
Tubo-Ovarian Abscess with Actinomyces odontolyticus: Case Report and Brief Review of Literature


 ,
,  ,
,
Abstract
1. Introduction
2. Case Report
3. Review of Literature
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hall, V.; Copsey, S. Propionibacterium, Lactobacillus, Actinomyces, and other non-spore-forming anaerobic gram-positive rods. In Manual of Clinical Microbiology, 11th ed.; Jorgensen, J., Carroll, C.J., Funke, G., Pfaller, A.M., Landry, L.M., Richter, S.S., Warnock, W.D., Eds.; ASM Press: Washington, DC, USA, 2015; p. 920. [Google Scholar]
- Valour, F.; Sénéchal, A.; Dupieux, C.; Karsenty, J.; Lustig, S.; Breton, P.; Gleizal, A.; Boussel, L.; Laurent, F.; Braun, E.; et al. Actinomycosis: Etiology, clinical features, diagnosis, treatment and management. Infect. Drug Resist. 2014, 7, 183. [Google Scholar]
- Cintron, J.R.; Del Pino, A.; Duarte, B.; Wood, D. Abdominal actinomycosis. Dis. Colon Rectum 1996, 39, 105. [Google Scholar] [CrossRef]
- Ortiz, M.E.; Croxatto, H.B.; Bardin, C.W. Mechanisms of Action of Intrauterine Devices. Obstet. Gynecol. Surv. 1996, 51 (Suppl. S12), 42S–51S. [Google Scholar] [CrossRef]
- Liljemark, W.F.; Bloomquist, C.G.; Bandt, C.L.; Pihlstrom, B.L.; Hinrichs, J.E.; Wolff, L.F. Comparison of the distribution of Actinomyces in dental plaque on inserted enamel and natural tooth surfaces in periodontal health and disease. Oral Microbiol. Immunol. 1993, 8, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.M.; Noska, A. Intrauterine device infection causing concomitant streptococcal toxic shock syndrome and pelvic abscess with Actinomyces odontolyticus bacteraemia. BMJ Case Rep. 2016, 2016, bcr2015213236. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.M.; Beck, P.P.; Vaznitsel, M.; Bran-Acevedo, A.; Hunter, M.; Ang, J.R.; Roland, W. Acute disseminated actinomycosis presenting as pneumonia with bilateral pulmonary nodules and pelvic osteomyelitis in an immunocompetent patient. IDCases 2022, 29, e01540. [Google Scholar] [CrossRef] [PubMed]
- Furuya, K.; Ito, K.; Sugiyama, K.; Fujita, A.; Kanemoto, H.; Shimada, T. A case of recurrent acute cholecystitis caused by Actinomyces odontolyticus, rare actinomycosis. BMC Infect. Dis. 2022, 22, 518. [Google Scholar] [CrossRef]
- Tu, J.; MacDonald, M.; Mansfield, D. Pulmonary actinomycosis and polymicrobial empyema in a patient with ABPA and bronchocoele. Respirol. Case Rep. 2022, 10, e0954. [Google Scholar] [CrossRef]
- Deltenre, M.; Thimmesch, M.; Creuven, M.; Pierart, F. Pulmonary actinomycosis caused by Actinomyces odontolyticus in a two-year-old child. Rev. Mal. Respir. 2022, 39, 270–274. [Google Scholar] [CrossRef]
- Razok, A.; Ali, M.; Aker, L.; Ziglam, H. Actinomyces odontolyticus bacteraemia associated with cervical and mediastinal abscesses in an immunocompetent patient: First reported case in Qatar. New Microbes New Infect. 2022, 45, 100956. [Google Scholar] [CrossRef]
- Kitano, H.; Hieda, K.; Kitagawa, H.; Nakaoka, Y.; Koba, Y.; Ota, K.; Shigemoto, N.; Hayashi, T.; Kashiyama, S.; Teishima, J.; et al. Case Report: Emphysematous Pyelonephritis With a Congenital Giant Ureterocele. Front. Pediatr. 2021, 9, 775468. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.-L.; Wu, C.-T.; Chang, Y.-C.; Fan, C.-K.; Lee, Y.-J. Case report of an unusual hepatic abscess caused by Actinomyces odontolyticus in a patient with human immunodeficiency virus infection. BMC Infect. Dis. 2021, 21, 998. [Google Scholar] [CrossRef] [PubMed]
- Farah Khoury, M.; Perek, S.; Raz-Pasteur, A. Implantable cardioverter defibrillator related Actinomyces Odontolyticus endocarditis and bacteremia-First reported case. IDCases 2021, 25, e01228. [Google Scholar] [CrossRef] [PubMed]
- Marques, P.M.; Quaresma, M.M.; Haghighi, E.; Barata, J.A. Radiation proctitis-related lumbar spondylodiscitis due to Actinomyces odontolyticus: A rare finding. BMJ Case Rep. 2021, 14, e237047. [Google Scholar] [CrossRef]
- Jain, H.; Singh, G.; Eranki, A. Actinomyces odontolyticus causing meningitis and cervical abscess. Bayl. Univ. Med. Cent. Proc. 2021, 34, 492–493. [Google Scholar] [CrossRef]
- Patel, K.; MacDonald, M.; Hmoud, H.; Czinn, E.; Wutawunashe, C.; Fisher, P. Aortic valve endocarditis by Actinomyces odontolyticus and Gemella morbillorum oral pathogens. IDCases 2021, 24, e01079. [Google Scholar] [CrossRef]
- Massey, M.; Barney, J. Pulmonary actinomycosis and marijuana vaping. BMJ Case Rep. 2021, 14, e240973. [Google Scholar] [CrossRef]
- Khiatah, B.; Shah, K.; Belikova, A.; Saeed, M. Sepsis due to Actinomyces odontolyticus as a Rare Complication of Neobladder. Case Rep. Infect. Dis. 2021, 2021, 6699046. [Google Scholar] [CrossRef] [PubMed]
- Tseng, J.; Wu, J.; Wang, J.; Tung, C. Suppurative mediastinal lymphadenitis caused by Actinomyces odontolyticus: Successfully diagnosed by endobronchial ultrasound-guided transbronchial needle aspiration. J. Postgrad. Med. 2021, 67, 46–48. [Google Scholar] [CrossRef]
- Yesilbas, O.; Yozgat, C.Y.; Nizam, O.G.; Duramaz, B.B.; Turel, O. Life-threatening multiple brain abscesses secondary to Actinomyces odontolyticus. Pediatr. Int. 2020, 62, 1307–1308. [Google Scholar] [CrossRef]
- Rueda, M.S.; Hefter, Y.; Stone, B.; Hahn, A.; Jantausch, B. A Premature Infant with Neonatal Actinomyces odontolyticus Sepsis. J. Pediatr. Infect. Dis. Soc. 2021, 10, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.J.; Shupak, R.P. Cervicofacial actinomycosis of the mandible in a paediatric patient. BMJ Case Rep. 2020, 13, e233681. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, H.; Wu, D.; Feng, M.; Yang, P.; Hu, X.; Tattevin, P.; Hong, G.; Chen, R.; Qiu, C. Pulmonary lesions associated with sputum culture-positive actinomycetes: Report of one case. Ann. Transl. Med. 2019, 7, 793. [Google Scholar] [CrossRef]
- Diab, C.; Almarzouq, A.; Ajise, O.; Barkati, S.; Tchervenkov, J.; Andonian, S. Renal actinomycosis presenting as uro-cutaneous fistula. Urol. Case Rep. 2019, 28, 101054. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Kusakabe, Y.; Enomoto, M.; Yamamoto, N.; Aihara, K.; Yamaoka, S.; Mishima, M. Drastically progressive lung cavity lesion caused by Actinomyces odontolyticus in a patient undergoing chemoradiotherapy: A case report and literature review. Respir. Med. Case Rep. 2019, 28, 100950. [Google Scholar] [CrossRef] [PubMed]
- Crisafulli, E.; Bernardinello, N.; Alfieri, V.; Pellegrino, F.; Lazzari, C.; Gnetti, L.; Chetta, A. A pulmonary infection by Actinomyces odontolyticus and Veillonella atypica in an immunocompetent patient with dental caries. Respirol. Case Rep. 2019, 7, e00493. [Google Scholar] [CrossRef]
- Yun, S.S.; Cho, H.S.; Heo, M.; Jeong, J.H.; Lee, H.R.; Ju, S.; Kim, J.Y.; You, J.W.; Cho, Y.J.; Jeong, Y.Y.; et al. Lung abscess by Actinomyces odontolyticus and Parvimonas micra co-infection presenting as acute respiratory failure: A case report. Medicine 2019, 98, e16911. [Google Scholar] [CrossRef]
- Schimmel, T.; Trawinski, H.; Karlas, T.; Wendt, S.; Lübbert, C. Polymicrobial liver abscesses and pleural empyema in a 40-year-old male after tooth extraction and closed periodontal treatment: A case report. Z Gastroenterol. 2019, 57, 600–605. [Google Scholar]
- Clyde, M.; McAllister, J.; Obeidallah, A.; Ahmad, I. Actinomyces odontolyticus infection 3 months post-robotic-assisted laparoscopic prostatectomy. BMJ Case Rep. 2019, 12, e228184. [Google Scholar] [CrossRef]
- Palmitessa, V.; Cuppone, R.; Monno, R.; Fumarola, L.; Lippolis, A. A case report of esophageal actinomycosis in an immunocompetent patient and review of the literature. New Microbiol. 2019, 42, 55–60. [Google Scholar]
- Gray, A.; Do, P. The case of the unwanted crystal: A case of pediatric pulmonary Actinomyces odonolyticus. Clin. Case Rep. 2018, 6, 1230–1231. [Google Scholar] [CrossRef] [PubMed]
- Prashant, N.; Azuhairy, A. Actinomycosis of Distal Phalanx Twenty Years after Flap Reconstruction of Index Finger: A Case Report. Malays. Orthop. J. 2018, 12, 48–50. [Google Scholar] [PubMed]
- Yanagisawa, R.; Minami, K.; Kubota, N.; Iwade, T.; Ogiso, Y. Asymptomatic subcutaneous cervical mass due to Actinomyces odontolyticus infection in a pyriform sinus fistula. Pediatr. Int. 2017, 59, 941–942. [Google Scholar] [CrossRef]
- Broly, E.; Risse, J.; Maschino, F.; Wahl, D. Cardiac Tamponade Due to Actinomyces odontolyticus Originating from a Dentigerous Cyst. J. Oral Maxillofac. Surg. 2016, 74, 2453–2456. [Google Scholar] [CrossRef]
- Weiand, D.; Barlow, G. The rising tide of bloodstream infections with Actinomyces species: Bimicrobial infection with Actinomyces odontolyticus and Escherichia coli in an intravenous drug user. Oxf. Med. Case Rep. 2014, 2014, 156–158. [Google Scholar] [CrossRef] [PubMed]
- Nebrera Navarro, F.; Ramirez Portero, C. Actinomyces odontolyticus pneumonia in a patient with iatrogenic A-hypogammaglobulinemia. Med. Clin. (Barc.) 2015, 145, 458. [Google Scholar] [CrossRef] [PubMed]
- Lensing, F.; Abele, T.; Wiggins, R., 3rd; Quigley, E. Laryngeal actinomycosis. Proc. Bayl. Univ. Med. Cent. 2014, 27, 35–36. [Google Scholar] [CrossRef] [PubMed]
- Rich, B.S.; Angeles, C.; Barie, P.S. Actinomyces odontolyticus Breast Abscess. Surg. Infect. 2013, 14, 331–332. [Google Scholar] [CrossRef]
- Chao, C.-T.; Liao, C.-H.; Lai, C.-C.; Hsueh, P.-R. Liver abscess due to Actinomyces odontolyticus in an immunocompetent patient. Infection 2011, 39, 77–79. [Google Scholar] [CrossRef]
- Antony, B.; Shivakumarappa, G.M.; Mohan, D.R. Empyema thoracis due to actinomyces odontolyticus. Indian J. Pathol. Microbiol. 2009, 52, 120. [Google Scholar] [CrossRef]
- Davanos, E.; Rahman, S.M.; Nogid, B. Treatment of Eikenellacorrodens and Actinomyces odontolyticus foot abscess in a penicillin-allergic patient. Ann. Pharmacother. 2008, 42, 1706–1710. [Google Scholar] [CrossRef] [PubMed]
- Pant, R.; Marshall, T.L.; Crosher, R.F. Facial actinomycosis mimicking a desmoid tumour: Case report. Br. J. Oral Maxillofac. Surg. 2008, 46, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Delarbre, X.; Auzary, C.; Bahnini, A.; Nordmann, P.; Delfraissy, J.F. Actinomyces odontolyticus isolation during prosthetic aortic graft infection with paraprosthetic duodenal fistula. Rev. Med. Interne 2007, 28, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Louerat, C.; Depagne, C.; Nesme, P.; Biron, F.; Guerin, J.C. Disseminated actinomycosis. Rev. Mal. Respir. 2005, 22, 473–476. [Google Scholar] [CrossRef]
- Cone, L.A.; Leung, M.M.; Hirschberg, J. Actinomyces odontolyticus bacteremia. Emerg. Infect. Dis. 2003, 9, 1629–1632. [Google Scholar] [CrossRef]
- Sofianou, D.; Avgoustinakis, E.; Dilopoulou, A.; Pournaras, S.; Tsirakidis, G.; Tsakris, A. Soft-tissue abscess involving Actinomyces odontolyticus and two Prevotella species in an intravenous drug abuser. Comp. Immunol. Microbiol. Infect. Dis. 2004, 27, 75–79. [Google Scholar] [CrossRef]
- Takiguchi, Y.; Terano, T.; Hirai, A. Lung Abscess Caused by Actinomyces odontolyticus. Intern. Med. 2003, 42, 723–725. [Google Scholar] [CrossRef] [PubMed]
- Alamillos-Granados, F.; Dean-Ferrer, A.; Garcίa-López, A.; López-Rubio, F. Actinomycotic ulcer of the oral mucosa: An unusual presentation of oral actinomycosis. Br. J. Oral Maxillofac. Surg. 2000, 38, 121–123. [Google Scholar] [CrossRef]
- Iancu, D.; Chua, A.; Schoch, P.E.; Cunha, B.A. Actinomyces odontolyticus pulmonary infection. Am. J. Med. 1999, 107, 293–294. [Google Scholar]
- Litwin, K.A.; Jadbabaie, F.; Villanueva, M. Case of Pleuropericardial Disease Caused by Actinomyces odontolyticus that Resulted in Cardiac Tamponade. Clin. Infect. Dis. 1999, 29, 219–220. [Google Scholar] [CrossRef]
- Pérez-Castrillón, J.L.; Gonzalez-Castaneda, C.; del Campo-Matias, F.; Bellido-Casado, J.; Diaz, G. Empyema Necessitatis due to Actinomyces odontolyticus. Chest 1997, 111, 1144. [Google Scholar] [CrossRef] [PubMed]
- Simpson, A.J.; Das, S.S.; Mitchelmore, I.J. Polymicrobial brain abscess involving Haemophilus paraphrophilus and Actinomyces odontolyticus. Postgrad. Med. J. 1996, 72, 297–298. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bassiri, A.G.; Girgis, R.E.; Theodore, J. Actinomyces odontolyticus thoracopulmonary infections. Two cases in lung and heart-lung transplant recipients and a review of the literature. Chest 1996, 109, 1109–1111. [Google Scholar] [PubMed]
- Dontfraid, F.; Ramphal, R. Bilateral Pulmonary Infiltrates in Association with Disseminated Actinomycosis. Clin. Infect. Dis. 1994, 19, 143–145. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.; Bayardelle, P.; Bélanger, R.; Fortin, L. Sacroiliitis and septicemia caused by Campylobacter rectus and Actinomyces odontolyticus. Can. J. Infect. Dis. 1994, 5, 133–136. [Google Scholar] [PubMed]
- Civen, R.; Väisänen, M.-L.; Finegold, S.M. Peritonsillar Abscess, Retropharyngeal Abscess, Mediastinitis, and Nonclostridial Anaerobic Myonecrosis: A Case Report. Clin. Infect. Dis. 1993, 16 (Suppl. S4), S299–S303. [Google Scholar] [CrossRef]
- Verrot, D.; Disdier, P.; Harlé, J.R.; Peloux, Y.; Garbes, L.; Arnaud, A.; Weiller, P.J. Pulmonary actinomycosis: Caused by Actinomyces odontolyticus? Rev. Med. Interne 1993, 14, 179–181. [Google Scholar] [CrossRef]
- Hooi, L.N.; Na, B.S.; Sin, K.S. A case of empyema thoracis caused by actinomycosis. Med. J. Malays. 1992, 47, 311–315. [Google Scholar]
- Peloux, Y.; Raoult, D.; Chardon, H.; Escarguel, J. Actinomyces odontolyticus infections: Review of six patients. J. Infect. 1985, 11, 125–129. [Google Scholar] [CrossRef]
- Klaaborg, K.-E.; Kronborg, O.; Olsen, H. Enterocutaneous fistulization due to Actinomyces odontolyticus. Report of a case. Dis. Colon Rectum 1985, 28, 526–527. [Google Scholar] [CrossRef]
- Ruutu, P.; Pentikäinen, P.J.; Larinkari, U.; Lempinen, M. Hepatic actinomycosis presenting as repeated cholestatic reactions. Scand. J. Infect. Dis. 1982, 14, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Baron, E.J.; Angevine, J.M.; Sundstrom, W. Actinomycotic pulmonary abscess in an immunosuppressed patient. Am. J. Clin. Pathol. 1979, 72, 637–639. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.D.; Hintz, C.S.; Haselby, R.C. Malar mass due to Actinomyces odontolyticus. J. Clin. Microbiol. 1977, 5, 658–660. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Zhang, P.; Jiao, G.; Lv, J.; Ma, C.; Song, X.; Zhang, J.; Wu, C.; Li, R.; Zhu, H. Mimicking uterine malignancy: Pelvic actinomycosis with giant uterine leiomyoma. IDCases 2020, 23, e00878. [Google Scholar] [CrossRef] [PubMed]
- García-García, A.; Ramírez-Durán, N.; Sandoval-Trujillo, H.; Romero-Figueroa, M.D.S. Pelvic actinomycosis. Can. J. Infect. Dis. Med. Microbiol. 2017, 2017, 9428650. [Google Scholar] [CrossRef]
- Liu, Y. Actinomycosis-induced adnexal and uterine masses mimicking malignancy on FDG PET/CT. Am. J. Obstet. Gynecol. 2019, 220, 281. [Google Scholar] [CrossRef]
- Guo, L.; Ye, L.; Zhao, Q.; Ma, Y.; Yang, J.; Luo, Y. Comparative study of MALDI-TOF MS and VITEK 2 in bacteria identification. J. Thorac. Dis. 2014, 6, 534–538. [Google Scholar]
- Rudolph, W.W.; Gunzer, F.; Trauth, M.; Bunk, B.; Bigge, R.; Schröttner, P. Comparison of VITEK 2, MALDI-TOF MS, 16S rRNA gene sequencing, and whole-genome sequencing for identification of Roseomonas mucosa. Microb. Pathog. 2019, 134, 103576. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference | Patient Age | Gender | Site of Infection | Microorganism Identification | Relevant Comorbidities/Invasive Procedures | Immune Status | Outcome |
|---|---|---|---|---|---|---|---|
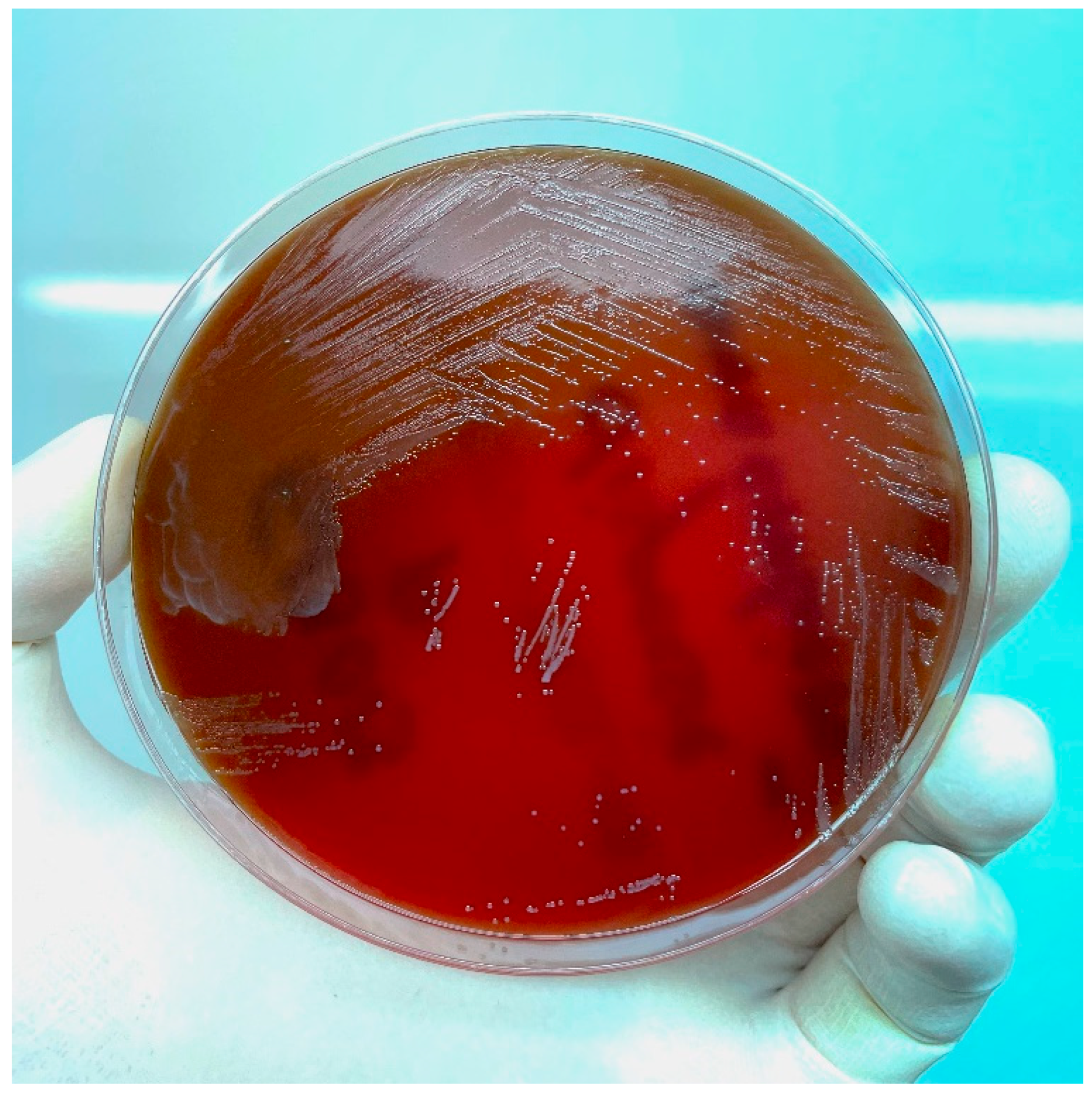
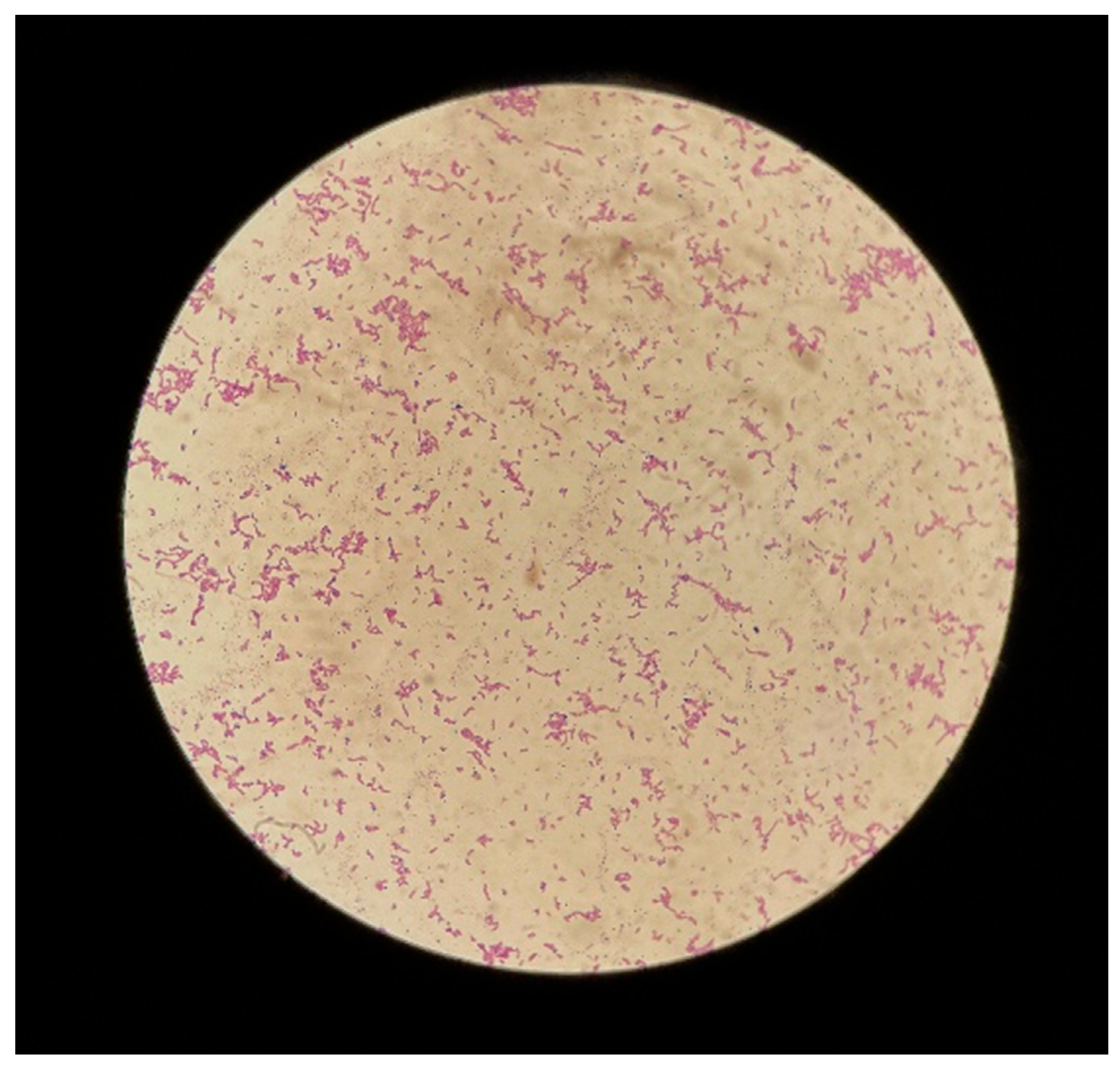
| This study | 48 | F | Tubo-ovarian | Gram stain, culture media aspect, and Vitek | Presence of IUD | Immunocompetent | Complete recovery |
| Patil SM. et al. [7] | 53 | M | Disseminated: pelvic and pulmonary | Gram stain and histopathological exam from pelvic fluid | Poor dental hygiene | Immunocompetent | Complete recovery |
| Furuya K. et al. [8] | 75 | M | Cholecist | Gram stain from bile | Recurring cholecystitis | Immunocompetent | Complete recovery |
| Tu J. et al. [9] | 43 | F | Pulmonary | N/A | Bronhocoele, Allergic pulmonary aspergillosis, recent tooth extraction, co-infection with L. rhamnosus and S. mitis | Immunocompetent | Ameliorated |
| Deltenre M. et al. [10] | 2 | M | Pulmonary | N/A | Acute bronchitis | Immunocompetent | Complete recovery |
| Razok A. et al. [11] | 32 | M | Disseminated: cervical and mediastinal | Pheonix technique, Maldi-TOF, DNA restriction analysis | Tooth extraction | Immunocompetent | Complete recovery |
| Kitano H. et al. [12] | 14 | F | Renal | MALDI-TOF | Co-infection with A. schaalii and P. asaccarolyticus | Immunocompetent | Ameliorated |
| Hsu SL. et al. [13] | 45 | M | Hepatic | MALDI-TOF | HIV infection, co-infection with C. albicans and S. constellatus | Immunodeficient | Died |
| Farah K.M. et al. [14] | 54 | M | Cardiac | Gram stain | Type 2 diabetes, chronic kidney disease, heart failure, cardioverter defibrillator implanted recently | Immunodeficient | Complete recovery |
| Marques PM. et al. [15] | 75 | M | L4–L5 vertebrae | Histopathological exam | Rectal adenocarcinoma with radiotherapy | Immunodeficient | Ameliorated |
| Jain H. et al. [16] | 73 | M | Disseminated: cervical, meningeal | N/A | Oropharyngeal carcinoma with chemotherapy | Immunodeficient | Complete recovery |
| Patel K. et al. [17] | 56 | F | Cardiac | N/A | Poor dental hygiene, aortic insufficiency | Immunocompetent | Complete recovery |
| Massey M. et al. [18] | 33 | M | Pulmonary | N/A | None | Immunocompetent | Complete recovery |
| Khiatak B. et al. [19] | 83 | M | Disseminated: sepsis | Gram stain, histopathological exam with immunofluorescence technique | Urothelial carcinoma | Immunodeficient | Ameliorated |
| Wu JJ. et al. [20] | 71 | M | Mediastinal | N/A | Chronic hepatitis C, hepatocellular carcinoma | Immunodeficient | Complete recovery |
| Yesilbas O. et al. [21] | 2.5 | M | Cerebral | Vitek | Abscess on the left hand | Immunocompetent | Complete recovery |
| Rueda MS. et al. [22] | Newborn | M | Disseminated: sepsis | MALDI-TOF | Dental infection 1 week pre-partum(mother) Premature (26 weeks old) | Immunodeficient | Complete recovery |
| Cho JJ. et al. [23] | 10 | F | Cervicofacial | Gram stain, culture media aspect | None | Immunocompetent | Complete recovery |
| Wang L. et al. [24] | 34 | M | Pulmonary | High-throughput gene detection | Undefined lung lesions | Immunocompetent | Complete recovery |
| Diab C. et al. [25] | 36 | M | Renal | Histopathological exam | Xanthogranulomatous pyelonephritis with calculus and urocutaneous fistula | Immunocompetent | Complete recovery |
| Matsumoto T. et al. [26] | 60 | M | Pulmonary | MALDI-TOF | Squamous cell lung carcinoma with chemo- and radiotherapy | Immunodeficient | Ameliorated |
| Crisafulli E. et al. [27] | 65 | M | Pulmonary | MALDI-TOF | Poor oral hygiene, co-infection with V. atypica | Immunocompetent | Complete recovery |
| Yun SS et al. [28] | 49 | M | Pulmonary | N/A | Poor oral hygiene | Immunocompetent | Complete recovery |
| Schimmel T. et al. [29] | 40 | M | Disseminated: hepatic, pleural | N/A | Multiple teeth extractions, co-infection with S. anginosus, S.constellatus, P. denticola | Immunocompetent | Complete recovery |
| Clyde M. et al. [30] | 60 | M | Pelvic:lymphocele | N/A | Prostatectomy | Immunocompetent | Complete recovery |
| Palmitessa V et al. [31] | 23 | M | Esophageal | Vitek | Refractory GERD | Immunocompetent | Complete recovery |
| Gray A. et al. [32] | 11 | F | Pulmonary | N/A | Recurrent pneumonia | Immunocompetent | Complete recovery |
| Prashant N. et al. [33] | N/A | M | 2nd phalanx | N/A | Degloving injury of the index finger treated with an anterior chest wall flap | Immunocompetent | Complete recovery |
| Yanagisawa R. et al. [34] | 2 | M | Cervical | 16S rRNA sequencing | None | Immunocompetent | Complete recovery |
| Broly E. et al. [35] | 52 | F | Pericardiac | N/A | Dentigerous cyst | Immunocompetent | Complete recovery |
| Wu CM. et al. [6] | 50 | F | Pelvic | Vitek | Presence of IUD, toxic shock syndrome with group A Streptococcus | Immunocompetent | Ameliorated |
| Weiand D. et al. [36] | 36 | M | Bacteriemia | Vitek,MALDI-TOF | Intravenous drug user, co-infection with E. coli | Immunodeficient | Ameliorated |
| NebreraNavaro F. et al. [37] | 68 | F | Pulmonary | 16S rRNA sequencing | Hodgkin’s lymphoma with chemotherapy, IgA deficit | Immunodeficient | Ameliorated |
| Lensing F. et al. [38] | 24 | M | Laryngeal | N/A | Inhalation injuries with subglottic stenosis | Immunocompetent | Complete recovery |
| Rich BS. et al. [39] | 40 | F | Breast | N/A | None | Immunocompetent | Complete recovery |
| Chao CT. et al. [40] | 78 | M | Hepatic | API, 16S rRNA sequencing | Dental procedures—tooth remodeling and replacement | Immunocompetent | Complete recovery |
| Mohan DR. et al. [41] | 68 | M | Pulmonary | Culture media aspect, Gram stain, biochemical properties | Poor oral hygiene | Immunocompetent | Complete recovery |
| Davanos E. et al. [42] | 39 | F | Right foot | Gram stain and culture media aspect | Type 2 diabetes, right foot injury, co-infection with E. corrodens | Immunodeficient | Complete recovery |
| Pant E. et al. [43] | 40 | M | Facial | Histopathological exam | Desmoid tumor | Immunocompetent | Complete recovery |
| Delarbre X. et al. [44] | 73 | M | Vascular (prosthetic aortic graft) | N/A | Periodontal disease | Immunocompetent | Complete recovery |
| Louerat C. et al. [45] | 52 | M | Disseminated: cerebral, pulmonary | N/A | Alcoholism | Immunocompetent | Ameliorated |
| Cone LA. et al. [46] | 62 | F | Bacteriemia | RapID ANA II System | Acute myelocytic leukmia with chemotherapy | Immunodeficient | Complete recovery |
| Cone LA. et al. [46] | 69 | F | Bacteriemia | RapID ANA II System | Giant cell arteritis, Azathioprine therapy | Immunodeficient | Complete recovery |
| Sofianou D. et al. [47] | 32 | M | Soft tissue (right femoral area) | API A System, Vitek, API 20NE System | Intravenous drug user | Immunodeficient | Ameliorated |
| Takiguchi Y. et al. [48] | 64 | F | Pulmonary | RapID ANA II System | Periodontal disease | Immunocompetent | Ameliorated |
| Alamillos-Granado FJ. et al. [49] | 74 | F | Oral mucosa | N/A | Insulin-dependent type 2 diabetes, recent dental extraction | Immunodeficient | Complete recovery |
| Iancu D. et al. [50] | 37 | F | Pulmonary | N/A | Sarcoidosis with prednisone therapy, diffuse large (B cell) lymphoma | Immunodeficient | Died |
| Litwin KA. et. al. [51] | 68 | M | Disseminated: pleural, pericardial | API 20A/An-IDENT System | Gastric surgery | Immunocompetent | Complete recovery |
| Pérez-Castrillón JL. et al. [52] | 50 | M | Pleural | N/A | Pneumectomy, pulmonary tuberculosis | Immunocompetent | Complete recovery |
| Simpson AJ. et al. [53] | 66 | F | Cerebral | N/A | Granuloma below a pre-molar tooth | Immunocompetent | Ameliorated |
| Bassiri AG. et al. [54] | 61 | M | Pulmonary | N/A | Lung transplant recipient (emphysema) | Immunodeficient | Complete recovery |
| Bassiri AG. et al. [54] | 43 | M | Disseminated: pericardial, mediastinal, osseous | N/A | Heart-lung transplant recipient (sarcoidosis, bullous lung disease) | Immunodeficient | Died |
| Dontfraid F. et al. [55] | 52 | M | Pulmonary | Vitek | Poor dental hygiene, periodontal disease, left ankle injury, alcoholism | Immunocompetent | Complete recovery |
| Harvey P. et al. [56] | 37 | M | Osseous (sacroiliac joint) | BACTEC NR7A | Multiple dental abscesses | Immunocompetent | Complete recovery |
| Civen R. et al. [57] | 45 | M | Disseminated: tonsillar, retropharyngeal, mediastinal | Vitek | Alcohol and cocaine abuse | Immunocompetent | Complete recovery |
| Verrot D. et al. [58] | 52 | F | Pulmonary | Gram stain and culture media aspect | Dilated bronchi post-B.pertussis infection | Immunocompetent | Complete recovery |
| Hooi LN. et al. [59] | 38 | F | Pleural | Gram stain and culture media aspect | Poor dental hygiene | Immunocompetent | Complete recovery |
| Peloux Y. et al. [60] | 19 | M | Pleural | N/A | Co-infection with F. necrophorum | Immunocompetent | Complete recovery |
| Peloux Y. et al. [60] | 40 | M | Right thumb | N/A | Right thumb injury, poor dental hygiene, co-infection with K. pneumoniae | Immunocompetent | Complete recovery |
| Peloux Y. et al. [60] | 54 | F | Ovarian | N/A | Ovarian cysts, alcoholic, co-infection with E. coli | Immunocompetent | Complete recovery |
| Peloux Y. et al. [60] | 30 | F | N/A | N/A | Co-infection with H. influenzae | Immunocompetent | Complete recovery |
| Peloux Y. et al. [60] | 47 | M | Arm | N/A | Co-infection with S. millieri and H. aphrophilus | Immunocompetent | Complete recovery |
| Peloux Y. et al. [60] | 65 | M | Submaxillary | N/A | None | Immunocompetent | Complete recovery |
| Klaaborg KE. et al. [61] | 78 | M | Sigmoid colon | N/A | Right hemicolectomy (cecum carcinoma), diverticulitis of the sigmoid colon, enterocutaneous fistula | Immunocompetent | Ameliorated |
| Ruutu P. et al. [62] | 37 | F | Disseminated: hepatic, renal, pleural | Gas-liquid chromatography | Paradental abscess, presence of IUD | Immunocompetent | Ameliorated |
| Baron EJ. et al. [63] | 61 | F | Pulmonary | Gas chromatography, biochemical characteristics | Polyarthropathy with longstanding treatment with prednisone | Immunodeficient | Complete recovery |
| Mitchell PD. et al. [64] | 54 | M | Malar | Gram stain, biochemical characteristics | Poor dental hygiene, periodontal disease, repeated injuries in the malar region | Immunocompetent | Complete recovery |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pană, A.G.; Neculicioiu, V.; Toc, D.A.; Sprinjan, G.D.; Rusu, M.C.; Costache, C. Tubo-Ovarian Abscess with Actinomyces odontolyticus: Case Report and Brief Review of Literature. Reports 2022, 5, 46. https://doi.org/10.3390/reports5040046
Pană AG, Neculicioiu V, Toc DA, Sprinjan GD, Rusu MC, Costache C. Tubo-Ovarian Abscess with Actinomyces odontolyticus: Case Report and Brief Review of Literature. Reports. 2022; 5(4):46. https://doi.org/10.3390/reports5040046
Chicago/Turabian StylePană, Adrian Gabriel, Vlad Neculicioiu, Dan Alexandru Toc, Gheorghe Dan Sprinjan, Mara Cristina Rusu, and Carmen Costache. 2022. "Tubo-Ovarian Abscess with Actinomyces odontolyticus: Case Report and Brief Review of Literature" Reports 5, no. 4: 46. https://doi.org/10.3390/reports5040046
APA StylePană, A. G., Neculicioiu, V., Toc, D. A., Sprinjan, G. D., Rusu, M. C., & Costache, C. (2022). Tubo-Ovarian Abscess with Actinomyces odontolyticus: Case Report and Brief Review of Literature. Reports, 5(4), 46. https://doi.org/10.3390/reports5040046