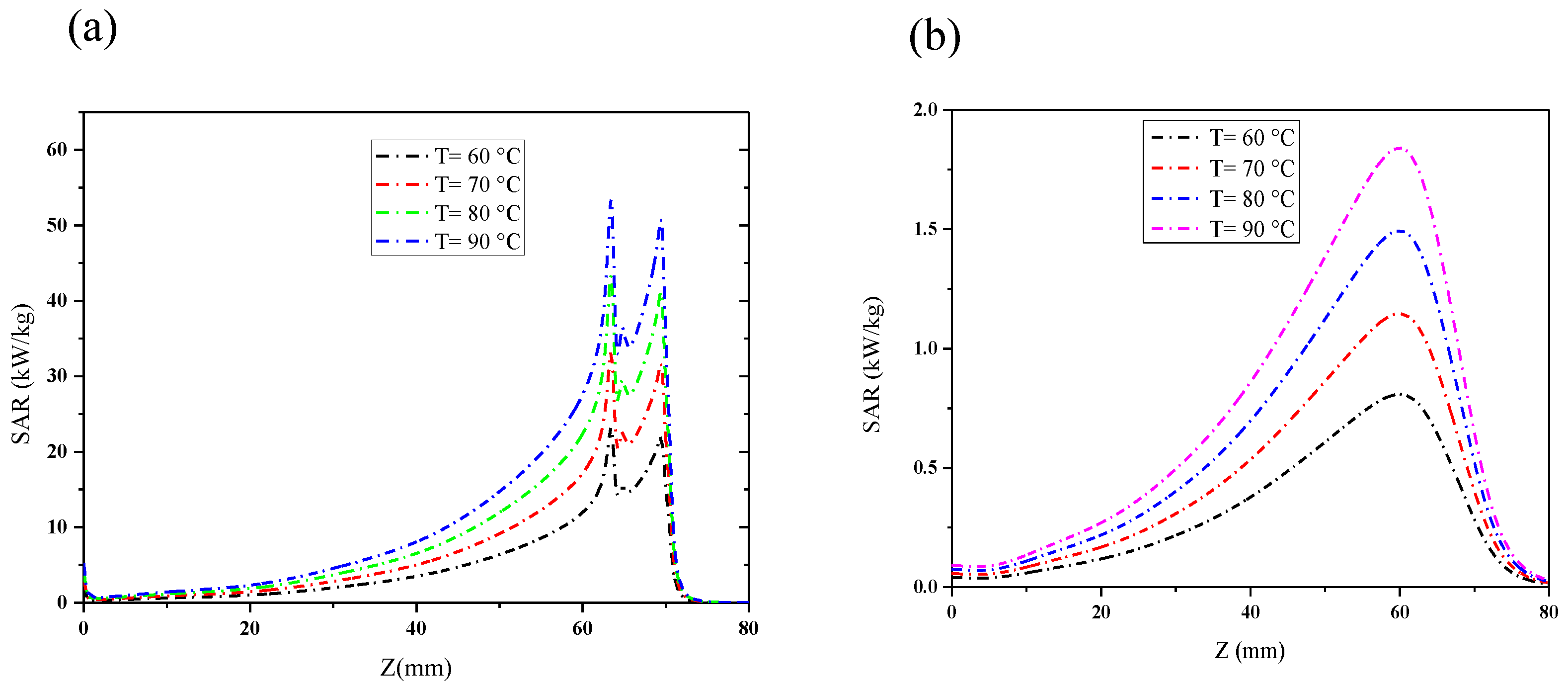
3.3. Effect of Target Tip Temperature on SAR
3.4. Effect of Target Tip Temperature on the Fraction of Necrotic Tissue
4. Conclusions
Funding
Data Availability Statement
Conflicts of Interest
References
- Zhu, Q.; Chua, M.H.; Ong, P.J.; Cheng Lee, J.J.; Le Osmund Chin, K.; Wang, S.; Kai, D.; Ji, R.; Kong, J.; Dong, Z.; et al. Recent advances in nanotechnology-based functional coatings for the built environment. Mater. Today Adv. 2022, 15, 100270. [Google Scholar] [CrossRef]
- An, C.; Sun, C.; Li, N.; Huang, B.; Jiang, J.; Shen, Y.; Wang, C.; Zhao, X.; Cui, B.; Wang, C.; et al. Nanomaterials and nanotechnology for the delivery of agrochemicals: Strategies towards sustainable agriculture. J. Nanobiotechnol. 2022, 20, 11. [Google Scholar] [CrossRef]
- Subramaniyan, V.; Fuloria, S.; Gupta, G.; Kumar, D.H.; Sekar, M.; Sathasivam, K.V.; Sudhakar, K.; Alharbi, K.S.; Al-Malki, W.H.; Afzal, O.; et al. A review on epidermal growth factor receptor’s role in breast and non-small cell lung cancer. Chem.-Biol. Interact. 2022, 351, 109735. [Google Scholar] [CrossRef] [PubMed]
- Roy, N.; Villavisanis, D.F.; Taub, P.J. Mitigating financial toxicity in breast cancer from diagnosis to treatment and reconstruction. Clin. Breast Cancer 2023, 23, e32–e36. [Google Scholar] [CrossRef] [PubMed]
- Beaver, S.K.; Mesa-Torres, N.; Pey, A.L.; Timson, D.J. NQO1: A target for the treatment of cancer and neurological diseases, and a model to understand loss of function disease mechanisms. Biochim. Biophys. Acta Proteins Proteom. 2019, 1867, 663–676. [Google Scholar] [CrossRef]
- Parsa, N. Environmental factors inducing human cancers. Iran. J. Public Health 2012, 41, 1–9. Available online: https://ijph.tums.ac.ir/index.php/ijph/article/view/2480 (accessed on 3 January 2024).
- George, J.; Lim, J.S.; Jang, S.J.; Cun, Y.; Ozretić, L.; Kong, G.; Leenders, F.; Lu, X.; Fernández-Cuesta, L.; Bosco, G.; et al. Comprehensive genomic profiles of small cell lung cancer. Nature 2015, 524, 47–53. [Google Scholar] [CrossRef]
- Donato, S.; Brombal, L.; Arana Peña, L.M.; Arfelli, F.; Contillo, A.; Delogu, P.; Di Lillo, F.; Di Trapani, V.; Fanti, V.; Longo, R.; et al. Optimization of a customized simultaneous algebraic reconstruction technique algorithm for phase-contrast breast computed tomography. Phys. Med. Biol. 2022, 67, 95012. [Google Scholar] [CrossRef]
- Dharmaiah, S.; Zeng, J.; Rao, V.S.; Zi, O.; Ma, T.; Yu, K.; Bhatt, H.; Shah, C.; Godley, A.; Xia, P.; et al. Clinical and dosimetric evaluation of recurrent breast cancer patients treated with hyperthermia and radiation. Int. J. Hyperth. 2019, 36, 986–992. [Google Scholar] [CrossRef]
- Oršolić, N.; Odeh, D.; Jembrek, M.J.; Knežević, J.; Kučan, D. Interactions between cisplatin and quercetin at physiological and hyperthermic conditions on cancer cells in vitro and in vivo. Molecules 2020, 25, 3271. [Google Scholar] [CrossRef]
- Bailey, C.W.; Sydnor, M.K., Jr. Current state of tumor ablation therapies. Dig. Dis. Sci. 2019, 64, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhu, N. Recent advances in microwave photonics. Front. Optoelectron. 2016, 9, 160–185. [Google Scholar] [CrossRef]
- Rosen, A.; Stuchly, M.A.; Vorst, A.V. Applications of RF/microwaves in medicine. IEEE Trans. Microw. Theory Tech. 2002, 50, 963–974. [Google Scholar] [CrossRef]
- Chandrasekaran, S.; Ramanathan, S.; Basak, T. Microwave food processing—A review. Food Res. Int. 2013, 52, 243–261. [Google Scholar] [CrossRef]
- Kim, J.; Mun, S.C.; Ko, H.-U.; Kim, K.-B.; Khondoker, M.A.H.; Zhai, L. Review of microwave assisted manufacturing technologies. Int. J. Precis. Eng. Manuf. 2012, 13, 2263–2272. [Google Scholar] [CrossRef]
- Vander Vorst, A.; Rosen, A.; Kotsuka, Y. RF/Microwave Interaction with Biological Tissues; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2006. [Google Scholar] [CrossRef]
- Parés, C.; Berjano, E.; González-Suárez, A. Effect of intracardiac blood flow pulsatility during radiofrequency cardiac ablation: Computer modeling study. Int. J. Hyperth. 2021, 38, 316–325. [Google Scholar] [CrossRef] [PubMed]
- Adabbo, G.; Andreozzi, A.; Iasiello, M.; Netti, P.A.; Vanoli, G.P. A 3D numerical model of controlled drug delivery to solid tumor by means of mild microwave hyperthermia-activated thermo-sensitive liposomes. Int. J. Therm. Sci. 2023, 193, 108528. [Google Scholar] [CrossRef]
- Testoni, S.G.G.; Healey, A.J.; Dietrich, C.F.; Arcidiacono, P.G. Systematic review of endoscopy ultrasound-guided thermal ablation treatment for pancreatic cancer. Endosc. Ultrasound 2020, 9, 83–100. [Google Scholar] [CrossRef]
- Wada, T.; Sugimoto, K.; Sakamaki, K.; Takahashi, H.; Kakegawa, T.; Tomita, Y.; Abe, M.; Yoshimasu, Y.; Takeuchi, H.; Itoi, T. Comparisons of radiofrequency ablation, microwave ablation, and irreversible electroporation by using propensity score analysis for early stage hepatocellular carcinoma. Cancers 2023, 15, 732. [Google Scholar] [CrossRef]
- Cornelis, F.H.; Marcelin, C.; Bernhard, J.C. Microwave ablation of renal tumors: A narrative review of technical considerations and clinical results. Diagn. Interv. Imaging 2017, 98, 287–297. [Google Scholar] [CrossRef]
- Prakash, P. Theoretical modeling for hepatic microwave ablation. Open Biomed. Eng. J. 2010, 4, 27–38. [Google Scholar] [CrossRef]
- Floridi, C.; De Bernardi, I.; Fontana, F.; Muollo, A.; Ierardi, A.M.; Agostini, A.; Fonio, P.; Squillaci, E.; Brunese, L.; Fugazzola, C.; et al. Microwave ablation of renal tumors: State of the art and development trends. Radiol. Medica 2014, 119, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Zhang, L.; Moser, M.A.J.; Zhang, W.; Zhang, B. A review of antenna designs for percutaneous microwave ablation. Phys. Medica 2021, 84, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Wakaki, T.; Michiyama, T.; Kuwano, S. A new interstitial choke embedded antenna for microwave ablation. IEICE Commun. Express 2017, 6, 435–438. [Google Scholar] [CrossRef]
- Wang, T.; Zhao, G.; Qiu, B. Theoretical evaluation of the treatment effectiveness of a novel coaxial multi-slot antenna for conformal microwave ablation of tumors. Int. J. Heat Mass Transf. 2015, 90, 81–91. [Google Scholar] [CrossRef]
- Radmilović-Radjenović, M.; Sabo, M.; Prnova, M.; Šoltes, L.; Radjenović, B. Finite element analysis of the microwave ablation method for enhanced lung cancer treatment. Cancers 2021, 13, 3500. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Zhao, J.; Li, W.; Yang, Y.; Liu, J.; Qian, Z. A coaxial slot antenna with frequency of 433 MHz for microwave ablation therapies: Design, simulation, and experimental research. Med. Biol. Eng. Comput. 2017, 55, 2027–2036. [Google Scholar] [CrossRef] [PubMed]
- Curto, S.; Taj-Eldin, M.; Fairchild, D.; Prakash, P. Microwave ablation at 915 MHz vs 2.45 GHz: A theoretical and experimental investigation. Med. Phys. 2015, 42, 6152–6161. [Google Scholar] [CrossRef]
- Tian, Z.; Cheng, Y.; Dong, T.; Gao, X.; Nan, Q. Numerical study for lung microwave ablation in different thermal and electrical properties. In World Congress on Medical Physics and Biomedical Engineering 2018. June 3–8, 2018, Prague, Czech Republic (Vol. 1); Lhotska, L., Sukupova, L., Lacković, I., Ibbot, G.S., Eds.; Springer Nature Singapore Pte Ltd.: Singapore, 2019; pp. 563–566. [Google Scholar] [CrossRef]
- Mai, X.; Wu, N.; Nan, Q.; Bi, S. Simulation study of microwave ablation of porous lung tissue. Appl. Sci. 2023, 13, 625. [Google Scholar] [CrossRef]
- Rattanadecho, P.; Keangin, P. Numerical study of heat transfer and blood flow in two-layered porous liver tissue during microwave ablation process using single and double slot antenna. Int. J. Heat Mass Transf. 2013, 58, 457–470. [Google Scholar] [CrossRef]
- Andreozzi, A.; Brunese, L.; Iasiello, M.; Tucci, C.; Vanoli, G.P. Modeling heat transfer in tumors: A review of thermal therapies. Ann. Biomed. Eng. 2019, 47, 676–693. [Google Scholar] [CrossRef]
- Nakayama, A.; Kuwahara, F. A general bioheat transfer model based on the theory of porous media. Int. J. Heat Mass Transf. 2008, 51, 3190–3199. [Google Scholar] [CrossRef]
- Selmi, M.; Iqbal, A.; Smida, A.; Waly, M.I.; Belmabrouk, H. Modeling of heat transfer distribution in tumor breast cancer during microwave ablation therapy. Microw. Opt. Technol. Lett. 2022, 64, 1364–1375. [Google Scholar] [CrossRef]
- Selmi, M.; Bajahzar, A.; Belmabrouk, H. Effects of target temperature on thermal damage during temperature-controlled MWA of liver tumor. Case Stud. Therm. Eng. 2022, 31, 101821. [Google Scholar] [CrossRef]
- Pennes, H.H. Analysis of tissue and arterial blood temperatures in the resting human forearm. 1948. J. Appl. Physiol. 1998, 85, 5–34. [Google Scholar] [CrossRef]
- Krishnan, R.; Christ, J. An investigation using specific absorption rate analysis to diagnose early-stage breast tumor using UWB antenna. Curr. Med. Imaging 2021, 17, 1425–1431. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, L.; Cavarzan, F.; Ciampitti, L.; Cremonesi, M.; Grilli, F.; Saccomandi, P. Thermophysical and mechanical properties of biological tissues as a function of temperature: A systematic literature review. Int. J. Hyperth. 2022, 39, 297–340. [Google Scholar] [CrossRef] [PubMed]
- Wardhana, G.; Almeida, J.P.; Abayazid, M.; Fütterer, J.J. Development of a thermal model for irreversible electroporation: An approach to estimate and optimize the IRE protocols. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 1325–1334. [Google Scholar] [CrossRef]
- Keangin, P.; Rattanadecho, P.; Wessapan, T. An analysis of heat transfer in liver tissue during microwave ablation using single and double slot antenna. Int. Commun. Heat Mass Transf. 2011, 38, 757–766. [Google Scholar] [CrossRef]
- Selmi, M.; Bin Dukhyil, A.A.; Belmabrouk, H. Numerical analysis of human cancer therapy using microwave ablation. Appl. Sci. 2020, 10, 211. [Google Scholar] [CrossRef]
- Singh, S.; Repaka, R. Effect of different breast density compositions on thermal damage of breast tumor during radiofrequency ablation. Appl. Therm. Eng. 2017, 125, 443–451. [Google Scholar] [CrossRef]
- Singh, S.; Repaka, R. Numerical investigation of convective cooling in minimizing skin burns during radiofrequency ablation of breast tumor. Sādhanā 2018, 43, 90. [Google Scholar] [CrossRef]
- Jasiński, M. Investigation of tissue thermal damage process with application of direct sensitivity method. Mol. Cell. Biomech. 2013, 10, 183–199. [Google Scholar] [CrossRef]
- Wang, X.R.; Gao, H.J.; Wu, S.C.; Jiang, T.; Zhou, Z.H.; Bai, Y.P. Numerical evaluation of ablation zone under different tip temperatures during radiofrequency ablation. Math. Biosci. Eng. 2019, 16, 2514–2531. [Google Scholar] [CrossRef] [PubMed]
- Lim, D.; Namgung, B.; Woo, D.G.; Choi, J.S.; Kim, H.S.; Tack, G.R. Effect of input waveform pattern and large blood vessel existence on destruction of liver tumor using radiofrequency ablation: Finite element analysis. J. Biomech. Eng. 2010, 132, 61003. [Google Scholar] [CrossRef] [PubMed]
- Radosevic, A.; Prieto, D.; Burdío, F.; Berjano, E.; Prakash, P.; Trujillo, M. Short pulsed microwave ablation: Computer modeling and ex vivo experiments. Int. J. Hyperth. 2021, 38, 409–420. [Google Scholar] [CrossRef]
- Chen, Z. Finite Element Methods and Their Applications; Springer: Berlin/Heidelberg, Germany, 2005. [Google Scholar] [CrossRef]
- Yang, D.; Converse, M.C.; Mahvi, D.M.; Webster, J.G. Expanding the bioheat equation to include tissue internal water evaporation during heating. IEEE Trans. Bio-Med. Eng. 2007, 54, 1382–1388. [Google Scholar] [CrossRef]
- Jamil, M.; Ng, E.Y. Quantification of the effect of electrical and thermal parameters on radiofrequency ablation for concentric tumour model of different sizes. J. Therm. Biol. 2015, 51, 23–32. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Selmi, M. Improved Modeling of Temperature Evolution during Lung Cancer Tumor Thermal Ablation. Physics 2024, 6, 164-176. https://doi.org/10.3390/physics6010012
Selmi M. Improved Modeling of Temperature Evolution during Lung Cancer Tumor Thermal Ablation. Physics. 2024; 6(1):164-176. https://doi.org/10.3390/physics6010012
Chicago/Turabian StyleSelmi, Marwa. 2024. "Improved Modeling of Temperature Evolution during Lung Cancer Tumor Thermal Ablation" Physics 6, no. 1: 164-176. https://doi.org/10.3390/physics6010012
APA StyleSelmi, M. (2024). Improved Modeling of Temperature Evolution during Lung Cancer Tumor Thermal Ablation. Physics, 6(1), 164-176. https://doi.org/10.3390/physics6010012