
Health and Heritage: The Bioarchaeological Discovery of a Probable Case of Developmental Dysplasia in an Adult Subject


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials
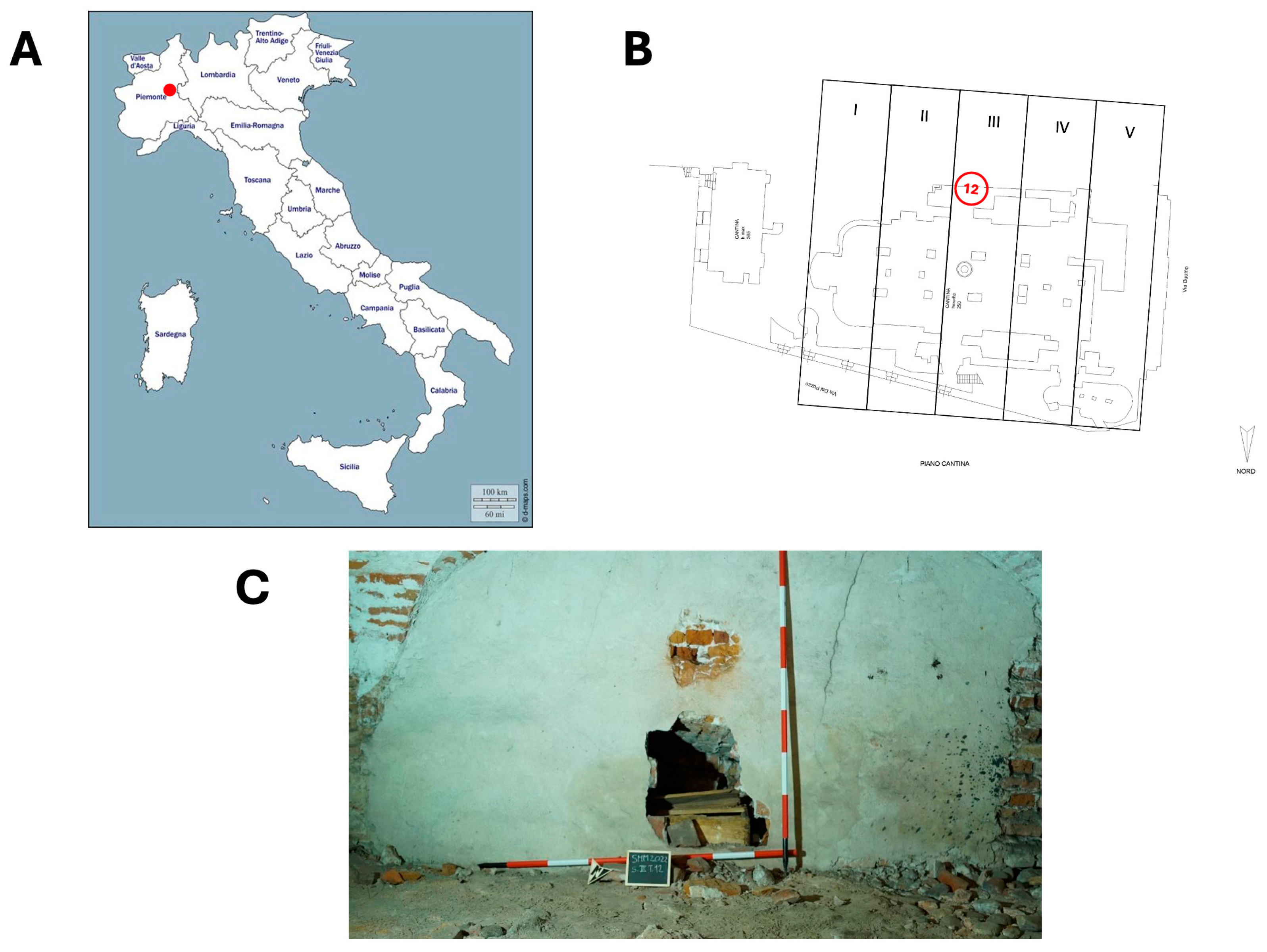
2.1. The Burial Site
2.2. Sector III, Funerary Unit 12
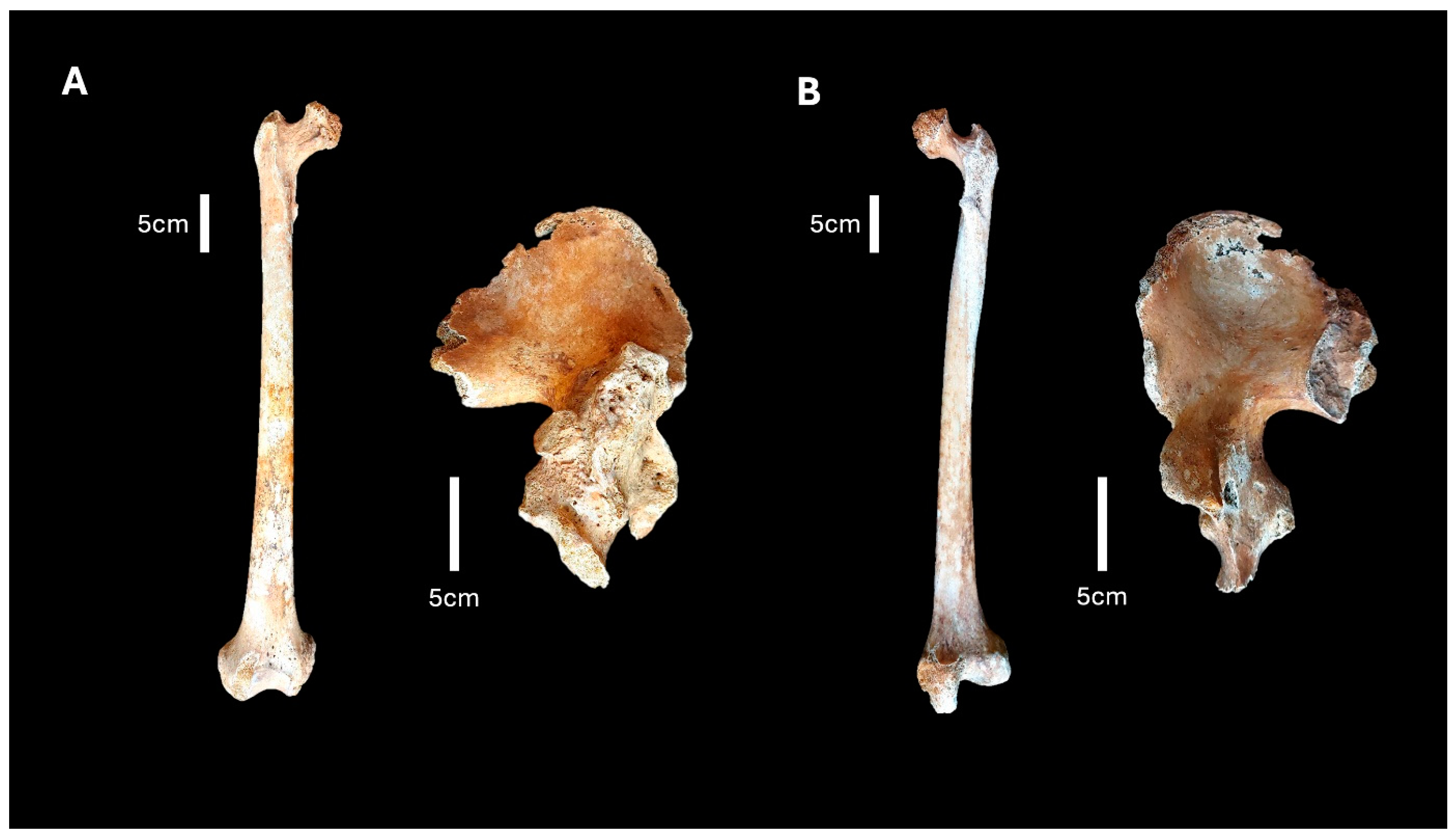
2.3. FU12 151
3. Methods
Radiographic Analyses
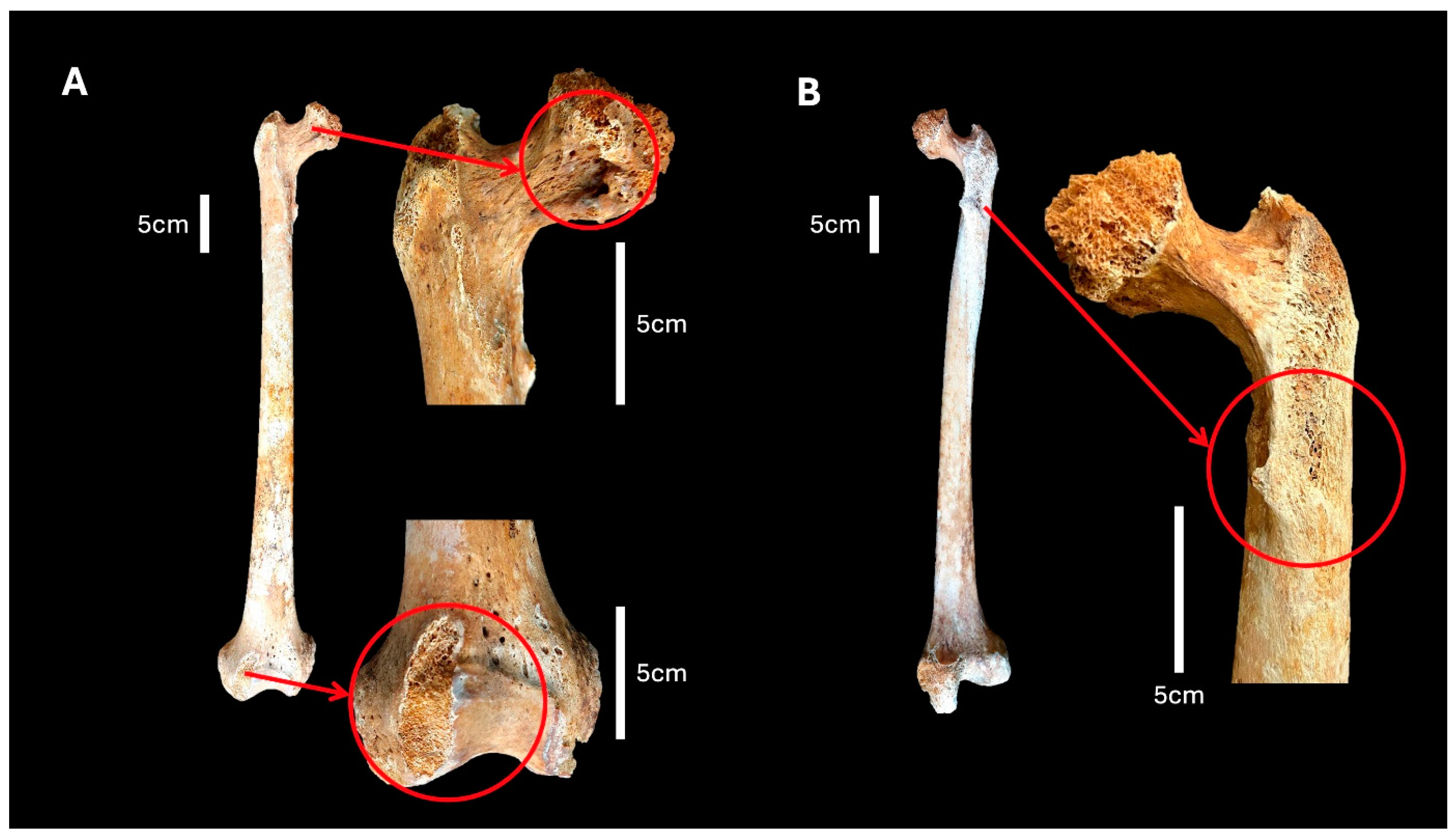
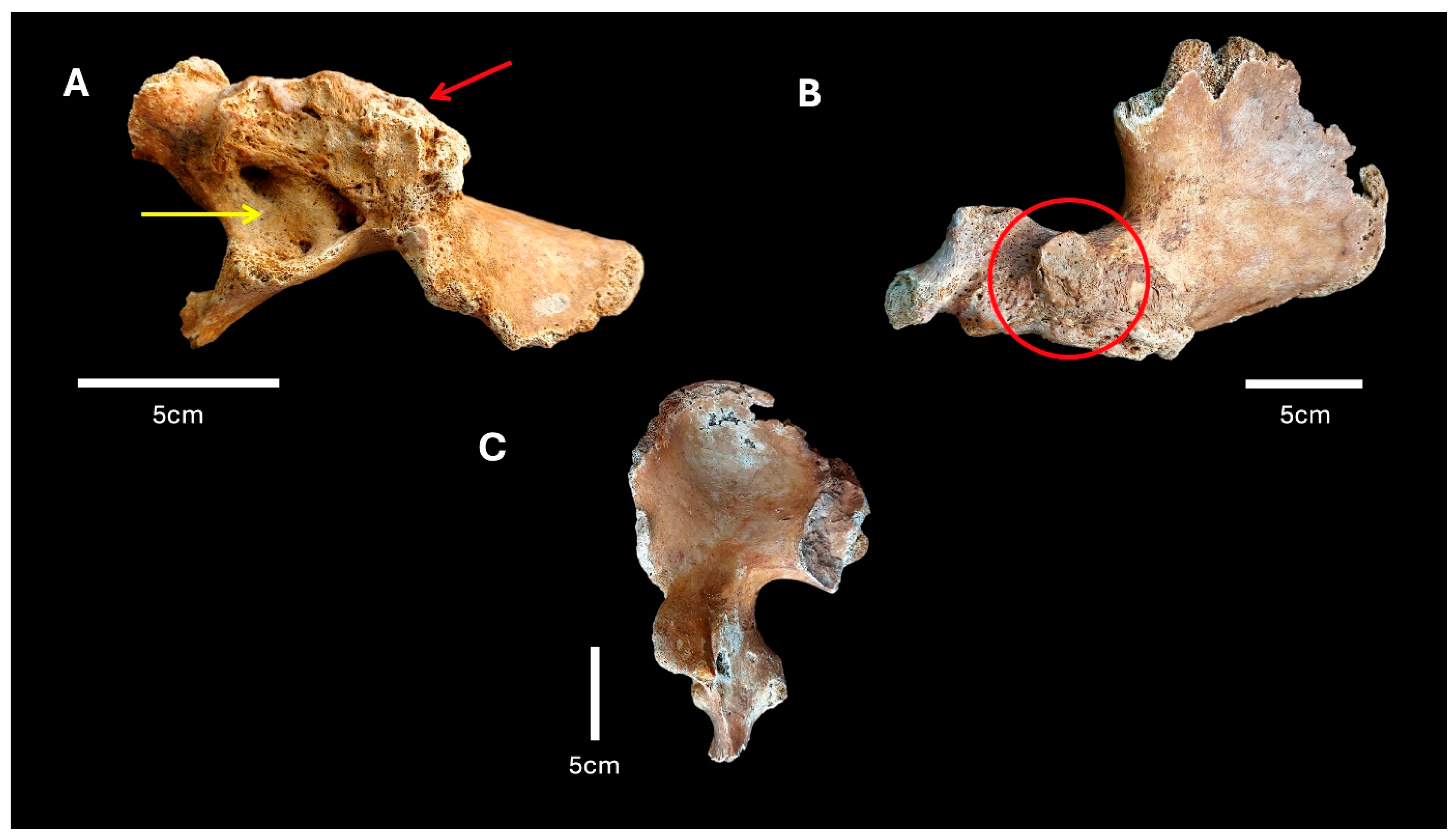
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Waldron, T. Paleopathology; Cambridge University Press: Cambridge, UK, 2020. [Google Scholar] [CrossRef]
- Roberts, C.A.; Manchester, K.L. The Archaeology of Disease, 2nd ed.; Cornell University Press: Ithaca, NY, USA, 1997; 243p, ISBN 080148440. [Google Scholar]
- Larsen, C.S. Bioarchaeology: Interpreting Behavior from the Human Skeleton, 2nd ed.; Part of Cambridge Studies in Biological and Evolutionary Anthropology; Cambridge University Press: Cambridge, UK, 2015. [Google Scholar]
- Auferhede, A.C.; Rodriguez-Martin, C. The Cambridge Encyclopedia of Human Paleopathology. Arthur C. Auferhede and Conrado Rodriguez-Martin, including a dental chapter by Odin Langsjoen. 1998. Cambridge University Press, England, xviii + 478 pp., 310 figures, references, index. $100.00 (cloth), ISBN 0-521-55203-6. Am. Antiq. 1999, 64, 562–563. [Google Scholar] [CrossRef]
- Ibrahim, M.M.; Smit, K. Anatomical Description and Classification of Hip Dysplasia. In Hip Dysplasia; Beaulé, P., Ed.; Springer: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Harsanyi, S.; Zamborsky, R.; Krajciova, L.; Kokavec, M.; Danisovic, L. Developmental Dysplasia of the Hip: A Review of Etiopathogenesis, Risk Factors, and Genetic Aspects. Medicina 2020, 56, 153. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sonoda, K.; Hara, T. “Anterior-shift sign”: A novel MRI finding of adult hip dysplasia. Arch. Orthop. Trauma Surg. 2022, 142, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Marras, F.; Asti, C.; Ciatti, C.; Pescia, S.; Locci, C.; Pisanu, F.; Doria, C.; Caggiari, G. Congenital hip dysplasia: The importance of early screening and treatment. Pediatr. Med. Chir. 2022, 44. [Google Scholar] [CrossRef] [PubMed]
- Plischuk, M.; De Feo, M.E.; Desántolo, B. Developmental dysplasia of the hip in female adult individual: Site Tres Cruces I, Salta, Argentina (Superior formative period, 400–1000 AD). Int. J. Paleopathol. 2018, 20, 108–113. [Google Scholar] [CrossRef]
- Spasovski, D.D. Introductory chapter: Five-dimensional approach to the developmental dysplasia of the hip. In Developmental Diseases of the Hip-Diagnosis and Management; Spasovski, D., Ed.; InTech: Takasago, Japan, 2017. [Google Scholar] [CrossRef]
- Arnaud, G.; Arnaud, S. Luxation congenital bilatérale de la hanche et manifesta tions d’hyperostose porotique sur un squelette d’époque paléo-chrétienne. Bull. Mém. Soc. Anthropol. Paris 1975, 2, 307–326, (XIII Série, 10.3406/bmsap). [Google Scholar] [CrossRef]
- Blondiaux, J.; Millot, F. Dislocation of the hip: Discussion of eleven cases from medieval France. Int. J. Osteoarchaeol. 1991, 1, 203–207. [Google Scholar] [CrossRef]
- Mafart, B.; Kéfi, R.; Béraud-Colomb, E. Palaeopathological and palaeogenetic study of 13 cases of developmental dysplasia of the hip with dislocation in a historical population from southern France. Int. J. Osteoarchaeol. 2007, 17, 26–38. [Google Scholar] [CrossRef]
- Dawes, J.; Magilton, J. The Cemetery of St. Helen-on-the-Walls, Aldwark. In The Archaeology of York; Council for British archaeology: London, UK, 1980; Volume 12. [Google Scholar]
- Wakely, J. Bilateral congenital dislocation of the hip, spina bifida occulta and spondylosis in a female skeleton from the medieval cemetery at Abingdon. Engl. J. Paleop. 1993, 1, 37–45. [Google Scholar]
- Mitchell, P.; Redfern, R. The prevalence of dislocation in developmental dysplasia of the hip in Britain over the past thousand years. J. Pediatr. Orthop. 2007, 27, 890–892. [Google Scholar] [CrossRef]
- Mitchell, P.; Redfern, R. Diagnostic criteria for developmental dislocation of the hip in human skeletal remains. Int. J. Osteoarchaeol. 2008, 18, 61–71. [Google Scholar] [CrossRef]
- Mitchell, P.; Redfern, R. Brief communication: Developmental dysplasia of the hip in medieval London. Am. J. Phys. Anthropol. 2011, 144, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Agnew, A.; Justus, H. Developmental Dysplasia of the Hip in a Child from Medieval Poland. Poster on 2013 Conference Paleopathology Association. 2013. Available online: http://www.slavia.org/posters/2013_agnew_ddh.pdf (accessed on 10 July 2024).
- Masnicová, S.; Beňuš, R. Developmental anomalies in skeletal remains from the Great Moravia and Middle Ages cemeteries at Devín (Slovakia). Int. J. Osteoarchaeol. 2003, 13, 266–274. [Google Scholar] [CrossRef]
- Eng, J.; Szöcs, P.; Hagen, C. Developmental dysplasia of the hip in a post-medieval Transylvanian population: Case study and diagnosis. Paleopathol. News 2009, 148, 25–32. [Google Scholar]
- Katzmarzyk, C.; Schats, R. Conflicting Pelvic Morphology in a Pathological Late Medieval Skeleton from the Netherlands. Poster on 2011 Conference of British Association for Human Identification (BAHID). 2011. Available online: https://www.academia.edu/3388868/Conflicting_Pelvic_Morphology_in_a_Pathological_Late_Medieval_Skeleton_from_the_Netherlands (accessed on 17 June 2024).
- Petrella, E.; Piciucchi, S.; Feletti, F.; Barone, D.; Piraccini, A.; Minghetti, C.; Gruppioni, G.; Poletti, V.; Bertocco, M.; Traversari, M. CT Scan of thirteen natural mummies dating back to the XVIXVIII centuries: An emerging tool to investigate living condi tions and diseases in history. PLoS ONE 2016, 11, e0154349. [Google Scholar] [CrossRef]
- Traversari, M.; Feletti, F.; Vazzana, A.; Gruppioni, G.; Frelat, M. Three cases of developmental dysplasia of the hip on partially mummified human remains (Roccapelago, Modena, 18th Century): A study of palaeopathological indicators through direct analysis and 3D virtual models. Bull. Mémoires Société Anthropol. Paris 2016, 28, 202–212. [Google Scholar] [CrossRef]
- Blatt, S.H. To swaddle, or not to swaddle? Paleoepidemiology of developmental dysplasia of the hip and the swaddling dilemma among the indigenous populations of North America. Am. J. Hum. Biol. 2015, 27, 116–128. [Google Scholar] [CrossRef] [PubMed]
- Clabeaux, M. Congenital dislocation of the hip in the prehistoric northeast. Bull. N. Y. Acad. Med. 1977, 53, 338–346. [Google Scholar]
- Ausel, E. Down But Not out: A Probable Case of Congenital Hip Dysplasia in a Late Prehistoric Native American Community. Paleopathology Association Scientific Program. In Proceedings of the 43rd Annual North American Meeting, Atlanta, GA, USA, 18–23 October 2016. [Google Scholar]
- Loder, R.T.; Skopelja, E.N. The epidemiology and demographics of hip dysplasia. ISRN Orthop. 2011, 2011, 238607. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Brothwell, D. Major congenital anomalies of the skeleton: Evidence from earlier population. In Diseases in Antiquity; Brothwell, D., Sandison, A., Eds.; Charles Thomas: Springfield, IL, USA, 1967; Chapter 34; pp. 423–443. [Google Scholar]
- Costa, M.; Llagostera, A. Coyo 3: Momentos finales del Período Medio en San Pedro de Atacama. Estud. Atacameños 1994, 11, 73–107. [Google Scholar] [CrossRef]
- Voegt, C.; Gunston, G.; Nortje, M.; Sealy, J.C.; He, L.; Le Roux, P.; Namayega, C.; Gibbon, V.E. Bilateral hip dysplasia in a South African male: A case study from the 17–18th century. Int. J. Paleopathol. 2023, 42, 27–33, ISSN 1879-9817. [Google Scholar] [CrossRef] [PubMed]
- Tibaldeschi, G. La Chiesa di S. Maria Maggiore di Vercelli e l’Assunzione di Paolo Borroni. Boll. Stor. Vercellese 1996, 2, 131–150. [Google Scholar]
- Sommo, G. Vercelli e la Memoria dell’antico. Schede e Documenti per un Approccio Alla Storia ed ai Problemi Dell’archeologia, Della Tutela e Conservazione in un Centro Della Provincia Piemon-Tese. Edizione Elettronica Archeovercelli.it. Gruppo Archeo-Logico Vercellese. Vercelli, Italy. 2008. Available online: http://www.archeovercelli.it/VERCELLI%20E%20LA%20MEMORIA.pdf (accessed on 27 June 2024).
- Caldano, S. Un cantiere per un capitolo canonicale di prestigio: Santa Maria Maggiore di Vercelli nel XII secolo. Arte Lomb. 2019, 186/187, 71–84. [Google Scholar]
- Fusco, R.; Messina, C.; Tesi, C.; Vanni, A. “Capta est ne Malitia Mutaret Intelletum Eius”. Study on a Natural Mummy from an Underground Cemetery (18–19th Century). Med. Hist. 2023, 7, e2023044. Available online: https://mattioli1885journals.com/index.php/MedHistor/article/view/15140 (accessed on 27 June 2024).
- Vanni, A.; Fusco, R.; Tesi, C.; Licata, M. Autopsy or anatomical dissection? Comparative analysis of an osteoarcheological sample from an 18-19th century hypo-geal cemetery (northern Italy). J. Archaeol. Sci. Rep. 2024, 54, 104418. [Google Scholar] [CrossRef]
- Vanni, A.; Fusco, R. Behind the Wall: A Paleopathological Examination of a Non-Adult Subject from the Cemetery of Santa Maria Maggiore, Vercelli. J. Bioarchaeol. Res. 2024, 2, e2024005. Available online: https://www.mattioli1885journals.com/index.php/JBR/article/view/15809 (accessed on 27 June 2024).
- Bettin, S. Archeologia e antropologia fisica a Santa Maria Maggiore di Vercelli [Corso di Laurea Triennale in Lettere]; Università del Piemonte Orientale: Vercelli, Italy, 2022. [Google Scholar]
- Lovejoy, C.O.; Meindl, R.S.; Pryzbeck, T.R.; Mensforth, R.P. Chronological metamorphosis of the auricular surface of the ilium: A new method for the determination of adult skeletal age at death. Am. J. Phys. Anthropol. 1985, 68, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Buikstra, J.E. Standards for data collection from human skeletal remains. Ark. Archaeol. Surv. Res. Ser. 1994, 44, 18. [Google Scholar]
- Phenice, T.W. A newly developed visual method of sexing the os pubis. Am. J. Phys. Anthropol. 1969, 30, 297–301. [Google Scholar] [CrossRef]
- Martin, R.; Saller, K. 1957–1962. Lehrbuch der Anthropologie, Stuttgart. Martin, R., & Saller, K. (1957). Lehrbuch der Anthropologie in Systematischer Darstellung Mit Besonderer Berücksichtigung der Anthropologischen Methoden (Vol. 1). G. Fischer. Available online: https://archive.org/details/lehrbuchderanthr00mart/page/n7/mode/2up (accessed on 27 June 2024).
- Assis, S.; Henderson, C.Y.; Casimiro, S.; Alves Cardoso, F. Is differential diagnosis attainable in disarticulated pathological bone remains? A case-study from a late 19th/early 20th century necropolis from Juncal (Porto de Mós, Portugal). Int. J. Paleopathol. 2018, 20, 26–37. [Google Scholar] [CrossRef]
- Solomon, L.; Ganz, R.; Leunig, M.; Monsell, F.; Learmonth, I. The hip. In Apley’s System of Orthopaedics and Fractures; Solomon, L., Warwick, D., Nayagam, S., Eds.; CRC Press: Boca Raton, FL, USA, 2010; pp. 493–545. [Google Scholar]
- Ortner, D.J. Identification of Pathological Conditions in Human Skeletal Remains, 3rd ed.; Buikstra, J.E., Ed.; Arizona State University: Tempe, AZ, USA, 2019. [Google Scholar]
- Giovagnorio, F. Manuale di Diagnostica per Immagini nella Pratica Medica, 3rd ed.; Società Editrice Esculapio: Bologna, Italy, 2021; p. 384. ISBN 9788893852548. [Google Scholar]
- Fusco, R.; Tesi, C.; Larentis, O. Paleopathological Evidence of Legg-Calve’-Perthes from the Medieval Cemetery of St. Agostino in Caravate, Northwestern Italy. Med. Hist. 2022, 5, e2021025. Available online: https://www.mattioli1885journals.com/index.php/MedHistor/article/view/12735 (accessed on 12 September 2024).
- Meier, M.E.; Appelman-Dijkstra, N.M.; Collins, M.T.; Geels, R.E.S.; Stanton, R.P.; de Witte, P.B.; Boyce, A.M.; van de Sande, M.A.J. Coxa Vara Deformity in Fibrous Dysplasia/McCune-Albright Syndrome: Prevalence, Natural History and Risk Factors: A Two-Center Study. J Bone Miner Res. 2023, 38, 968–975. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Kim, G.K. Chapter 61—Coxa Vara. In High Yield Orthopaedics, 1st ed.; Elsevier Health Sciences Publisher: Amsterdam, The Netherlands, 2010; p. 125. ISBN 9781416002369. [Google Scholar] [CrossRef]
- Gül, D.; Orsçelik, A.; Akpancar, S. Treatment of Osteoarthritis Secondary to Developmental Dysplasia of the Hip with Prolotherapy Injection versus a Supervised Progressive Exercise Control. Med. Sci. Monit. 2020, 26, e919166. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Licata, M.; Iorio, S.; Benaglia, P.; Tosi, A.; Borgo, M.; Armocida, G.; Ronga, M.; Ruspi, A.; Verzeletti, A.; Rossetti, C. Biomechanical analysis of a femur fracture in osteoarchaeology: Reconstruction of pathomechanics, treatment and gait. J. Forensic Leg. Med. 2019, 61, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Wenger, D.R.; Bomar, J.D. Historical Aspects of DDH. Indian J. Orthop. 2021, 55, 1360–1371. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lafferty, C.M.; Sartoris, D.J.; Tyson, R.; Resnick, D.; Kursunoglu, S.; Pate, D.; Sutherland, D. Acetabular alterations in untreated congenital dysplasia of the hip: Computed tomography with multiplanar re-formation and three-dimensional analysis. J. Comput. Assist. Tomogr. 1986, 10, 84–91. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossetti, N.; Fusco, R.; Messina, C.; Vanni, A.; Licata, M. Health and Heritage: The Bioarchaeological Discovery of a Probable Case of Developmental Dysplasia in an Adult Subject. Heritage 2024, 7, 5295-5306. https://doi.org/10.3390/heritage7100249
Rossetti N, Fusco R, Messina C, Vanni A, Licata M. Health and Heritage: The Bioarchaeological Discovery of a Probable Case of Developmental Dysplasia in an Adult Subject. Heritage. 2024; 7(10):5295-5306. https://doi.org/10.3390/heritage7100249
Chicago/Turabian StyleRossetti, Nicol, Roberta Fusco, Carmelo Messina, Arianna Vanni, and Marta Licata. 2024. "Health and Heritage: The Bioarchaeological Discovery of a Probable Case of Developmental Dysplasia in an Adult Subject" Heritage 7, no. 10: 5295-5306. https://doi.org/10.3390/heritage7100249
APA StyleRossetti, N., Fusco, R., Messina, C., Vanni, A., & Licata, M. (2024). Health and Heritage: The Bioarchaeological Discovery of a Probable Case of Developmental Dysplasia in an Adult Subject. Heritage, 7(10), 5295-5306. https://doi.org/10.3390/heritage7100249