.png)



Gastrointestinal Group Education for Children and Adolescents with Functional Abdominal Pain Disorders—A Feasibility Study of a Brief Intervention

 ,
,
Abstract
:1. Introduction
2. Results
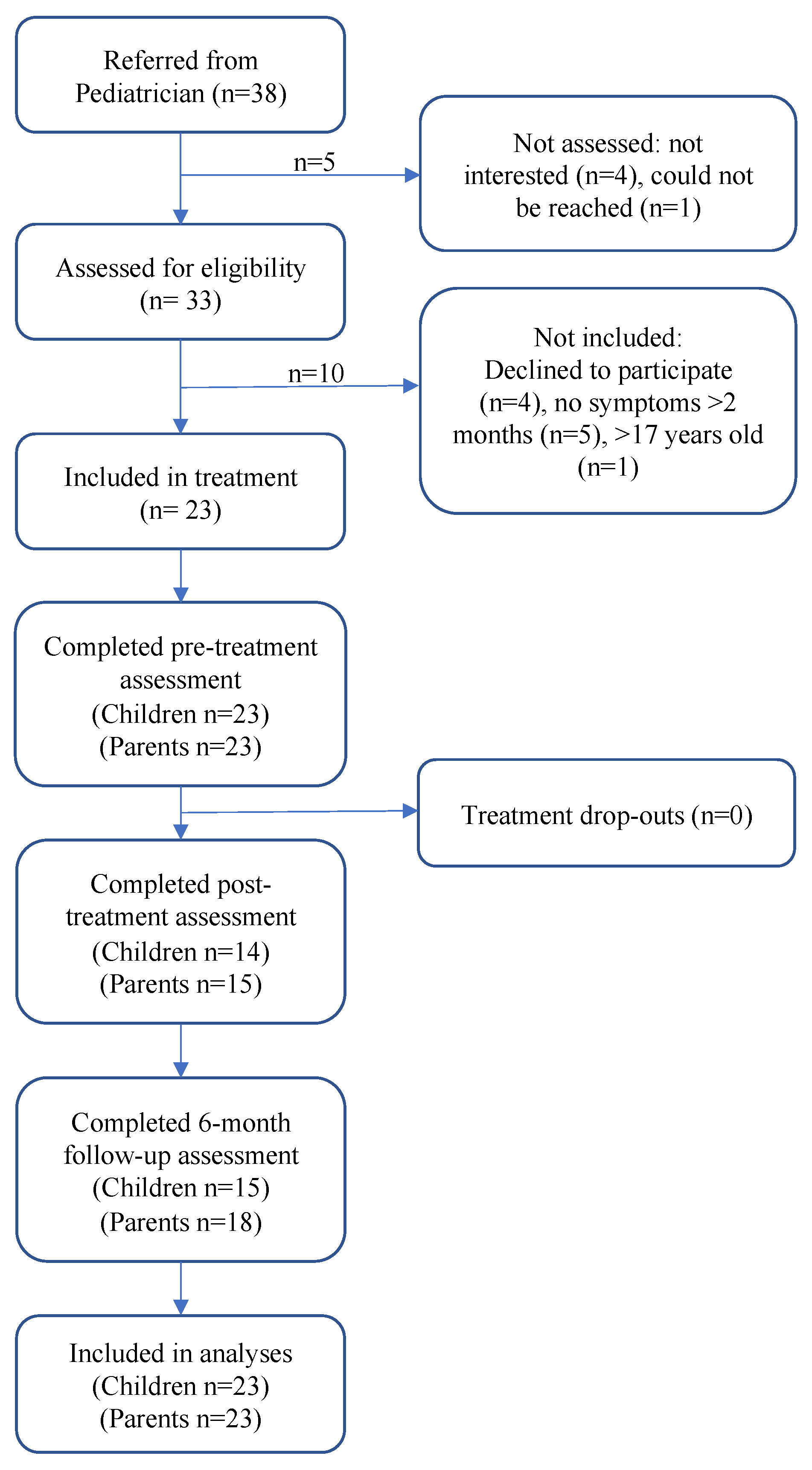
2.1. Description of Sample
2.2. Primary Aim, Feasibility and Acceptability
2.3. Secondary Aim, Results of Outcome Measures
2.3.1. Children and Adolescents
2.3.2. Parents
3. Discussion
4. Material and Methods
4.1. Study Design, Recruitment, Setting, and Participants
4.2. Collection, Handling, and Data Protection
4.3. Outcome Measures
4.3.1. Feasibility
4.3.2. Children’s Outcome Measures Assessed
4.3.3. Parent’s Outcome Measures
4.4. Intervention and Content
- Pediatric gastroenterologist (AU). Introduction and presentation of participants. Basic anatomy and physiology about the gastrointestinal tract, etiology, and diagnostics of FAPDs.
- Pediatric dietician (JW). Lifestyle and dietary factors such as eating regular meals, avoiding long intervals between meals, taking time for meals, and eating in a calm environment. Information on foods that can trigger symptoms, for example, food allergy and food intolerance such as FODMAPs (fermentable, oligosaccarides, disaccarides, monosaccarides, and polyoles). Explaining that excessive limitation of large food groups should be avoided, since it can lead to nutritional deficiencies and impaired growth.
- Pediatric gastroenterologist (AU). Explaining how to become an “expert of one’s own disease”, that is, getting to know one’s symptoms and when medicines and doctor’s appointments are needed. Presentation of the gut–brain axis, stress, protective factors, and brief information about evidence-based treatment.
- Pediatric psychologist trained in CBT (MB). General information about psychological factors regarding abdominal pain, acceptance, and coping. Principles of CBT, how fear of gastrointestinal symptoms and avoidance behavior affect symptoms.
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Board Review
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CBT | Cognitive behavioral therapy |
| FAPDs | Functional abdominal pain disorders |
| FD | Functional dyspepsia |
| GI | Gastrointestinal |
| FAP-NOS | Functional abdominal pain–not otherwise specified |
| IBS | Irritable bowel syndrome |
| VAS | Visual analogue scale |
References
- Uusijarvi, A.; Alm, J.; Lindblad, F.; Olen, O. Irritable bowel syndrome and functional abdominal pain in five-year-old children are related to lifestyle. Acta Paediatr. 2016, 105, 971–978. [Google Scholar] [CrossRef]
- Uusijarvi, A.; Bergstrom, A.; Simren, M.; Ludvigsson, J.F.; Kull, I.; Wickman, M.; Alm, J.; Olen, O. Use of antibiotics in infancy and childhood and risk of recurrent abdominal pain—A Swedish birth cohort study. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc. 2014, 26, 841–850. [Google Scholar] [CrossRef]
- Korterink, J.J.; Diederen, K.; Benninga, M.A.; Tabbers, M.M. Epidemiology of pediatric functional abdominal pain disorders: A meta-analysis. PLoS ONE 2015, 10, e0126982. [Google Scholar] [CrossRef]
- Hyams, J.S.; Di Lorenzo, C.; Saps, M.; Shulman, R.J.; Staiano, A.; van Tilburg, M. Functional Disorders: Children and Adolescents. Gastroenterology 2016, 150, 1456–1468.e2. [Google Scholar] [CrossRef]
- Simren, M.; Barbara, G.; Flint, H.J.; Spiegel, B.M.; Spiller, R.C.; Vanner, S.; Verdu, E.F.; Whorwell, P.J.; Zoetendal, E.G. Intestinal microbiota in functional bowel disorders: A Rome foundation report. Gut 2013, 62, 159–176. [Google Scholar] [CrossRef]
- Friesen, C.; Colombo, J.; Schurman, J. Update on the Role of Allergy in Pediatric Functional Abdominal Pain Disorders: A Clinical Perspective. Nutrients 2021, 13, 2056. [Google Scholar] [CrossRef]
- Karunanayake, A.; Devanarayana, N.M.; Rajindrajith, S. Early life events in functional abdominal pain disorders in children. PLoS ONE 2022, 17, e0275419. [Google Scholar] [CrossRef]
- Ayonrinde, O.T.; Sanfilippo, F.M.; O’Sullivan, T.A.; Adams, L.A.; Ayonrinde, O.A.; Robinson, M.; Oddy, W.H.; Olynyk, J.K. Bowel patterns, gastrointestinal symptoms, and emotional well-being in adolescents: A cohort study. J. Gastroenterol. Hepatol. 2019, 34, 1946–1954. [Google Scholar] [CrossRef] [PubMed]
- von Gontard, A.; Moritz, A.M.; Thome-Granz, S.; Equit, M. Abdominal pain symptoms are associated with anxiety and depression in young children. Acta Paediatr. 2015, 104, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Dhroove, G.; Chogle, A.; Saps, M. A million-dollar work-up for abdominal pain: Is it worth it? J. Pediatr. Gastroenterol. Nutr. 2010, 51, 579–583. [Google Scholar] [CrossRef] [PubMed]
- Stordal, K.; Nygaard, E.A.; Bentsen, B.S. Recurrent abdominal pain: A five-year follow-up study. Acta Paediatr. 2005, 94, 234–236. [Google Scholar] [PubMed]
- Crushell, E.; Rowland, M.; Doherty, M.; Gormally, S.; Harty, S.; Bourke, B.; Drumm, B. Importance of parental conceptual model of illness in severe recurrent abdominal pain. Pediatrics 2003, 112, 1368–1372. [Google Scholar] [CrossRef] [PubMed]
- Thapar, N.; Benninga, M.A.; Crowell, M.D.; Di Lorenzo, C.; Mack, I.; Nurko, S.; Saps, M.; Shulman, R.J.; Szajewska, H.; van Tilburg, M.A.L.; et al. Paediatric functional abdominal pain disorders. Nat. Rev. Dis. Primers 2020, 6, 89. [Google Scholar] [CrossRef] [PubMed]
- Rajindrajith, S.; Zeevenhooven, J.; Devanarayana, N.M.; Perera, B.J.C.; Benninga, M.A. Functional abdominal pain disorders in children. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 369–390. [Google Scholar] [CrossRef] [PubMed]
- Santucci, N.R.; Saps, M.; van Tilburg, M.A. New advances in the treatment of paediatric functional abdominal pain disorders. Lancet Gastroenterol. Hepatol. 2020, 5, 316–328. [Google Scholar] [CrossRef] [PubMed]
- Newlove-Delgado, T.V.; Martin, A.E.; Abbott, R.A.; Bethel, A.; Thompson-Coon, J.; Whear, R.; Logan, S. Dietary interventions for recurrent abdominal pain in childhood. Cochrane Database Syst. Rev. 2017, 3, CD010972. [Google Scholar] [CrossRef] [PubMed]
- Wallace, C.; Gordon, M.; Sinopoulou, V.; Akobeng, A.K. Probiotics for management of functional abdominal pain disorders in children. Cochrane Database Syst. Rev. 2023, 2, CD012849. [Google Scholar] [CrossRef]
- Pensabene, L.; Salvatore, S.; Turco, R.; Tarsitano, F.; Concolino, D.; Baldassarre, M.E.; Borrelli, O.; Thapar, N.; Vandenplas, Y.; Staiano, A.; et al. Low FODMAPs diet for functional abdominal pain disorders in children: Critical review of current knowledge. J. Pediatr. (Rio J.) 2019, 95, 642–656. [Google Scholar] [CrossRef]
- Martin, A.E.; Newlove-Delgado, T.V.; Abbott, R.A.; Bethel, A.; Thompson-Coon, J.; Whear, R.; Logan, S. Pharmacological interventions for recurrent abdominal pain in childhood. Cochrane Database Syst. Rev. 2017, 3, CD010973. [Google Scholar] [CrossRef]
- Bonnert, M.; Olen, O.; Lalouni, M.; Benninga, M.A.; Bottai, M.; Engelbrektsson, J.; Hedman, E.; Lenhard, F.; Melin, B.; Simren, M.; et al. Internet-Delivered Cognitive Behavior Therapy for Adolescents With Irritable Bowel Syndrome: A Randomized Controlled Trial. Am. J. Gastroenterol. 2017, 112, 152–162. [Google Scholar] [CrossRef]
- Lalouni, M.; Ljotsson, B.; Bonnert, M.; Ssegonja, R.; Benninga, M.; Bjureberg, J.; Hogstrom, J.; Sahlin, H.; Simren, M.; Feldman, I.; et al. Clinical and Cost Effectiveness of Online Cognitive Behavioral Therapy in Children With Functional Abdominal Pain Disorders. Clin. Gastroenterol. Hepatol. 2019, 17, 2236–2244 e2211. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Venkatanarayanan, N.; Kumar, L. A Systematic Review and Meta-Analysis of the Efficacy of Cognitive Behavioral Therapy for the Management of Pediatric Migraine. Headache 2017, 57, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Bonnert, M.; Olen, O.; Bjureberg, J.; Lalouni, M.; Hedman-Lagerlof, E.; Serlachius, E.; Ljotsson, B. The role of avoidance behavior in the treatment of adolescents with irritable bowel syndrome: A mediation analysis. Behav. Res. Ther. 2018, 105, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Lalouni, M.; Hesser, H.; Bonnert, M.; Hedman-Lagerlof, E.; Serlachius, E.; Olen, O.; Ljotsson, B. Breaking the vicious circle of fear and avoidance in children with abdominal pain: A mediation analysis. J. Psychosom. Res. 2021, 140, 110287. [Google Scholar] [CrossRef] [PubMed]
- Rexwinkel, R.; Vlieger, A.M.; Saps, M.; Tabbers, M.M.; Benninga, M.A. A therapeutic guide on pediatric irritable bowel syndrome and functional abdominal pain-not otherwise specified. Eur. J. Pediatr. 2022, 181, 2603–2617. [Google Scholar] [CrossRef] [PubMed]
- Labus, J.; Gupta, A.; Gill, H.K.; Posserud, I.; Mayer, M.; Raeen, H.; Bolus, R.; Simren, M.; Naliboff, B.D.; Mayer, E.A. Randomised clinical trial: Symptoms of the irritable bowel syndrome are improved by a psycho-education group intervention. Aliment. Pharmacol. Ther. 2013, 37, 304–315. [Google Scholar] [CrossRef] [PubMed]
- Lalouni, M.; Olen, O.; Bonnert, M.; Hedman, E.; Serlachius, E.; Ljotsson, B. Exposure-Based Cognitive Behavior Therapy for Children with Abdominal Pain: A Pilot Trial. PLoS ONE 2016, 11, e0164647. [Google Scholar] [CrossRef] [PubMed]
- Bonnert, M.; Olen, O.; Lalouni, M.; Hedman-Lagerlof, E.; Sarnholm, J.; Serlachius, E.; Ljotsson, B. Internet-Delivered Exposure-Based Cognitive-Behavioral Therapy for Adolescents With Functional Abdominal Pain or Functional Dyspepsia: A Feasibility Study. Behav. Ther. 2019, 50, 177–188. [Google Scholar] [CrossRef]
- Flik, C.E.; van Rood, Y.R.; de Wit, N.J. Systematic review: Knowledge and educational needs of patients with irritable bowel syndrome. Eur. J. Gastroenterol. Hepatol. 2015, 27, 367–371. [Google Scholar] [CrossRef]
- Brodwall, A.; Glavin, K.; Lagerlov, P. Parents’ experience when their child has chronic abdominal pain: A qualitative study in Norway. BMJ Open 2018, 8, e021066. [Google Scholar] [CrossRef]
- Brodwall, A.; Brekke, M. Children’s and adolescents’ experiences with functional abdominal pain: A qualitative study in Norway. BMJ Open 2021, 11, e048949. [Google Scholar] [CrossRef] [PubMed]
- den Braber, P.; van Driel, J.; Broekhuijsen, D.; Wienen, B.; Bekhof, J. Patterns and seasonality in pediatric referrals for functional somatic symptoms. J. Investig. Med. 2022, 70, 1545–1548. [Google Scholar] [CrossRef] [PubMed]
- Lindfors, P.; Axelsson, E.; Engstrand, K.; Storsrud, S.; Jerlstad, P.; Tornblom, H.; Ljotsson, B.; Simren, M.; Ringstrom, G. Online Education Is Non-Inferior to Group Education for Irritable Bowel Syndrome: A Randomized Trial and Patient Preference Trial. Clin. Gastroenterol. Hepatol. 2020, 19, 743–751.e1. [Google Scholar] [CrossRef] [PubMed]
- Borkovec, T.D.; Nau, S.D. Credibility of analogue therapy rationales. J. Behav. Ther. Exp. Psychiatry 1972, 3, 257–260. [Google Scholar] [CrossRef]
- Ringstrom, G.; Storsrud, S.; Lundqvist, S.; Westman, B.; Simren, M. Development of an educational intervention for patients with Irritable Bowel Syndrome (IBS): A pilot study. BMC Gastroenterol. 2009, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL 4.0: Reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Lane, M.M.; Burwinkle, T.M.; Fontaine, E.N.; Youssef, N.N.; Schwimmer, J.B.; Pardee, P.E.; Pohl, J.F.; Easley, D.J. Health-related quality of life in pediatric patients with irritable bowel syndrome: A comparative analysis. J. Dev. Behav. Pediatr. 2006, 27, 451–458. [Google Scholar] [CrossRef]
- Walker, L.S.; Beck, J.E.; Garber, J.; Lambert, W. Children’s Somatization Inventory: Psychometric properties of the revised form (CSI-24). J. Pediatr. Psychol. 2009, 34, 430–440. [Google Scholar] [CrossRef]
- Reme, S.E.; Darnley, S.; Kennedy, T.; Chalder, T. The development of the irritable bowel syndrome-behavioral responses questionnaire. J. Psychosom. Res. 2010, 69, 319–325. [Google Scholar] [CrossRef]
- Hicks, C.L.; von Baeyer, C.L.; Spafford, P.A.; van Korlaar, I.; Goodenough, B. The Faces Pain Scale-Revised: Toward a common metric in pediatric pain measurement. Pain 2001, 93, 173–183. [Google Scholar] [CrossRef]
- Ahlen, J.; Ghaderi, A. Evaluation of the Children’s Depression Inventory-Short Version (CDI-S). Psychol. Assess. 2017, 29, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Ahlen, J.; Vigerland, S.; Ghaderi, A. Development of the Spence Children’s Anxiety Scale—Short Version (SCAS-S). J. Psychopathol. Behav. Assess. 2018, 40, 288–304. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Included (n = 23) | Not Included (n = 15) | p a | |
|---|---|---|---|
| Children | |||
| Age in years, M (SD); range | 11.9 (±2.5); 9–17 | 12.9 (±2.8); 9–18 | 0.346 |
| Girl, n (%) | 14 (61) | 9 (60) | 0.959 |
| Ethnicity, n (%) | |||
| Born in Sweden | 22 (96) | ||
| At least one parent born outside Sweden | 6 (26) | ||
| Duration of abdominal problems in years, M (SD); range | 6.5 (3.5); 1–14 | ||
| Diagnosis, n (%) | |||
| IBS b | 12 (52) | ||
| FD c | 6 (26) | ||
| FAP-nos d | 5 (22) | ||
| Referring care unit, n (%) | |||
| Secondary care | 22 (96) | ||
| Tertiary care | 1 (4) | ||
| At least one parent with abdominal problems, n (%) | 7 (30) | ||
| Medications for abdominal symptoms e, n (%) | 15 (65) | ||
| Depression CDI-S ≥ 3 f, n (%) | 11 (48) | ||
| Parents (n = 23) | |||
| Education, n (%) g | |||
| High school < 3 years | 0 | ||
| High school ≥ 3 years | 7 (30) | ||
| University ≥ 3 years | 16 (70) |
| Pre M, (SD) | Post M, (SD) | Pre vs. Post | 6 m Follow-Up, M, (SD) | Pre vs. 6 m Follow-Up | |||
|---|---|---|---|---|---|---|---|
| n = 23 | n = 14 | p a | d b [95% CI] | n = 15 | p a | d b [95% CI] | |
| C-scale c | 29.00 (9.8) | ||||||
| PedsQL Gastro d | 63.9 (18.6) | 71.7 (13.9) | 0.003 * | −0.69 [−1.14, −0.23] | 72.2 (16.5) | 0.009 * | −0.60 [−1.03, −0.15] |
| PedsQL QOL e | 72.9 (14.8) | 76.2 (13.5) | 0.008 * | −0.61 [−1.06, −0.16] | 79.1 (14.9) | 0.029 * | −0.49 [−0.92, −0.05] |
| BRQ-C f | 37.1 (15.3) | 34.4 (15.2) | 0.045 * | 0.44 [0.01, 0.87] | 31.1 (12.7) | 0.037 * | 0.46 [0.03, 0.89] |
| CSI gastro g | 11.8 (5.5) | 10.0 (4.8) | 0.007 * | 0.63 [0.17, 1.07] | 8.9 (5.3) | 0.007 * | 0.62 [0.17, 1.06] |
| Self-reported knowledge h | 2.2 (2.2) | 5.6 (3.0) | <0.001 * | −1.12 [−1.63, −0.58] | |||
| Self-reported satisfaction h | 2.7 (2.5) | 5.8 (2.8) | <0.001 * | −0.84 [−1.31, −0.35] | |||
| Faces intensity i | 5.1 (2.5) | 4.9 (2.9) | 0.418 | 5.1 (2.8) | 1.0 | ||
| Pain frequency j | 3.2 (2.0) | 2.5 (2.0) | 0.096 | 2.5 (1.8) | 0.041 * | 0.45 [0.02, 0.88] | |
| Pain-free days k | 2.5 (2.3) | 3.1 (2.5) | 0.144 | 3.4 (2.5) | 0.063 | ||
| CDI-S l | 3.3 (3.6) | 3.1 (4.0) | 0.610 | 3.5 (4.2) | 0.650 | ||
| SCAS-S m | 15.6 (9.7) | 14.4 (9.1) | 0.130 | 14.1 (7.9) | 0.353 | ||
| Post vs. 6 m follow-up | |||||||
| School absence n | 1.2 (1.2) | 1.2 (1.3) | 0.805 | ||||
| School leaving o | 0.7 (0.8) | 0.8 (1.0) | 0.773 | ||||
| Medication, abdominal symptoms p | 1.2 (1.3) | 1.1 (1.2) | 0.668 | ||||
| SAQ q | 3.5 (1.0) | 4.1 (1.4) | |||||
| Pre M, (SD) | Post M, (SD) | Pre vs. Post | 6 m Follow-Up, M, (SD) | Pre vs. 6 m Follow-Up | |||
|---|---|---|---|---|---|---|---|
| n = 23 | n = 15 | p a | d b [95% CI] | n = 18 | p a | d b [95% CI] | |
| Parent on child’s symptoms | |||||||
| C-scale c | 29.0 (8.5) | ||||||
| Parents PedsQL Gastro d | 56.2 (16.9) | 63.2 (15.8) | 0.002 * | −0.73 [−1.19, −0.27] | 69.8 (15.8) | <0.001 * | −0.90 [−1.38, −0.40] |
| Parents PedsQL QOL e | 71.1 (18.0) | 74.3 (18.8) | 0.078 | 82.2 (12.4) | 0.012 * | −0.57 [−1.01, −0.12] | |
| CSI gastro f | 10.6 (5.9) | 8.8 (5.2) | 0.027 * | 0.49 [0.05, 0.92] | 6.5 (4.7) | <0.001 * | 0.86 [0.37, 1.33] |
| GSRS g | 27.3 (18.7) | 28.1 (19.0) | 0.508 | 27.4 (14.8) | 0.987 | ||
| SCAS-P h | 25.0 (21.7) | 23.0 (22.4) | 0.151 | 18.3 (13.3) | 0.104 | ||
| Parent’s self-assessment n = 16 | |||||||
| Parent’s own self-reported knowledge i | 3.0 (2.4) | 5.9 (2.7) | <0.001 * | −1.03 [−1.53, −0.51] | |||
| Parent’s own self-reported satisfaction i | 2.7 (2.4) | 6.2 (2.8) | <0.001 * | −1.01 [−1.51, −0.50] | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Löfgren, E.; Lindfors, P.; Nilsson, K.; Wannstedt, J.; Bonnert, M.; Uusijärvi, A. Gastrointestinal Group Education for Children and Adolescents with Functional Abdominal Pain Disorders—A Feasibility Study of a Brief Intervention. Gastrointest. Disord. 2024, 6, 1-12. https://doi.org/10.3390/gidisord6010001
Löfgren E, Lindfors P, Nilsson K, Wannstedt J, Bonnert M, Uusijärvi A. Gastrointestinal Group Education for Children and Adolescents with Functional Abdominal Pain Disorders—A Feasibility Study of a Brief Intervention. Gastrointestinal Disorders. 2024; 6(1):1-12. https://doi.org/10.3390/gidisord6010001
Chicago/Turabian StyleLöfgren, Emilia, Perjohan Lindfors, Karin Nilsson, Jenny Wannstedt, Marianne Bonnert, and Agneta Uusijärvi. 2024. "Gastrointestinal Group Education for Children and Adolescents with Functional Abdominal Pain Disorders—A Feasibility Study of a Brief Intervention" Gastrointestinal Disorders 6, no. 1: 1-12. https://doi.org/10.3390/gidisord6010001
APA StyleLöfgren, E., Lindfors, P., Nilsson, K., Wannstedt, J., Bonnert, M., & Uusijärvi, A. (2024). Gastrointestinal Group Education for Children and Adolescents with Functional Abdominal Pain Disorders—A Feasibility Study of a Brief Intervention. Gastrointestinal Disorders, 6(1), 1-12. https://doi.org/10.3390/gidisord6010001