
Is IBD Disk a Reliable Tool to Detect Depression in IBD Patients? A Comparison with Becks’ Depression Inventory


Abstract
1. Introduction
2. Results
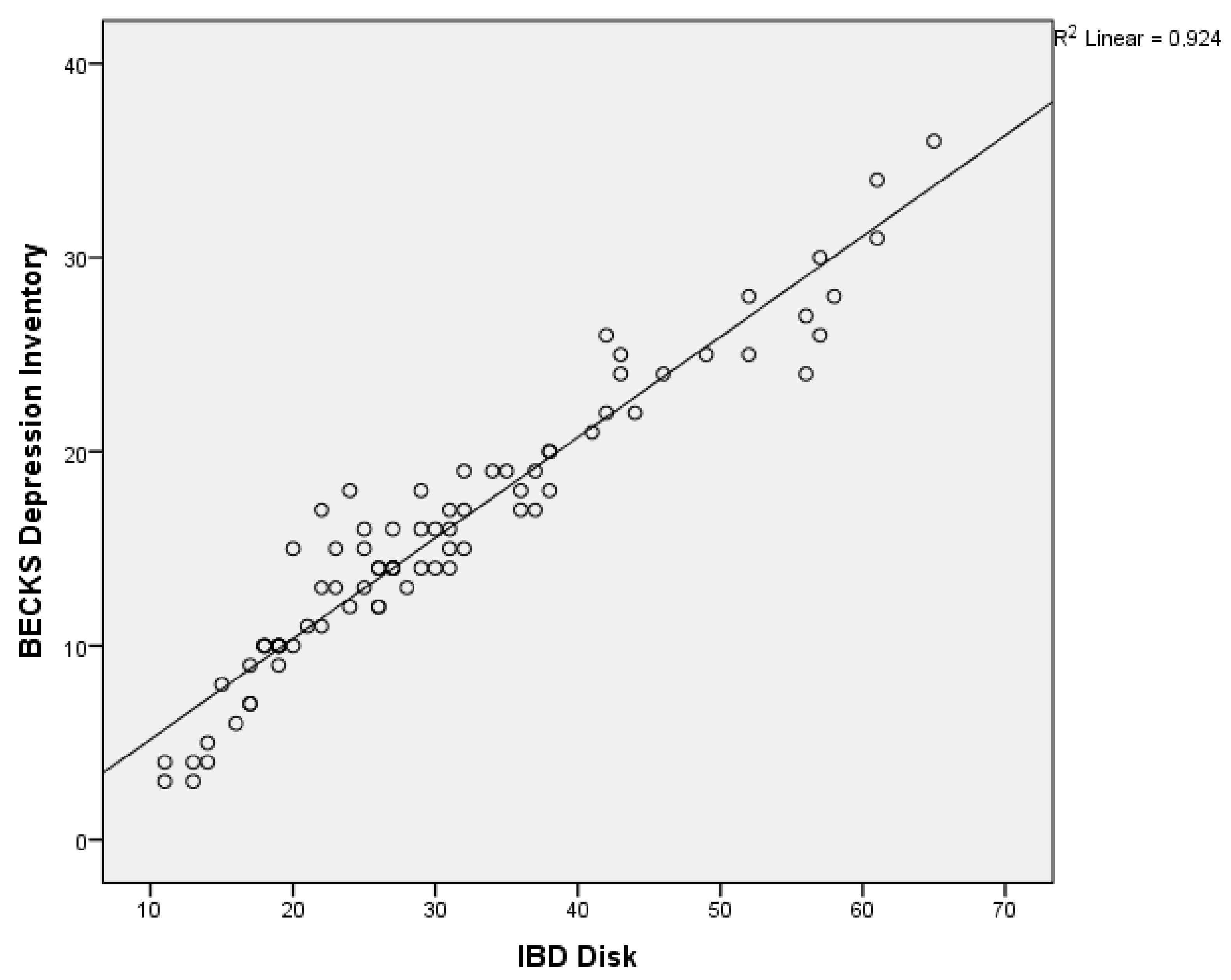
2.1. Score Values and Correlations
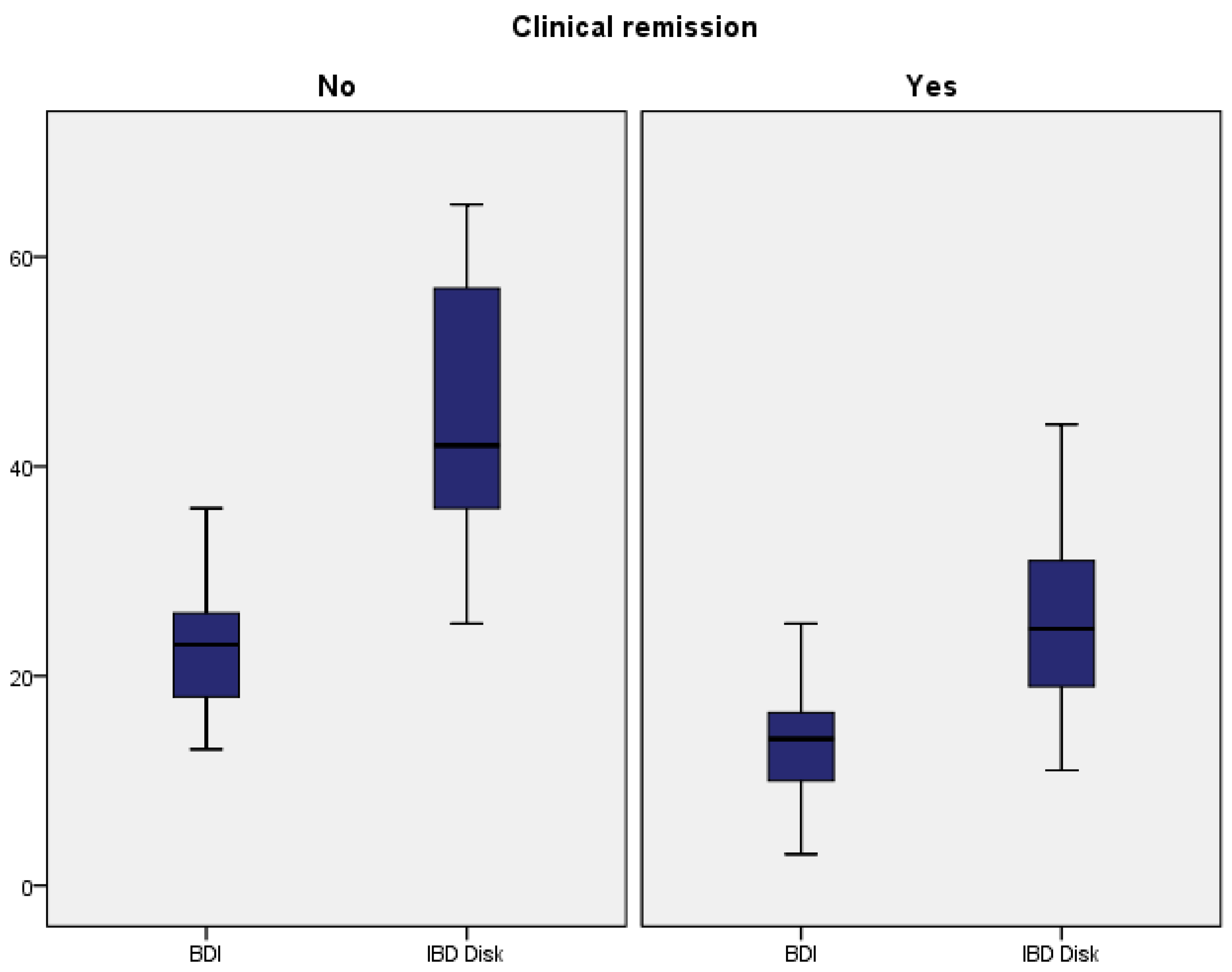
2.2. Performance and Differences Between the Tests
3. Discussion
4. Materials and Methods
4.1. Study Design and Participants
4.2. Questionnaires
4.3. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L.; Colombel, J.F. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef]
- Pierik, M.; Yang, H.; Barmada, M.M.; Cavanaugh, J.A.; Annese, V.; Brant, S.R.; Cho, J.H.; Duerr, R.H.; Hugot, J.P.; McGovern, D.P.; et al. The IBD international genetics consortium provides further evidence for linkage to IBD4 and shows gene-environment interaction. Inflamm. Bowel Dis. 2005, 11, 1–7. [Google Scholar] [CrossRef]
- Barberio, B.; Zamani, M.; Black, C.J.; Savarino, E.V.; Ford, A.C. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Vavricka, S.R.; Schoepfer, A.; Scharl, M.; Lakatos, P.L.; Navarini, A.; Rogler, G. Extraintestinal manifestations of inflammatory bowel disease. Inflamm. Bowel Dis. 2015, 21, 1982–1992. [Google Scholar] [CrossRef] [PubMed]
- Mikocka-Walus, A.; Knowles, S.R.; Keefer, L.; Graff, L. Controversies Revisited: A Systematic Review of the Comorbidity of Depression and Anxiety with Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2016, 22, 752–762. [Google Scholar] [CrossRef]
- Taft, T.H.; Quinton, S.; Jedel, S.; Simons, M.; Mutlu, E.A.; Hanauer, S.B. Posttraumatic Stress in Patients with Inflammatory Bowel Disease: Prevalence and Relationships to Patient-Reported Outcomes. Inflamm. Bowel Dis. 2022, 28, 710–719. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef] [PubMed]
- Avinir, A.; Dar, S.; Taler, M.; Haj, O.; Gothelf, D.; Kopylov, U.; Ben-Horin, S.; Mekori-Domachevsky, E. Keeping it simple: Mental health assessment in the Gastroenterology Department—Using the Hospital Anxiety and Depression Scale (HADS) for Patients with IBDin Israel. Therap. Adv. Gastroenterol. 2022, 15, 17562848211066439. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kappelman, M.D.; Long, M.D.; Martin, C.; DeWalt, D.A.; Kinneer, P.M.; Chen, W.; Lewis, J.D.; Sandler, R.S. Evaluation of the patient reported outcomes measurement information system in a large cohort of patients with inflammatory bowel diseases. Clin. Gastroenterol. Hepatol. 2014, 12, 1315–1323.e2. [Google Scholar] [CrossRef]
- Cohen, B.L.; Zoëga, H.; Shah, S.A.; Leleiko, N.; Lidofsky, S.; Bright, R.; Flowers, N.; Law, M.; Moniz, H.; Merrick, M.; et al. Fatigue is highly associated with poor health-related quality of life, disability and depression in newly diagnosed patients with inflammatory bowel disease, independent of disease activity. Aliment. Pharmacol. Ther. 2014, 39, 811–822. [Google Scholar] [CrossRef]
- Gao, N.; Qiao, Z.; Yan, S.; Zhu, L. Evaluation of health-related quality of life and influencing factors in patients with Crohn disease. J. Int. Med. Res. 2022, 50, 3000605221098868. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gong, G.; Xu, C.; Zhang, Z.; Zheng, Y. Association between depression and anxiety with the risk and flare of inflammatory bowel disease: A systematic review and meta-analysis. Intern. Emerg. Med. 2024, 20, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Seaton, N.; Hudson, J.; Harding, S.; Norton, S.; Mondelli, V.; Jones, A.S.K.; Moss-Morris, R. Do interventions for mood improve inflammatory biomarkers in inflammatory bowel disease? a systematic review and meta-analysis. EBioMedicine 2024, 100, 104910. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Choi, K.; Chun, J.; Han, K.; Park, S.; Soh, H.; Kim, J.; Lee, J.; Lee, H.J.; Im, J.P.; Kim, J.S. Risk of anxiety and depression in patients with inflammatory bowel disease: A nationwide, population-based study. J. Clin. Med. 2019, 8, 654. [Google Scholar] [CrossRef]
- Bisgaard, T.H.; Allin, K.H.; Elmahdi, R.; Jess, T. The bidirectional risk of inflammatory bowel disease and anxiety or depression: A systematic review and meta-analysis. Gen. Hosp. Psychiatry 2023, 83, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Gupta, Y.K.; Dhaliwal, A.S.; Kahlon, B.K.; Bansal, V.; Mahajan, R.; Mehta, V.; Singh, D.; Kaur, R.; Bansal, N.; et al. Inflammatory bowel disease (IBD)-disk accurately predicts the daily life burden and parallels disease activity in patients with IBD. Intest. Res. 2023, 21, 375–384. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Simrén, M.; Axelsson, J.; Gillberg, R.; Abrahamsson, H.; Svedlund, J.; Björnsson, E.S. Quality of life in inflammatory bowel disease in remission: The impact of IBS-like symptoms and associated psychological factors. Am. J. Gastroenterol. 2002, 97, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Mittermaier, C.; Dejaco, C.; Waldhoer, T.; Oefferlbauer-Ernst, A.; Miehsler, W.; Beier, M.; Tillinger, W.; Gangl, A.; Moser, G. Impact of depressive mood on relapse in patients with inflammatory bowel disease: A prospective 18-month follow-up study. Psychosom. Med. 2004, 66, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Neuendorf, R.; Harding, A.; Stello, N.; Hanes, D.; Wahbeh, H. Depression and anxiety in patients with Inflammatory Bowel Disease: A systematic review. J. Psychosom. Res. 2016, 87, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W. Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Çataltepe, E.; Ekmen, N.; Cindoruk, M. Comparison of depression and anxiety in inflammatory bowel patients treated with anti- TNF or immune modulators. J. Exp. Clin. Med. 2023, 40, 47–51. [Google Scholar] [CrossRef]
- Byrne, G.; Rosenfeld, G.; Leung, Y.; Qian, H.; Raudzus, J.; Nunez, C.; Bressler, B. Prevalence of Anxiety and Depression in Patients with Inflammatory Bowel Disease. Can. J. Gastroenterol. Hepatol. 2017, 2017, 6496727. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sochal, M.; Małecka-Panas, E.; Gabryelska, A.; Talar-Wojnarowska, R.; Szmyd, B.; Krzywdzińska, M.; Białasiewicz, P. Determinants of Sleep Quality in Inflammatory Bowel Diseases. J. Clin. Med. 2020, 9, 2921. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Peyrin-Biroulet, L.; Cieza, A.; Sandborn, W.J.; Coenen, M.; Chowers, Y.; Hibi, T.; Kostanjsek, N.; Stucki, G.; Colombel, J.F.; International Programme to Develop New Indexes for Crohn’s Disease (IPNIC) Group. Development of the first disability index for inflammatory bowel disease based on the international classification of functioning, disability and health. Gut 2012, 61, 241–247. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ghosh, S.; Louis, E.; Beaugerie, L.; Bossuyt, P.; Bouguen, G.; Bourreille, A.; Ferrante, M.; Franchimont, D.; Frost, K.; Hebuterne, X.; et al. Development of the IBD Disk: A Visual Self-administered Tool for Assessing Disability in Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2017, 23, 333–340. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Silva Mendes, S.; Ferreira, P.; Antunes, P.; Gonçalves, M.; Leal, T.; Gonçalves, B.; Rebelo, A.; Arroja, B.; Caetano, A.C.; Gonçalves, R.; et al. Validation of the IBD-Disk in a Portuguese cohort. Eur. J. Gastroenterol. Hepatol. 2021, 33 (Suppl. 1), e961–e969. [Google Scholar] [CrossRef] [PubMed]
- Katsoula, A.; Axiaris, G.; Mpitouli, A.; Palatianou, M.; Christidou, A.; Dimitriadis, N.; Nakos, A.; Pastras, P.; Kourkoulis, P.; Karatzas, P.; et al. The Inflammatory Bowel Disease-Disk Tool for Assessing Disability in Inflammatory Bowel Disease Patients: Validation of the Greek Version. J. Clin. Med. 2023, 12, 3023. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meeralam, Y.; Al-Zanbagi, A.B.; Al Saedi, M.; Alharthi, W.; Sabbahi, H.A.; Alhejaili, T.; Shariff, M.K. IBD-Disk as a tool estimating the prevalence of inflammatory bowel disease-related disability and associated influencing factors in Saudi Arabia: A cross-sectional study. Saudi J. Gastroenterol. 2023, 29, 309–315. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
| Characteristics | Value (n = 82) |
|---|---|
| Age (mean +/− SD) | 43.11 +/− 13.7 |
| Gender—Female (%) | 30 (36.6%) |
| Gender—male (%) | 52 (63.4%) |
| Ulcerative colitis (%) | 32 (39.0%) |
| UC—Proctitis (%) | 5 (15.6%) |
| UC—Left colitis (%) | 18 (56.3%) |
| UC—Pancolitis (%) | 10 (31.3%) |
| Crohn’s Disease (%) | 50 (61.0%) |
| CD—Ileal involvement (%) | 8 (16.0%) |
| CD—Colonic involvement (%) | 5 (10.0%) |
| CD—Ileocolonic involvement (%) | 36 (72.0%) |
| CD—Upper digestive tract involvement (%) | 1 (2.0%) |
| CD—Perianal disease (%) | 8 (16.0%) |
| CD—Stricturing phenotype (%) | 32 (64.0%) |
| CD—Penetrating phenotype (%) | 14 (28.0%) |
| Surgical intervention (%) | 22 (26.8%) |
| 5-ASA medication (%) | 76 (92.7%) |
| Biologic therapy (%) | 82 (100%) |
| Clinical remission (%) | 60 (73.2%) |
| Endoscopic remission (%) | 49 (59.7%) |
| BDI vs. IBD Disk Question | rs(80) | p-Value |
|---|---|---|
| Q1–Q7—depression | 0.835 | <0.001 |
| Q12–Q3—social interactions | 0.723 | <0.001 |
| Q14–Q8—body image | 0.904 | <0.001 |
| Q15–Q4—job performance | 0.772 | <0.001 |
| Q16–Q5—quality of sleep | 0.637 | <0.001 |
| Q21–Q9—sexual activity | 0.884 | <0.001 |
| Test | Nagelkerke Value | B | Wald | p-Value | Exp (B) -OR | 95% CI |
|---|---|---|---|---|---|---|
| BDI | 0.456 | −0.24 | 17.94 | 0.001 | 0.78 | 0.69–0.87 |
| IBD Disk | 0.437 | −0.11 | 18.47 | 0.001 | 0.88 | 0.84–0.93 |
| Test | Clinical Remission | Test Value | |
|---|---|---|---|
| Yes | No | ||
| BDI | 13.35 (5.64) | 22.73 (6.51) | W = 180.00 ** |
| IBD | 25.90 (10.51) | 43.45 (12.62) | W = 178.00 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spataru, T.; Stemate, A.; Cozma, M.; Fleschiu, A.; Popescu, R.; Negreanu, L. Is IBD Disk a Reliable Tool to Detect Depression in IBD Patients? A Comparison with Becks’ Depression Inventory. Gastrointest. Disord. 2025, 7, 23. https://doi.org/10.3390/gidisord7010023
Spataru T, Stemate A, Cozma M, Fleschiu A, Popescu R, Negreanu L. Is IBD Disk a Reliable Tool to Detect Depression in IBD Patients? A Comparison with Becks’ Depression Inventory. Gastrointestinal Disorders. 2025; 7(1):23. https://doi.org/10.3390/gidisord7010023
Chicago/Turabian StyleSpataru, Teodora, Ana Stemate, Marina Cozma, Alexandru Fleschiu, Remus Popescu, and Lucian Negreanu. 2025. "Is IBD Disk a Reliable Tool to Detect Depression in IBD Patients? A Comparison with Becks’ Depression Inventory" Gastrointestinal Disorders 7, no. 1: 23. https://doi.org/10.3390/gidisord7010023
APA StyleSpataru, T., Stemate, A., Cozma, M., Fleschiu, A., Popescu, R., & Negreanu, L. (2025). Is IBD Disk a Reliable Tool to Detect Depression in IBD Patients? A Comparison with Becks’ Depression Inventory. Gastrointestinal Disorders, 7(1), 23. https://doi.org/10.3390/gidisord7010023