1. Introduction
According to the literature, up to 40% of young children suffer from feeding disorders, most of them having behavioral factors, including food neophobia, as a dominant issue [
1,
2,
3]. Food neophobia is defined as a reluctance to consume or an unwillingness to try unknown foods [
4]. Every human organism displays, to a certain extent, the natural avoidance of new foods. This phenomenon is associated with adaptive evolutionary conditioning. Its role was to protect an organism from the possibility of intoxication with novel, unknown food. In the present times, where food seems to be safe due to our knowledge and technological processing, food neophobia has a negative impact on the variety of food choices, with special concern for meat, fruits, and vegetables [
5,
6] Consequently, the child’s diet can be unbalanced, lacking in nutrients, and too low or too high in energy.
The mechanism conditioning the onset of food neophobia has not been fully understood. Children’s eating behaviors are influenced by both intrinsic (genetics, age, gender) and environmental (family, peers, community, and society) factors [
7]. According to the results of a recent systemic review conducted by Thamara de Oliveira Torres and co-workers, the main factors associated with food neophobia were: parental influence on children’s eating habits, children’s innate preference for sweet and savory flavors, influence of the sensory aspect of the food, parents’ exerting pressure on for the child to eat, parents’ lack of encouragement and/or affection at mealtime, childhood anxiety, and diets with low variety and low nutritional quality [
4].
It is known that an infant is born with an innate preference for the sweet taste. Between three and four months of age, it develops a natural preference for the salty and umami tastes [
8]. Bitter and sour tastes are difficult and demanding for infants and their acceptance is acquired with time and repeated exposures to the individual foods.
The bitter taste perception is genetically determined, and differs due to the haplotypes generated by three polymorphisms in the region of the gene encoding TAS2R83 receptor [
9]. Differences in TAS2R38 bitter taste gene were associated with acceptance of the first complementary food in infants, suggesting a possible involvement in eating behavior at weaning [
10]. TAS2R is a member of the bitter taste receptors family and is associated with the sensitivity to taste phenyltiocarbamide (PTC) and 6-propylthiouracil (6-PROP). On this basis, subjects can be divided into tasters (with the strong perception to bitter taste) and non-tasters (with weak or no reaction to PTC or 6-PROP). A 2003 report by Kim et al. shows that the two common haplotypes of the gene (the recessive AVI and the dominant PAV) account for about 85% of the bimodal taste response observed [
11]. Composed of 1002 nucleotides, TAS2R38 contains three missense-coding single nucleotide polymorphisms (SNPs) at positions 145 (proline or alanine), 785 (alanine or valine), and 886 (valine or isoleucine). Despite the eight possible amino acid combinations, only six haplotypes have been observed with respect to taste sensitivity: PAV and AVI as the most common, AAI and AAV as rare, PAI and PVI as extremely rare. Typically, individuals with at least one copy of the dominant PAV haplotype have the ability to taste PTC/6-PROP, in contrast to AVI homozygotes which do not, and the rare haplotypes AAI and AAV have been both observed to confer an intermediate sensitivity [
12]. Interestingly, people with a particular combination of haplotypes, i.e., AVI/PAV heterozygotes, are more likely to change sensitivity to bitterness 6-PROP over time (gradual decrease in bitterness sensitivity) [
13].
Subjects with different taste sensitivities may present diverse responses to the nutrient stimulation, and therefore different metabolic hormone secretions. Increased sensitivity to 6-PROP has been associated with the lower acceptance of green vegetables in children and adults [
14]. On contrary, vegetable intake in Japanese preschool children was associated with food neophobia (measured with the Child Food Neophobia Scale, CFNS), but not with 6-PROP sensitivity [
15]. Taste sensitivity to 6-PROP was related to the higher BMI z-scores in six-year-old children [
16].
The impact of good nutrition early in life can reach far into the future. Knowledge of risk factors for the development of food neophobia may facilitate both an understanding of the problem, and conducting therapy. According to the main finding of Myles S. Faith’s and co-workers’ study, genes play a substantial role in young children’s tendency to avoid new food, accounting for 72% of the variance in this trait. Thus, in the opinion of the authors, genes appear to influence a range of eating patterns that emerge during childhood [
17]. To our knowledge, no study to date has explored the influence of genetically determined hypersensitivity to the bitter taste on food neophobia in early childhood. It is also unclear whether food neophobia is associated with poor nutritional status. Food neophobic children may tend to have insufficient calories intake, relative to their energy needs, due to their reluctance to try new food, however data on this topic is lacking. It is also the first study that has explored the correlation between the gut-brain hormonal axis, enteric peptides, and child food neophobia.
Therefore, the aim of our prospective study was to determine the role of the gut-brain hormonal axis and the effects of the enteric peptides, as well as the role of the genetically determined sensitivity to the bitter taste, on the development of child food neophobia and subsequently, its possible association with nutritional status.
3. Discussion
Childhood is an exceptional period of life for health interventions, as health-related behaviors are being formed, including those correlated to the future prevention of obesity and diet-related diseases. Food neophobia may lead to impaired nutritional status, as well as to limited food preferences. To determine if childhood picky eating or food neophobia is associated with childhood weight status, or with becoming underweight, overweight, or obese later in childhood, Callie et al. conducted a systematic review [
18]. No association existed between childhood weight status and food neophobia, and results were unclear for picky eating. The results of our analysis are consistent with those presented by Callie and co-workers. In our study the groups (neophobic vs control) did not differ statistically significantly from each other in terms of anthropometric parameters (
p = 0.194). Mean BMI percentile in neophobia group was 38.67 (min. 0.40; max. 92.00) and in control group 47.95 (min. 4.00; max. 85.00).
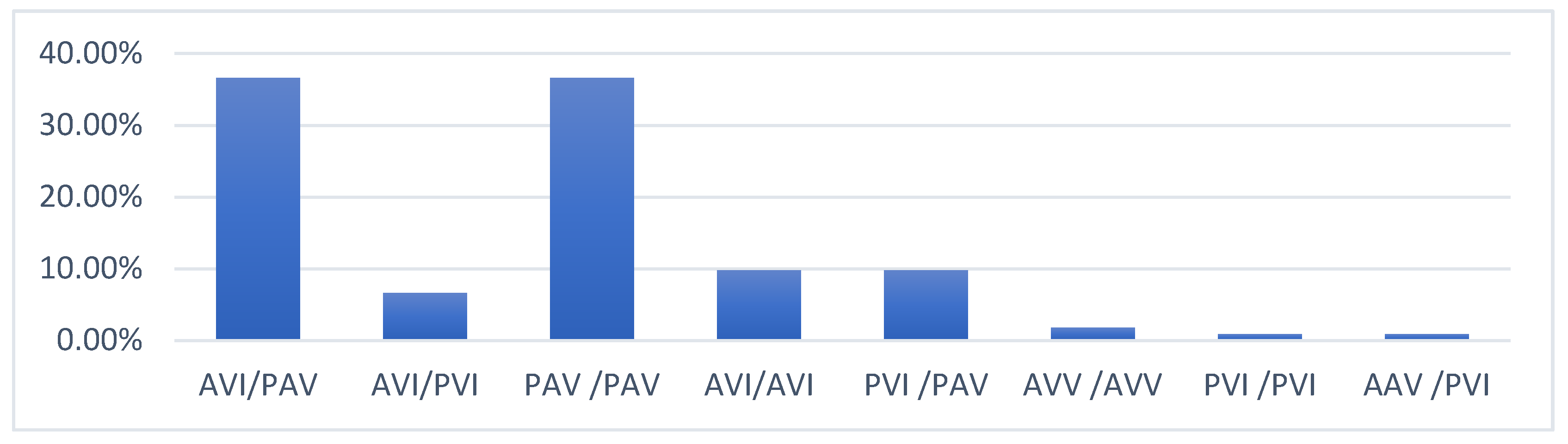
According to the results presented by Boxer et al., the prevalence of the PAV haplotype was 42.3%, AVI 53.1%, AAV 2.5%, AAI 1.2%, PAI 0.8%, and PVI 0.1%. The authors proved that bitter taste sensitivity to PROP exists as a broad range, and not exclusively as non-tasters or medium tasters. The most frequent diplotype among the investigated subjects in our research was heterozygous AVI (40.2%) and homozygous PAV (36.6%). Fewer participants (9.8%) had the AVI homozygous diplotype. The interesting finding of this study is that correlation between 6-PRO perception and genotype was not confirmed in our trial (
p = 0.064). Our conclusions should be interpreted in light of study limitations and need to be replicated with a larger sample. The available literature suggests that some children may require additional strategies to accept and consume bitter-tasting fruits and vegetables and that genetic predisposition may be modified by repeated exposure [
19].
The important known factors that may indirectly influence feeding difficulties and the course of food neophobia include the diet during pregnancy and lactation, or the mode of food exposure and its repetition [
20]. Sensory characteristics have been singled out as one of the most influential determinants of eating behavior, and among these, textures are the main reason for food rejection or acceptance in children, while the sounds accompanying the disintegration of food in the oral cavity, which correlate to the textures, also play a part in acceptance or lack thereof [
21]. According to the available data, increased sensitivity to 6-PROP was associated with the lower acceptance of green vegetables by children and adults [
14]. Vegetable intake in preschool children was associated with food neophobia (measured with the CFNS), but not with 6-PROP sensitivity [
15]. The results of our analysis confirm the role of hypersensitivity to bitter taste in the development of food neophobia. The present findings expand current knowledge about the additional factors associated with the child food neophobia.
It should be noted that bitter sensitivity changes over the lifespan and is affected by the person’s genotype for alleles with the bitter receptor TAS2R38. These developmental sensory changes are most marked for people who have a particular haplotype combination, i.e., AVI/PAV heterozygotes [
13].
NPY plays a role in food consumption via various factors: fexample, it has orexigenic effect, triggered by the energy deficiency, resulting in corresponding signalling in the hypothalamus [
22]. It stimulates food intake with a preferential effect on carbohydrate intake. In humans and animals, elevated plasma NPY levels were observed in several stress conditions, including exercise, hypoxia, cold exposure, tissue injury, ischemia, and hemorrhagic shock [
23]. We found, unexpectedly, that the serum level of NPY in patients with food neophobia was significantly higher than in the control group (
p = 0.03). The correlation between the serum level of the other gut-brain hormonal axis and enteric peptides with food neophobia has not been proven. Only a few studies have addressed the impact of gut-brain hormonal axis or enteric peptides on dietary habits. It was shown in previous studies that elevated serum leptin, particularly in obese adult individuals, should be taken as a warning sign of energy imbalance, poor diet, hyperinsulinemia, insulin resistance, or changes in other metabolic risk factors that are strongly associated with cardiovascular disease and type 2 diabetes. Obesity was also associated with increased serum leptin levels and insulin resistance, but the authors emphasize the necessity for further multi-centric studies to prove the possible relationship, which might help devise plans to manage obesity [
24]. The function of leptin itself is well documented as a controller of the food intake, energy expenditure, and body weight [
25,
26]. Wang et al. have shown that leptin and IGF-1 levels are increased in tasters in comparison to non-tasters [
27]. Researchers suggested that increased leptin levels may have an impact on the differences in the control of energy homeostasis between tasters and non-tasters.
A group of authors from Wilmington investigated plasma ghrelin and obestatin in children with failure to thrive (FTT) and obesity as compared with age-matched controls. Fasting ghrelin and obestatin levels did not differ significantly in children with FTT [
28]. Adiponectin is the richest adipokine in human plasma, and it is mainly secreted from white adipose tissue. Adiponectin circulates in blood as high-molecular, middle-molecular, and low-molecular weight isoforms. Numerous studies have demonstrated its insulin-sensitizing, anti-atherogenic, and anti-inflammatory effects [
29]. Lower adiponectin levels are observed in individuals with obesity and those at risk for cardiovascular disease [
30]. Adiponectin concentrations were elevated in the infants with eating problems [
31]. However, this was a cross-sectional association, therefore the causal relationship needs further investigation.
The cause of developing limited food preferences remains unknown. To our knowledge, this is the first study on the relationship between innate taste sensitivity and the brain-gut interaction and the development of child food neophobia. These data provide further evidence that bitter taste sensitivity to 6-PROP plays an important role in the development of child food neophobia. We have proved that genetic determinants are not enough for the development of food neophobia in children. Additional factors, such as parental influence, are very important [
32].
Due to their selective diet, children with neophobia may be at risk of malnutrition. In the light of our research results, due to their elevated serum NPY levels, these groups of children should be checked regularly in order to monitor their nutritional status at an older age, but our results suggest that the food choices of children with food neophobia may be directed towards a higher carbohydrate intake, which may increase the risk of being overweight or obese in the future. Neuropeptide Y has functions that are closely related to appetite regulation and obesity formation [
33]. Prospective studies should clarify whether food neophobia at the age of 18–36 months increases the risk of obesity later in life.
The correlation between the gut-brain hormonal axis, enteric peptides, and child food neophobia needs further research.
4. Materials and Methods
4.1. Study Design
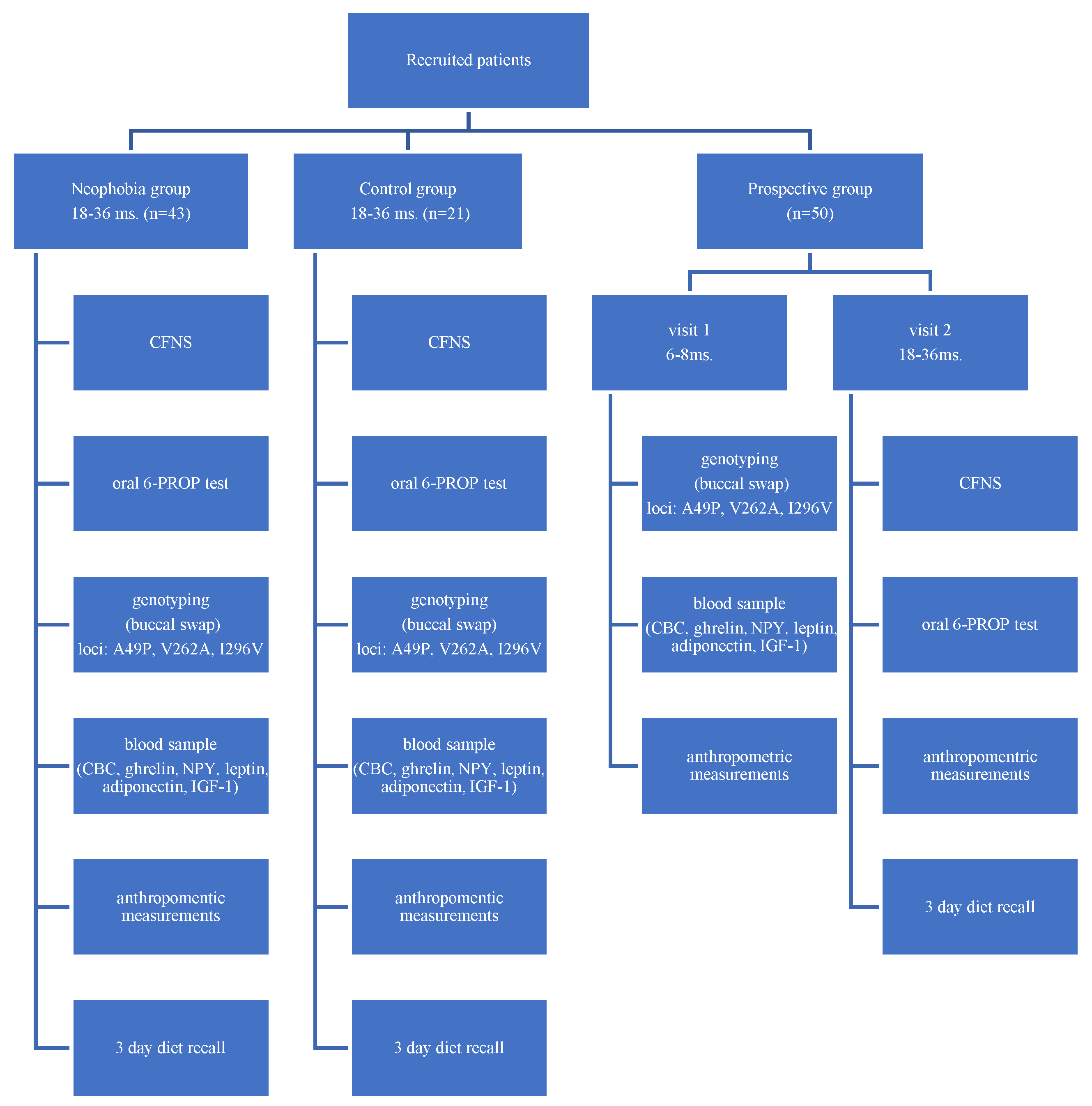
The study had two parts—the first part was performed on children aged 18–36 months with diagnosed food neophobia and their age-matched controls; the second part involved prospective assessment of the infants at 6 months of age, with a follow-up investigation at 18–36 months of age (prospective group).
Figure 2 presents the flowchart of study design.
In the first part of study, participants were assessed with the Child Food Neophobia Scale (CFNS) and based on the scale result were classified into two groups: a neophobia group and a control group. Children in the neophobia group were recruited from children referred to our clinic because of a feeding disorder, as well as via self-application through the social media (dedicated Facebook page was created for the purposes of the study). The control group formed children with minor clinical problems, recruited in a local outpatient clinic and via self-application through the social media. Gastrointestinal and metabolic diseases, as well as a failure to thrive, were the exclusion criteria for both, control and neophobia groups. Genotyping for bitter taste sensitivity was performed using buccal swabs for all participants in the study. Furthermore, all patients underwent an oral 6-PROP test, anthropometric measurements, and tests for serum levels of leptin, adiponectin, IGF-1, ghrelin, NPY, and complete blood count (CBC) measurements, from a blood sample after 4 h fasting.
In a parallel study, healthy infants (prospective group) were recruited through a local pediatric outpatient clinic and also through self-application via social media. At the first visit, genotyping for bitter taste sensitivity was performed using buccal swabs, as well as anthropometric measurements, and serum levels of leptin, adiponectin, IGF-1, ghrelin, NPY, and CBC measurements from blood samples after 4 h fasting. During the second visit, participants were assessed with the CFNS, anthropometric measurements, and 6-PROP test for the bitter taste sensitivity. The control visit was done remotely due to the epidemiological situation related to the COVID-19 pandemic.
4.2. Assessment of the Food Neophobia
Information pertaining to child food neophobia was obtained through a parent-reported questionnaire, based on the translation of the Child Food Neophobia Scale (CFNS) [
34,
35]. The CFNS is a 8-item instrument that assesses the degree of food neophobia or avoidance of new food. The instrument was completed by parents. The CFNS has a range of 8–40, with higher scores reflecting greater amounts of the trait. Each question is answered on a 1–5 Likert scale (Strongly disagree, Disagree, Neither agree nor disagree, Agree, Strongly agree)
Table 10.
4.3. Assessment of the Taste Sensitivity
The genetic testing for the three polymorphisms in the region of the gene encoding TAS2R83 receptor was performed (loci: A49P, V262A, I296V) by MEDGEN Medical Center (Warsaw, Poland). On the basis of haplotype distribution, participants were divided into two groups: tasters (with high sensitivity to PROP) and non-tasters (with low bitter sensitivity).
Furthermore, all participants at the age of 18–36 months had an oral N-Propylthiouracil Test Paper, PROP (Precision Laboratories) performed, in order to confirm taste sensitivity. Patients were phenotyped as tasters (symptomatic negative reaction/grimace/crying after contact of the tongue with the test paper) and non-tasters (no reaction to test paper).
4.4. Laboratory Tests
The complete blood count (CBC) was performed using basic laboratory equipment. The level of hormones and peptides responsible for the feeling of satiety (leptin, adiponectin, IGF-1), as well as peptides accountable for the feeling of hunger (NPY, ghrelin) were assessed after 4 h of fasting in all children. The assays were performed using commercial ELISA kits (Cloud-Clone Corp., City of Katy, TX, USA; Labnoratorini medicina a.s., Brno, Czech Republic; Mediagnost, Reutlingen, Germany).
4.5. Ethical Considerations
All the procedures were reviewed and approved by the Independent Review Board (Bioethical Committee Children’s Memorial Health Institute, Approval Number: 204/KBE/2015). Patients’ caregivers gave their written informed consent prior to enrolment in the study.
4.6. Statistical Analysis
Statistical analyzes were carried out using the IBM SPSS Statistics version 26 package. The basic descriptive statistics, chi-square tests of independence, Pearson correlation coefficient r, Spearman’s r correlation analysis rho, Student’s t-tests, and Mann–Whitney tests, as well as Kruskal–Wallis tests, were applied. The level of statistical significance was α = 0.05.


 ,
, 



{kind=link}
{kind=link}