Cross Sectional Study of the Community Self-Reported Risk of Obstructive Sleep Apnoea (OSA) and Awareness in Thessaly, Greece

 ,
,  and
and 
Abstract
:1. Introduction
2. Results
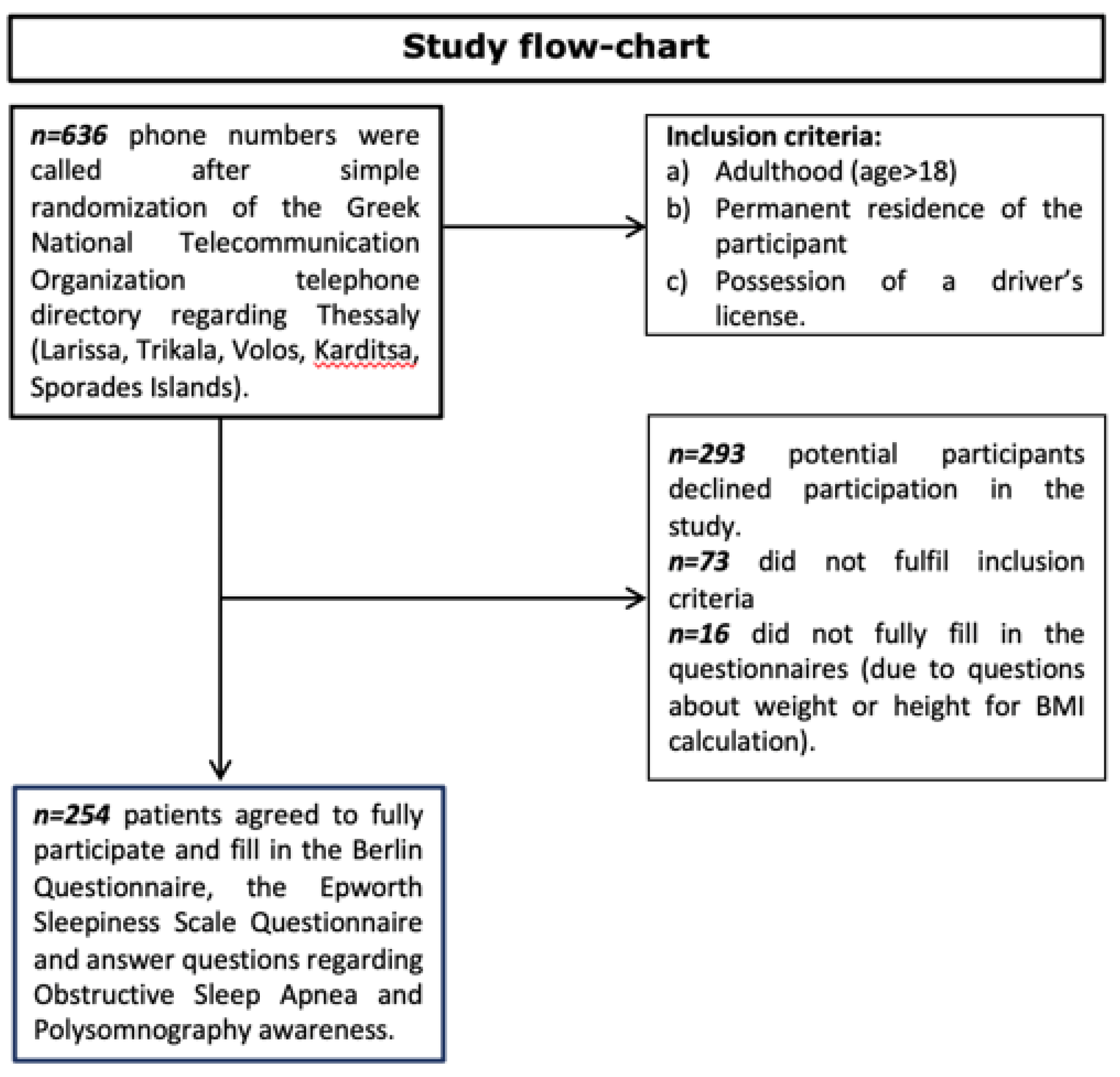
2.1. Sample Characteristics and Responsiveness Rate
2.2. OSAS Risk According to BQ and ESS
2.3. Participants’ Awareness Regarding OSAS and Its Clinical Diagnosis
3. Discussion
4. Materials and Methods
4.1. Study Protocol
4.2. Assessment Tools
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Obstructive Sleep Apnoea Syndrome at Chronic Respiratory Diseases. Available online: http://www.who.int/respiratory/other/Obstructive_sleep_apnoea_syndrome/en/ (accessed on 14 April 2021).
- White, D.P. Pathophysiology of obstructive sleep apnoea. Thorax 1995, 50, 797–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Academy of Sleep Medicine (AASM). Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999, 22, 667–689. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.L.; Hoyos, C.M.; Killick, R.; Sutherland, K.; Cistulli, P.A.; Zwar, N.; Yee, B.J.; Marks, G.; Grunstein, R.R.; Wong, K.K.H.; et al. Development and validation of a model for diagnosis of obstructive sleep apnoea in primary care. Respirology 2021, 10, 989–996. [Google Scholar] [CrossRef]
- Toraldo, D.; Passali, D.; Sanna, A.; De Nuccio, F.; Conte, L.; De Benedetto, M. Cost-effectiveness strategies in OSAS management: A short review. Acta Otorhinolaryngol. Ital. 2017, 37, 447–453. [Google Scholar] [CrossRef]
- Pace, A.; Iannella, G.; Rossetti, V.; Visconti, I.C.; Gulotta, G.; Cavaliere, C.; De Vito, A.; Maniaci, A.; Cocuzza, S.; Magliulo, G.; et al. Diagnosis of Obstructive Sleep Apnea in Patients with Allergic and Non-Allergic Rhinitis. Medicina 2020, 56, 454. [Google Scholar] [CrossRef] [PubMed]
- Alexandropoulou, A.; Vavougios, G.; Hatzoglou, C.; Gourgoulianis, K.; Zarogiannis, S. Risk Assessment for Self Reported Obstructive Sleep Apnea and Excessive Daytime Sleepiness in a Greek Nursing Staff Population. Medicina 2019, 55, 468. [Google Scholar] [CrossRef] [Green Version]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef] [Green Version]
- Hiestand, D.M.; Britz, P.; Goldman, M.; Phillips, B. Prevalence of symptoms and risk of sleep apnea in the US population: Results from the National Sleep Foundation Sleep in America 2005 Poll. Chest 2006, 130, 780–786. [Google Scholar] [CrossRef] [Green Version]
- Hrubos-Strøm, H.; Randby, A.; Namtvedt, S.K.; Kristiansen, H.A.; Einvik, G.; Benth, J.; Somers, V.K.; Nordhus, I.H.; Russel, M.B.; Dammen, T.; et al. A Norwegian population-based study on the risk and prevalence of obstructive sleep apnea The Akershus Sleep Apnea Project (ASAP). J. Sleep Res. 2011, 20, 162–170. [Google Scholar] [CrossRef] [Green Version]
- Frangopoulos, F.; Nicolaou, I.; Zannetos, S.; Economou, N.T.; Adamide, T.; Georgiou, A.; Trakada, G. Estimating obstructive sleep apnea in Cyprus: A randomised, stratified epidemiological study using STOP-Bang sleep apnea questionnaire. Sleep Med. 2019, 61, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Pataka, A.; Daskalopoulou, E.; Kalamaras, G.; Fekete Passa, K.; Argyropoulou, P. Evaluation of five different questionnaires for assessing sleep apnea syndrome in a sleep clinic. Sleep Med. 2014, 15, 776–781. [Google Scholar] [CrossRef]
- Chami, H.A.; Bechnak, A.; Isma’eel, H.; Talih, F.; Nasreddine, L.; Nasrallah, M.; Tamim, H. Sleepless in Beirut: Sleep difficulties in an urban environment with chronic psychosocial stress. J. Clin. Sleep Med. 2019, 15, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Jniene, A.; El Ftouh, M.; El Fassy Fihry, M.T. Study of the prevalence of sleep apnea syndrome’s symptoms in a Moroccan population. Tuberk Toraks. 2012, 60, 108–113. [Google Scholar] [CrossRef]
- Thorarinsdottir, E.H.; Bjornsdottir, E.; Benediktsdottir, B.; Janson, C.; Gislason, T.; Aspelund, T.; Kuna, S.T.; Pack, A.I.; Arnardottir, E.S. Definition of excessive daytime sleepiness in the general population: Feeling sleepy relates better to sleep-related symptoms and quality of life than the Epworth Sleepiness Scale score. Results from an epidemiological study. J. Sleep Res. 2019, 28, e12852. [Google Scholar] [CrossRef]
- Jaussent, I.; Morin, C.M.; Ivers, H.; Dauvilliers, Y. Natural history of Excessive Daytime Sleepiness: A population-based 5-year longitudinal study. Sleep 2020, 43, zsz249. [Google Scholar] [CrossRef] [PubMed]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Original Contribution Increased Prevalence of Sleep-Disordered Breathing in Adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Tufik, S.; Santos-Silva, R.; Taddei, J.A.; Bittencourt, L.R. Obstructive sleep apnea syndrome in the Sao Paulo Epidemiologic Sleep Study. Sleep Med. 2010, 11, 441–446. [Google Scholar] [CrossRef]
- Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The occurrence of sleep disordered breathing in middleaged adults. N. Engl. J. Med. 1993, 328, 12305. [Google Scholar] [CrossRef] [Green Version]
- Bixler, E.O.; Vgontzas, A.N.; Lin, H.M.; Ten Have, T.; Rein, J.; Vela-Bueno, A.; Kales, A. Prevalence of sleep-disordered breathing in women: Effects of gender. Am. J. Respir. Crit. Care Med. 2001, 163, 608–613. [Google Scholar] [CrossRef]
- Bearpark, H.; Elliott, L.; Grunstein, R.; Cullen, S.; Schneider, H.; Althaus, W.; Sullivan, C. Snoring and sleep apnea: A population study in Australian men. Am. J. Respir. Crit. Care Med. 1995, 151, 1459–1465. [Google Scholar] [CrossRef] [PubMed]
- Udwadia, Z.F.; Doshi, A.V.; Lonkar, S.G.; Singh, C.I. Prevalence of sleep disordered breathing and sleep apnea in middle-aged urban Indian men. Am. J. Respir. Crit. Care Med. 2004, 169, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Ip, M.S.; Lam, B.; Lauder, I.J.; Tsang, K.W.; Chung, K.F.; Mok, Y.W.; Lam, W.K. A community study of sleep-disordered breathing in middle-aged Chinese men in Hong Kong. Chest 2001, 119, 62–69. [Google Scholar] [CrossRef]
- Kim, J.; In, K.; Kim, J.; You, S.; Kang, K.; Shim, J.; Lee, S.; Lee, J.; Lee, S.; Park, C.; et al. Prevalence of sleep-disordered breathing in middle-aged Korean men and women. Am. J. Respir. Crit. Care Med. 2004, 170, 1108–1113. [Google Scholar] [CrossRef]
- Li, J.; McEvoy, R.D.; Zheng, D.; Loffler, K.A.; Wang, X.; Redline, S.; Woodman, R.J.; Anderson, C.S. Self-reported Snoring Patterns Predict Stroke Events in High-Risk Patients With OSA: Post Hoc Analyses of the SAVE Study. Chest 2020, 158, 2146–2154. [Google Scholar] [CrossRef]
- Cammaroto, G.; Bianchi, G.; Zhang, H.; Veer, V.; Kotecha, B.; Jacobowitz, O.; Llatas, M.C.; de Apodaca, P.M.R.; Lugo, R.; Meccariello, G.; et al. Sleep medicine in otolaryngology units: An international survey. Sleep Breath. 2021, 25, 2141–2152. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, L.; Brady, E.M.; Freeman, S.C.; Polmann, H.; Réus, J.C.; Flores-Mir, C.; De Luca Canto, G.; Robertson, N.; Squire, I.B. Diagnostic accuracy of screening questionnaires for obstructive sleep apnoea in adults in different clinical cohorts: A systematic review and meta-analysis. Sleep Breath. 2021, 1–26. [Google Scholar] [CrossRef]
- Chiu, H.Y.; Chen, P.Y.; Chuang, L.P.; Chen, N.H.; Tu, Y.K.; Hsieh, Y.J.; Wang, Y.C.; Guilleminault, C. Diagnostic accuracy of the Berlin questionnaire, STOP-BANG, STOP, and Epworth sleepiness scale in detecting obstructive sleep apnea: A bivariate meta-analysis. Sleep Med. Rev. 2017, 36, 57–70. [Google Scholar] [CrossRef]
- Senaratna, C.V.; Perret, J.L.; Matheson, M.C.; Lodge, C.J.; Lowe, A.J.; Cassim, R.; Russell, M.A.; Burgess, J.A.; Hamilton, G.S.; Dharmage, S.C. Validity of the Berlin questionnaire in detecting obstructive sleep apnea: A systematic review and meta-analysis. Sleep Med. Rev. 2017, 36, 116–124. [Google Scholar] [CrossRef]
- Tan, A.; Yin, J.D.; Tan, L.W.; van Dam, R.M.; Cheung, Y.Y.; Lee, C.H. Using the Berlin Questionnaire to Predict Obstructive Sleep Apnea in the General Population. J. Clin. Sleep Med. 2017, 13, 427–432. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.G.; Bland, J.M. Statistics notes. Treatment allocation in controlled trials: Why randomise? BMJ 1999, 318, 1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouloukaki, I.; Komninos, I.D.; Mermigkis, C.; Micheli, K.; Komninou, M.; Moniaki, V.; Mauroudi, E.; Siafakas, N.M.; Schiza, S.E. Translation and validation of Berlin questionnaire in primary health care in Greece. BMC Pulm. Med. 2013, 13, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsara, V.; Serasli, E.; Amfilochiou, A.; Constyantinidis, T.; Christaki, P. Greek version of the Epworth Sleepiness Scale. Sleep Breath 2004, 8, 91–95. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Males (84/254; 33.07%) | Females (170/254; 66.93%) | p Value | |
|---|---|---|---|
| Age (years) | 54.12 ± 17.00 | 54.11 ± 15.74 | >0.05 |
| BMI (kg/m²) | 27.66 ± 4.79 | 26.25 ± 5.13 | 0.036 |
| Smokers (%) | 53.73 | 32.12 | <0.05 |
| BQ High Risk | ESS High Risk | BQ and ESS High Risk | ||||
|---|---|---|---|---|---|---|
| Gender | M (#) | F (#) | M (#) | F (#) | M (#) | F (#) |
| Larissa | 7 | 5 | 1 | 3 | 0 | 1 |
| (n = 56) | ||||||
| Volos | 4 | 9 | 1 | 5 | 0 | 2 |
| (n = 50) | ||||||
| Trikala (n = 50) | 5 | 8 | 3 | 3 | 2 | 0 |
| Karditsa (n = 48) | 5 | 9 | 4 | 3 | 2 | 0 |
| Sporades (n = 50) | 4 | 12 | 1 | 3 | 1 | 2 |
| Total (n = 254) | 25 | 43 | 10 | 17 | 5 | 5 |
| % over total per gender | 29.76% | 25.29% | 11.90% | 10.00% | 5.95% | 2.94% |
| % over total | 26.77% | 10.63% | 3.94% | |||
| Awareness Regarding OSAS | Awareness Regarding OSAS Diagnosis | Awareness Regarding PSG | ||||
|---|---|---|---|---|---|---|
| Gender | M (#) | F (#) | M (#) | F (#) | M (#) | F (#) |
| Larissa (n = 56) | 7 | 20 | 2 | 5 | 5 | 9 |
| Volos (n = 50) | 17 | 16 | 3 | 6 | 4 | 6 |
| Trikala (n = 50) | 11 | 24 | 5 | 6 | 5 | 12 |
| Karditsa (n = 48) | 13 | 20 | 4 | 8 | 6 | 6 |
| Sporades (n = 50) | 10 | 25 | 3 | 5 | 2 | 8 |
| Total (n = 254) | 58 | 105 | 17 | 30 | 22 | 41 |
| % over total per gender | 69.05% | 61.76% | 20.24% | 17.65% | 26.19% | 24.12% |
| % over total | 64.17% | 18.50% | 24.80% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kassas, P.; Vavougios, G.D.; Hatzoglou, C.; Gourgoulianis, K.I.; Zarogiannis, S.G. Cross Sectional Study of the Community Self-Reported Risk of Obstructive Sleep Apnoea (OSA) and Awareness in Thessaly, Greece. Clocks & Sleep 2022, 4, 16-22. https://doi.org/10.3390/clockssleep4010004
Kassas P, Vavougios GD, Hatzoglou C, Gourgoulianis KI, Zarogiannis SG. Cross Sectional Study of the Community Self-Reported Risk of Obstructive Sleep Apnoea (OSA) and Awareness in Thessaly, Greece. Clocks & Sleep. 2022; 4(1):16-22. https://doi.org/10.3390/clockssleep4010004
Chicago/Turabian StyleKassas, Petros, Georgios D. Vavougios, Chrissi Hatzoglou, Konstantinos I. Gourgoulianis, and Sotirios G. Zarogiannis. 2022. "Cross Sectional Study of the Community Self-Reported Risk of Obstructive Sleep Apnoea (OSA) and Awareness in Thessaly, Greece" Clocks & Sleep 4, no. 1: 16-22. https://doi.org/10.3390/clockssleep4010004
APA StyleKassas, P., Vavougios, G. D., Hatzoglou, C., Gourgoulianis, K. I., & Zarogiannis, S. G. (2022). Cross Sectional Study of the Community Self-Reported Risk of Obstructive Sleep Apnoea (OSA) and Awareness in Thessaly, Greece. Clocks & Sleep, 4(1), 16-22. https://doi.org/10.3390/clockssleep4010004