
Multidisciplinary Management of Acute Esophageal Necrosis Secondary to Alcoholic Lactic Acidosis: A Case Report

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction and Clinical Significance
2. Case Presentation
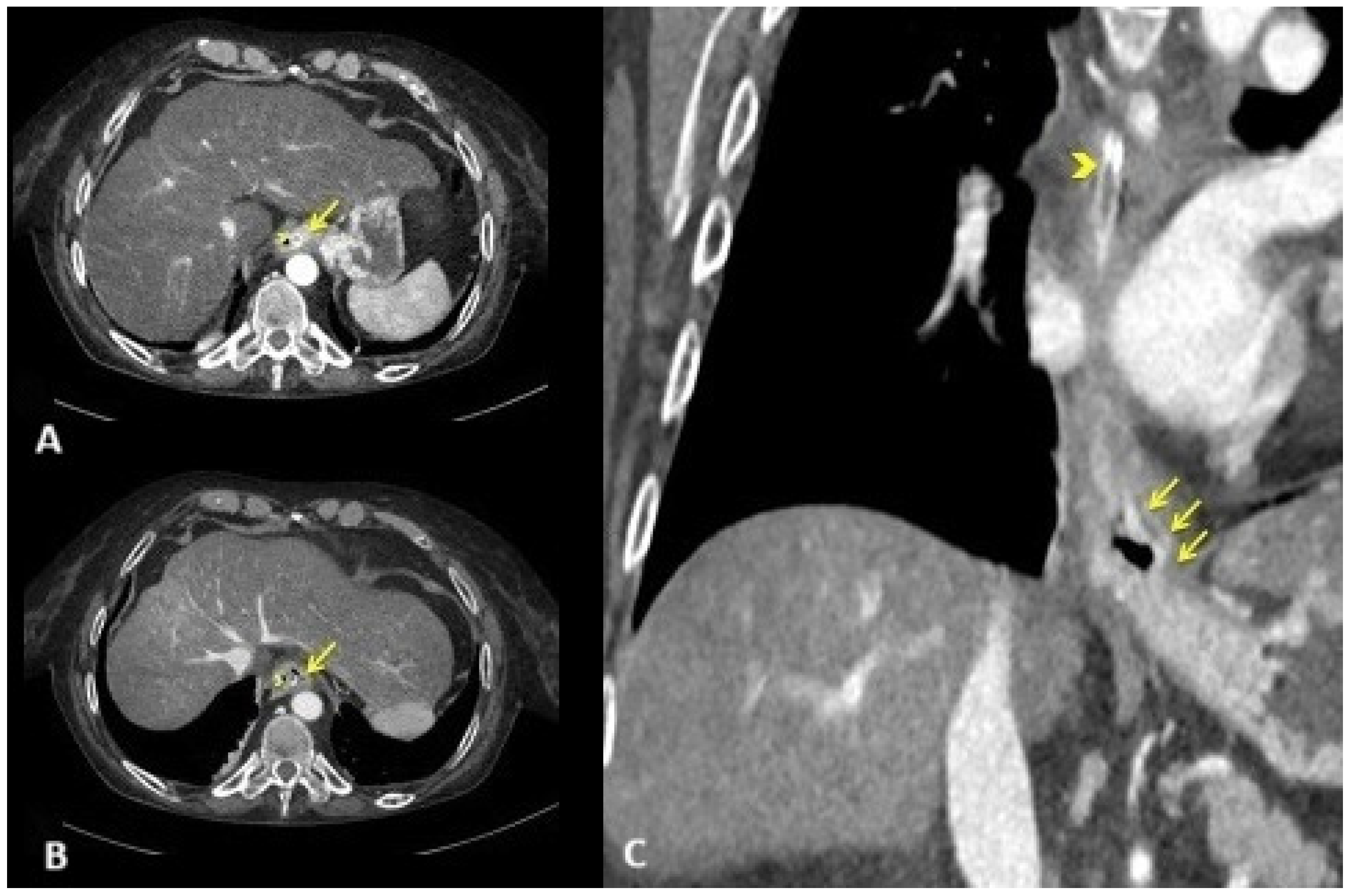
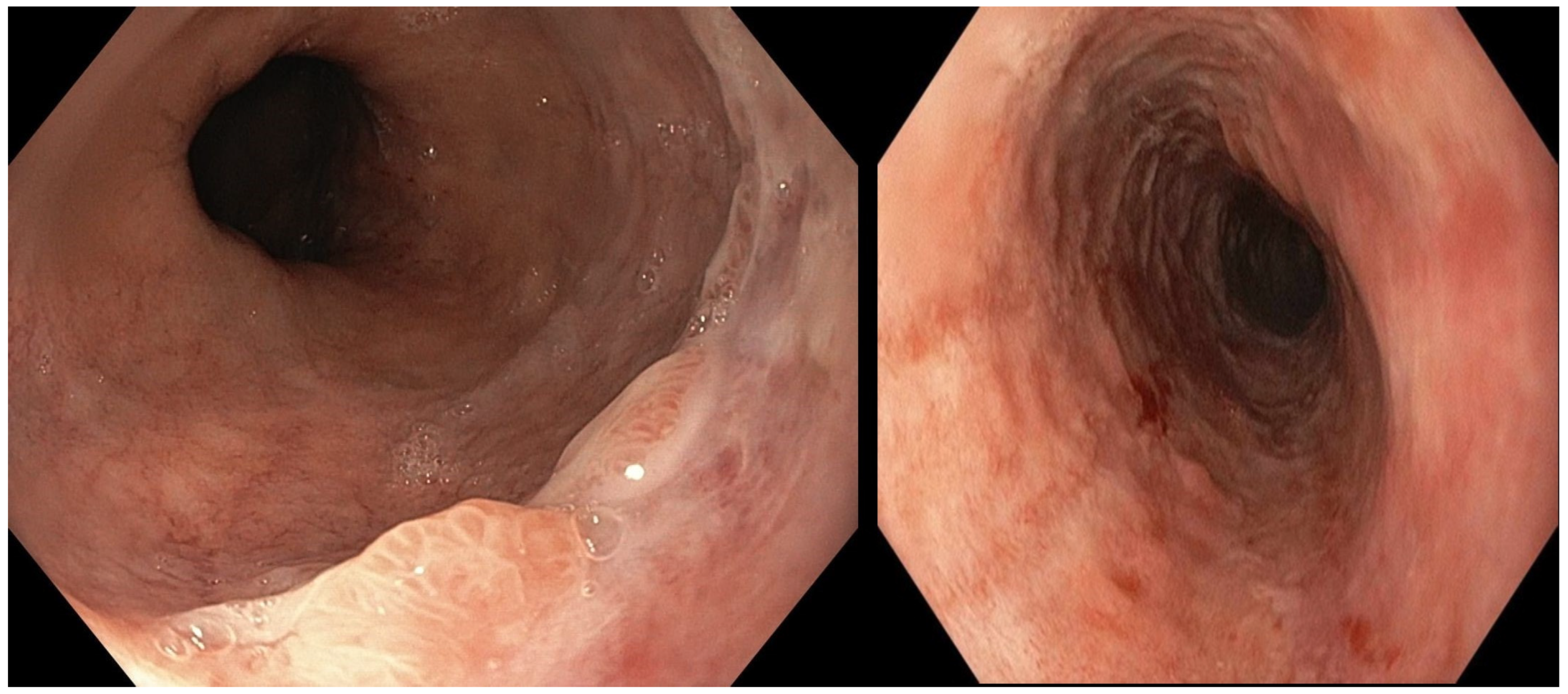
2.1. Diagnostic Evaluation
2.2. Treatment and Outcome
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goldenberg, S.P.; Wain, S.L.; Marignani, P. Acute necrotizing esophagitis. Gastroenterology 1990, 98, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Schizas, D.; Theochari, N.A.; Mylonas, K.S.; Kanavidis, P.; Spartalis, E.; Triantafyllou, S.; Economopoulos, K.P.; Theodorou, D.; Liakakos, T. Acute esophageal necrosis: A systematic review and pooled analysis. World J. Gastrointest. Surg. 2020, 27, 104–115. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gurvits, G.E. Black esophagus: Acute esophageal necrosis syndrome. World J. Gastroenterol. 2010, 14, 3219–3225. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sheikh, A.B.; Mirza, S.; Abbas, R.; Javed, N.; Nguyen, A.; Hanif, H.; Farooq, A. Acute Esophageal Necrosis: An In-depth Review of Pathogenesis, Diagnosis and Management. J Community Hosp. Intern. Med. Perspect. 2022, 31, 96–103. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Orlando, D.; Carabotti, M.; Ruggeri, M.; Esposito, G.; Corleto, V.D.; Di Giulio, E.; Annibale, B. Occurrence of Acute Oesophageal Necrosis (Black Oesophagus) in a Single Tertiary Centre. J. Clin. Med. 2019, 24, 1532. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lamers, C.R.; Mares, W.G.N.; Bac, D.J. Black esophagus: A case series and literature review of acute esophageal necrosis. Scand. J. Gastroenterol. 2018, 53, 1421–1424. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, A.; Chaudhary, F.S.; Naqvi, H.A.; Saleh, N.; Farooqi, R.; Yousaf, M.N. Black esophagus: A syndrome of acute esophageal necrosis associated with active alcohol drinking. BMJ Open Gastroenterol. 2020, 7, e000466. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abdullah, H.M.; Ullah, W.; Abdallah, M.; Khan, U.; Hurairah, A.; Atiq, M. Clinical presentations, management, and outcomes of acute esophageal necrosis: A systemic review. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Endo, T.; Sakamoto, J.; Sato, K.; Takimoto, M.; Shimaya, K.; Mikami, T.; Munakata, A.; Shimoyama, T.; Fukuda, S. Acute esophageal necrosis caused by alcohol abuse. World J. Gastroenterol. 2005, 21, 5568–5570. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rehman, O.; Jaferi, U.; Padda, I.; Khehra, N.; Atwal, H.; Parmar, M. Epidemiology, Pathogenesis, and Clinical Manifestations of Acute Esophageal Necrosis in Adults. Cureus 2021, 25, e16618. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gurvits, G.E.; Shapsis, A.; Lau, N.; Gualtieri, N.; Robilotti, J.G. Acute esophageal necrosis: A rare syndrome. J. Gastroenterol. 2007, 42, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Augusto, F.; Fernandes, V.; Cremers, M.I.; Oliveira, A.P.; Lobato, C.; Alves, A.L.; Pinho, C.; de Freitas, J. Acute necrotizing esophagitis: A large retrospective case series. Endoscopy 2004, 36, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Gurvits, G.E.; Cherian, K.; Shami, M.N.; Korabathina, R.; El-Nader, E.M.; Rayapudi, K.; Gandolfo, F.J.; Alshumrany, M.; Patel, H.; Chowdhury, D.N.; et al. Black esophagus: New insights and multicenter international experience in 2014. Dig. Dis. Sci. 2015, 60, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Ben Soussan, E.; Savoye, G.; Hochain, P.; Hervé, S.; Antonietti, M.; Lemoine, F.; Ducrotté, P. Acute esophageal necrosis: A 1-year prospective study. Gastrointest. Endosc. 2002, 56, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Dias, E.; Santos-Antunes, J.; Macedo, G. Diagnosis and management of acute esophageal necrosis. Ann. Gastroenterol. 2019, 32, 529–540. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Templeton, A.H.; Carter, K.L.; Sheron, N.; Gallagher, P.J.; Verrill, C. Sudden unexpected death in alcohol misuse--an unrecognized public health issue? Int. J. Environ. Res. Public Health 2009, 6, 3070–3081. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stacpoole, P.W.; Wright, E.C.; Baumgartner, T.G.; Bersin, R.M.; Buchalter, S.; Curry, S.H.; Duncan, C.; Harman, E.M.; Henderson, G.N.; Jenkinson, S.; et al. Natural history course of acquired lactic acidosis in adults DCA-Lactic Acidosis Study Group. Am. J. Med. 1994, 97, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.C.; Chan, K.S.; Tseng, K.L.; Weng, S.F. Prognosis of alcohol-associated lactic acidosis in critically ill patients: An 8-year study. Sci. Rep. 2016, 6, 35368. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kraut, J.A.; Madias, N.E. Lactic Acidosis: Current Treatments and Future Directions. Am. J. Kidney Dis. 2016, 68, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Karthiraj, N.; Ramakrishnan, N.; Mani, A.K. Hemodialysis for Lactic Acidosis. Indian J. Crit. Care Med. 2017, 21, 537–538. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orsini, L.; Martino, A.; Picascia, O.; Di Serafino, M.; Lombardi, G. Multidisciplinary Management of Acute Esophageal Necrosis Secondary to Alcoholic Lactic Acidosis: A Case Report. Reports 2025, 8, 25. https://doi.org/10.3390/reports8010025
Orsini L, Martino A, Picascia O, Di Serafino M, Lombardi G. Multidisciplinary Management of Acute Esophageal Necrosis Secondary to Alcoholic Lactic Acidosis: A Case Report. Reports. 2025; 8(1):25. https://doi.org/10.3390/reports8010025
Chicago/Turabian StyleOrsini, Luigi, Alberto Martino, Ornella Picascia, Marco Di Serafino, and Giovanni Lombardi. 2025. "Multidisciplinary Management of Acute Esophageal Necrosis Secondary to Alcoholic Lactic Acidosis: A Case Report" Reports 8, no. 1: 25. https://doi.org/10.3390/reports8010025
APA StyleOrsini, L., Martino, A., Picascia, O., Di Serafino, M., & Lombardi, G. (2025). Multidisciplinary Management of Acute Esophageal Necrosis Secondary to Alcoholic Lactic Acidosis: A Case Report. Reports, 8(1), 25. https://doi.org/10.3390/reports8010025