
A Comparison of Post-Operative Occlusion with 3-D vs. 2-D Miniplate Fixation in the Management of Isolated Mandibular Angle Fractures


 , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maurer, P.; Eckert, A.W.; Kriwalsky, M.S.; Schubert, J. Scope and limitations of methods of mandibular reconstruction: A long-term follow-up. Br. J. Oral Maxillofac. Surg. 2010, 48, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Qiamuddin. Analysis of 362 cases of maxillofacial injuries in northern region of Pakistan. Pak. Oral Dent. J. 1991, 11, 35–43. [Google Scholar]
- Kim, K.; Ibrahim, A.M.S.; Koolen, P.G.L.; Lee, B.T.; Lin, S.J. Trends in Facial Fracture Treatment Using the American College of Surgeons National Surgical Quality Improvement Program Database. Plast. Reconstr. Surg. 2014, 133, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Vyas, A.; Mazumdar, U.; Khan, F.; Mehra, M.; Parihar, L.; Purohit, C. A study of mandibular fractures over a 5-year period of time: A retrospective study. Contemp. Clin. Dent. 2014, 5, 452–455. [Google Scholar] [CrossRef]
- Sehgal, S.; Ramanujam, L.; Prasad, K.; Krishnappa, R. Three-dimensional v/s standard titanium miniplate fixation in the management of mandibular fractures–A randomized clinical study. J. Cranio-Maxillofac. Surg. 2015, 42, 1292–1299. [Google Scholar] [CrossRef]
- Amjad, S.; Adnan Ali, S.; Abdus, S. Pattern and management of mandibular fractures: A study conducted on 264 patients. Pak. Oral Dent. J. 2007, 27, 103–106. [Google Scholar]
- Gadicherla, S.; Sasikumar, P.; Gill, S.S.; Bhagania, M.; Kamath, A.T.; Pentapati, K.C. Mandibular Fractures and Associated Factors at a Tertiary Care Hospital. Arch. Trauma Res. 2016, 5, e30574. [Google Scholar] [CrossRef]
- Tiwari, A.; Lata, J.; Mishra, M. Influence of the impacted mandibular third molars on fractures of the mandibular angle and condyle—A prospective clinical study. J. Oral Biol. Craniofacial Res. 2016, 6, 227–230. [Google Scholar] [CrossRef]
- Al-Moraissi, E.A.; Ellis, E. What Method for Management of Unilateral Mandibular Angle Fractures Has the Lowest Rate of Postoperative Complications? A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2014, 72, 2197–2211. [Google Scholar] [CrossRef]
- Lee, J.-H. Treatment of Mandibular Angle Fractures. Arch. Craniofacial Surg. 2017, 18, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Zanakis, S.; Tasoulas, J.; Angelidis, I.; Dendrinos, C. Tooth in the line of angle fractures: The impact in the healing process. A retrospective study of 112 patients. J. Cranio-Maxillofac. Surg. 2015, 43, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Danda, A.K. Comparison of a Single Noncompression Miniplate Versus 2 Noncompression Miniplates in the Treatment of Mandibular Angle Fractures: A Prospective, Randomized Clinical Trial. J. Oral Maxillofac. Surg. 2010, 68, 1565–1567. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O.; Jensen, S.S.; Kofod, T.; Schwartz, O.; Hillerup, S. Open or closed repositioning of mandibular fractures: Is there a difference in healing outcome? A systematic review. Int. Assoc. Dent. Traumatol. 2008, 24, 17–21. [Google Scholar] [CrossRef]
- Tams, J.; van Loon, J.-P.; Otten, B.; Bos, R.R. A computer study of biodegradable plates for internal fixation of mandibular angle fractures. J. Oral Maxillofac. Surg. 2001, 59, 404–407. [Google Scholar] [CrossRef]
- Zhu, W. Failure Analysis of the Superior Lateral Plate Technique for Mandibular Angle Fractures. J. Oral Maxillofac. Surg. 2019, 77, 107–108. [Google Scholar] [CrossRef]
- Champy, M.; Loddé, J.; Schmitt, R.; Jaeger, J.; Muster, D. Mandibular osteosynthesis by miniature screwed plates via a buccal approach. J. Maxillofac. Surg. 1978, 6, 14–21. [Google Scholar] [CrossRef]
- Yazdani, J.; Talesh, K.T.; Hosein, M.; Motamedi, K.; Fekri, S.; Hajmohammadi, S. Mandibular Angle Fractures: Comparison of One Miniplate vs. Two Mini- plates. Trauma Mon. 2013, 18, 17–20. [Google Scholar] [CrossRef]
- Alkan, A.; Çelebi, N.; Özden, B.; Baş, B.; Inal, S. Biomechanical comparison of different plating techniques in repair of mandibular angle fractures. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 104, 752–756. [Google Scholar] [CrossRef]
- Sadhwani, B.S.; Anchlia, S. Conventional 2.0 mm miniplates versus 3-D plates in mandibular fractures. Ann. Maxillofac. Surg. 2013, 3, 154–159. [Google Scholar] [CrossRef]
- Farmand, M.; Dupoirieux, L. The value of 3-dimensional plates in maxillofacial surgery. Rev. De Stomatol. Et De Chir. Maxillo-Faciale 1992, 93, 353–357. [Google Scholar]
- Singh, R.K.; Chand, S.; Pal, U.S.; Das, S.K.; Sinha, V.P. Matrix miniplate versus locking miniplate in the management of displaced mandibular angle fractures. Natl. J. Maxillofac. Surg. 2013, 4, 225–228. [Google Scholar] [CrossRef]
- Wusiman, P.; Taxifulati, D.; Weidong, L.; Moming, A. Three-dimensional versus standard miniplate, lag screws versus miniplates, locking plate versus non-locking miniplates: Management of mandibular fractures, a systematic review and meta-analysis. J. Dent. Sci. 2019, 14, 66–80. [Google Scholar] [CrossRef]
- Bohner, L.; Beiglboeck, F.; Schwipper, S.; Lustosa, R.M.; Segura, C.P.M.; Kleinheinz, J.; Jung, S. Treatment of Mandible Fractures Using a Miniplate System: A Retrospective Analysis. J. Clin. Med. 2020, 9, 2922. [Google Scholar] [CrossRef] [PubMed]
- Erdmann, D.; Follmar, K.E.; DeBruijn, M.; Bruno, A.D.; Jung, S.-H.; Edelman, D.; Mukundan, S.; Marcus, J.R. A Retrospective Analysis of Facial Fracture Etiologies. Ann. Plast. Surg. 2008, 60, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Gutta, R.; Tracy, K.; Johnson, C.; James, L.E.; Krishnan, D.G.; Marciani, R.D. Outcomes of Mandible Fracture Treatment at an Academic Tertiary Hospital: A 5-Year Analysis. J. Oral Maxillofac. Surg. 2014, 72, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Schierle, H.P.; Schmelzeisen, R.; Rahn, B. Experimental studies of the biomechanical stability of different miniplate configurations for the mandibular angle. Kiefer Gesichts-Chir. 1996, 41, 166–170. [Google Scholar]
- Vineeth, K.; Lalitha, R.M.; Prasad, K.; Ranganath, K.; Shwetha, V.; Singh, J. “A comparative evaluation between single noncompression titanium miniplate and three dimensional titanium miniplate in treatment of mandibular angle fracture”—A randomized prospective study. J. Cranio-Maxillofac. Surg. 2013, 41, 103–109. [Google Scholar] [CrossRef]
- Al-Tairi, N.; Shoushan, M.; Khedr, M.S.; Abd-Alal, S. Comparison of three-dimensional plate versus double miniplate osteosynthesis for treatment of unfavorable mandibular angle fractures. Tanta Dent. J. 2015, 12, 89–98. [Google Scholar] [CrossRef]
- Al-Moraissi, E.; Mounair, R.; El-Sharkawy, T.; El-Ghareeb, T. Comparison between three-dimensional and standard miniplates in the management of mandibular angle fractures: A prospective, randomized, double-blind, controlled clinical study. Int. J. Oral Maxillofac. Surg. 2015, 44, 316–321. [Google Scholar] [CrossRef]
- Wusiman, P.; Nie, B.; Li, W.D.; Moming, A. Management of mandibular angle fractures using 3- dimensional or standard miniplates: A systematic review and meta-analysis. J. Cranio-Maxillofac. Surg. 2019, 47, 622–628. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Patients above 16 years diagnosed with isolated mandibular angle fractures | Previously treated mandibular angle fractures |
| Infected fractures | |
| Comminuted fractures | |
| Completely edentulous patients | |
| Medically compromised patients |
| Gender Distribution | ||||
|---|---|---|---|---|
| Group A | Group B | Total | p-Value | |
| Males | 30 (57.7%) | 42 (80.8%) | 72 (69.2%) | 0.02 |
| Females | 22 (42.3% | 10 (19.2%) | 32 (30.8) | |
| Etiology of Fractures | ||||
| Fall | 28 (53.8%) | 8 (15.4%) | 36 (34.6%) | 0.01 |
| RTA | 20 (38.5) | 38 (73.1%) | 58 (55.8%) | |
| Assault | 4 (7.7%) | 6 (11.5%) | 10 (9.6%) | |
| Age Group | ||||
| 16–30 | 27 (51.9%) | 43 (82.7%) | 70 (67.8%) | 0.01 |
| 31–40 | 22 (42.3%) | 7 (13.5%) | 29 (27.9) | |
| 41–60 | 3 (5.8%) | 2 (3.8%) | 5 (4.8%) | |
| Total | 52 (100%) | 52 (100%) | 104 (100%) | |
| Group A | Group B | Total | p-Value | |
|---|---|---|---|---|
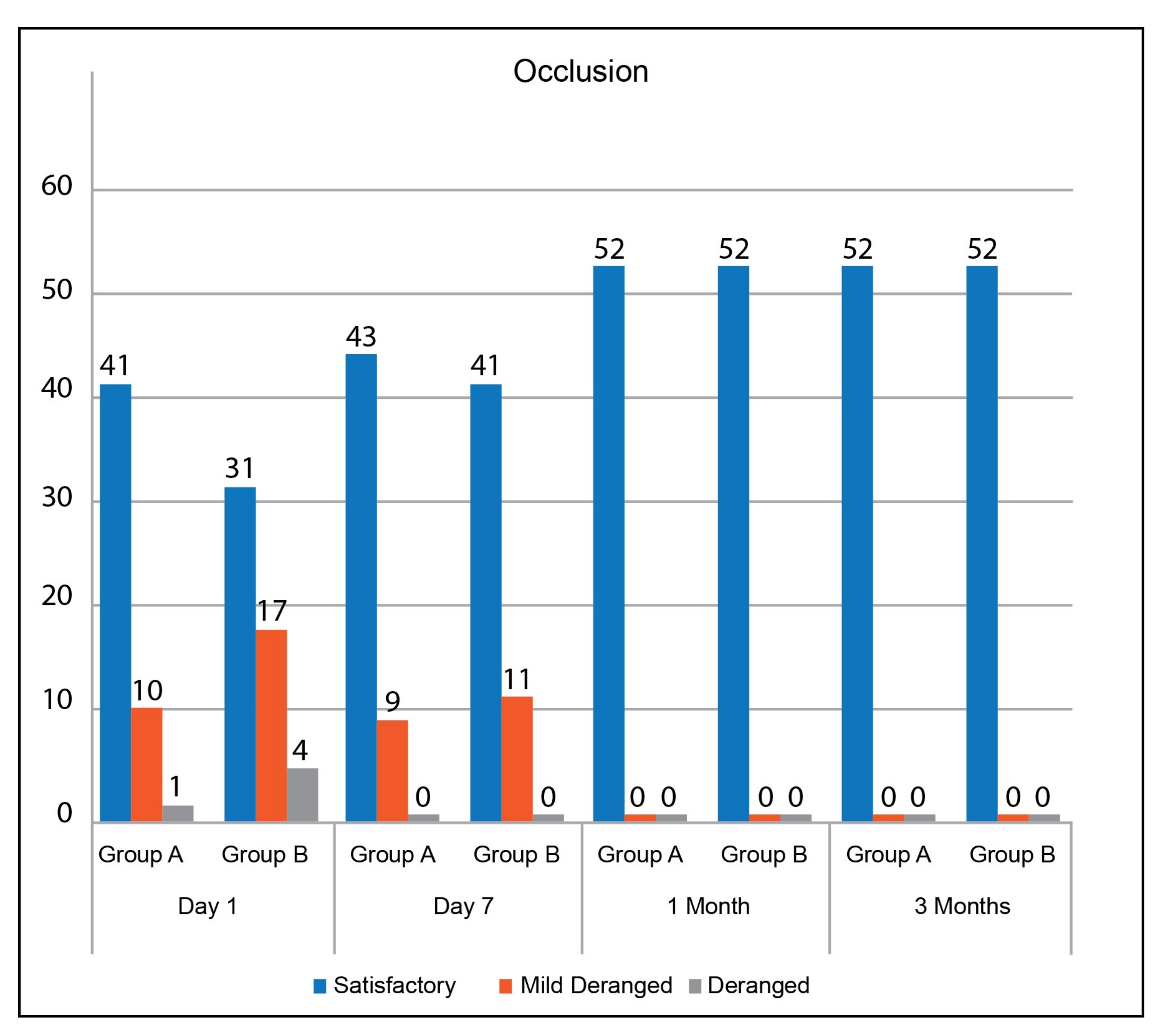
| Occlusion Day 1 | ||||
| Satisfactory | 41 (78.8%) | 31 (59.6%) | 72 (69.2%) | 0.11 |
| Mildly Deranged | 10 (19.2%) | 17 (32.7%) | 27 (26.0%) | |
| Deranged | 1 (1.9%) | 4 (7.7%) | 5 (4.8%) | |
| Occlusion Day 7 | ||||
| Satisfactory | 43 (82.7%) | 41 (78.8%) | 84 (80.8%) | 0.62 |
| Mildly Deranged | 9 (17.3%) | 11 (21.2%) | 20 (19.2%) | |
| Deranged | 0 | 0 | 0 | |
| Total | 52 (100%) | 52 (100%) | 104 (100%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mujtaba, A.; Malik, N.R.; Umer, M.F.; Mujtaba, H.; Zofeen, S.; Rana, Z.A. A Comparison of Post-Operative Occlusion with 3-D vs. 2-D Miniplate Fixation in the Management of Isolated Mandibular Angle Fractures. J 2022, 5, 107-113. https://doi.org/10.3390/j5010008
Mujtaba A, Malik NR, Umer MF, Mujtaba H, Zofeen S, Rana ZA. A Comparison of Post-Operative Occlusion with 3-D vs. 2-D Miniplate Fixation in the Management of Isolated Mandibular Angle Fractures. J. 2022; 5(1):107-113. https://doi.org/10.3390/j5010008
Chicago/Turabian StyleMujtaba, Anosha, Namrah Rafiq Malik, Muhammad Farooq Umer, Hasan Mujtaba, Shumaila Zofeen, and Zahoor Ahmad Rana. 2022. "A Comparison of Post-Operative Occlusion with 3-D vs. 2-D Miniplate Fixation in the Management of Isolated Mandibular Angle Fractures" J 5, no. 1: 107-113. https://doi.org/10.3390/j5010008
APA StyleMujtaba, A., Malik, N. R., Umer, M. F., Mujtaba, H., Zofeen, S., & Rana, Z. A. (2022). A Comparison of Post-Operative Occlusion with 3-D vs. 2-D Miniplate Fixation in the Management of Isolated Mandibular Angle Fractures. J, 5(1), 107-113. https://doi.org/10.3390/j5010008