
Neuromyelitis Optica Diagnosis in Two Elderly Patients with Systematic Lupus Erythematosus: A Case Series

 , ,
, ,  ,
,
Abstract
1. Introduction and Clinical Significance
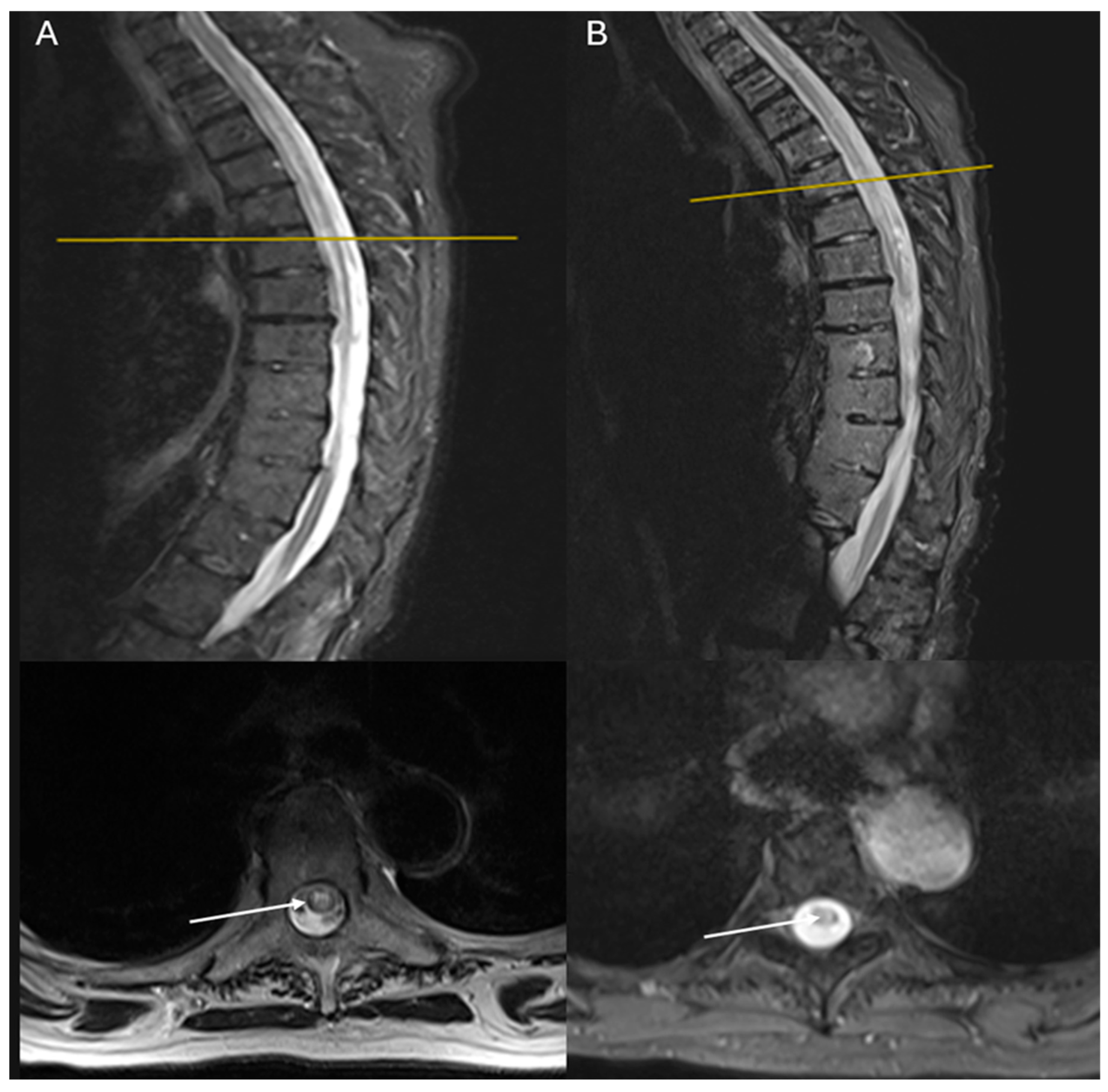
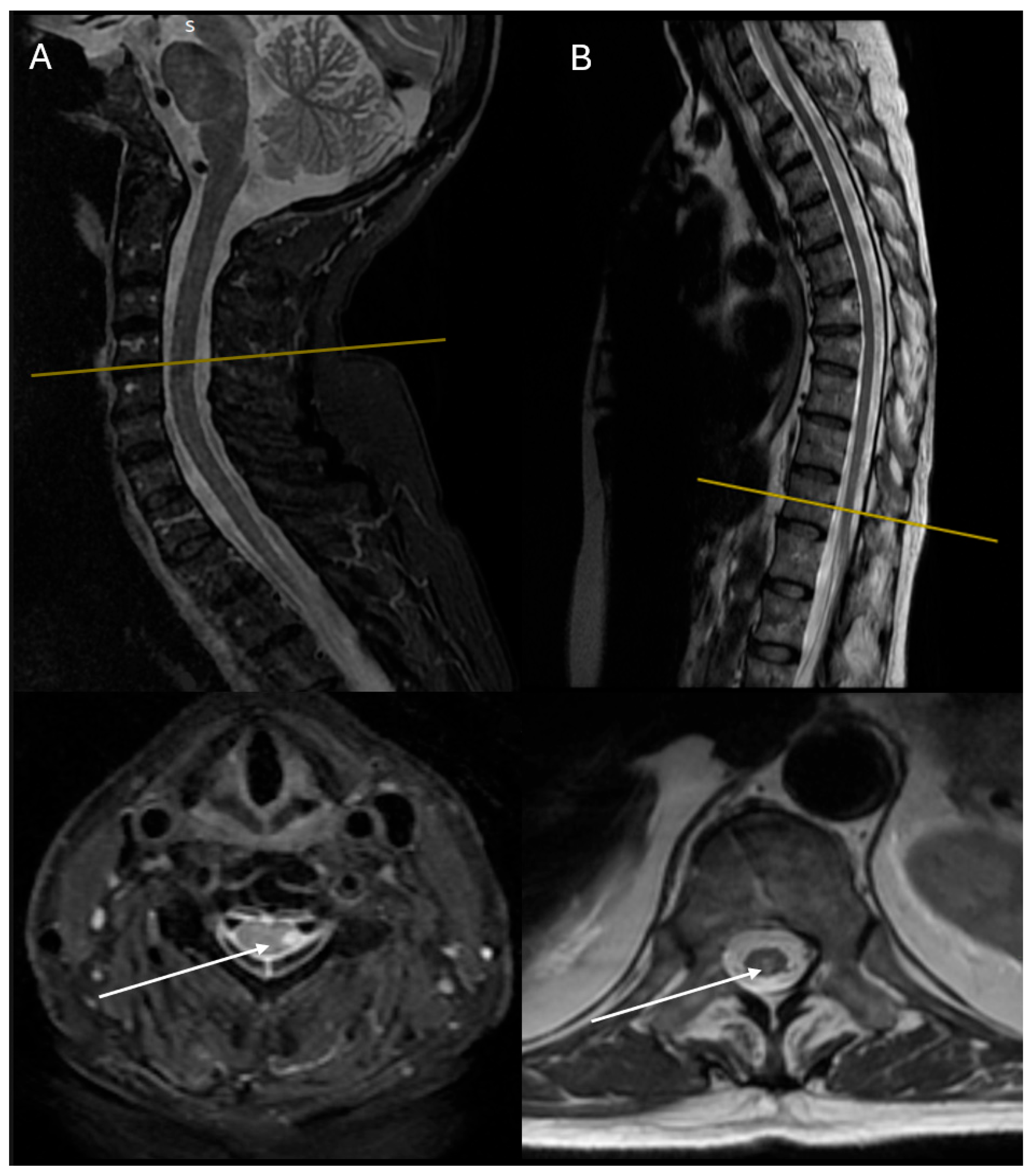
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NMOSD | Neuromyelitis optica spectrum disorder |
| SLE | Systematic lupus erythematosus |
| AQ4 | Aquaporin-4 |
| mRS | Modified Rankin Scale |
| ECG | Electrocardiogram |
| CT | Computed tomography |
| MRI | Magnetic resonance imaging |
| CSF | Cerebrospinal fluid |
| LP | Lumbar puncture |
| ELISA | Enzyme-linked immunosorbent assay |
| CYC | Cyclophosphamide |
| RTX | Rituximab |
| EDSS | Expanded Disability Status Scale |
References
- Wingerchuk, D.M.; Lucchinetti, C.F. Neuromyelitis Optica Spectrum Disorder. N. Engl. J. Med. 2022, 387, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Hryb, J.P.; Chiganer, E.; Contentti, E.C.; Di Pace, J.L.; Lessa, C.; Perassolo, M.B. Myelitis in Systemic Lupus Erythematosus: Clinical Features, Immunological Profile and Magnetic Resonance Imaging of Five Cases. Spinal Cord. Ser. Cases 2016, 2, 16005. [Google Scholar] [CrossRef] [PubMed]
- Aringer, M.; Costenbader, K.H.; Daikh, D.I.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.; Kamen, D.L.; et al. 2019 EULAR/ACR Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1400–1412. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Sawalha, A.H. Drug-Induced Lupus Erythematosus: An Update on Drugs and Mechanisms. Curr. Opin. Rheumatol. 2018, 30, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Vaglio, A.; Grayson, P.C.; Fenaroli, P.; Gianfreda, D.; Boccaletti, V.; Ghiggeri, G.M.; Moroni, G. Drug-Induced Lupus: Traditional and New Concepts. Autoimmun. Rev. 2018, 17, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Palace, J.; Lin, D.-Y.; Zeng, D.; Majed, M.; Elsone, L.; Hamid, S.; Messina, S.; Misu, T.; Sagen, J.; Whittam, D.; et al. Outcome Prediction Models in AQP4-IgG Positive Neuromyelitis Optica Spectrum Disorders. Brain 2019, 142, 1310–1323. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Kermode, A.G.; Hu, X.; Qiu, W. Risk of Relapse in Patients with Neuromyelitis Optica Spectrum Disorder: Recognition and Preventive Strategy. Mult. Scler. Relat. Disord. 2020, 46, 102522. [Google Scholar] [CrossRef] [PubMed]
- Kopp, C.R.; Prasad, C.B.; Naidu, S.; Sharma, V.; Misra, D.P.; Agarwal, V.; Sharma, A. Overlap Syndrome of Anti-Aquaporin-4 Positive Neuromyelitis Optica Spectrum Disorder and Systemic Lupus Erythematosus: A Systematic Review of Individual Patient Data. Lupus 2023, 32, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- Wright, S.K.; Wassmer, E.; Vincent, A. Pathogenic Antibodies to AQP4: Neuromyelitis Optica Spectrum Disorder (NMOSD). Biochim. Et. Biophys. Acta (BBA)-Biomembr. 2021, 1863, 183772. [Google Scholar] [CrossRef] [PubMed]
- Wingerchuk, D.M.; Lennon, V.A.; Pittock, S.J.; Lucchinetti, C.F.; Weinshenker, B.G. Revised Diagnostic Criteria for Neuromyelitis Optica. Neurology 2006, 66, 1485–1489. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhou, J.; Li, Y.; Wei, L.; Xu, X.; Zhang, J.; Yang, K.; Wei, S.; Zhang, W. Adverse Events of Rituximab in Neuromyelitis Optica Spectrum Disorder: A Systematic Review and Meta-Analysis. Ther. Adv. Neurol. Disord. 2021, 14, 17562864211056710. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Chai, B.; Gu, C.; Wu, R.; Dong, T.; Yao, Y.; Zhang, Y. Effectiveness of Rituximab in Neuromyelitis Optica: A Meta-Analysis. BMC Neurol. 2019, 19, 36. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.; Lu, T.; Wang, Y.; Fang, L.; Li, R.; Kermode, A.G.; Qiu, W. Rapid Exacerbation of Neuromyelitis Optica after Rituximab Treatment. J. Clin. Neurosci. 2016, 26, 168–170. [Google Scholar] [CrossRef] [PubMed]
- McKeon, A.; Pittock, S. Individualized Rituximab Treatment for Neuromyelitis Optica Spectrum Disorders. JAMA Neurol. 2013, 70, 1102–1104. [Google Scholar] [CrossRef] [PubMed]
- Aspden, J.W.; Murphy, M.A.; Kashlan, R.D.; Xiong, Y.; Poznansky, M.C.; Sîrbulescu, R.F. Intruders or Protectors-the Multifaceted Role of B Cells in CNS Disorders. Front. Cell Neurosci. 2023, 17, 1329823. [Google Scholar] [CrossRef] [PubMed]
- Asavapanumas, N.; Tradtrantip, L.; Verkman, A.S. Targeting the Complement System in Neuromyelitis Optica Spectrum Disorder. Expert. Opin. Biol. Ther. 2021, 21, 1073–1086. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhao, M.; Yao, M.; Yang, Z.; Li, B.; Yin, L.; Geng, X. Tocilizumab Treatment in Neuromyelitis Optica Spectrum Disorders: Updated Meta-Analysis of Efficacy and Safety. Mult. Scler. Relat. Disord. 2023, 80, 105062. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Case 1 | Case 1—Follow-Up | Case 2 | Case 2—Follow-Up | |
|---|---|---|---|---|
| Age of NMOSD Diagnosis | 78 | 79 | 71 | 72 |
| Level | T3–T8 | T3–T8 | C3–C7 | C4–C7, T10–T12 |
| Neurological Manifestation | Incomplete paraparesis T4 level | Indifferent | Incomplete paraparesis C4 level, worse on the left side | Improved—slight residual weakness on the left lower extremity distally |
| LP: | 0 cells, Glucose: 62 mg/dL, Protein: 69 mg/dL, LDH: 51, culture (−) cytology (−) for malignancy | - | 0 cells, Glucose: 51 mg/dL, Protein: 32 mg/dL, LDH: 46, culture (−) cytology (−) for malignancy (presence of cellular elements compatible with the inflammatory process) | - |
| Oligoclonal Bands | Type 3 | - | Type 3 | - |
| Anti-AQ4 | 320 | 100 | 3200 | 100 |
| Significant Workup | PCR HHV-6 (+) AΝA (+) and dsDNA (+) | - | ↓C3: 71, ↓C4: 4 | - |
| Treatment | Iv methyl-prednisolone 1gr × 5 days -> stop due to pancreatic reaction 2 cycles CYC | 2 cycles RTX | Iv methyl-prednisolone 1gr × 5 days, with gradual per os tapering up to 16 mg. 2 cycles CYC | 2 cycles RTX |
| EDSS | 7.5 | 7.5 | 7 | 4 |
| Outcome | Stagnant—bedridden | Improved—able to stand and walk with support and self-service capability | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Astara, K.; Lypiridou, M.; Kalafatakis, K.; Nikolaou, G.; Stouraitis, G. Neuromyelitis Optica Diagnosis in Two Elderly Patients with Systematic Lupus Erythematosus: A Case Series. Reports 2025, 8, 110. https://doi.org/10.3390/reports8030110
Astara K, Lypiridou M, Kalafatakis K, Nikolaou G, Stouraitis G. Neuromyelitis Optica Diagnosis in Two Elderly Patients with Systematic Lupus Erythematosus: A Case Series. Reports. 2025; 8(3):110. https://doi.org/10.3390/reports8030110
Chicago/Turabian StyleAstara, Kyriaki, Maria Lypiridou, Konstantinos Kalafatakis, Georgios Nikolaou, and Georgios Stouraitis. 2025. "Neuromyelitis Optica Diagnosis in Two Elderly Patients with Systematic Lupus Erythematosus: A Case Series" Reports 8, no. 3: 110. https://doi.org/10.3390/reports8030110
APA StyleAstara, K., Lypiridou, M., Kalafatakis, K., Nikolaou, G., & Stouraitis, G. (2025). Neuromyelitis Optica Diagnosis in Two Elderly Patients with Systematic Lupus Erythematosus: A Case Series. Reports, 8(3), 110. https://doi.org/10.3390/reports8030110