Increased Resilience Weakens the Relationship between Perceived Stress and Anxiety on Sleep Quality: A Moderated Mediation Analysis of Higher Education Students from 7 Countries

 , , , , , ,
, , , , , ,  , , , ,
, , , ,
Abstract
1. Introduction
- (1)
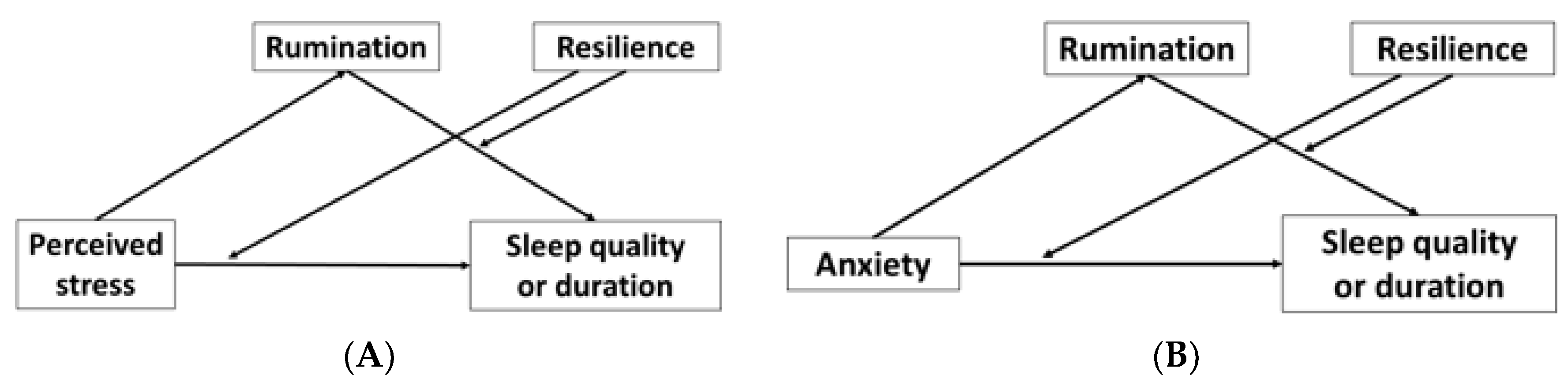
- Higher levels of perceived stress would be associated with decreased sleep quality and duration through increased rumination.
- (2)
- Higher levels of anxiety would be associated with decreased sleep quality and duration through increased rumination.
- (3)
- Students with higher levels of resilience were likely to be protected from the negative impact of perceived stress and anxiety on sleep quality and sleep duration.
2. Results
2.1. Participant Characteristics
2.2. Mental Health and Sleep Behaviors Influenced by COVID-19
2.3. Mediation and Moderation Analyses
2.3.1. Correlations between Examined Variables
2.3.2. Model 1 Moderated Mediation Model of Perceived Stress on Sleep Quality
2.3.3. Model 2 Moderated Mediation Model of Perceived Stress on Sleep Duration
2.3.4. Model 3 Moderated Mediation Model of Perceived Stress on Sleep Quality
2.3.5. Model 4 Moderated Mediation Model of Perceived Stress on Sleep Quality
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Demographics
4.3. Assessment of Perceived Stress and Anxiety
4.4. Assessment of Psychological Resilience and Rumination
4.5. Assessment of Sleep Duration and Quality
4.6. Assessment of How COVID-19 Impacted the Factors Described Above
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Varghese, R.P.; Norman, T.S.J.; Thavaraj, S. Perceived stress and self efficacy among college students: A global review. Psychology 2015, 5, 15–24. [Google Scholar] [CrossRef]
- Talwar, P.; Othman, M.K.; Othman, A.E.A.; Mua, M.S.; Mughal, H.Y. Socio-demographic determinants and prevalence of depression, anxiety, and stress among Malaysian university students. J. Indian Acad. Appl. Psychol. 2017, 43, 296–304. [Google Scholar]
- Gao, W.; Ping, S.; Liu, X. Gender differences in depression, anxiety, and stress among college students: A longitudinal study from China. J. Affect. Disord. 2020, 263, 292–300. [Google Scholar] [CrossRef]
- Boumosleh, J.M.; Jaalouk, D. Depression, anxiety, and smartphone addiction in university students—A cross sectional study. PLoS ONE 2017, 12, e0182239. [Google Scholar] [CrossRef] [PubMed]
- Evans, T.M.; Bira, L.; Gastelum, J.B.; Weiss, L.T.; Vanderford, L.N. Evidence for a mental health crisis in graduate education. Nat. Biotechnol. 2018, 36, 282–284. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Hoying, J.; Melnyk, B.M.; Hutson, E.; Tan, A. Prevalence and correlates of depression, anxiety, stress, healthy beliefs, and lifestyle behaviors in first-year graduate health sciences students. Worldviews Evid. Based Nurs. 2020, 17, 49–59. [Google Scholar] [CrossRef]
- Moore, C.J.; Cunningham, S.A. Social position, psychological stress, and obesity: A systematic review. J. Acad. Nutr. Diet. 2012, 112, 518–526. [Google Scholar] [CrossRef]
- De Vriendt, T.; Moreno, L.A.; de Henauw, S. Chronic stress and obesity in adolescents: Scientific evidence and methodological issues for epidemiological research. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 511–519. [Google Scholar] [CrossRef]
- Sparrenberger, F.; Cichelero, F.T.; Ascoli, A.M.; Fonseca, F.P.; Weiss, G.; Berwanger, O.; Fuchs, S.C.; Moreira, L.B.; Fuchs, F.D. Does psychosocial stress cause hypertension? A systematic review of observational studies. J. Hum. Hyperten. 2009, 23, 1. [Google Scholar] [CrossRef]
- Liu, M.-Y.; Li, N.; Li, W.A.; Khan, H. Association between psychosocial stress and hypertension: A systematic review and meta-analysis. Neurol. Res 2017, 39, 573–580. [Google Scholar] [CrossRef] [PubMed]
- WEB-USI-MH-report-1.pdf. Available online: http://usi.ie/wp-content/uploads/2019/08/WEB-USI-MH-report-1.pdf (accessed on 28 June 2020).
- Johnson, E.O.; Roth, T.; Breslau, N. The association of insomnia with anxiety disorders and depression: Exploration of the direction of risk. J. Psychiatr. Res. 2006, 40, 700–708. [Google Scholar] [CrossRef] [PubMed]
- van Reeth, O.; Weibel, L.; Spiegel, K.; Leproult, R.; Dugovic, C.; Maccari, S. Physiology of sleep (review)–Interactions between stress and sleep: From basic research to clinical situations. Sleep Med. Rev. 2000, 4, 201–219. [Google Scholar] [CrossRef]
- Kim, E.-J.; Dimsdale, J.E. The effect of psychosocial stress on sleep: A review of polysomnographic evidence. Behav. Sleep. Med. 2007, 5, 256–278. [Google Scholar] [CrossRef]
- Patel, S.R. Reduced sleep as an obesity risk factor. Obes. Rev. 2009, 10, 61–68. [Google Scholar] [CrossRef]
- James, E.G.; Steven, B.H.; Bernadette, B.-A.; Ruud, M.B.; Felix, K.; Thomas, G.P.; Andrew, G.R.; Gary, K.Z.; Dolores, M. Short sleep duration as a risk factor for hypertension: Analyses of the first national health and nutrition examination survey. Hypertension 2006, 47, 833–839. [Google Scholar] [CrossRef]
- Choi, D.-W.; Chun, S.-Y.; Lee, S.A.; Han, K.-T.; Park, E.-C. Association between sleep duration and perceived stress: Salaried worker in circumstances of high workload. Int. J. Environ. Res. Public Health 2018, 15, 796. [Google Scholar] [CrossRef]
- Luenda, E.C.; James, E.S.; Anna, M.; Claudia, M.; John, M.V.; Desta, F.; Michael, E.A.; Bryan, J.V.; Cecil, M.B. Association of perceived stress with sleep duration and sleep quality in police officers. Int. J. Emerg. Ment. Health 2011, 13, 229–241. [Google Scholar]
- Wu, Z.H.; Stevens, R.G.; Tennen, H.; North, C.S.; Grady, J.J.; Holzer, C. Sleep quality among low-income young women in southeast Texas predicts changes in perceived stress through hurricane Ike. Sleep 2015, 38, 1121–1128. [Google Scholar] [CrossRef]
- Herawati, K.; Gayatri, D. The correlation between sleep quality and levels of stress among students in Universitas Indonesia. Enferm. Clínica 2019, 29, 357–361. [Google Scholar] [CrossRef]
- Taylor, N.D.; Fireman, G.D.; Levin, R. Trait hostility, perceived stress, and sleep quality in a sample of normal sleepers. Sleep Disord. 2013, 2013, 735812. [Google Scholar] [CrossRef] [PubMed]
- Eliasson, A.H.; Kashani, M.; Mayhew, M.; Ude, A.; Hoffman, J.; Vernalis, M. Reducing perceived stress improves sleep quality: A longitudinal outcomes study. CHEST 2010, 138, 913A. [Google Scholar] [CrossRef]
- Oh, C.-M.; Kim, H.Y.; Na, H.K.; Cho, K.H.; Chu, M.K. The effect of anxiety and depression on sleep quality of individuals with high risk for insomnia: A population-based study. Front. Neurol. 2019, 10, 849. [Google Scholar] [CrossRef] [PubMed]
- Ramsawh, H.J.; Stein, M.B.; Belik, S.-L.; Jacobi, F.; Sareen, J. Relationship of anxiety disorders, sleep quality, and functional impairment in a community sample. J. Psychiatr. Res. 2009, 43, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Zhang, Q.; Du, Y.; Ye, Y.; He, Q. Associations of physical activity, screen time with depression, anxiety and sleep quality among Chinese college freshmen. PLoS ONE 2014, 9, e100914. [Google Scholar] [CrossRef]
- Lazanis, R.S. Stress and emotion, a new synthesis. J. Psychiatr. Ment. Health Nurs. 1999, 6, 410–411. [Google Scholar] [CrossRef]
- Harvey, A.G. A cognitive model of insomnia. Behav. Res. Ther. 2002, 40, 869–893. [Google Scholar] [CrossRef]
- Yang, Y.; Cao, S.; Shields, G.S.; Teng, Z.; Liu, Y. The relationships between rumination and core executive functions: A meta-analysis. Depress. Anxiety 2017, 34, 37–50. [Google Scholar] [CrossRef]
- Pillai, V.; Steenburg, L.A.; Ciesla, J.A.; Roth, T.; Drake, C.L. A seven day actigraphy-based study of rumination and sleep disturbance among young adults with depressive symptoms. J. Psychosom. Res. 2014, 77, 70–75. [Google Scholar] [CrossRef]
- Carney, C.E.; Harris, A.L.; Moss, T.G.; Edinger, J.D. Distinguishing rumination from worry in clinical insomnia. Behav. Res. Ther. 2010, 48, 540–546. [Google Scholar] [CrossRef]
- Lamis, D.A.; Hirsch, J.K.; Pugh, K.C.; Topciu, R.; Nsamenang, S.A.; Goodman, A.; Duberstein, P.R. Perceived cognitive deficits and depressive symptoms in patients with multiple sclerosis: Perceived stress and sleep quality as mediators. Mult. Scler. Relat. Disord. 2018, 25, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Ana, P.A.; Maria, J.S.; Ana, M.P.; Ana, T.P.; Nuno, M.; Sandra, C.B.; Mariana, M.; Carolina, R.; António, M. Sleep difficulties in college students: The role of stress, affect and cognitive processes. Psychiatry Res. 2018, 260, 331–337. [Google Scholar] [CrossRef]
- Zoccola, P.M.; Dickerson, S.S.; Lam, S. Rumination predicts longer sleep onset latency after an acute psychosocial stressor. Psychosom. Med. 2009, 71, 771–775. [Google Scholar] [CrossRef] [PubMed]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The construct of resilience: A critical evaluation and guidelines for future work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef]
- Carver, C.S. Resilience and thriving: Issues, models, and linkages. J. Soc. Issues 1998, 54, 245–266. [Google Scholar] [CrossRef]
- Wingo, A.P.; Wrenn, G.; Pelletier, T.; Gutman, A.R.; Bradley, B.; Ressler, K.J. Moderating effects of resilience on depression in individuals with a history of childhood abuse or trauma exposure. J. Affect. Disord. 2010, 126, 411–414. [Google Scholar] [CrossRef]
- Kalangestani, P.Z.; Faghirpoor, M. The relationship between psychological resilience and rumination with coping skills among the adolescents in the care centers affiliated to guilan welfare organziation. Int. J. Humanit. Cult. Stud. 2016, 0, 735–745. [Google Scholar]
- Li, T.; Liu, T.; Han, J.; Zhang, M.; Li, Z.; Zhu, Q.; Wang, A. The relationship among resilience, rumination and posttraumatic growth in hemodialysis patients in North China. Psychol. Health Med. 2018, 23, 442–453. [Google Scholar] [CrossRef]
- Pietrzak, R.H.; Johnson, D.C.; Goldstein, M.B.; Malley, J.C.; Southwick, S.M. Psychological resilience and postdeployment social support protect against traumatic stress and depressive symptoms in soldiers returning from Operations Enduring Freedom and Iraqi Freedom. Depress. Anxiety 2019, 26, 745–751. [Google Scholar] [CrossRef]
- Houpy, J.C.; Lee, W.W.; Woodruff, J.N.; Pincavage, A.T. Medical student resilience and stressful clinical events during clinical training. Med. Educ. Online 2017, 22, 1320187. [Google Scholar] [CrossRef]
- Skrove, M.; Romundstad, P.; Indredavik, M.S. Resilience, lifestyle and symptoms of anxiety and depression in adolescence: The Young-HUNT study. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 407–416. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, D.P. Integrating mediators and moderators in research design. Res. Soc. Work Pract. 2011, 21, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.S.; West, S.G.; Reno, R.R. Multiple Regression: Testing and Interpreting Interactions; SAGE: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- Brown, S.; Kafka, A.C. Covid-19 has worsened the student mental-health crisis. Can resilience training fix it? In The Chronicle of Higher Education; The Chronicle of Higher Education Inc.: Washington, DC, USA, 2020. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis, Second Edition: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Neria, Y.; Nandi, A.; Galea, S. Post-traumatic stress disorder following disasters: A systematic review. Psychol. Med. 2008, 38, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.T.F.; Yang, X.; Tsui, H.Y.; Kim, J.H. Impacts of SARS on health-seeking behaviors in general population in Hong Kong. Prev. Med. 2005, 41, 454–462. [Google Scholar] [CrossRef]
- Lau, J.T.F.; Yang, X.; Tsui, H.Y.; Pang, E.; Wing, Y.K. Positive mental health-related impacts of the SARS epidemic on the general public in Hong Kong and their associations with other negative impacts. J. Infect. 2006, 53, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, M.L.; Lai-Ming, H.; Steve, K.K.C.; Sai-Yin, H.; John, B.-S.; Ray, Y.L.C.; Anthony, J.H.; Tai-Hing, L.; Richard, F. Longitudinal assessment of community psychobehavioral responses during and after the 2003 outbreak of severe acute respiratory syndrome in Hong Kong. Clin. Infect. Dis. 2005, 40, 1713–1720. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Becker, S.P.; Jarrett, M.A.; Luebbe, A.M.; Garner, A.A.; Burns, G.L.; Kofler, M.J. Sleep in a large, multi-university sample of college students: Sleep problem prevalence, sex differences, and mental health correlates. Sleep Health 2018, 4, 174–181. [Google Scholar] [CrossRef]
- 2017_CCMH_Report-1r4m88x.pdf. Available online: https://ccmh.psu.edu/files/2018/02/2017_CCMH_Report-1r4m88x.pdf (accessed on 28 June 2020).
- Chang, A.K.; Choi, J. Predictors of sleep quality among young adults in Korea: Gender differences. Issues Ment. Health Nurs. 2016, 37, 918–928. [Google Scholar] [CrossRef]
- Jue, C.; Zhen, W.; Boliang, G.; Jon, A.; Haiyin, Z.; Xiuzhen, J.; Yong, X.; Jianyin, Q.; Zeping, X.; Min, Y. Negative affect mediates effects of psychological stress on disordered eating in young Chinese women. PLoS ONE 2012, 7, e46878. [Google Scholar] [CrossRef]
- Lemma, S.; Gelaye, B.; Berhane, Y.; Worku, A.; Williams, M.A. Sleep quality and its psychological correlates among university students in Ethiopia: A cross-sectional study. BMC Psychiatry 2012, 12, 237. [Google Scholar] [CrossRef] [PubMed]
- Di Benedetto, M.; Towt, C.J.; Jackson, M.L. A cluster analysis of sleep quality, self-care behaviors, and mental health risk in australian university students. Behav. Sleep Med. 2020, 18, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Student_wellbeing_report_28052019_DEF.pdf. Available online: https://ris.utwente.nl/ws/portalfiles/portal/172853563/Student_wellbeing_report_28052019_DEF.pdf (accessed on 28 June 2020).
- Kecklund, G.; Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ 2016, 355, i5210. [Google Scholar] [CrossRef] [PubMed]
- Augner, C. Associations of subjective sleep quality with depression score, anxiety, physical symptoms and sleep onset latency in young students. Cent. Eur. J. Public Health 2011, 19, 115–117. [Google Scholar] [CrossRef]
- John, U.; Meyer, C.; Rumpf, H.-J.; Hapke, U. Relationships of psychiatric disorders with sleep duration in an adult general population sample. J. Psychiatr. Res. 2005, 39, 577–583. [Google Scholar] [CrossRef]
- Chiara, B.; Gemma, B.; Bernd, F.; Kai, S.; Christoph, N.; Ulrich, V.; Caterina, L.; Dieter, R. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef]
- Neckelmann, D.; Mykletun, A.; Dahl, A.A. Chronic insomnia as a risk factor for developing anxiety and depression. Sleep 2007, 30, 873–880. [Google Scholar] [CrossRef]
- Ford, D.E.; Kamerow, D.B. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA 1989, 262, 1479–1484. [Google Scholar] [CrossRef]
- Fatima, W.; Shahid, A.; Imran, M.; Manzoor, J.; Hasnain, S.; Rana, S.; Mahmood, S. Leptin deficiency and leptin gene mutations in obese children from Pakistan. Int. J. Pediatr. Obes. 2011, 6, 419–427. [Google Scholar] [CrossRef]
- Alice, J.C.; Paula, S.; Theis, L.; Poul, J.; Marianna, V.; Jaana, P.; Mika, K.; Naja, H.R.; Jussi, V. Onset of impaired sleep and cardiovascular disease risk factors: A longitudinal study. Sleep 2016, 39, 1709–1718. [Google Scholar] [CrossRef]
- Anothaisintawee, T.; Reutrakul, S.; van Cauter, E.; Thakkinstian, A. Sleep disturbances compared to traditional risk factors for diabetes development: Systematic review and meta-analysis. Sleep Med. Rev. 2016, 30, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Slavish, D.C.; Graham-Engeland, J.E. Rumination mediates the relationships between depressed mood and both sleep quality and self-reported health in young adults. J. Behav. Med. 2015, 38, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Buboltz, W.C., Jr.; Brown, F.M.A.; Soper, B. Sleep habits and patterns of college students: A preliminary study. J. Am. Coll. Health 2001, 50, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Querstret, D.; Cropley, M. Assessing treatments used to reduce rumination and/or worry: A systematic review. Clin. Psychol. Rev. 2013, 33, 996–1009. [Google Scholar] [CrossRef]
- De Bruin, E.J.; Bögels, S.M.; Oort, F.J.; Meijer, A.M. Efficacy of cognitive behavioral therapy for iInsomnia in adolescents: A randomized controlled trial with internet therapy, group therapy and a waiting list condition. Sleep 2015, 38, 1913–1926. [Google Scholar] [CrossRef]
- Liu, X.; Liu, C.; Tian, X.; Zou, G.; Li, G.; Kong, L.; Li, P. Associations of perceived stress, resilience and social support with sleep disturbance among community-dwelling adults. Stress Health 2016, 32, 578–586. [Google Scholar] [CrossRef]
- Prichard, J.R.; Hartmann, M.E. Follow-up to Hartmann & Prichard: Should universities invest in promoting healthy sleep? A question of academic and economic significance. Sleep Health 2019, 5, 320–325. [Google Scholar] [CrossRef]
- Friedrich, A.; Schlarb, A.A. Let’s talk about sleep: A systematic review of psychological interventions to improve sleep in college students. J. Sleep Res. 2018, 27, 4–22. [Google Scholar] [CrossRef]
- Bowen, L. Assessing the effectiveness of online cognitive behavioral therapy in adults with chronic insomnia: A systematic review and meta-analysis. Lynchburg J. Med. Sci. 2019, 1, 6. Available online: https://digitalshowcase.lynchburg.edu/dmscjournal/vol1/iss3/6 (accessed on 28 June 2020).
- Shatkin, J.P.; Diamond, U.; Zhao, Y.; DiMeglio, J.; Chodaczek, M.; Bruzzese, J.-M. Effects of a risk and resilience course on stress, coping skills, and cognitive strategies in college students. Teach. Psychol. 2016, 43, 204–210. [Google Scholar] [CrossRef]
- Julieta, G.; Géraldine, D.; Maris, V.; Adam, P.W.; Jan, S.; Alice, B.; Neal, L.; Emma, H.; Prof, P.B.J. A mindfulness-based intervention to increase resilience to stress in university students (the Mindful Student Study): A pragmatic randomised controlled trial. Lancet Public Health 2018, 3, e72–e81. [Google Scholar] [CrossRef]
- Sevilla-Llewellyn-Jones, J.; Santesteban-Echarri, O.; Pryor, I.; McGorry, P.; Alvarez-Jimenez, M. Web-based mindfulness interventions for mental health treatment: Systematic review and meta-analysis. JMIR Ment. Health 2018, 5, e10278. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, P.M.; Mahoney, A.E.J.; Moulds, M.L. Are worry, rumination, and post-event processing one and the same? Development of the repetitive thinking questionnaire. J. Anxiety Disord. 2010, 24, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Sohn, S.I.; Kim, D.H.; Lee, M.Y.; Cho, Y.W. The reliability and validity of the korean version of the pittsburgh sleep quality index. Sleep Breath. 2012, 16, 803–812. [Google Scholar] [CrossRef] [PubMed]
- Mervosh, S.; Lee, J.C.; Gamio, L.; Popovich, N. See how all 50 states are reopening. In The New York Times; The New York Times Company: New York, NY, USA, 2020. [Google Scholar]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Wolf, E.J.; Harrington, K.M.; Clark, S.L.; Miller, M.W. Sample size requirements for structural equation models: An evaluation of power, bias, and solution propriety. Educ. Psychol. Meas. 2013, 76, 913–934. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef]
- Hayes, A.F. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation and Conditional Process Modeling [White Paper]. 2012. Available online: http://www.afhayes.com/public/process2012.pdf (accessed on 28 June 2020).
- Potthoff, R.F. On the Johnson-Neyman technique and some extensions thereof. Psychometrika 1964, 29, 241–256. [Google Scholar] [CrossRef]


{kind=link}
| Location | Social Restriction Measures in Place | Sex n (%) | Undergraduate vs. Graduate n (%) | Domestic vs. International n (%) |
|---|---|---|---|---|
| China | Some online classes and some in-person classes resumed | M = 36 (32.4) F = 75 (67.6) Other = 0 | U = 94 (84.7) G = 17 (15.3) | D = 106 (95.5) I = 5 (4.5) |
| Ireland | Online classes only | M = 53 (27.6) F = 138 (71.9) Other = 1 (0.5) | U = 154 (80.2) G = 38 (19.8) | D = 179 (93.2) I = 13 (6.8) |
| Malaysia | Online classes only | M = 19 (20.9) F = 72 (79.1) Other = 0 | U = 88 (96.7) G = 3 (3.3) | D = 74 (81.3) I = 17 (18.7) |
| South Korea | Some online classes and some in-person classes resumed | M = 54 (60.7) F = 35 (39.3) Other = 0 | U = 41(46.1) G = 48 (53.9) | D = 84 (94.4) I = 5 (5.6) |
| Taiwan | Some online classes and some in-person classes resumed | M = 202 (53.6) F = 155 (41.1) Other = 20 (5.3) | U = 360 (95.5) G = 17 (4.5) | D = 360 (95.5) I = 17 (4.5) |
| The Netherlands | Online classes only | M = 22 (19.3) F = 92 (80.7) Other = 0 | U = 114 (100) G = 0 | D = 46 (40.4) I = 68 (59.6) |
| United States | Online classes only | M = 308 (24.1) F = 935 (73.0) Other = 37 (2.0) | U = 951 (74.3) G = 327 (25.7) | D = 1113 (87.0) I = 167 (13) |
| Total | M = 694 (30.8) F = 1502 (66.7) Other = 58 (2.5) Total = 2254 | U = 1802 (79.9) G = 452 (20.1) | D = 1962 (87.0) I = 292 (13.0) |
| Health Parameters | Category | n (%) |
|---|---|---|
| Anxiety | Minimal anxiety | 711 (31.6) |
| Mild anxiety | 722 (32.0) | |
| Moderate anxiety | 456 (20.2) | |
| Severe anxiety | 364 (16.2) | |
| Perceived stress | Low stress | 337 (15.0) |
| Moderate stress | 1425 (63.2) | |
| High stress | 492 (21.8) | |
| Sleep quality * | Good sleeper | 890 (39.7) |
| Poor sleeper | 1352 (60.3) | |
| Sleep duration | Met ≥ 7 h of sleep per day | 1628 (72.2) |
| Did not meet the above sleep duration recommendation | 626 (27.8) |
| n | Greater Perceived Stress (%) | Greater Financial Stress (%) | Reduced Resilience to Stress (%) | Greater Repetitive Negative Thinking (%) | Greater Negative Mood (%) | Greater * Anxiety (%) | Reduced Sleep Duration (%) | Increased Sleep Duration (%) | Reduced Sleep Quality (%) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Total | 2254 | 60.2 | 41.7 | 29.5 | 50.1 | 50.9 | 63.9 | 17.1 | 44.6 | 32.1 |
| Undergraduate | 1802 | 59.3 | 41.6 | 29.9 | 50.0 | 50.6 | 64.3 | 17.5 | 44.9 | 32.2 |
| Graduate | 452 | 63.7 | 42.0 | 28.1 | 50.4 | 52.2 | 62.8 | 15.5 | 44.0 | 31.6 |
| Domestic | 1962 | 60.2 | 40.9 | 29.3 | 49.3 | 51.0 | 64.0 | 16.8 | 44.2 | 31.3 |
| International | 292 | 59.6 | 46.9 | 30.8 | 55.1 | 50.0 | 62.9 | 19.2 | 47.3 | 37.3 |
| Measures a | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| (1) Sleep quality (PSQI) b | - | −0.33 * | −0.28 * | 0.41 * | 0.43 * | −0.50 * | 0.04 | 0.19 * |
| (2) Sleep duration (hours) | - | 0.05 | −0.05 | −0.05 | −0.08 * | −0.11 * | −0.07 * | |
| (3) Resilience | - | −0.47 * | −0.50 * | −0.42 * | 0.09 * | −0.27 | ||
| (4) Rumination | - | 0.62 * | 0.67 * | −0.09 * | 0.09 * | |||
| (5) Perceived stress | - | 0.69 * | −0.12 * | 0.10 * | ||||
| (6) Anxiety | − | −0.05 | 0.16 * | |||||
| (7) Age (years) | - | 0.19 * | ||||||
| (8) BMI (Kg/m2) | - | |||||||
| Mean ± SD | 6.8 ± 3.5 | 7.5 ± 1.2 | 3.2 ± 0.7 | 82.9 ± 23.0 | 20.6 ± 6.8 | 8.2 ± 5.8 | 22.5 ± 5.5 | 24.4 ± 5.6 |
| Variables | B | SE | t | p Value |
|---|---|---|---|---|
| Perceived stress → rumination | 2.04 | 0.05 | 37.90 | <0.001 |
| Rumination → sleep quality | 0.01 | 0.02 | 0.75 | 0.46 |
| Perceived stress → sleep quality | 0.35 | 0.06 | 5.91 | <0.001 |
| Bootstrap | Effect | SE | LL 95% CI | UL 95% CI |
| Rumination | 0.06 | 0.01 | 0.05 | 0.08 |
| Variables | B | SE | t | p Value |
|---|---|---|---|---|
| Resilience → sleep quality | 0.69 | 0.36 | 1.89 | 0.06 |
| Interaction 1 → sleep quality | −0.06 | 0.02 | −3.68 | <0.001 |
| Interaction 2 → sleep quality | 0.01 | 0.01 | 1.03 | 0.30 |
| Conditional indirect effect of resilience | Resilience scores | Indirect effect (SE) | LL 95% CI | UL 95% CI |
| 2.46 | 0.19 (0.02) | 0.15 | 0.23 | |
| 3.18 | 0.14 (0.01) | 0.12 | 0.17 | |
| 3.90 | 0.10 (0.02) | 0.06 | 0.13 | |
| Conditional direct effect of resilience Johnson-Neyman test | Resilience scores | Direct effect (SE) | LL 95% CI | UL 95% CI |
| 1.00 | 0.29 (0.04) | 0.05 | 0.08 | |
| 1.80 | 0.23 (0.03) | 0.18 | 0.29 | |
| 2.60 | 0.18 (0.02) | 0.15 | 0.22 | |
| 3.40 | 0.13 (0.01) | 0.10 | 0.16 | |
| 4.20 | 0.08 (0.02) | 0.04 | 0.12 | |
| 4.40 | 0.07 (0.02) | 0.02 | 0.11 | |
| 4.61 | 0.05 (0.03) | 0.00 | 0.10 | |
| 4.80 | 0.04 (0.03) | −0.02 | 0.10 | |
| 5.00 | 0.03 (0.03) | −0.04 | 0.09 |
| Variables | B | SE | t | p Value |
|---|---|---|---|---|
| Perceived stress → rumination | 2.04 | 0.05 | 37.90 | <0.001 |
| Rumination → sleep duration | 0.01 | 0.01 | 1.14 | 0.25 |
| Perceived stress → sleep duration | −0.03 | 0.02 | −1.08 | 0.28 |
| Bootstrap | Effect | SE | LL 95% CI | UL 95% CI |
| Rumination | −0.002 | 0.003 | −0.01 | 0.001 |
| Variables | B | SE | t | p Value |
|---|---|---|---|---|
| Resilience → sleep duration | 0.21 | 0.16 | 1.34 | 0.18 |
| Interaction 1 → sleep duration | 0.01 | 0.01 | 0.83 | 0.40 |
| Interaction 2 → sleep duration | −0.003 | 0.002 | −1.38 | 0.17 |
| Conditional indirect effect of resilience | Resilience scores | Indirect effect (SE) | LL 95% CI | UL 95% CI |
| 2.46 | 0.002 (0.005) | −0.008 | 0.012 | |
| 3.18 | −0.002 (0.003) | −0.008 | 0.004 | |
| 3.90 | −0.007 (0.004) | −0.015 | 0.001 | |
| Conditional direct effect of resilience | Resilience scores | Direct effect (SE) | LL 95% CI | UL 95% CI |
| 2.46 | −0.011 (0.008) | −0.027 | 0.004 | |
| 3.18 | −0.007 (0.005) | −0.017 | 0.003 | |
| 3.90 | −0.003 (0.007) | −0.016 | 0.011 |
| Variables | B | SE | t | p Value |
|---|---|---|---|---|
| Anxiety → rumination | 2.60 | 0.06 | 41.23 | <0.001 |
| Rumination → sleep quality | 0.01 | 0.02 | 0.78 | 0.43 |
| Anxiety → sleep quality | 0.35 | 0.07 | 5.03 | <0.001 |
| Bootstrap | Effect | SE | LL 95% CI | UL 95% CI |
| Rumination | 0.05 | 0.01 | 0.03 | 0.07 |
| Variables | B | SE | t | p Value |
|---|---|---|---|---|
| Resilience → sleep quality | −0.13 | 0.36 | −0.36 | 0.72 |
| Interaction 1 → sleep quality | −0.04 | 0.02 | −1.88 | 0.06 |
| Interaction 2 → sleep quality | 0.002 | 0.005 | −1.88 | 0.73 |
| Conditional indirect effect of resilience | Resilience scores | Indirect effect (SE) | LL 95% CI | UL 95% CI |
| 2.46 | 0.05 (0.01) | 0.02 | 0.07 | |
| 3.18 | 0.05 (0.01) | 0.03 | 0.07 | |
| 3.90 | 0.05 (0.01) | 0.03 | 0.08 | |
| Conditional direct effect of resilience | Resilience scores | Direct effect (SE) | LL 95% CI | UL 95% CI |
| 2.46 | 0.25 (0.02) | 0.21 | 0.29 | |
| 3.18 | 0.22 (0.02) | 0.19 | 0.25 | |
| 3.90 | 0.19 (0.02) | 0.15 | 0.24 | |
| Conditional direct effect of resilience Johnson-Neyman test | Resilience scores | Direct effect (SE) | LL 95% CI | UL 95% CI |
| 1.00 | 0.31 (0.05) | 0.21 | 0.40 | |
| 1.80 | 0.28 (0.03) | 0.21 | 0.34 | |
| 2.60 | 0.24 (0.02) | 0.21 | 0.28 | |
| 3.40 | 0.21 (0.02) | 0.18 | 0.24 | |
| 4.20 | 0.18 (0.03) | 0.14 | 0.23 | |
| 4.40 | 0.17 (0.03) | 0.11 | 0.23 | |
| 4.60 | 0.16 (0.03) | 0.10 | 0.23 | |
| 5.00 | 0.15 (0.04) | 0.06 | 0.23 |
| Variables | B | SE | t | p Value |
|---|---|---|---|---|
| Anxiety → rumination | 2.61 | 0.06 | 41.24 | <0.001 |
| Rumination → sleep duration | 0.01 | 0.01 | 1.00 | 0.32 |
| Anxiety → sleep duration | −0.02 | 0.03 | −0.75 | 0.45 |
| Bootstrap | Effect | SE | LL 95% CI | UL 95% CI |
| Rumination | 0.001 | 0.004 | −0.007 | 0.009 |
| Variables | B | SE | t | p Value |
|---|---|---|---|---|
| Resilience → sleep duration | 0.26 | 0.17 | 1.55 | 0.12 |
| Interaction 1 → sleep duration | 0.002 | 0.010 | 0.19 | 0.85 |
| Interaction 2 → sleep duration | −0.002 | 0.003 | −1.00 | 0.32 |
| Conditional indirect effect of resilience | Resilience scores | Indirect effect (SE) | LL 95% CI | UL 95% CI |
| 2.46 | 0.006 (0.007) | −0.007 | 0.019 | |
| 3.18 | 0.001 (0.004) | −0.007 | 0.009 | |
| 3.90 | −0.004 (0.006) | −0.015 | 0.008 | |
| Conditional direct effect of resilience | Resilience scores | Direct effect (SE) | LL 95% CI | UL 95% CI |
| 2.46 | −0.019 (0.009) | −0.036 | −0.001 | |
| 3.18 | −0.017 (0.006) | −0.029 | −0.005 | |
| 3.90 | −0.016 (0.010) | −0.035 | 0.003 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, C.; Zan, M.C.H.; Cho, M.J.; Fenton, J.I.; Hsiao, P.Y.; Hsiao, R.; Keaver, L.; Lai, C.-C.; Lee, H.; Ludy, M.-J.; et al. Increased Resilience Weakens the Relationship between Perceived Stress and Anxiety on Sleep Quality: A Moderated Mediation Analysis of Higher Education Students from 7 Countries. Clocks & Sleep 2020, 2, 334-353. https://doi.org/10.3390/clockssleep2030025
Du C, Zan MCH, Cho MJ, Fenton JI, Hsiao PY, Hsiao R, Keaver L, Lai C-C, Lee H, Ludy M-J, et al. Increased Resilience Weakens the Relationship between Perceived Stress and Anxiety on Sleep Quality: A Moderated Mediation Analysis of Higher Education Students from 7 Countries. Clocks & Sleep. 2020; 2(3):334-353. https://doi.org/10.3390/clockssleep2030025
Chicago/Turabian StyleDu, Chen, Megan Chong Hueh Zan, Min Jung Cho, Jenifer I. Fenton, Pao Ying Hsiao, Richard Hsiao, Laura Keaver, Chang-Chi Lai, HeeSoon Lee, Mary-Jon Ludy, and et al. 2020. "Increased Resilience Weakens the Relationship between Perceived Stress and Anxiety on Sleep Quality: A Moderated Mediation Analysis of Higher Education Students from 7 Countries" Clocks & Sleep 2, no. 3: 334-353. https://doi.org/10.3390/clockssleep2030025
APA StyleDu, C., Zan, M. C. H., Cho, M. J., Fenton, J. I., Hsiao, P. Y., Hsiao, R., Keaver, L., Lai, C.-C., Lee, H., Ludy, M.-J., Shen, W., Swee, W. C. S., Thrivikraman, J., Tseng, K.-W., Tseng, W.-C., & Tucker, R. M. (2020). Increased Resilience Weakens the Relationship between Perceived Stress and Anxiety on Sleep Quality: A Moderated Mediation Analysis of Higher Education Students from 7 Countries. Clocks & Sleep, 2(3), 334-353. https://doi.org/10.3390/clockssleep2030025