
Catatonia in a Possible Case of Moderate Neuroleptic Malignant Syndrome: A Case Report

 ,
, 
Abstract
1. Introduction and Clinical Significance
2. Case Presentation
2.1. Patient Information
2.2. Mental State and Physical Examinations
2.3. Clinical Findings and Diagnosis
2.4. Treatment and Clinical Evolution
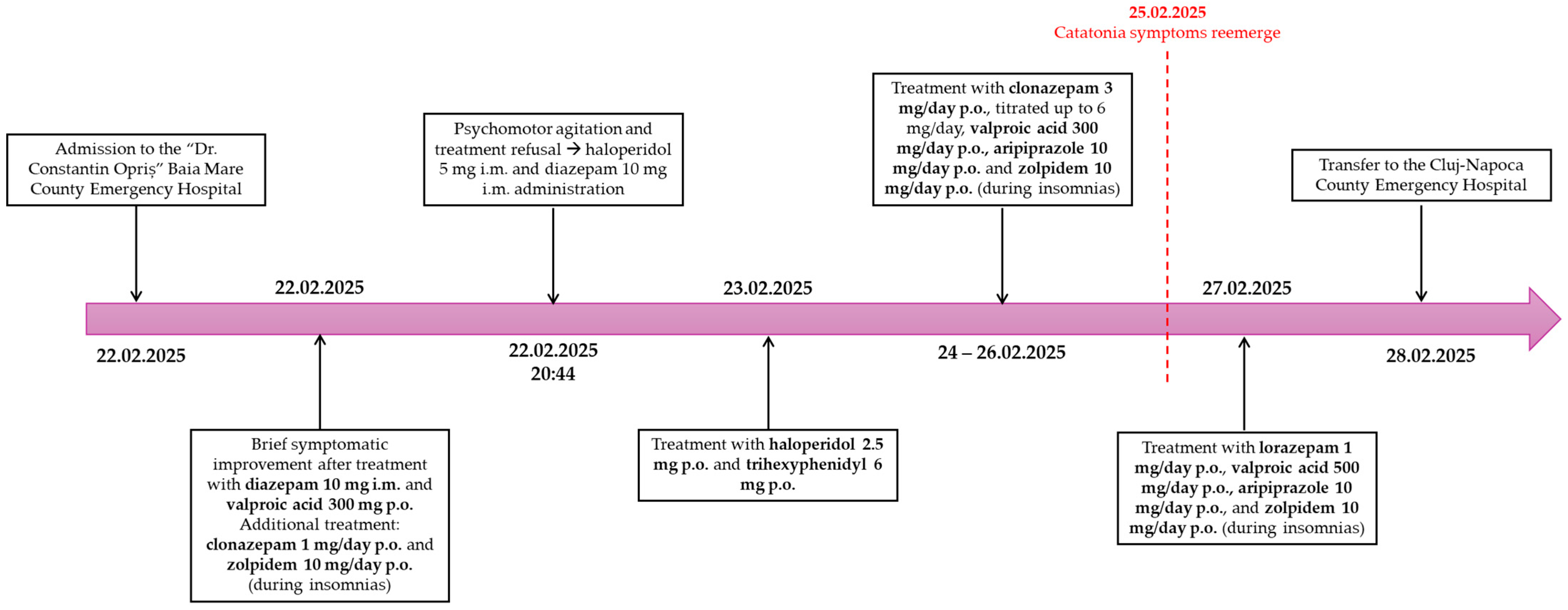
2.5. Timeline
2.6. Follow-Up and Outcomes
3. Discussion
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| p.o. | Per os |
| i.m. | Intramuscular |
| i.v. | Intravenous |
| s.c. | Subcutaneous |
| IU | International Unit |
| mmHg | Millimeter of Mercury |
| bpm | Beats per Minute |
References
- Edinoff, A.N.; Kaufman, S.E.; Hollier, J.W.; Virgen, C.G.; Karam, C.A.; Malone, G.W.; Cornett, E.M.; Kaye, A.M.; Kaye, A.D. Catatonia: Clinical Overview of the Diagnosis, Treatment, and Clinical Challenges. Neurol. Int. 2021, 13, 570–586. [Google Scholar] [CrossRef]
- Hirjak, D.; Foucher, J.R.; Ams, M.; Jeanjean, L.C.; Kubera, K.M.; Wolf, R.C.; Northoff, G. The Origins of Catatonia—Systematic Review of Historical Texts between 1800 and 1900. Schizophr. Res. 2024, 263, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Crișan, C.; Ungureanu, D. Sindromul Catatonic. In Urgențe Psihiatrice; Crișan, C., Moisuc, C.-R., Ungureanu, D., Eds.; Editura Medicală Universitară “Iuliu Hațieganu”: Cluj-Napoca, Romania, 2024; pp. 34–43. ISBN 978-606-075-296-7. [Google Scholar]
- Crişan, C.; Pop, R.F.; Bota, A.C.; Stan, A. Dissociative Stupor in Young Adults. Challenges in Differential Diagnosis and Treatment Management. Psihiatru.ro 2022, 1, 42. [Google Scholar] [CrossRef]
- Crișan, C.A.; Milhem, Z.; Stretea, R.; Țața, I.-M.; Cherecheș, R.M.; Micluția, I.V. A Narrative Review on REM Sleep Deprivation: A Promising Non-Pharmaceutical Alternative for Treating Endogenous Depression. J. Pers. Med. 2023, 13, 306. [Google Scholar] [CrossRef]
- Rogers, J.P.; Oldham, M.A.; Fricchione, G.; Northoff, G.; Ellen Wilson, J.; Mann, S.C.; Francis, A.; Wieck, A.; Elizabeth Wachtel, L.; Lewis, G.; et al. Evidence-Based Consensus Guidelines for the Management of Catatonia: Recommendations from the British Association for Psychopharmacology. J. Psychopharmacol. 2023, 37, 327–369. [Google Scholar] [CrossRef]
- Oldham, M.A. Describing the Features of Catatonia: A Comparative Phenotypic Analysis. Schizophr. Res. 2024, 263, 82–92. [Google Scholar] [CrossRef]
- Mormando, C.; Francis, A. Catatonia Revived: A Unique Syndrome Updated. Int. Rev. Psychiatry 2020, 32, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Fink, M.; Taylor, M.A. Catatonia: A History. In Catatonia: A Clinician’s Guide to Diagnosis and Treatment; Cambridge University Press: Cambridge, UK, 2003; pp. 1–18. ISBN 9780511543777. [Google Scholar]
- Ungureanu, D. Urgențe Medicamentoase. In Urgențe Psihiatrice; Crișan, C., Moisuc, C.-R., Ungureanu, D., Eds.; Editura Medicală Universitară „Iuliu Hațieganu”: Cluj-Napoca, Romania, 2024; pp. 147–185. ISBN 978-606-075-296-7. [Google Scholar]
- McCutcheon, R.A.; Kelly, J.; Pillinger, T. Neuroleptic Malignant Syndrome. In The Maudlsey Practice Guidelines for Physical Health Conditions in Psychiatry; Taylor, D.M., Gaughran, F., Pillinger, T., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2021; pp. 679–682. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revised (DSM-5-TR); American Psychiatric Association: Washington, DC, USA, 2022. [Google Scholar]
- Kyotani, Y.; Zhao, J.; Nakahira, K.; Yoshizumi, M. The Role of Antipsychotics and Other Drugs on the Development and Progression of Neuroleptic Malignant Syndrome. Sci. Rep. 2023, 13, 18459. [Google Scholar] [CrossRef]
- Gurrera, R.J. A Systematic Review of Sex and Age Factors in Neuroleptic Malignant Syndrome Diagnosis Frequency. Acta Psychiatr. Scand. 2017, 135, 398–408. [Google Scholar] [CrossRef]
- Connell, J.; Oldham, M.; Pandharipande, P.; Dittus, R.S.; Wilson, A.; Mart, M.; Heckers, S.; Ely, E.W.; Wilson, J.E. Malignant Catatonia: A Review for the Intensivist. J. Intensive Care Med. 2023, 38, 137–150. [Google Scholar] [CrossRef]
- Desai, S.; Hirachan, T.; Toma, A.; Gerolemou, A. Malignant Catatonia Versus Neuroleptic Malignant Syndrome. Cureus 2021, 13, e15818. [Google Scholar] [CrossRef]
- Orsolini, L.; Volpe, U. Expert Guidance on the Differential Diagnosis of Neuroleptic Malignant Syndrome. Expert Rev. Neurother. 2025, 25, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Carroll, B.T.; Taylor, R.E. The Nondichotomy Between Lethal Catatonia and Neuroleptic Malignant Syndrome. J. Clin. Psychopharmacol. 1997, 17, 235–236. [Google Scholar] [CrossRef]
- Fink, M. Neuroleptic Malignant Syndrome and Catatonia: One Entity or Two? Biol. Psychiatry 1996, 40, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Gaebel, W.; Hasan, A.; Falkai, P. S3 Guideline for Schizophrenia AWMF Register No. 038-009; German Association for Psychiatry, Psychotherapy and Psychosomatics, DGPPN (Deutsche Gesellschaft Für Psychiatrie Und Psychotherapie, Psychosomatik Und Nervenheilkunde e.V.): Berlin, Germany, 2019; Volume 2019, pp. 1–92. [Google Scholar]
- Schönfeldt-Lecuona, C.; Kuhlwilm, L.; Cronemeyer, M.; Neu, P.; Connemann, B.J.; Gahr, M.; Sartorius, A.; Mühlbauer, V. Treatment of the Neuroleptic Malignant Syndrome in International Therapy Guidelines: A Comparative Analysis. Pharmacopsychiatry 2020, 53, 51–59. [Google Scholar] [CrossRef]
- Strawn, J.R.; Keck, P.E.; Caroff, S.N. Neuroleptic Malignant Syndrome. Am. J. Psychiatry 2007, 164, 870–876. [Google Scholar] [CrossRef]
- Woodbury, M.M.; Woodbury, M.A. Case Study: Neuroleptic-Induced Catatonia as a Stage in the Progression toward Neuroleptic Malignant Syndrome. J. Am. Acad. Child Adolesc. Psychiatry 1992, 31, 1161–1164. [Google Scholar] [CrossRef]
- Lee, J.W.Y. Neuroleptic-Induced Catatonia. J. Clin. Psychopharmacol. 2010, 30, 3–10. [Google Scholar] [CrossRef]
- Radu, M.; Ciucă, A.; Crișan, C.; Pintea, S.; Predescu, E.; Șipos, R.; Moldovan, R.; Băban, A. The Impact of Psychiatric Disorders on Caregivers: An Integrative Predictive Model of Burden, Stigma, and Well-being. Perspect. Psychiatr. Care 2022, 58, 2372–2382. [Google Scholar] [CrossRef]
- Bush, G.; Fink, M.; Petrides, G.; Dowling, F.; Francis, A. Catatonia. I. Rating Scale and Standardized Examination. Acta Psychiatr. Scand. 1996, 93, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Guy, W. Clinical Global Impressions. In ECDU Assessment Manual for Psychopharmacology (Revised); Guy, W., Ed.; National Institute of Mental Health: Rockville, MD, USA, 1976; pp. 217–221. [Google Scholar]
- Leucht, S.; Kane, J.; Kissling, W.; Hamman, J.; Etschel, E.; Engel, R. What Does the PANSS Mean? Schizophr. Res. 2005, 79, 231–238. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Descriptions and Diagnostic Requirements for ICD-11 Mental, Behavioural and Neurodevelopmental Disorders; World Health Organization: Geneva, Switzerland, 2024; ISBN 9789240077263. [Google Scholar]
- Lin, C.-C.; Hung, Y.-Y.; Tsai, M.-C.; Huang, T.-L. The Lorazepam and Diazepam Protocol for Catatonia Due to General Medical Condition and Substance in Liaison Psychiatry. PLoS ONE 2017, 12, e0170452. [Google Scholar] [CrossRef] [PubMed]
- Iluț, S.; Vesa, Ş.C.; Văcăraș, V.; Brăiță, L.; Dăscălescu, V.-C.; Fantu, I.; Mureșanu, D.-F. Biological Risk Factors Influencing Vascular Cognitive Impairments: A Review of the Evidence. Brain Sci. 2023, 13, 1094. [Google Scholar] [CrossRef]
- Verner, L.J.; Kollmar, C.L.; Dietrich, D.E. Neuroleptic Malignant Syndrome or Haloperidol Toxicity: A Case Report and Differential Diagnosis. J. Psychiatr. Intensive Care 2006, 2, 122–123. [Google Scholar] [CrossRef]
- Wijdicks, E.F.M.; Ropper, A.H. Neuroleptic Malignant Syndrome. N. Engl. J. Med. 2024, 391, 1130–1138. [Google Scholar] [CrossRef]
- Regenbogen-Li, I.S.; Rapp, M.A. Letter: Seventeen-Year-Old Develops Neuroleptic Malignant Syndrome after Brief Low-Dose Exposure to Aripiprazole: A Case Report. J. Child Adolesc. Psychopharmacol. 2025. [Google Scholar] [CrossRef] [PubMed]
- Hammerman, S.; Lam, C.; Caroff, S.N. Neuroleptic Malignant Syndrome and Aripiprazole. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 639–641. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, V.; Direk, M.Ç.; Güneş, S.; Okuyaz, Ç.; Toros, F. Neuroleptic Malignant Syndrome Associated with Valproate in an Adolescent. Clin. Psychopharmacol. Neurosci. 2017, 15, 76–78. [Google Scholar] [CrossRef]
- Naranjo, C.A.; Busto, U.; Sellers, E.M.; Sandor, P.; Ruiz, I.; Roberts, E.A.; Janecek, E.; Domecq, C.; Greenblatt, D.J. A Method for Estimating the Probability of Adverse Drug Reactions. Clin. Pharmacol. Ther. 1981, 30, 239–245. [Google Scholar] [CrossRef]
- Gurrera, R.J.; Caroff, S.N.; Cohen, A.; Carroll, B.T.; DeRoos, F.; Francis, A.; Frucht, S.; Gupta, S.; Levenson, J.L.; Mahmood, A.; et al. An International Consensus Study of Neuroleptic Malignant Syndrome Diagnostic Criteria Using the Delphi Method. J. Clin. Psychiatry 2011, 72, 1222–1228. [Google Scholar] [CrossRef] [PubMed]
- Levenson, J.L. Neuroleptic Malignant Syndrome. Am. J. Psychiatry 1985, 142, 1137–1145. [Google Scholar] [CrossRef] [PubMed]
- Coffey, M.J. Catatonia: Treatment and Prognosis. Available online: https://www.uptodate.com/contents/catatonia-treatment-and-prognosis?search=catatoniatreatment&source=search_result&selectedTitle=1~64&usage_type=default&display_rank=1 (accessed on 9 June 2025).



{kind=link}
{kind=link}
{kind=link}
| NMS Stage | Clinical Symptoms | Reference |
|---|---|---|
| Stage I (Drug-induced Parkinsonism) | Rigidity, tremor | [20,21,22,23] |
| Stage II (Drug-induced Catatonia) | Rigidity, tremor, stupor | [20,21,22,23] |
| Stage III (Mild NMS) | Mild rigidity, catatonia or confusion, temperature ≤ 38 °C, heart rate ≤ 100 bpm | [20,21,22,23] |
| Stage IV (Moderate NMS) | Moderate rigidity, catatonia or confusion, temperature 38–40 °C, heart rate 100–120 bpm | [20,21,22,23] |
| Stage V (Severe NMS) | Severe rigidity, catatonia or confusion, temperature ≥ 40 °C, heart rate ≥ 120 bpm | [20,21,22,23] |
| 1 March 2025 | 3 March 2025 | 5 March 2025 | 7–12 March 2025 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter | Reference Range | Value | Interpretation | Value | Interpretation | Value | Interpretation | Value | Interpretation |
| ALT | <50 U/L | 49 U/L | ✓ | 50 U/L | ✓ | - | - | - | - |
| AST | <50 U/L | 159 U/L | ↑ | 71 U/L | ↑ | 48 U/L | - | - | - |
| CK | <171 U/L | 4908 U/L | ↑ | 1270 U/L | ↑ | 393 U/L | ↑ | - | - |
| CPK-MB | <24 U/L | 48 U/L | ↑ | - | - | - | - | - | - |
| Feritin | 20–250 ng/mL | 320 ng/mL | ↑ | - | - | - | - | - | - |
| Glycemia | 74–106 mg/dL | 67 mg/dL | ↓ | - | - | - | - | 73 mg/dL | ↓ |
| LDH | <248 U/L | 438 U/L | ↑ | - | - | - | - | 302 U/L | ↑ |
| CRP | <0.5 mg/dL | 6.27 mg/dL | ↑ | 1.80 mg/dL | ↑ | 2.01 mg/dL | ↑ | - | - |
| D-Dimers | <243 ng/mL | 12,189 ng/mL | ↑ | - | - | - | - | 660 ng/mL | ↑ |
| WBC | 4.5–11.5 × 109/L | 13.20 × 109/L | ↑ | 13.49 × 109/L | ↑ | 13.43 × 109/L | ↑ | 15.17 × 109/L | ↑ |
| NEUT# | 1.5–6.6 × 109/L | 10.45 × 109/L | ↑ | 12.09 × 109/L | ↑ | 11.27 × 109/L | ↑ | 11.84 × 109/L | ↑ |
| MONO# | 0.21–0.92 × 109/L | 1.03 × 109/L | ↑ | 0.58 × 109/L | ✓ | 0.87 × 109/L | ✓ | 0.93 × 109/L | ↑ |
| ESR | <15 mm/h | - | ↑ | 71 mm/h | - | - | - | - | - |
| Folic acid | 5.9–23.2 ng/mL | - | - | - | - | - | - | 2.83 ng/mL | ↓ |
| B12 vitamin | 180–914 pg/mL | - | - | - | - | - | - | 329 pg/mL | ✓ |
| FT4 | 0.9–1.53 ng/dL | - | - | - | - | - | - | 1.29 ng/dL | ✓ |
| TSH | 0.51–4.17 uIU/mL | - | - | - | - | - | - | 1.55 uIU/mL | ✓ |
| Date | Test | Result |
|---|---|---|
| 26 February 2025 | Native cranial CT scan | No cerebral oedema. No suggestive intracerebral heterodense lesions for increased intracranial pressure of any cause or recent ischemic stroke. No cerebral parenchymatous hemorrhagic zones. Ventricular system on the median line, with normal content. Free subarachnoid spaces. |
| 28 February 2025 | Cerebral MRI scan with contrast | No areas of acute ischemia. No intra- or extracerebral hemorrhagic accumulations. No evidenced lesions on the cerebral parenchyma, supra- or infratentorial. No evidenced cerebral or meningeal pathological modifications by the contrast. |
| Date | Test | Result | Observations |
|---|---|---|---|
| 3 March 2025 | Bacteriological blood exam | No developed aerobic and/or anaerobic bacteria after 5 days of incubation | - |
| 7 March 2025 | Fungal CSF exam | Absent Candida spp. | - |
| 7 March 2025 | Microbiology CSF exam | Absent Streptococcus spp., Staphylococcus aureus, Enterobacterales, Enterococcus spp., Pseudomonas spp., Acinetobacter spp., Candida spp. | - |
| 7 March 2025 | CSF cytology | Acellular smears | - |
| 13 March 2025 | Microbiology urine exam | Klebsiella pneumoniae ESBL 100.000 CFU/mL | Sensitive to meropenem, gentamycin, ciprofloxacin, and amikacin. Resistant to cefuroxime axetil, ceftazidime, amoxicillin + clavulanic acid, and ceftriaxone |
| Test | Result | Reference Range |
|---|---|---|
| Anti-Herpes simplex type 1 IgG antibodies | Non-reactive | Non-reactive |
| Anti-Herpes simplex type 1 IgM antibodies | Non-reactive | Non-reactive |
| Anti-Herpes simplex type 2 IgG antibodies | Non-reactive | Non-reactive |
| Anti-Herpes simplex type 2 IgM antibodies | Non-reactive | Non-reactive |
| Anti-Cytomegalovirus IgM antibodies | Non-reactive | Non-reactive |
| Anti-Cytomegalovirus IgG antibodies | <4 AU/mL | <4 AU/mL—Non-reactive ≥4–<6 AU/mL—Uncertain ≥6 AU/mL—Reactive |
| Anti-VZV IgG antibodies | Reactive | Non-reactive |
| Anti-VZV IgM antibodies | Non-reactive | Non-reactive |
| Anti-Epstein–Barr virus VCA IgM antibodies | Non-reactive | Non-reactive |
| Pathogen | Result * |
|---|---|
| Enterovirus | Undetectable |
| Herpes simplex virus 1 | Undetectable |
| Herpes simplex virus 2 | Undetectable |
| Human parechovirus | Undetectable |
| Human herpes virus 6 | Undetectable |
| Varicella zoster virus | Undetectable |
| S. pneumoniae | Undetectable |
| Neisseria meningitidis | Undetectable |
| S. agalactiae | Undetectable |
| Listeria monocytogenes | Undetectable |
| Hemophilus influenzae | Undetectable |
| Escherichia coli K1 | Undetectable |
| S. pyogenes | Undetectable |
| Mycoplasma pneumoniae | Undetectable |
| Cryptococcus neoformans/gattii | Undetectable |
| Test | Sample Type | Result | Reference Range |
|---|---|---|---|
| Anti-NMDA receptor antibodies | CSF | <1:1 | <1:1 |
| Serum | <1:10 | <1:10 | |
| Anti-GAD II antibodies | CSF | negative | - |
| Serum | <5.00 UI/mL | <10.00 UI/mL—negative ≥10.00 UI/mL—positive | |
| Anti-Amphiphysin IgG antibodies | CSF | negative | negative |
| Serum | |||
| Anti-C2 IgG antibodies | CSF | negative | negative |
| Serum | |||
| Anti-PNMA2 (Ma2/Ta) IgG antibodies | CSF | negative | negative |
| Serum | |||
| Anti-Ri IgG antibodies | CSF | negative | negative |
| Serum | |||
| Anti-Hu IgG antibodies | CSF | negative | negative |
| Serum | |||
| Anti-Yo IgG antibodies | CSF | negative | negative |
| Serum | |||
| Anti-Recoverin IgG antibodies | CSF | negative | negative |
| Serum | |||
| Anti-SOX1 IgG antibodies | CSF | negative | negative |
| Serum | |||
| Anti-Titin IgG antibodies | CSF | negative | negative |
| Serum | |||
| Anti-GAD64/65 antibodies | CSF | negative | negative |
| Anti-Tr/DNER antibodies | CSF | negative | negative |
| Protein 14-3-3 | CSF | negative * | - |
| NMS | Catatonia ** |
|---|---|
| Exposure to a dopamine antagonist within 72 h prior to the symptom development | Stupor |
| Hyperthermia (>38.0 °C on at least two occasions, orally measured) with profuse diaphoresis * | Catalepsy |
| Generalized rigidity, described as “lead pipe” rigidity | Waxy flexibility |
| CK levels elevated at least 4 times over the reference range | Mutism |
| Changes in mental status (delirium or altered consciousness) | Negativism |
| Autonomic activation and instability—tachycardia (>25% above the baseline values), diaphoresis, elevated blood pressure (≥20 mmHg for the diastolic blood pressure or ≥25 mmHg for the systolic blood pressure within 24 h) | Posturing |
| Urinary incontinence | Mannerism |
| Pallor | Stereotypy |
| Tachypnea (>50% above the baseline values) | Agitation, not influenced by external stimuli |
| Respiratory distress | Grimacing |
| Laboratory abnormalities (leukocytosis, metabolic acidosis, hypoxia, decreased serum iron levels, increased serum muscle enzymes levels and catecholamines) | Echolalia |
| Echopraxia | |
| ±Evidence that the disturbance is the direct pathophysiological consequence of another condition (for catatonic disorder due to another medical condition) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ungureanu, D.; Mitrea, P.-Ș.; Iluț, S.; Taloș, A.; Crișan, C.-A. Catatonia in a Possible Case of Moderate Neuroleptic Malignant Syndrome: A Case Report. Reports 2025, 8, 134. https://doi.org/10.3390/reports8030134
Ungureanu D, Mitrea P-Ș, Iluț S, Taloș A, Crișan C-A. Catatonia in a Possible Case of Moderate Neuroleptic Malignant Syndrome: A Case Report. Reports. 2025; 8(3):134. https://doi.org/10.3390/reports8030134
Chicago/Turabian StyleUngureanu, Daniel, Patricia-Ștefania Mitrea, Silvina Iluț, Aurora Taloș, and Cătălina-Angela Crișan. 2025. "Catatonia in a Possible Case of Moderate Neuroleptic Malignant Syndrome: A Case Report" Reports 8, no. 3: 134. https://doi.org/10.3390/reports8030134
APA StyleUngureanu, D., Mitrea, P.-Ș., Iluț, S., Taloș, A., & Crișan, C.-A. (2025). Catatonia in a Possible Case of Moderate Neuroleptic Malignant Syndrome: A Case Report. Reports, 8(3), 134. https://doi.org/10.3390/reports8030134