Abstract
Crohn’s disease is a chronic inflammatory disease affecting the gastrointestinal tract. Expert guidelines now recommend regular objective assessments as part of a treat-to-target approach. Intestinal ultrasound provides a noninvasive, patient-friendly modality for assessing Crohn’s disease without the risk of radiation exposure and does not require fasting or bowel preparation. Enhancement techniques, including oral and intravenous contrast, can improve disease-activity and complication detection. Due to its acceptability, intestinal ultrasound can be performed frequently, allowing for closer disease-activity monitoring and treatment adjustments. There have been significant advances in the utility of intestinal ultrasound; particularly for assessing disease activity during pregnancy and fibrosis detection utilising elastography. This review provides a comprehensive overview of performing intestinal ultrasound, the diagnostic accuracy, role in disease-activity monitoring, and recent advances in utilising ultrasound for the assessment of luminal Crohn’s disease.
1. Introduction
Crohn’s disease (CD) is a chronic autoimmune disease with increasing worldwide prevalence [1]. Small bowel involvement, either in isolation or with colonic disease, occurs in approximately 90% of patients with typical findings including ulceration, inflammation, and strictures [2]. The current gold standard for CD activity assessment is ileocolonoscopy, however, resource constraints and the invasive nature of this assessment make this difficult to perform frequently. The recent selecting therapeutic targets in inflammatory bowel disease two (STRIDE-2) guidelines have highlighted the increasing importance of using noninvasive modalities to evaluate CD activity. Several imaging techniques can accurately assess the small bowel, including computed tomography, magnetic resonance imaging, and ultrasound [3,4]. Cross-sectional imaging modalities such as magnetic resonance enterography (MRE) and computed tomography enterography (CTE), however, carry patient risks including exposure to ionising radiation (for CT assessment) and intravenous contrast [3].
Intestinal ultrasound (IUS) is an increasingly accepted imaging modality for the assessment of colonic and small bowel CD [3,5]. IUS retains significant advantages over both MRE and CT due to the lack of ionising radiation exposure, not requiring oral or intravenous contrast administration, a lack of fasting requirements, and a shortened image acquisition duration [6]. Additionally, the lack of sedation or complex machinery allows for active engagement with the patient at the time of IUS performance and patients have reported improved disease and symptom understanding as well as greater confidence in making informed decision to managing their disease [7,8]. This review article will discuss the accuracy of IUS as a modality in assessing CD activity and complications. Novel areas of use, such as sonoelastography and use in pregnancy settings, will also be discussed and the techniques involved in performing intestinal ultrasound will be explored.
2. Performing Intestinal Ultrasound
2.1. Patient Preparation
A key advantage of intestinal ultrasound is the ability to perform assessment with minimal preparation, making it potentially viable as a bedside assessment tool, therefore allowing for immediate therapeutic changes based upon real-time disease-activity assessment [9,10,11]. As a result of this, patient preparation prior to IUS remains controversial with no established consensus protocol. Fasting for 4 to 6 h before the examination has been proposed to reduce excessive bowel gas and reduce gut motility, which can impede bowel wall assessment, although a clear benefit of routine fasting is yet to be demonstrated [12,13,14,15]. This ease of performance with minimal preparation makes it a highly acceptable method of small bowel imaging.
2.2. General Technique of Ultrasound
IUS scanning requires a systematic approach to ensure that all relevant segments of the bowel are assessed. This approach is often operator dependent and varies according to the clinical scenario. General principles recommend the initial use of a low frequency (3–5 MHz) convex probe to obtain a general crude overview of the bowel, tracking from the sigmoid colon through to the caecum or vice versa. Subsequent examination is performed using a mid-range to high-frequency (>5 MHz) linear probe, which allows a more detailed assessment of bowel wall thickness, doppler vascularity, and other markers of disease activity.
The terminal ileum is typically found in the right iliac fossa and should be traced as far proximally as possible. Proximal segments of the small bowel are difficult to trace, however probing the abdomen in parallel segments cranially and caudally may allow for the detection of more proximal segments of the disease. A recommended IUS technique has been published by the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) [16].
2.3. Enhancement Techniques
Small intestine contrast ultrasound (SICUS) and contrast enhanced ultrasound (CEUS) can be used when assessing for CD complications such as small bowel strictures and for differentiating inflammatory from infective pathology [17,18,19]. SICUS typically involves ingestion of oral macrogol contrast consisting of polyethylene glycol (PEG) (dose ranging from 125 to 800 mL) dissolved in 250 mL of tap water with a median ingestion time of 30 to 45 min prior to image acquisition [20].
CEUS relies on the intravenous administration of contrast typically consisting of phospholipid-stabilised microbubbles filled with sulphur hexafluoride [20]. These microbubbles have characteristic enhancement patterns in patients with active CD and its complications, which can be detected with IUS [21].
3. Findings and Accuracy of IUS in CD Activity Assessment
3.1. Accuracy in Small Bowel CD Activity Assessment
Expert centres generally find intestinal ultrasound to be highly sensitive and specific for the assessment of disease activity in Crohn’s disease. In a large multicentre study, the sensitivity and specificity of IUS in detecting small bowel CD were 92% (95% confidence interval (CI), 84–96%) and 84% (95% CI, 65–94%) compared to a panel-derived reference standard [22]. These results are similar to a previously performed systematic review in which IUS demonstrated a sensitivity and specificity of 80% (95% CI, 72–88%) and 97% (95% CI, 95–98%) for the diagnosis of suspected CD compared to a reference standard including ileocolonoscopy, radiology, and histopathology [23]. Sensitivity improved to 89% (95% CI, 84–94%) for the initial assessment in established patients with CD and improved further for ileal-specific disease to 93% (95% CI, 87–99%) [23].
In relation to determining the extent of small bowel CD, a recent study demonstrated a sensitivity and specificity of 70% (95% CI, 62–78%) and 81% (95% CI 64–91%) with IUS, respectively, which was 10% (95% CI, 1–18%; p = 0·027) lower than the sensitivity of MRE for assessing small bowel extent in CD [22]. Whilst IUS performed well in detecting small bowel CD, MRE may be a better modality for determining the length of small bowel involvement in patients with CD.
Disease activity is assessed through the measurement of sonographic parameters by the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB). The definitions of complication parameters in IUS are summarised in Table 1 and the parameters are outlined in the following sections.

Table 1.
IUS definition of penetrating complications of CD from EFSUMB [24].
3.2. Bowel Wall Thickness
Bowel wall thickness (BWT) is the most commonly utilised parameter to assess disease activity with IUS [24]. It is measured as the distance from the interface between the serosa and muscle proper to the interface between the mucosa and lumen layer [16]. A BWT value > 3 mm has shown a sensitivity and specificity of 89% and 96%, respectively in detecting active luminal CD when referenced against ileocolonoscopy or histopathology [25]. Higher BWT measurements ≥ 4 mm have demonstrated a similar accuracy to >3 mm with a sensitivity of 87% and a specificity of 98% so either of these cut-offs are considered to represent active disease [25]. In addition, BWT has been shown to have good intraobserver concordance (κ = 0.81 [0.69, 0.93]) [26]. Disruption of bowel wall stratification often occurs in conjunction with increased BWT. Disruption of bowel wall stratification is often associated with bowel inflammation and has been associated with an increased need for future surgical resection [27,28].
3.3. Doppler Vascularity
Colour doppler signal (CDS) of the bowel wall is estimated and graded as part of routine IUS assessment. In a normal bowel wall, doppler signal is absent, however in the presence of inflammation, CDS has been shown to increase. A good correlation between CDS and mucosal has been previously determined. Whilst multiple CD specific IUS indices incorporating CDS have been developed (see later section), the Limberg score is still the most widely performed CDS in IUS (Table 2).
Table 2.
Limberg score.
3.4. Inflammatory Mesenteric Fat and Lymphadenopathy
Mesenteric fat and associated regional lymphadenopathy (≥1 cm) can be seen around segments of inflamed bowel with IUS as increased hyperechogenicity. The presence of both inflammatory mesenteric fat and regional lymphadenopathy is often associated with other abnormal parameters in IUS and can be associated with a peri-intestinal inflammatory process and be representative of active CD [24,29]. Novel IUS indices of activity, including the recent IBUS-SAS (see Table 3) have recognised the importance of inflammatory mesenteric fat changes and incorporated their presence into activity-assessment scoring [30].
Table 3.
IUS indices of activity in CD.
3.5. Peristalsis
Peristalsis of small bowel loops is a normal finding with the absence of peristalsis being a key differentiating feature between the small and large bowel. The absence or a reduction of small bowel peristalsis is often an adjunct finding to small bowel thickening and inflammation [39].
3.6. Strictures
In a systematic review of imaging assessment of small intestine strictures, IUS showed sensitivity and specificity ranging between 80–100% and 63–75%, respectively, in detecting strictures compared to surgical histopathological resection specimens [40]. SICUS had an improved performance with sensitivity and specificity ranges 88–98% and 88–100% [40]. MRE performed better than IUS at small bowel stricture detection with sensitivity and specificity ranges of 75–100% and 91–96% [40]. In a recent head-to-head study, SICUS demonstrated a near perfect agreement (κ = 0.85) with MRE in detecting stricture number and location using a surgical resection specimen as the reference standard [41]. This highlights the potential capacity of enhanced techniques in bridging the gap between IUS and conventional cross-sectional small-bowel imaging in detecting tructuring CD.
Differentiating between fibrotic and inflammatory strictures is difficult with IUS. A systematic review and meta-analysis demonstrated that IUS including CEUS is inadequate at differentiating between fibrotic and inflammatory strictures [42].
3.7. Enteric Fistula and Abscess Detection
IUS can be used to identify both enteric fistula and abscesses. In a systematic review where IUS was performed prior to surgery, the pooled sensitivity and specificity of IUS in detection of enteric fistula was 74% (95% CI, 67–79%) and 95% (95% CI, 91–97%), respectively [43]. Abscess detection with IUS had a sensitivity of 84% (95% CI, 79–88%) and a specificity of 93% (95% CI, 89–95%) compared to surgery. Both fistula and abscess detection sensitivity with IUS was similar to that of MRE [43].
Contrast enhancement during IUS may further improve the identification of internal fistulae and abscesses in patients with CD. In a study of 67 patients with CD, the sensitivity of SICUS for detecting fistulae was 88% and 100% for identifying abscesses compared to surgical resection [41]. The concordance between SICUS and MRE was substantial for fistula detection (κ = 0.65) [41]. CEUS is particularly useful in differentiating between an abscess and an inflammatory mass. When performing CEUS, inflammatory masses show intralesional enhancement, while abscess enhancement is limited to the wall [21]. In a retrospective study of 71 patients with an intraabdominal mass, the differentiation between phlegmon and abscess with CEUS was comparable to cross-sectional imaging or surgical and percutaneous drainage (κ = 0.972) [18]. The overall sensitivity, specificity, and accuracy of CEUS for the diagnosis of abscess vs. phlegmon were 97%, 100%, and 98% [18]. In clinical scenarios whereby cross-sectional imaging is contraindicated, CEUS represents an attractive alternate to the detection and differentiation of intraabdominal masses related to CD. Illustrated examples of abnormal IUS parameters are shown in Figure 1.
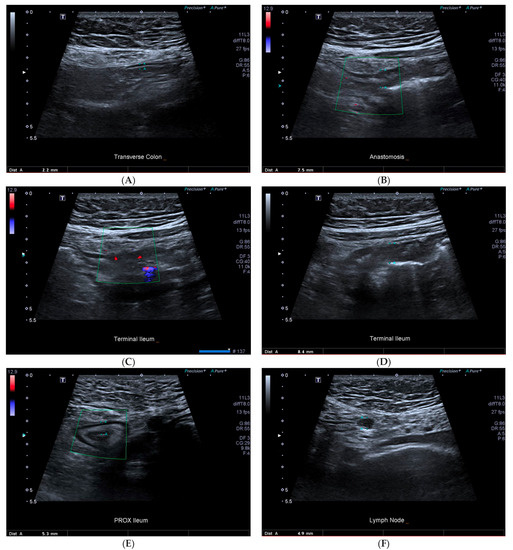
Figure 1.
43-year-old female with prior ileocolonic resection with CD recurrence at the anastomosis and neoterminal ileum. (A) normal transverse colon, (B) anastomotic recurrence with increased bowel wall thickening, (C) terminal ileum showing Limberg three colour doppler signal, (D) terminal ileum wall thickening, (E) proximal small bowel wall thickening, (F) normal sized lymph node.
4. IUS Indices
Multiple IUS indices of CD activity assessment have been developed primarily for standardisation of assessments when used for clinical trials [44,45]. A summary of the developed IUS indices is provided in Table 3. The original IUS CD activity index developed by Limberg et al. used a composite of BWT and CDS. In a retrospective study of 32 patients, the Limberg score was correlated against a reference standard of ileal histology and was determined to have a significant (p < 0.05) association with active disease (κ = 0.66; sensitivity 95%; specificity 69%) [36]. In a subsequent retrospective analysis of 108 patients a good correlation between the simplified endoscopic score (SES)-CD and the IUS-based Limberg score was observed (Þ = 0.709, p < 0.001) [35]. Furthermore, in 22 patients a significant (p = 0.005) difference between active and nonactive surgical histopathological resection specimens and the Limberg score was observed [35].
Subsequent IUS indices have been developed primarily utilising BWT and CDS as the assessed parameters with few including other sonographic parameters such as bowel wall stratification, inflammatory fat, and the presence of lymph nodes [31,34,38]. More recently, an expert consensus group from the International Bowel Ultrasound Group (IBUS) developed the IBUS-segmental activity score (IBUS-SAS) [30]. This novel IUS activity index utilises a composite BWT, inflammatory fat, CDS, and bowel wall stratification with a multicentre international validation study in progress.
A key limitation of the current scores is the lack of external validation as well as significant concerns relating to the external validity of the parameters used. Expert consensus statements pertaining to the use IUS scoring in luminal CD have been published [46]. Of the currently developed IUS indices assessed, none were found to be appropriate for use in luminal CD. BWT increased bowel wall vascularity, loss of bowel wall stratification, and mesenteric inflammatory fat were identified as ideal components of future IUS CD activity indices [46]. In the future, IUS activity indices could represent a logical way in standardising reporting. Further studies are still needed to validate current IUS activity assessment scores in CD and determine its accuracy outside of trial settings.
5. Response to Therapy and Monitoring
Whilst endoscopic assessment for mucosal healing (MH) remains the gold standard in disease-activity assessment for Crohn’s disease, IUS has also demonstrated efficacy in assessing response to therapy [47]. A key limitation in studies grading IUS response parameters is the heterogeneity of defining sonographic responses to treatment [48]. More recently, an expert consensus statement defined a sonographic response in CD as a reduction of BWT >25% of baseline or >2 mm or >1.0 mm and one CDS reduction [48].
The correlation between IUS disease-activity response and other measures of disease activity was evaluated in a cohort of 234 patients with active CD receiving therapies, including steroids, immunomodulators, and biological agents [49]. At 3 and 12 months, all assessed IUS parameters including BWT, fibrofatty proliferation and CDS showed significant reductions following the initiation of therapy (p < 0.01 for all parameters at months 3 and 12). The improvement in BWT correlated with the normalisation of the C-reactive protein after 3 months (p < 0.001) [49], and a reduction in the Harvey Bradshaw index (HBI) also correlated with the reduction in BWT [49]. Sonographic response may also assist in the early detection of response to therapy and therefore allow changes in treatment earlier in the course of therapy. In a study of 52 patients with CD initiating antitumour necrosis factor (TNF) therapy, early sonographic response after 12 weeks of therapy was more likely to result in sonographic improvement at 52 weeks compared to individuals who did not achieve a week 12 response (85% vs. 28%; p < 0.0001). The lack of sonographic improvement at 52 weeks was more likely to result in change or dose escalation in therapy or surgical requirement (65% vs. 11%) [50].
Another potential advantage of IUS over ileocolonoscopy is the ability to assess for transmural healing (TH) in CD assessment. In a study of 133 patients with CD, TH assessed with IUS and MH assessed through endoscopy (SES-CD) showed a good correlation (κ = 0.63; p < 0.001) [51]. More patients achieved MH compared with TH, though this was not statistically significant (38% vs. 25%) [51]. The achievement of TH may be particularly relevant as a treatment target as it has been shown to independently predict steroid-free clinical remission (odds ratio (OR), 52.6; p < 0.001), drug escalation (OR, 0.1; p = 0.002), and hospitalisation (OR, 0.05; p = 0.005) in patients with CD [52].
CEUS and SICUS are useful modalities to assess CD response [53,54] to therapy. In a study of 30 patients with active CD on therapy, CEUS had a good correlation with endoscopy in demonstrating disease remission (κ = 0.73, p < 0.001) [54]. In a recent study of patients with CD receiving anti-TNF therapy, the CEUS parameters response was higher in those with clinical and endoscopic responses compared to nonresponders [55]. Moreover, the response to therapy detected with SICUS has been associated with better long-term outcomes, including reduced need for surgery and corticosteroid use [53]. With STRIDE-2 guidelines now recommending more frequent CD activity assessment, IUS presents a feasible alternative to alternative modalities such as MRE and ileocolonoscopy. Furthermore, there is emerging evidence that TH through IUS assessment may be a better treatment target than MH though long-term follow-up studies in this setting are needed [56]. Both SICUS and CEUS have a significant capacity in monitoring response to therapy in CD though further studies are needed.
6. Postoperative Recurrence
Whilst ileocolonoscopy remains the gold standard of assessment in postoperative CD, IUS is an appealing noninvasive surrogate modality allowing for close follow-up [3]. The thickness of the bowel wall at the anastomosis has been demonstrated to correlate closely to degree of endoscopic recurrence (based on the Rutgeerts score) [57,58]. In a prospective cohort of 45 patients one year after ileocolonic resection, a BWT > 3 mm showed a sensitivity and specificity of 79% and 95%, respectively, for mild endoscopic recurrence of CD (Rutgeerts i1-2) [59]. A receiver operative curve (ROC) analysis, BWT > 5 mm showed sensitivity and specificity of 94% and 100%, respectively, in discriminating severe endoscopic recurrence (Rutgeerts i3-4) with an excellent agreement with endoscopy (κ = 0.90) [59]. A subsequent meta-analysis demonstrated a pooled sensitivity and specificity of 94% (95% CI, 86–97%) and 84% (95% CI, 62–94%; diagnostic accuracy 90%) in determining postoperative CD recurrence compared with ileocolonoscopy [60]. An anastomosis BWT of >5.5 mm demonstrated a sensitivity of 84% (95% CI, 74–91%) and a specificity of 98% (95% CI, 93–99%) in predicting severe endoscopic recurrence (Rugeerts i3-4) [60].
The use of intravenous and oral contrast enhanced IUS in postoperative CD has been studied extensively [58,60,61,62,63]. In the largest prospective study of 72 patients, a BWT > 3 mm with SICUS correlated moderately with an endoscopic Rutgeerts’ score (p = 0.0001, r = 0.67) [58]. SICUS showed a sensitivity and specificity of 93% and 20%, respectively, for detecting CD recurrence [58]. In a subsequent, meta-analysis the pooled sensitivity and specificity was 99% (95% CI, 99%–100%) and 74% (95% CI, 73–74%), respectively, for SICUS in demonstrating postoperative CD recurrence [60].
The use of CEUS to improve the detection of postoperative CD has had varying results and may be less important with modern equipment [61,62]. In early studies, CEUS had better sensitivity for detecting endoscopic recurrence than conventional IUS (98% vs. 90%) [62]. However, more recent studies suggest that adding CEUS does not improve the detection of postoperative recurrence compared to standard IUS at 6 months postresection [64]. Furthermore, CEUS showed the same sensitivity (90%) and specificity (87%) as a BWT > 6 mm in detecting severe endoscopic recurrence (Rutgeerts i3-4) [61]. Larger randomised studies are required to determine whether diagnostic accuracy is improved with CEUS compared to standard IUS or SICUS in postoperative CD recurrence.
Despite advances in postoperative CD assessment with IUS, guidelines still recommend endoscopy within 6–12 months of surgery, though with growing centres of expertise, IUS or potentially CEUS could be used as an alternative noninvasive modality of assessment in this setting although further evidence is needed to support this approach [3].
7. Novel Areas of Utility
7.1. Sonoelastography
Sonoelastography is a diagnostic ultrasound technique that measures tissue elasticity and stiffness and may have utility in discriminating fibrosis from inflammation. Strain and shear-wave elastography (SWE) have been studied in fibrosis detection for IUS [65]. Strain elastography requires repeated probe pressure on the abdominal wall to determine a strain ratio. SWE mitigates the need for repeated probe pressure and measures tissue elasticity in kilopascals (kPa).
In a pilot study of 23 patients with CD, strain elastography, measured as a strain ratio had an excellent discriminatory ability for severe bowel fibrosis (AuROC: 0.917; 95% CI interval, 0.79–1.00) compared to a surgical resection as the reference standard with higher strain ratios seen in more severe grades of fibrosis [66]. SWE performance was determined in a cohort of 35 patients undergoing surgical resection, with higher SWE values seen in severe grades of fibrosis [67]. Using 22.55 KPa as a cut-off level, SWE had an excellent capacity in discriminating between mild or moderate and severe fibrosis (AuROC: 0.81 p = 0.002, sensitivity 70%, specificity 92%) compared to a surgical resection sample as the reference standard [67]. In this study, SWE was unable to differentiate between grades of inflammatory strictures, potentially limiting its use to fibrotic disease only [67].
In a recent meta-analysis inclusive of six studies, SWE and strain elastography were demonstrated to be potentially useful markers in CD-related fibrosis detection [65]. The pooled standardised mean strain ratio was significantly higher in bowel segments with fibrotic strictures than in those without fibrotic strictures with a standardised mean difference of 0.85 (95% CI, 0–1.71; p = 0.05) [65]. The pooled standardised mean strain value was higher in bowel segments with fibrotic strictures than in those without fibrotic strictures, but did not reach statistical significance with a mean difference of 1.0 (95% CI, −0.11–2.10; p = 0.08) [65]. The meta-analysis had significant weaknesses due to the limited patient numbers and high heterogeneity between the performed studies. Sonoelastography is clearly an emerging imaging sonographic tool in determining bowel fibrosis, but further studies are needed to determine its true capacity in this setting.
7.2. Pregnancy
The sonographic evaluation of CD in pregnancy has received growing attention [68,69,70]. Compared to alternative assessment modalities such as MRE and endoscopy, IUS has advantages such as the lack of intravenous contrast or procedural risks associated with endoscopy. IUS has demonstrated a moderate to strong correlation with clinical activity (r = 0.60, p < 0.0001) in pregnant patients with IBD though feasibility appears to be reduced from the third trimester onwards (first vs. third trimester: 91% vs. 22%, p < 0.0001) [68]. Adequate ileal assessment has been seen in as low as 59% of pregnant patients with IBD beyond 20 weeks’ gestation compared to 91% prior to week 20 [69]. In the largest study of IUS in pregnant patients with IBD, Flanagan et al. demonstrated a weak positive correlation between bowel wall thickness and calprotectin (r = 0.26, p = 0.03) [69]. The overall accuracy of IUS in pregnant women with IBD showed a specificity of 83%, sensitivity of 74%, and a negative predictive value of 90% compared to faecal calprotectin [69]. Significant challenges of IUS validation in pregnant CD patients will continue to remain due to the inability to correlate sonographic findings with the gold standard of ileocolonoscopy in the pregnant IBD cohort. Further studies are required to determine the accuracy of IUS in pregnant patients with CD.
8. Limitations of IUS
Sonographic assessment of CD is subject to a number of patient and procedural limitations that can impact activity assessment. Assessment of the small bowel is largely limited to the terminal ileum with the length of disease as well as segments of the mid and proximal small bowel better assessed with MRE [22]. Accurate rectal assessment can also be challenging given its position posterior to the bladder when performing transabdominal IUS [71]. Patient-related limitations can be seen in obese patients where assessment with the high-frequency linear probe is limited due to its inability to penetrate to deeper bowel segments [71]. This could potentially be overcome through the use of a lower-frequency convex probe at the sacrifice of image quality.
9. Conclusions
IUS has advantages in the assessment of CD compared to other modalities such as MRE, CTE, and ileocolonoscopy. Furthermore, IUS has been established to accurately assess small bowel disease activity with several meta-analyses now demonstrating the accuracy of IUS in this setting. Additionally, use in the assessment of pregnant patients with CD, in whom radiologic assessment is limited to noncontrast MRE. Whilst, many have been developed, few have been validated, thus limiting their role to research settings. With an increasing number of IUS being performed worldwide, IUS is likely to continue to increase in use in CD and thus standardisation of reporting using IUS activity indices should be a focus in future studies.
Author Contributions
Writing and editing, A.B.; supervision, D.R.V.L.; Writing, editing, and supervision, A.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Chouraki, V.; Savoye, G.; Dauchet, L.; Vernier-Massouille, G.; Dupas, J.-L.; Merle, V.; Laberenne, J.-E.; Salomez, J.-L.; Lerebours, E.; Turck, D.; et al. The changing pattern of Crohn’s disease incidence in northern France: A continuing increase in the 10- to 19-year-old age bracket (1988–2007). Aliment. Pharmacol. Ther. 2011, 33, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohn’s Colitis 2018, 13, 144–164K. [Google Scholar] [CrossRef]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.V.; Friedman, A.B.; Wright, E.K.; Taylor, K.M.; Begun, J.; Maconi, G.; Maaser, C.; Novak, K.L.; Kucharzik, T.; Atkinson, N.S.S.; et al. Gastrointestinal ultrasound in inflammatory bowel disease: An underused resource with potential paradigm-changing application. Gut 2018, 67, 973–985. [Google Scholar] [CrossRef] [PubMed]
- Hata, J.; Imamura, H. The Use of Transabdominal Ultrasound in Inflammatory Bowel Disease. Korean J. Radiol. 2022, 23, 308–321. [Google Scholar] [CrossRef]
- Rajagopalan, A.; Sathananthan, D.; An, Y.; Van De Ven, L.; Martin, S.; Fon, J.; Costello, S.P.; Begun, J.; Bryant, R.V. Gastrointestinal ultrasound in inflammatory bowel disease care: Patient perceptions and impact on disease-related knowledge. JGH Open 2019, 4, 267–272. [Google Scholar] [CrossRef]
- Friedman, A.B.; Asthana, A.; Knowles, S.R.; Robbins, A.; Gibson, P.R. Effect of point-of-care gastrointestinal ultrasound on decision-making and management in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2021, 54, 652–666. [Google Scholar] [CrossRef]
- Novak, K.; Tanyingoh, D.; Petersen, F.; Kucharzik, T.; Panaccione, R.; Ghosh, S.; Kaplan, G.G.; Wilson, A.; Kannengiesser, K.; Maaser, C. Clinic-based Point of Care Transabdominal Ultrasound for Monitoring Crohn’s Disease: Impact on Clinical Decision Making. J. Crohn’s Colitis 2015, 9, 795–801. [Google Scholar] [CrossRef]
- Wright, E.K.; Wang, I.; Wong, D.; Bell, S.J.; Connell, W.R.; Thompson, A.J.; Novak, K.L.; Kamm, M.A. Accuracy of point-of-care intestinal ultrasound for Crohn’s disease. Australas. J. Ultrasound Med. 2020, 23, 176–182. [Google Scholar] [CrossRef]
- Bots, S.; De Voogd, F.; De Jong, M.; Ligtvoet, V.; Löwenberg, M.; Duijvestein, M.; Ponsioen, C.Y.; D’Haens, G.; Gecse, K.B. Point-of-care Intestinal Ultrasound in IBD Patients: Disease Management and Diagnostic Yield in a Real-world Cohort and Proposal of a Point-of-care Algorithm. J. Crohn’s Colitis 2021, 16, 606–615. [Google Scholar] [CrossRef]
- Panes, J.; Bouhnik, Y.; Reinisch, W.; Stoker, J.; Taylor, S.; Baumgart, D.; Danese, S.; Halligan, S.; Marincek, B.; Matos, C.; et al. Imaging techniques for assessment of inflammatory bowel disease: Joint ECCO and ESGAR evidence-based consensus guidelines. J. Crohn’s Colitis 2013, 7, 556–585. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, N.S.S.; Bryant, R.V.; Dong, Y.; Maaser, C.; Kucharzik, T.; Maconi, G.; Asthana, A.K.; Blaivas, M.; Goudie, A.; Gilja, O.H.; et al. How to perform gastrointestinal ultrasound: Anatomy and normal findings. World J. Gastroenterol. 2017, 23, 6931–6941. [Google Scholar] [CrossRef] [PubMed]
- Sinan, T.; Leven, H.; Sheikh, M. Is fasting a necessary preparation for abdominal ultrasound? BMC Med. Imaging 2003, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Ehrenstein, B.P.; Froh, S.; Schlottmann, K.; Schölmerich, J.; Schacherer, D. To eat or not to eat? Effect of fasting prior to abdominal sonography examinations on the quality of imaging under routine conditions: A randomized, examiner-blinded trial. Scand. J. Gastroenterol. 2009, 44, 1048–1054. [Google Scholar] [CrossRef]
- Nylund, K.; Maconi, G.; Hollerweger, A.; Ripolles, T.; Pallotta, N.; Higginson, A.; Serra, C.; Dietrich, C.F.; Sporea, I.; Saftoiu, A.; et al. EFSUMB Recommendations and Guidelines for Gastrointestinal Ultrasound-Part 1: Examination Techniques and Normal Findings (Short version). Ultraschall der Med.-Eur. J. Ultrasound 2016, 38, 273–284. [Google Scholar] [CrossRef]
- Parente, F.; Greco, S.; Molteni, M.; Anderloni, A.; Sampietro, G.M.; Danelli, P.; Bianco, R.; Gallus, S.; Porro, G.B. Oral contrast enhanced bowel ultrasonography in the assessment of small intestine Crohn’s disease. A prospective comparison with conventional ultrasound, x ray studies, and ileocolonoscopy. Gut 2004, 53, 1652–1657. [Google Scholar] [CrossRef]
- Ripollés, T.; Martínez-Pérez, M.J.; Paredes, J.M.; Vizuete, J.; García-Martínez, E.; Jiménez-Restrepo, D.H. Contrast-enhanced ultrasound in the differentiation between phlegmon and abscess in Crohn’s disease and other abdominal conditions. Eur. J. Radiol. 2013, 82, e525–e531. [Google Scholar] [CrossRef]
- Medellin, A.; Merrill, C.; Wilson, S.R. Role of contrast-enhanced ultrasound in evaluation of the bowel. Abdom. Radiol. 2017, 43, 918–933. [Google Scholar] [CrossRef]
- Mocci, G.; Migaleddu, V.; Cabras, F.; Sirigu, D.; Scanu, D.; Virgilio, G.; Marzo, M. SICUS and CEUS imaging in Crohn’s disease: An update. J. Ultrasound 2017, 20, 1–9. [Google Scholar] [CrossRef]
- Ripollés, T.; Martínez-Pérez, M.J.; Blanc, E.; Delgado, F.; Vizuete, J.; Paredes, J.M.; Vilar, J. Contrast-enhanced ultrasound (CEUS) in Crohn’s disease: Technique, image interpretation and clinical applications. Insights Into Imaging 2011, 2, 639–652. [Google Scholar] [CrossRef] [PubMed]
- A Taylor, S.; Mallett, S.; Bhatnagar, G.; Baldwin-Cleland, R.; Bloom, S.; Gupta, A.; Hamlin, P.J.; Hart, A.L.; Higginson, A.; Jacobs, I.; et al. Diagnostic accuracy of magnetic resonance enterography and small bowel ultrasound for the extent and activity of newly diagnosed and relapsed Crohn’s disease (METRIC): A multicentre trial. Lancet Gastroenterol. Hepatol. 2018, 3, 548–558. [Google Scholar] [CrossRef]
- Calabrese, E.; Maaser, C.; Zorzi, F.; Kannengiesser, K.; Hanauer, S.B.; Bruining, D.H.; Iacucci, M.; Maconi, G.; Novak, K.L.; Panaccione, R.; et al. Bowel Ultrasonography in the Management of Crohn’s Disease. A Review with Recommendations of an International Panel of Experts. Inflamm. Bowel Dis. 2016, 22, 1168–1183. [Google Scholar] [CrossRef]
- Maconi, G.; Nylund, K.; Ripolles, T.; Calabrese, E.; Dirks, K.; Dietrich, C.F.; Hollerweger, A.; Sporea, I.; Saftoiu, A.; Maaser, C.; et al. EFSUMB Recommendations and Clinical Guidelines for Intestinal Ultrasound (GIUS) in Inflammatory Bowel Diseases. Ultraschall der Med.-Eur. J. Ultrasound 2018, 39, 304–317. [Google Scholar] [CrossRef]
- Dong, J.; Wang, H.; Zhao, J.; Zhu, W.; Zhang, L.; Gong, J.; Li, Y.; Gu, L.; Li, J. Ultrasound as a diagnostic tool in detecting active Crohn’s disease: A meta-analysis of prospective studies. Eur. Radiol. 2013, 24, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Sævik, F.; Eriksen, R.; Eide, G.E.; Gilja, O.H.; Nylund, K. Development and Validation of a Simple Ultrasound Activity Score for Crohn’s Disease. J. Crohn’s Colitis 2020, 15, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Maconi, G.; Carsana, L.; Fociani, P.; Sampietro, G.M.; Ardizzone, S.; Cristaldi, M.; Parente, F.; Vago, G.L.; Taschieri, A.M.; Porro, G.B. Small bowel stenosis in Crohn’s disease: Clinical, biochemical and ultrasonographic evaluation of histological features. Aliment. Pharmacol. Ther. 2003, 18, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Rigazio, C.; Ercole, E.; Laudi, C.; Daperno, M.; Lavagna, A.; Crocellà, L.; Bertolino, F.; Viganò, L.; Sostegni, R.; Pera, A.; et al. Abdominal bowel ultrasound can predict the risk of surgery in Crohn’s disease: Proposal of an ultrasonographic score. Scand. J. Gastroenterol. 2009, 44, 585–593. [Google Scholar] [CrossRef]
- Maconi, G.; Greco, S.; Duca, P.; Ardizzone, S.; Massari, A.; Cassinotti, A.; Radice, E.; Porro, G.B. Prevalence and clinical significance of sonographic evidence of mesenteric fat alterations in Crohn’s disease. Inflamm. Bowel Dis. 2008, 14, 1555–1561. [Google Scholar] [CrossRef]
- Novak, K.L.; Nylund, K.; Maaser, C.; Petersen, F.; Kucharzik, T.; Lu, C.; Allocca, M.; Maconi, G.; de Voogd, F.; Christensen, B.; et al. Expert Consensus on Optimal Acquisition and Development of the International Bowel Ultrasound Segmental Activity Score [IBUS-SAS]: A Reliability and Inter-rater Variability Study on Intestinal Ultrasonography in Crohn’s Disease. J. Crohn’s Colitis 2020, 15, 609–616. [Google Scholar] [CrossRef]
- Allocca, M.; Craviotto, V.; Dell’Avalle, C.; Furfaro, F.; Zilli, A.; D’Amico, F.; Bonovas, S.; Peyrin-Biroulet, L.; Fiorino, G.; Danese, S. Bowel ultrasound score is accurate in assessing response to therapy in patients with Crohn’s disease. Aliment. Pharmacol. Ther. 2021, 55, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Allocca, M.; Craviotto, V.; Bonovas, S.; Furfaro, F.; Zilli, A.; Peyrin-Biroulet, L.; Fiorino, G.; Danese, S. Predictive Value of Bowel Ultrasound in Crohn’s Disease: A 12-Month Prospective Study. Clin. Gastroenterol. Hepatol. 2021, 20, e723–e740. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Ding, S.-S.; Zhang, K.; Liu, L.-N.; Guo, L.-H.; Sun, L.-P.; Zhang, Y.-F.; Sun, X.-M.; Ren, W.-W.; Zhao, C.-K.; et al. Correlation between ultrasound consolidated score and simple endoscopic score for determining the activity of Crohn’s disease. Br. J. Radiol. 2020, 93, 20190614. [Google Scholar] [CrossRef] [PubMed]
- Novak, K.L.; Kaplan, G.G.; Panaccione, R.; Afshar, E.E.; Tanyingoh, D.; Swain, M.; Kellar, A.; Wilson, S. A Simple Ultrasound Score for the Accurate Detection of Inflammatory Activity in Crohn’s Disease. Inflamm. Bowel Dis. 2017, 23, 2001–2010. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Kunisaki, R.; Kinoshita, H.; Yamamoto, H.; Kimura, H.; Hanzawa, A.; Shibata, N.; Yonezawa, H.; Miyajima, E.; Sakamaki, K.; et al. Use of color Doppler ultrasonography for evaluating vascularity of small intestinal lesions in Crohn’s disease: Correlation with endoscopic and surgical macroscopic findings. Scand. J. Gastroenterol. 2013, 49, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Drews, B.H.; Barth, T.F.E.; Hänle, M.M.; Akinli, A.S.; Mason, R.A.; Muche, R.; Thiel, R.; Pauls, S.; Klaus, J.; Von Boyen, G.; et al. Comparison of sonographically measured bowel wall vascularity, histology, and disease activity in Crohn’s disease. Eur. Radiol. 2009, 19, 1379–1386. [Google Scholar] [CrossRef]
- Pascu, M.; Roznowski, A.B.; Müller, H.-P.; Adler, A.; Wiedenmann, B.; Dignass, A.U. Clinical Relevance of Transabdominal Ultrasonography and Magnetic Resonance Imaging in Patients With Inflammatory Bowel Disease of the Terminal Ileum and Large Bowel. Inflamm. Bowel Dis. 2004, 10, 373–382. [Google Scholar] [CrossRef]
- Neye, H.; Voderholzer, W.; Rickes, S.; Weber, J.; Wermke, W.; Lochs, H. Evaluation of Criteria for the Activity of Crohn’s Disease by Power Doppler Sonography. Dig. Dis. 2004, 22, 67–72. [Google Scholar] [CrossRef]
- Jauregui-Amezaga, A.; Rimola, J. Role of Intestinal Ultrasound in the Management of Patients with Inflammatory Bowel Disease. Life 2021, 11, 603. [Google Scholar] [CrossRef]
- Bettenworth, D.; Bokemeyer, A.; Baker, M.; Mao, R.; Parker, C.E.; Nguyen, T.; Ma, C.; Panés, J.; Rimola, J.; Fletcher, J.G.; et al. Assessment of Crohn’s disease-associated small bowel strictures and fibrosis on cross-sectional imaging: A systematic review. Gut 2019, 68, 1115–1126. [Google Scholar] [CrossRef]
- Kumar, S.; Hakim, A.; Alexakis, C.; Chhaya, V.; Tzias, D.; Pilcher, J.; Vlahos, J.; Pollok, R. Small intestinal contrast ultrasonography for the detection of small bowel complications in Crohn’s disease: Correlation with intraoperative findings and magnetic resonance enterography. J. Gastroenterol. Hepatol. 2014, 30, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Jiang, W.; Wang, L.; Mao, X.; Ye, Z.; Zhang, H. Intestinal Ultrasound for Differentiating Fibrotic or Inflammatory Stenosis in Crohn’s Disease: A Systematic Review and Meta-analysis. J. Crohn’s Colitis 2022, 30, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Panes, J.; Bouzas, R.; Chaparro, M.; García-Sánchez, V.; Gisbert, J.P.; De Guereñu, B.M.; Mendoza, J.L.; Paredes, J.M.; Quiroga, S.; Ripollés, T.; et al. Systematic review: The use of ultrasonography, computed tomography and magnetic resonance imaging for the diagnosis, assessment of activity and abdominal complications of Crohn’s disease. Aliment. Pharmacol. Ther. 2011, 34, 125–145. [Google Scholar] [CrossRef] [PubMed]
- Goodsall, T.M.; Nguyen, T.M.; Parker, C.E.; Ma, C.; Andrews, J.M.; Jairath, V.; Bryant, R.V. Systematic Review: Gastrointestinal Ultrasound Scoring Indices for Inflammatory Bowel Disease. J. Crohn’s Colitis 2020, 15, 125–142. [Google Scholar] [CrossRef] [PubMed]
- Bots, S.; Nylund, K.; Löwenberg, M.; Gecse, K.; Gilja, O.H.; D’Haens, G. Ultrasound for Assessing Disease Activity in IBD Patients: A Systematic Review of Activity Scores. J. Crohn’s Colitis 2018, 12, 920–929. [Google Scholar] [CrossRef]
- Goodsall, T.M.; Jairath, V.; Feagan, B.G.; Parker, C.E.; Nguyen, T.M.; Guizzetti, L.; Asthana, A.K.; Begun, J.; Christensen, B.; Friedman, A.B.; et al. Standardisation of intestinal ultrasound scoring in clinical trials for luminal Crohn’s disease. Aliment. Pharmacol. Ther. 2021, 53, 873–886. [Google Scholar] [CrossRef]
- Calabrese, E.; Rispo, A.; Zorzi, F.; De Cristofaro, E.; Testa, A.; Costantino, G.; Viola, A.; Bezzio, C.; Ricci, C.; Prencipe, S.; et al. Ultrasonography Tight Control and Monitoring in Crohn’s Disease During Different Biological Therapies: A Multicenter Study. Clin. Gastroenterol. Hepatol. 2021, 20, e711–e722. [Google Scholar] [CrossRef]
- Ilvemark, J.F.K.F.; Hansen, T.; Goodsall, T.M.; Seidelin, J.B.; Farhan, H.A.; Allocca, M.; Begun, J.; Bryant, R.V.; Carter, D.; Christensen, B.; et al. Defining Transabdominal Intestinal Ultrasound Treatment Response and Remission in Inflammatory Bowel Disease: Systematic Review and Expert Consensus Statement. J. Crohn’s Colitis 2021, 16, 554–580. [Google Scholar] [CrossRef]
- Kucharzik, T.; Wittig, B.M.; Helwig, U.; Börner, N.; Rössler, A.; Rath, S.; Maaser, C.; Naumann, A.; Pelster, G.; Spengler, J.; et al. Use of Intestinal Ultrasound to Monitor Crohn’s Disease Activity. Clin. Gastroenterol. Hepatol. 2016, 15, 535–542.e2. [Google Scholar] [CrossRef]
- Ripollés, T.; Paredes, J.M.; Martínez-Pérez, M.J.; Rimola, J.; Jauregui-Amezaga, A.; Bouzas, R.; Martin, G.; Moreno-Osset, E. Ultrasonographic Changes at 12 Weeks of Anti-TNF Drugs Predict 1-year Sonographic Response and Clinical Outcome in Crohn’s Disease. Inflamm. Bowel Dis. 2016, 22, 2465–2473. [Google Scholar] [CrossRef]
- Castiglione, F.; Testa, A.; Rea, M.; De Palma, G.D.; Diaferia, M.; Musto, D.; Sasso, F.; Caporaso, N.; Rispo, A. Transmural Healing Evaluated by Bowel Sonography in Patients with Crohn’s Disease on Maintenance Treatment with Biologics. Inflamm. Bowel Dis. 2013, 19, 1928–1934. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Li, W.; Zhuang, N.; Yang, H.; Liu, W.; Zhou, W.; Jiang, Y.; Li, J.; Zhu, Q.; Qian, J. Comparison of transmural healing and mucosal healing as predictors of positive long-term outcomes in Crohn’s disease. Ther. Adv. Gastroenterol. 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Zorzi, F.; Ghosh, S.; Chiaramonte, C.; Lolli, E.; Ventura, M.; Onali, S.; De Cristofaro, E.; Fantini, M.C.; Biancone, L.; Monteleone, G.; et al. Response Assessed by Ultrasonography as Target of Biological Treatment for Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2020, 18, 2030–2037. [Google Scholar] [CrossRef] [PubMed]
- Moreno, N.; Ripollés, T.; Paredes, J.M.; Ortiz, I.; Martínez, M.J.; López, A.; Delgado, F.; Moreno-Osset, E. Usefulness of abdominal ultrasonography in the analysis of endoscopic activity in patients with Crohn’s disease: Changes following treatment with immunomodulators and/or anti-TNF antibodies. J. Crohn’s Colitis 2014, 8, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Laterza, L.; Ainora, M.E.; Garcovich, M.; Galasso, L.; Poscia, A.; Di Stasio, E.; Lupascu, A.; Riccardi, L.; Scaldaferri, F.; Armuzzi, A.; et al. Bowel contrast-enhanced ultrasound perfusion imaging in the evaluation of Crohn’s disease patients undergoing anti-TNFα therapy. Dig. Liver Dis. 2020, 53, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, R.; Tjandra, D.; Patwardhan, A.; Mingos, N.; Gibson, R.; Boussioutas, A.; Ardalan, Z.; Al-Ani, A.; Gibson, P.R.; Christensen, B. Toward transmural healing: Sonographic healing is associated with improved long-term outcomes in patients with Crohn’s disease. Aliment. Pharmacol. Ther. 2022, 56, 84–94. [Google Scholar] [CrossRef]
- Macedo, C.P.; Costa, M.S.; Gravito-Soares, E.; Gravito-Soares, M.; Ferreira, A.M.; Portela, F.; Figueiredo, P. Role of Intestinal Ultrasound in the Evaluation of Postsurgical Recurrence in Crohn’s Disease: Correlation with Endoscopic Findings. GE-Port. J. Gastroenterol. 2021, 29, 178–186. [Google Scholar] [CrossRef]
- Calabrese, E.; Petruzziello, C.; Onali, S.; Condino, G.; Zorzi, F.; Pallone, F.; Biancone, L. Severity of postoperative recurrence in Crohn’s disease: Correlation between endoscopic and sonographic findings. Inflamm. Bowel Dis. 2009, 15, 1635–1642. [Google Scholar] [CrossRef]
- Rispo, A.; Bucci, L.; Pesce, G.; Sabbatini, F.; De Palma, G.D.; Grassia, R.; Compagna, A.; Testa, A.; Castiglione, F. Bowel sonography for the diagnosis and grading of postsurgical recurrence of Crohn’s disease. Inflamm. Bowel Dis. 2006, 12, 486–490. [Google Scholar] [CrossRef]
- Rispo, A.; Imperatore, N.; Testa, A.; Nardone, O.M.; Luglio, G.; Caporaso, N.; Castiglione, F. Diagnostic Accuracy of Ultrasonography in the Detection of Postsurgical Recurrence in Crohn’s Disease: A Systematic Review with Meta-analysis. Inflamm. Bowel Dis. 2018, 24, 977–988. [Google Scholar] [CrossRef]
- Martínez, M.J.; Ripollés, T.; Paredes, J.M.; Moreno-Osset, E.; Pazos, J.M.; Blanc, E. Intravenous Contrast-Enhanced Ultrasound for Assessing and Grading Postoperative Recurrence of Crohn’s Disease. Am. J. Dig. Dis. 2019, 64, 1640–1650. [Google Scholar] [CrossRef] [PubMed]
- Paredes, J.M.; Ripollés, T.; Cortés, X.; Moreno, N.; Martínez, M.J.; Bustamante-Balén, M.; Delgado, F.; Moreno-Osset, E. Contrast-enhanced ultrasonography: Usefulness in the assessment of postoperative recurrence of Crohn’s disease. J. Crohn’s Colitis 2013, 7, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Castiglione, F.; Bucci, L.; Pesce, G.; De Palma, G.D.; Camera, L.; Cipolletta, F.; Testa, A.; Diaferia, M.; Rispo, A. Oral contrast-enhanced sonography for the diagnosis and grading of postsurgical recurrence of Crohn’s disease. Inflamm. Bowel Dis. 2008, 14, 1240–1245. [Google Scholar] [CrossRef] [PubMed]
- Herraiz Hidalgo, L.; Alvarez Moreno, E.; Carrascoso Arranz, J.; Cano Alonso, R.; de Vega Fernández, V.M. Magnetic resonance enterography: Review of the technique for the study of Crohn’s disease. Radiologia 2011, 53, 421–433. [Google Scholar] [CrossRef]
- Vestito, A.; Marasco, G.; Maconi, G.; Festi, D.; Bazzoli, F.; Zagari, R.M. Role of Ultrasound Elastography in the Detection of Fibrotic Bowel Strictures in Patients with Crohn’s Disease: Systematic Review and Meta-Analysis. Ultraschall der Med.-Eur. J. Ultrasound 2019, 40, 646–654. [Google Scholar] [CrossRef]
- Fraquelli, M.; Branchi, F.; Cribiù, F.M.; Orlando, S.; Casazza, G.; Magarotto, A.; Massironi, S.; Botti, F.; Contessini-Avesani, E.; Conte, D.; et al. The Role of Ultrasound Elasticity Imaging in Predicting Ileal Fibrosis in Crohn’s Disease Patients. Inflamm. Bowel Dis. 2015, 21, 2605–2612. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Mao, R.; Li, X.-H.; Cao, Q.-H.; Chen, Z.-H.; Liu, B.-X.; Chen, S.-L.; Chen, B.-L.; He, Y.; Zeng, Z.-R.; et al. Real-Time Shear Wave Ultrasound Elastography Differentiates Fibrotic from Inflammatory Strictures in Patients with Crohn’s Disease. Inflamm. Bowel Dis. 2018, 24, 2183–2190. [Google Scholar] [CrossRef]
- De Voogd, F.; Joshi, H.; Van Wassenaer, E.; Bots, S.; D’Haens, G.; Gecse, K. Intestinal Ultrasound to Evaluate Treatment Response During Pregnancy in Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2021, 28, 1045–1052. [Google Scholar] [CrossRef]
- Flanagan, E.; Wright, E.K.; Begun, J.; Bryant, R.V.; An, Y.-K.; Ross, A.L.; Kiburg, K.V.; Bell, S.J. Monitoring Inflammatory Bowel Disease in Pregnancy Using Gastrointestinal Ultrasonography. J. Crohn’s Colitis 2020, 14, 1405–1412. [Google Scholar] [CrossRef]
- Leung, Y.; Shim, H.H.; Wilkens, R.; Tanyingoh, D.; Afshar, E.E.; Sharifi, N.; Pauls, M.; Novak, K.L.; Kaplan, G.G.; Panaccione, R.; et al. The Role of Bowel Ultrasound in Detecting Subclinical Inflammation in Pregnant Women with Crohn’s Disease. J. Can. Assoc. Gastroenterol. 2018, 2, 153–160. [Google Scholar] [CrossRef]
- Asthana, A.K.; Friedman, A.B.; Maconi, G.; Maaser, C.; Kucharzik, T.; Watanabe, M.; Gibson, P.R. The failure of gastroenterologists to apply intestinal ultrasound in inflammatory bowel disease in the Asia-Pacific: A need for action. J. Gastroenterol. Hepatol. 2014, 30, 446–452. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).