
Percutaneous Peripheral Nerve Stimulation in Chemotherapy-Induced Neuropathy: A Case Report

 ,
,  , and
, and 
Abstract
1. Introduction and Clinical Significance
2. Case Presentation
2.1. Patient Information
2.2. Clinical Findings
2.3. Patient Evolution
2.4. Diagnostic Assessment
2.5. Therapeutic Intervention
2.6. Study Variables and Follow-Up
2.7. Results
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CIPN | Chemotherapy-induced peripheral neuropathy |
| FDA | Food and Drug Administration |
| PENS | Percutaneous peripheral nerve stimulation |
| EORTC QLQ-CIPN20 | European Organization for Research and Treatment of Cancer questionnaire for evaluating CIPN |
| QST | Quantitative sensory testing |
| MDT | Mechanical detection thresholds |
| VT | Vibration thresholds |
| TDT | Temperature detection thresholds |
| CDT | Cold detection test |
| WDT | Heat detection test |
References
- Hu, L.Y.; Mi, W.L.; Wu, G.-C.; Wang, Y.Q.; Mao-Ying, Q.L. Prevention and Treatment for Chemotherapy-Induced Peripheral Neuropathy: Therapies Based on CIPN Mechanisms. Curr. Neuropharmacol. 2019, 17, 184–196. [Google Scholar] [CrossRef]
- Hwang, M.S.; Lee, H.Y.; Lee, J.H.; Choi, T.Y.; Lee, J.H.; Ko, Y.S.; Choi, S.Y.; Park, T.Y. Protocol for a systematic review and meta-analysis of the efficacy of acupuncture and electroacupuncture against chemotherapy-induced peripheral neuropathy. Medicine 2019, 98, e15098. [Google Scholar] [CrossRef]
- Hershman, D.L.; Weimer, L.H.; Wang, A.; Kranwinkel, G.; Brafman, L.; Fuentes, D.; Awad, D.; Crew, K.D. Association between patient reported outcomes and quantitative sensory tests for measuring long-term neurotoxicity in breast cancer survivors treated with adjuvant paclitaxel chemotherapy. Breast Cancer Res. Treat. 2011, 125, 767–774. [Google Scholar] [CrossRef]
- Tofthagen, C. Surviving chemotherapy for colon cancer and living with the consequences. J. Palliat. Med. 2010, 13, 1389–1391. [Google Scholar] [CrossRef] [PubMed]
- Nardone, R.; Buratti, T.; Golaszewski, S.; Bratti, A.; Caleri, F.; Tezzon, F.; Ladurner, G.; Mitterer, M. Delayed oxaliplatin-induced sensorimotor polyneuropathy. Onkologie 2009, 32, 10. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.; Ferdousi, M.; Gosal, D.; Boon, C.; Matsumoto, K.; Mak, T.; Marshall, A.; Frank, B.; Malik, R.A.; Alam, U. Chemotherapy-Induced Peripheral Neuropathy: Epidemiology, Pathomechanisms and Treatment. Oncol. Ther. 2021, 9, 385–450. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, R.S.; Saini, C.; Hussain, N.; Javed, S.; Prokop, L.; Her, Y.F. Global estimates of prevalence of chronic painful neuropathy among patients with chemotherapy-induced peripheral neuropathy: Systematic review and meta-analysis of data from 28 countries, 2000–2024. Reg. Anesth. Pain Med. 2025. [Google Scholar] [CrossRef]
- Hammond, E.A.; Pitz, M.; Steinfeld, K.; Lambert, P.; Shay, B. An Exploratory Randomized Trial of Physical Therapy for the Treatment of Chemotherapy-Induced Peripheral Neuropathy. Neurorehabilit. Neural Repair. 2020, 34, 235–246. [Google Scholar] [CrossRef]
- Kim, J.H.; Dougherty, P.M.; Abdi, S. Basic science and clinical management of painful and non-painful chemotherapy-related neuropathy. Gynecol. Oncol. 2015, 136, 453–459. [Google Scholar] [CrossRef]
- Staff, N.P.; Grisold, A.; Grisold, W.; Windebank, A.J. Chemotherapy-induced peripheral neuropathy: A current review. Ann. Neurol. 2017, 81, 772–781. [Google Scholar] [CrossRef]
- Bae, E.H.; Greenwald, M.K.; Schwartz, A.G. Chemotherapy-Induced Peripheral Neuropathy: Mechanisms and Therapeutic Avenues. Neurotherapeutics 2021, 18, 2384–2396. [Google Scholar] [CrossRef]
- Ristić, D.; Spangenberg, P.; Ellrich, J. Analgesic and antinociceptive effects of peripheral nerve neurostimulation in an advanced human experimental model. Eur. J. Pain 2008, 12, 480–490. [Google Scholar] [CrossRef] [PubMed]
- Kupers, R.; Laere, K.V.; Calenbergh, F.V.; Gybels, J.; Dupont, P.; Baeck, A.; Plaghki, L. Multimodal therapeutic assessment of peripheral nerve stimulation in neuropathic pain: Five case reports with a 20-year follow-up. Eur. J. Pain 2011, 15, 161.e1–161.e9. [Google Scholar] [PubMed]
- D’souza, R.S.; Her, Y.F.; Jin, M.Y.; Morsi, M.; Abd-Elsayed, A. Neuromodulation Therapy for Chemotherapy-Induced Peripheral Neuropathy: A Systematic Review. Biomedicines 2022, 10, 1909. [Google Scholar] [CrossRef] [PubMed]
- Ghoname, E.-S.A.; White, P.F.; Ahmed, H.E.; Hamza, M.A.; Craig, W.F.; Noe, C.E. Percutaneous electrical nerve stimulation: An alternative to TENS in the management of sciatica. Pain 1999, 83, 193–199. [Google Scholar] [CrossRef]
- Hamza, M.A.; White, P.F.; Craig, W.F.; Ghoname, E.S.; Ahmed, H.E.; Proctor, T.J.; Noe, C.E.; Vakharia, A.S.; Gajraj, N. Percutaneous electrical nerve stimulation: A novel analgesic therapy for diabetic neuropathic pain. Diabetes Care 2000, 23, 365–370. [Google Scholar] [CrossRef]
- Raphael, J.H.; Raheem, T.A.; Southall, J.L.; Bennett, A.; Ashford, R.L.; Williams, S. Randomized double-blind sham-controlled crossover study of short-term effect of percutaneous electrical nerve stimulation in neuropathic pain. Pain Med. 2011, 12, 1515–1522. [Google Scholar] [CrossRef]
- Gilmore, C.; Ilfeld, B.; Rosenow, J.; Li, S.; Desai, M.; Hunter, C.; Rauck, R.; Kapural, L.; Nader, A.; Mak, J.; et al. Percutaneous peripheral nerve stimulation for the treatment of chronic neuropathic postamputation pain: A multicenter, randomized, placebo-controlled trial. Reg. Anesth. Pain Med. 2019, 44, 637–645. [Google Scholar] [CrossRef]
- Loprinzi, C.L.; Lacchetti, C.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Hertz, D.L.; Kelley, M.R.; Lavino, A.; Lustberg, M.B.; Paice, J.A.; et al. Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy in Survivors of Adult Cancers: ASCO Guideline Update. J. Clin. Oncol. 2020, 38, 3325–3348. [Google Scholar] [CrossRef]
- Lu, C.; Bao, W.; Deng, D.; Li, R.; Li, G.; Zou, S.; Wang, Y. Efficacy of electroacupuncture with different frequencies in the treatment of chemotherapy-induced peripheral neuropathy: A study protocol for a randomized controlled trial. Front. Neurol. 2022, 13, 843886. [Google Scholar] [CrossRef]
- Li, R.; Lu, J.; Wang, M.; Zhang, P.; Fang, H.; Yang, K.; Wang, L.; Zhuang, J.; Tian, Z.; Yang, J.; et al. Ultrasound-Guided Median Nerve Electrical Stimulation to Promote Upper Limb Function Recovery after Stroke. Evid. Based Complement. Altern. Med. 2022, 2022, 3590057. [Google Scholar] [CrossRef]
- Chu, X.L.; Song, X.Z.; Li, Y.R.; Wu, Z.R.; Li, Q.; Li, Q.W.; Gu, X.S.; Ming, D. An ultrasound-guided percutaneous electrical nerve stimulation regimen devised using finite element modeling promotes functional recovery after median nerve transection. Neural Regen. Res. 2022, 18, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.; Huh, B.; Kim, H.K.; Kim, K.-H.; Abdi, S. Treatment of Chemotherapy-Induced Peripheral Neuropathy: Systematic Review and Recommendations. Pain Physician 2018, 21, 571–592. [Google Scholar] [CrossRef] [PubMed]
- Velasco, R.; Bruna, J. Chemotherapy-induced peripheral neuropathy: An unresolved issue. Neurologia 2010, 25, 116–131. [Google Scholar] [CrossRef]
- Weaver, K.R.; Griffioen, M.A.; Klinedinst, N.J.; Galik, E.; Duarte, A.C.; Colloca, L.; Resnick, B.; Dorsey, S.G.; Renn, C.L. Quantitative Sensory Testing Across Chronic Pain Conditions and Use in Special Populations. Front. Pain Res. 2022, 2, 779068. [Google Scholar] [CrossRef]
- Rolke, R.; Magerl, W.; Campbell, K.A.; Schalber, C.; Caspari, S.; Birklein, F.; Treede, R. Quantitative sensory testing: A comprehensive protocol for clinical trials. Eur. J. Pain 2006, 10, 77. [Google Scholar] [CrossRef]
- Zhi, W.I.; Baser, R.E.; Kwon, A.; Chen, C.; Li, S.Q.; Piulson, L.; Seluzicki, C.; Panageas, K.S.; Harte, S.E.; Mao, J.J.; et al. Characterization of chemotherapy-induced peripheral neuropathy using patient-reported outcomes and quantitative sensory testing. Breast Cancer Res. Treat. 2021, 186, 761–768. [Google Scholar] [CrossRef]
- Cata, J.P.; Cordella, J.V.; Burton, A.W.; Hassenbusch, S.J.; Weng, H.R.; Dougherty, P.M. Spinal cord stimulation relieves chemotherapy-induced pain: A clinical case report. J. Pain Symptom Manag. 2004, 27, 72–78. [Google Scholar] [CrossRef]
- Li, T.; Mizrahi, D.; Goldstein, D.; Kiernan, M.C.; Park, S.B. Chemotherapy and peripheral neuropathy. Neurol. Sci. 2021, 42, 4109–4121. [Google Scholar] [CrossRef]
- San-Emeterio-Iglesias, R.; Minaya-Muñoz, F.; Romero-Morales, C.; De-La-Cruz-Torres, B. Correct Sciatic Nerve Management to Apply Ultrasound-Guided Percutaneous Neuromodulation in Patients with Chronic Low Back Pain: A Pilot Study. Neuromodulation 2021, 24, 1067–1074. [Google Scholar] [CrossRef]
- Xin, Y.Y.; Wang, J.X.; Xu, A.J. Electroacupuncture ameliorates neuroinflammation in animal models. Acupunct. Med. 2022, 40, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Ellrich, J.; Lamp, S. Peripheral nerve stimulation inhibits nociceptive processing: An electrophysiological study in healthy volunteers. Neuromodulation 2005, 8, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Bari, A.; Pouratian, N. Brain imaging correlates of peripheral nerve stimulation. Surg. Neurol. Int. 2012, 3, 260–268. [Google Scholar] [CrossRef]
- Lai, M.-I.; Pan, L.-L.; Tsai, M.-W.; Shih, Y.-F.; Wei, S.-H.; Chou, L.-W. Investigating the Effects of Peripheral Electrical Stimulation on Corticomuscular Functional Connectivity Stroke Survivors. Top. Stroke Rehabil. 2016, 23, 154–162. [Google Scholar] [CrossRef]
- Chen, X.H.; Han, J.S. Analgesia induced by electroacupuncture of different frequencies is mediated by different types of opioid receptors: Another cross-tolerance study. Behav. Brain Res. 1992, 47, 143–149. [Google Scholar] [CrossRef]
- Ghoname, E.S.; Craig, W.F.; White, P.F.; Ahmed, H.E.; Hamza, M.A.; Gajraj, N.M.; Vakharia, A.S.; Noe, C.E. The effect of stimulus frequency on the analgesic response to percutaneous electrical nerve stimulation in patients with chronic low back pain. Anesth. Analg. 1999, 88, 841–846. [Google Scholar]
- Ahmed, S.; Haddad, C.; Subramaniam, S.; Khattab, S.; Kumbhare, D. The Effect of Electric Stimulation Techniques on Pain and Tenderness at the Myofascial Trigger Point: A Systematic Review. Pain Med. 2019, 20, 1774–1788. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Baseline | Week 4 | Week 12 | Change (Baseline–Week 12) | Percentage Change |
|---|---|---|---|---|---|
| Tingling (0–4) | 3/4 | 3/4 | 2/4 | −1 | −33% |
| Cramps (0–4) | 2/4 | 2/4 | 2/4 | 0 | 0% |
| Stabbing pain (0–4) | 3/4 | 0/4 | 0/4 | −3 | −100% |
| Functional difficulties (0–4) | 2/4 | 0/4 | 0/4 | −2 | −100% |
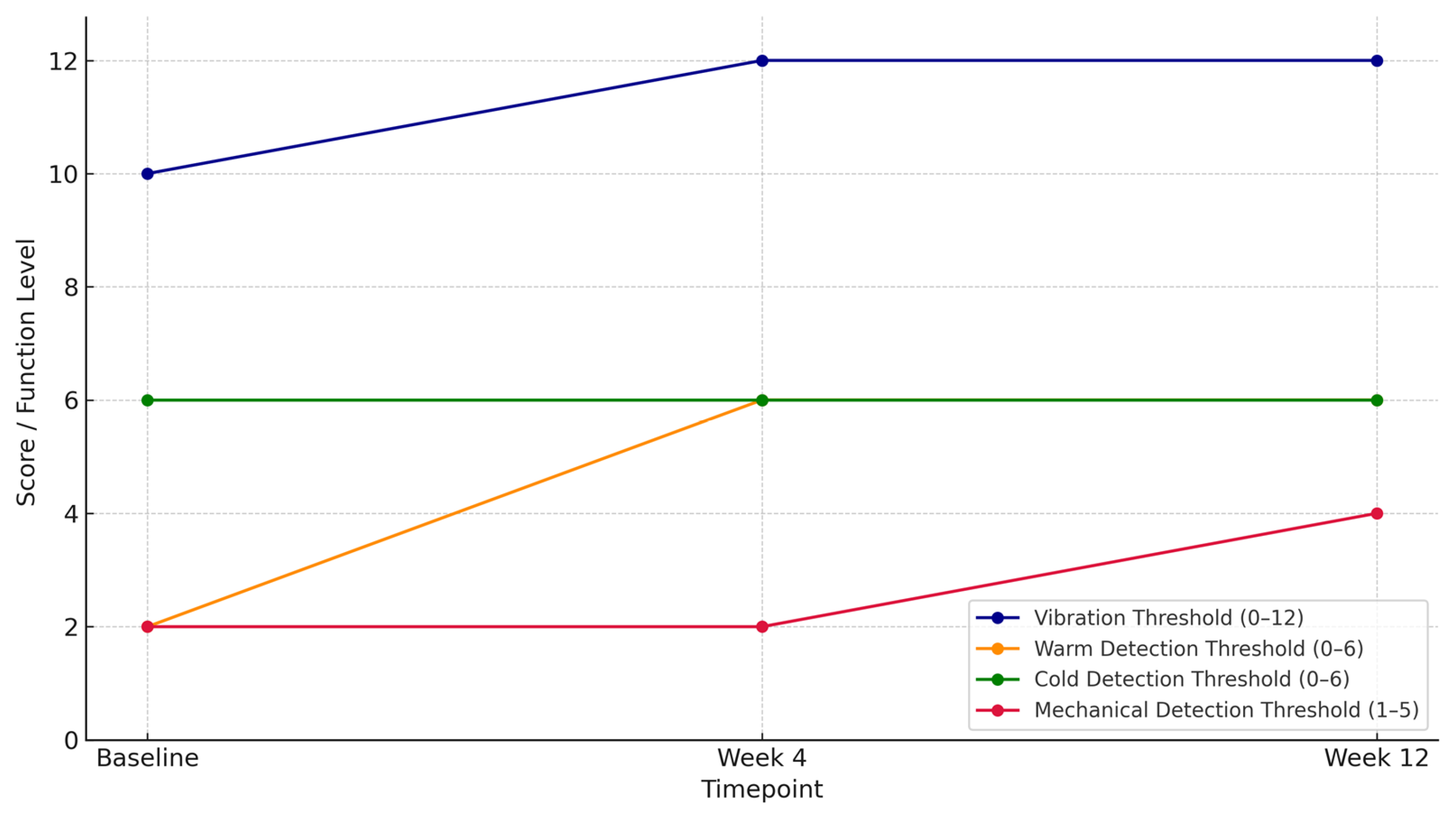
| Vibration Thresholds (0–12) | 10/12 | 12/12 | 12/12 | +2 | +20% |
| Warm Detection Thresholds (0–6) | 2/6 | 6/6 | 6/6 | +4 | +67% |
| Cold Detection Thresholds (0–6) | 6/6 | 6/6 | 6/6 | 0 | 0% |
| Mechanical Detection Thresholds | Decreased protective sensation | No change | Reduced light-touch sensitivity | Partial recovery | — |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mogedano-Cruz, S.; Romero-Morales, C.; de la Cueva-Reguera, M.; Campbell, K.L.; Herrero, P. Percutaneous Peripheral Nerve Stimulation in Chemotherapy-Induced Neuropathy: A Case Report. Reports 2025, 8, 133. https://doi.org/10.3390/reports8030133
Mogedano-Cruz S, Romero-Morales C, de la Cueva-Reguera M, Campbell KL, Herrero P. Percutaneous Peripheral Nerve Stimulation in Chemotherapy-Induced Neuropathy: A Case Report. Reports. 2025; 8(3):133. https://doi.org/10.3390/reports8030133
Chicago/Turabian StyleMogedano-Cruz, Sara, Carlos Romero-Morales, Mónica de la Cueva-Reguera, Kristin L. Campbell, and Pablo Herrero. 2025. "Percutaneous Peripheral Nerve Stimulation in Chemotherapy-Induced Neuropathy: A Case Report" Reports 8, no. 3: 133. https://doi.org/10.3390/reports8030133
APA StyleMogedano-Cruz, S., Romero-Morales, C., de la Cueva-Reguera, M., Campbell, K. L., & Herrero, P. (2025). Percutaneous Peripheral Nerve Stimulation in Chemotherapy-Induced Neuropathy: A Case Report. Reports, 8(3), 133. https://doi.org/10.3390/reports8030133