
Intrathecal Cell Therapy with Autologous Bone Marrow Stromal Cells as a New Tool for Neurologic Sequels after Spinal Cord Surgery: A Report of Two Cases

 ,
,
Abstract
1. Introduction
2. Cases
2.1. Patient Selection
2.2. Cell Therapy Treatment
3. Description of Cases
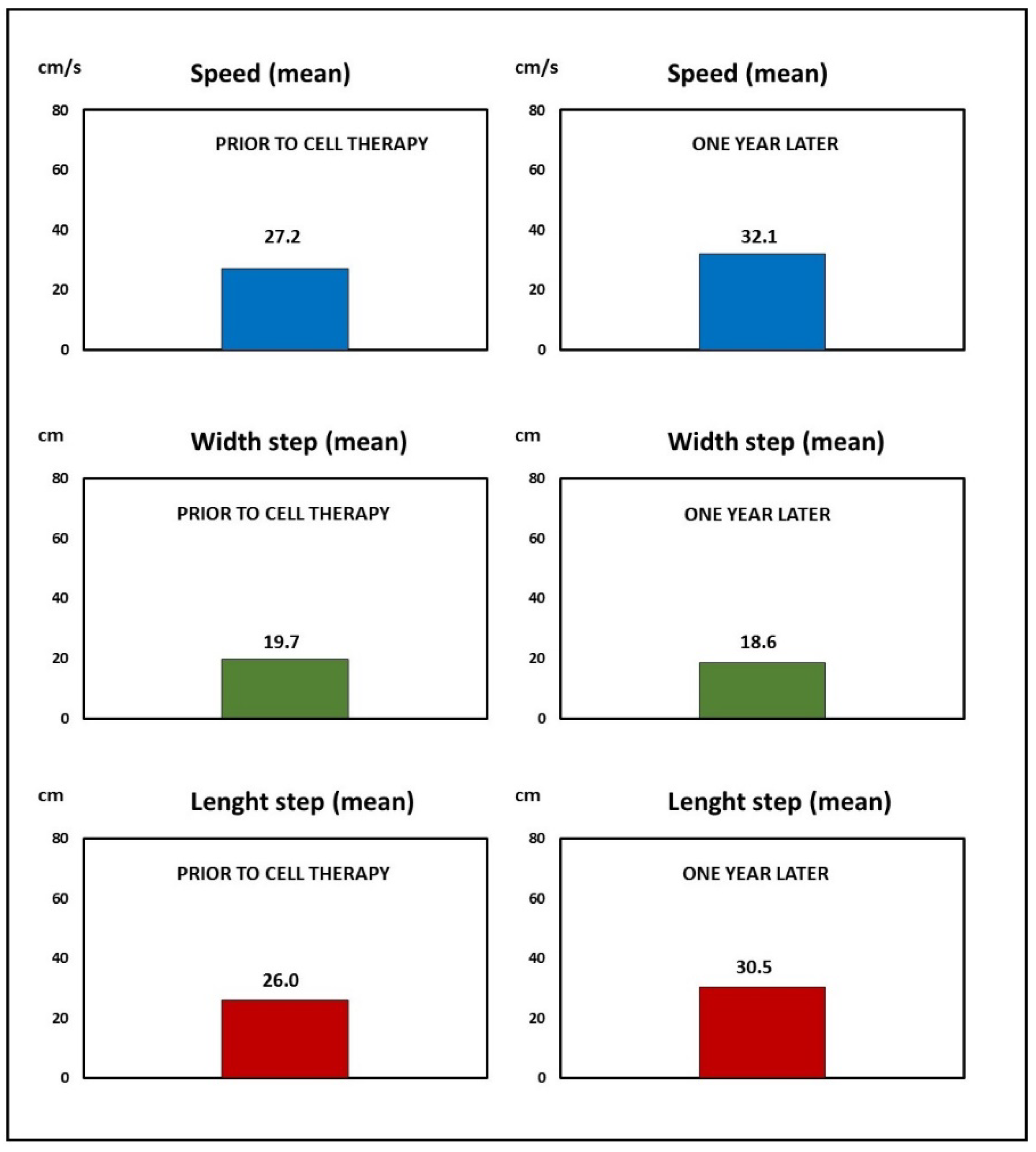
3.1. Case 1
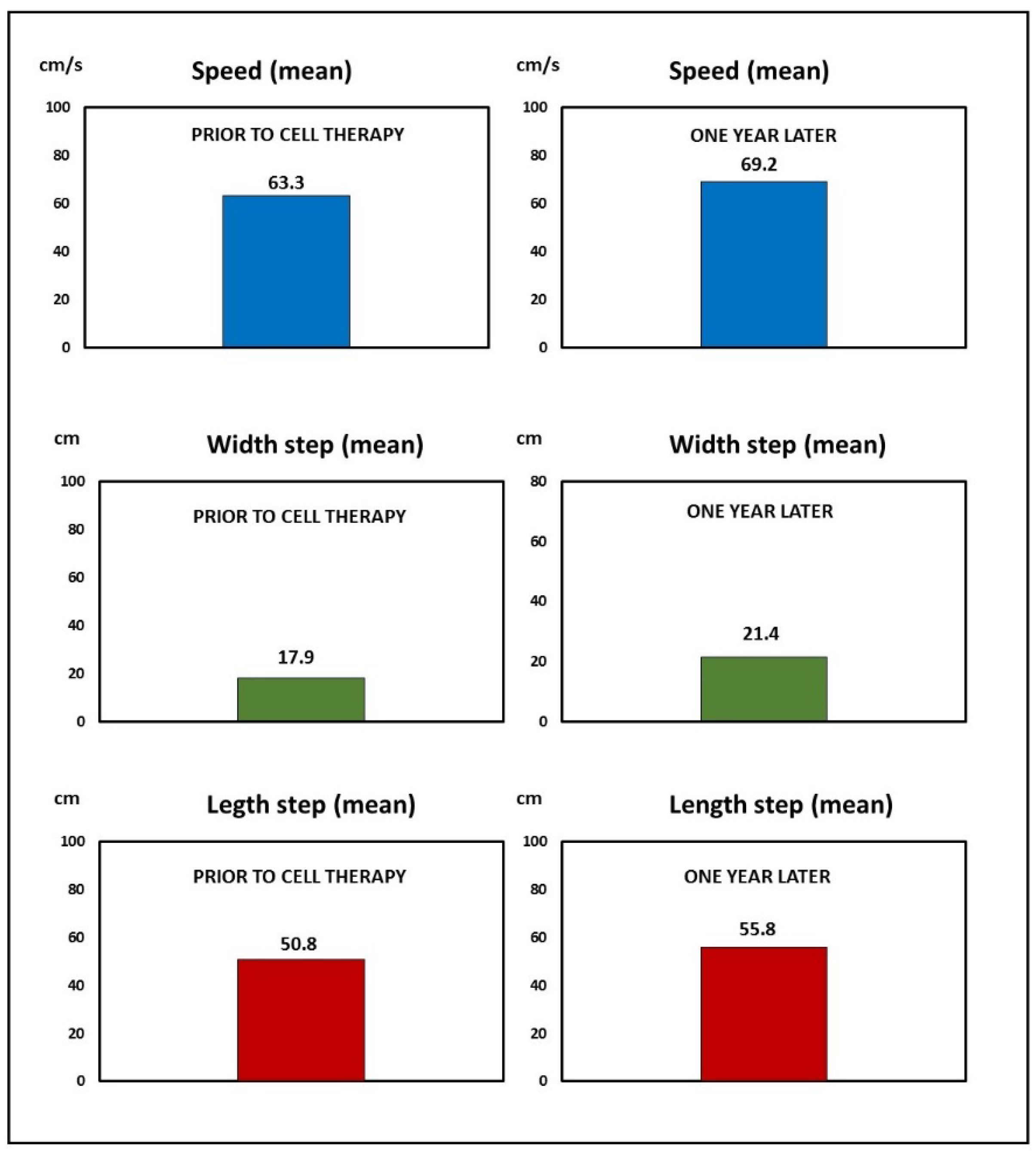
3.2. Case 2
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Furlan, J.C.; Sakakibara, B.M.; Miller, W.C.; Krassioukov, A.V. Global incidence and prevalence of traumatic spinal cord injury. Can. J. Neurol. Sci. 2013, 40, 456–464. [Google Scholar] [CrossRef]
- National Spinal Cord Injury Statistical Center. Traumatic Spinal Cord Injury Facts and Figures at a Glance; University of Alabama at Birmingham: Birmingham, AL, USA, 2022. [Google Scholar]
- Rowland, J.W.; Hawryluk, G.W.; Kwon, B.; Fehlings, M.G. Current status of acute spinal cord injury pathophysiology and emerging therapies: Promise on the horizon. Neurosurg. Focus 2008, 25, E2. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Tang, Y.; Vogel, L.C.; Devivo, M.J. Causes of spinal cord injury. Top. Spinal Cord Inj. Rehabil. 2013, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Prokopienko, M.; Kunert, P.; Podgórska, A.; Marchel, A. Surgical treatment of intramedullary ependymomas. Neurol. Neurochir. Pol. 2017, 51, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Stillerman, C.B.; Chen, T.C.; Couldwell, W.T.; Zhang, W.; Weiss, M.H. Experience in the surgical management of 82 symptomatic herniated thoracic discs and review of the literature. J. Neurosurg. 1998, 88, 623–633. [Google Scholar] [CrossRef]
- Börm, W.; Bäzner, U.; König, R.W.; Kretschmer, T.; Antoniadis, G.; Kandenwein, J. Surgical treatment of thoracic disc herniations via tailored posterior approaches. Eur. Spine J. 2011, 20, 1684–1690. [Google Scholar] [CrossRef] [PubMed]
- Vaquero, J.; Zurita, M.; Rico, M.A.; Bonilla, C.; Aguayo, C.; Fernández, C.; Tapiador, N.; Sevilla, M.; Morejón, C.; Montilla, J.; et al. Repeated subarachnoid administrations of autologous mesenchymal stromal cells supported in autologous plasma improve quality of life in patients suffering incomplete spinal cord injury. Cytotherapy 2017, 19, 349–359. [Google Scholar] [CrossRef]
- Vaquero, J.; Zurita, M.; Rico, M.A.; Aguayo, C.; Bonilla, C.; Marin, E.; Tapiador, N.; Sevilla, M.; Vazquez, D.; Carballido, J.; et al. Intrathecal administration of autologous mesenchymal stromal cells for spinal cord injury: Safety and efficacy of the 100/3 guideline. Cytotherapy 2018, 20, 806–819. [Google Scholar] [CrossRef]
- Saini, R.; Pahwa, B.; Agrawal, D.; Singh, P.K.; Gujjar, H.; Mishra, S.; Jagdevan, A.; Misra, M.C. Efficacy and outcome of bone marrow derived stem cells transplanted via intramedullary route in acute complete spinal cord injury—A randomized placebo controlled trial. J. Clin. Neurosci. 2022, 100, 7–14. [Google Scholar] [CrossRef]
- Smirnov, V.A.; Radaev, S.M.; Morozova, Y.V.; Ryabov, S.I.; Yadgarov, M.Y.; Bazanovich, S.A.; Lvov, I.S.; Talypov, A.E.; Grin’, A.A. Systemic Administration of Allogeneic Cord Blood Mononuclear Cells in Adults with Severe Acute Contusion Spinal Cord Injury: Phase 1/2a Pilot Clinical Study-Safety and Primary Efficacy Evaluation. World Neurosurg. 2022, 161, e319–e338. [Google Scholar] [CrossRef]
- Tang, Q.R.; Xue, H.; Zhang, Q.; Guo, Y.; Xu, H.; Liu, Y.; Liu, J.M. Evaluation of the Clinical Efficacy of Stem Cell Transplantation in the Treatment of Spinal Cord Injury: A Systematic Review and Meta-Analysis. Cell Transplant. 2021, 30, 9636897211067804. [Google Scholar] [CrossRef] [PubMed]
- Larocca, T.F.; Macêdo, C.T.; Souza, B.; Andrade-Souza, Y.M.; Villarreal, C.F.; Matos, A.C.; Silva, D.N.; da Silva, K.N.; de Souza, C.; Paixão, D.; et al. Image-guided percutaneous intralesional administration of mesenchymal stromal cells in subjects with chronic complete spinal cord injury: A pilot study. Cytotherapy 2017, 19, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Tang, F.; Zhao, Y.; Han, G.; Yin, N.; Li, X.; Chen, B.; Han, S.; Jiang, X.; Yun, C.; et al. Significant Improvement of Acute Complete Spinal Cord Injury Patients Diagnosed by a Combined Criteria Implanted with NeuroRegen Scaffolds and Mesenchymal Stem Cells. Cell Transplant. 2018, 27, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Curtis, E.; Martin, J.R.; Gabel, B.; Sidhu, N.; Rzesiewicz, T.K.; Mandeville, R.; Van Gorp, S.; Leerink, M.; Tadokoro, T.; Marsala, S.; et al. A First-in-Human, Phase I Study of Neural Stem Cell Transplantation for Chronic Spinal Cord Injury. Cell Stem Cell 2018, 22, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Oraee-Yazdani, S.; Akhlaghpasand, M.; Golmohammadi, M.; Hafizi, M.; Zomorrod, M.S.; Kabir, N.M.; Oraee-Yazdani, M.; Ashrafi, F.; Zali, A.; Soleimani, M. Combining cell therapy with human autologous Schwann cell and bone marrow-derived mesenchymal stem cell in patients with subacute complete spinal cord injury: Safety considerations and possible outcomes. Stem Cell Res. Ther. 2021, 12, 445. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Pang, M.; Du, C.; Liu, Z.Y.; Chen, Z.H.; Wang, N.X.; Zhang, L.M.; Chen, Y.Y.; Mo, J.; Dong, J.W.; et al. Repeated subarachnoid administrations of allogeneic human umbilical cord mesenchymal stem cells for spinal cord injury: A phase 1/2 pilot study. Cytotherapy 2021, 23, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Vaquero, J.; Zurita, M.; Rico, M.A.; Bonilla, C.; Aguayo, C.; Montilla, J.; Bustamante, S.; Carballido, J.; Marin, E.; Martinez, F.; et al. An approach to personalized cell therapy in chronic complete paraplegia: The Puerta de Hierro phase I/II clinical trial. Cytotherapy 2016, 18, 1025–1036. [Google Scholar] [CrossRef]
- Woodforde, J.M.; Merskey, H. Some relationships between subjective measures of pain. J. Psychosom. Res. 1972, 16, 173–178. [Google Scholar] [CrossRef]
- Krogh, K.; Christensen, P.; Sabroe, S.; Laurberg, S. Neurogenic bowel dysfunction score. Spinal Cord. 2006, 44, 625–631. [Google Scholar] [CrossRef]
- Geffner, L.F.; Santacruz, P.; Izurieta, M.; Flor, L.; Maldonado, B.; Auad, A.H.; Montenegro, X.; Gonzalez, R.; Silva, F. Administration of autologous bone marrow stem cells into spinal cord injury patients via multiple routes is safe and improves their quality of life: Comprehensive case studies. Cell Transplant. 2008, 17, 1277–1293. [Google Scholar] [CrossRef]
- Kirshblum, S.C.; Burns, S.P.; Biering-Sorensen, F.; Donovan, W.; Graves, D.E.; Jha, A.; Johansen, M.; Jones, L.; Krassioukov, A.; Mulcahey, M.J.; et al. International standards for neurological classification of spinal cord injury (revised 2011). J. Spinal Cord Med. 2011, 34, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.L.; Wang, X.R.; Li, M.M.; Tao, Z.H.; Teng, W.W.; Saijilaf. Mesenchymal Stromal Cell Therapy in Spinal Cord Injury: Mechanisms and Prospects. Front. Cell. Neurosci. 2022, 16, 862673. [Google Scholar] [CrossRef] [PubMed]
- Tahmasebi, F.; Barati, S. Effects of mesenchymal stem cell transplantation on spinal cord injury patients. Cell Tissue Res. 2022. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- de Araújo, L.T.; Macêdo, C.T.; Damasceno, P.; das Neves, Í.; de Lima, C.S.; Santos, G.C.; de Santana, T.A.; Sampaio, G.; Silva, D.N.; Villarreal, C.F.; et al. Clinical Trials Using Mesenchymal Stem Cells for Spinal Cord Injury: Challenges in Generating Evidence. Cells 2022, 11, 1019. [Google Scholar] [CrossRef] [PubMed]
- Tabakow, P.; Jarmundowicz, W.; Czapiga, B.; Fortuna, W.; Miedzybrodzki, R.; Czyz, M.; Huber, J.; Szarek, D.; Okurowski, S.; Szewczyk, P.; et al. Transplantation of autologous olfactory ensheathing cells in complete human spinal cord injury. Cell Transplant. 2013, 22, 1591–1612. [Google Scholar] [CrossRef] [PubMed]
- Mackay-Sim, A.; Féron, F.; Cochrane, J.; Bassingthwaighte, L.; Bayliss, C.; Davies, W.; Fronek, P.; Gray, C.; Kerr, G.; Licina, P.; et al. Autologous olfactory ensheathing cell transplantation in human paraplegia: A 3-year clinical trial. Brain 2008, 131, 2376–2386. [Google Scholar] [CrossRef]
- Vaquero, J.; Zurita, M.; Rico, M.A.; Aguayo, C.; Fernández, C.; Gutiérrez, R.; Rodríguez-Boto, G.; Saab, A.; Hassan, R.; Ortega, C. Intrathecal administration of autologous bone marrow stromal cells improves neuropathic pain in patients with spinal cord injury. Neurosci. Lett. 2018, 670, 14–18. [Google Scholar] [CrossRef]
- Guadalajara Labajo, H.; León Arellano, M.; Vaquero Crespo, J.; Valverde Núñez, I.; García-Olmo, D. Objective demonstration of improvement of neurogenic bowel dysfunction in a case of spinal cord injury following stem cell therapy. J. Surg. Case Rep. 2018, 2018, rjy300. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CASE 1 | ||
|---|---|---|
| Right gastrocnemius medial | Previous | After cell therapy |
| Latency (ms) | 93.9 | 34.8 |
| Amplitude (mV) | 0.1 | 0.5 |
| Right abductor hallucis | Previous | After cell therapy |
| Latency (ms) | 101.4 | 35.7 |
| Amplitude (mV) | 0.5 | 2.1 |
| Right abductor hallucis | Previous | After cell therapy |
| Latency (ms) | 24.3 | 21.0 |
| Amplitude (mV) | 0.8 | 1.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zurita, M.; Bonilla, C.; Aguayo, C.; Fernández-Mateos, C.; Martínez, P.; De La Calle, S.; Repollés, N.; Moñivas, E. Intrathecal Cell Therapy with Autologous Bone Marrow Stromal Cells as a New Tool for Neurologic Sequels after Spinal Cord Surgery: A Report of Two Cases. Reports 2022, 5, 43. https://doi.org/10.3390/reports5040043
Zurita M, Bonilla C, Aguayo C, Fernández-Mateos C, Martínez P, De La Calle S, Repollés N, Moñivas E. Intrathecal Cell Therapy with Autologous Bone Marrow Stromal Cells as a New Tool for Neurologic Sequels after Spinal Cord Surgery: A Report of Two Cases. Reports. 2022; 5(4):43. https://doi.org/10.3390/reports5040043
Chicago/Turabian StyleZurita, Mercedes, Celia Bonilla, Concepción Aguayo, Cecilia Fernández-Mateos, Paula Martínez, Silvia De La Calle, Nieves Repollés, and Esther Moñivas. 2022. "Intrathecal Cell Therapy with Autologous Bone Marrow Stromal Cells as a New Tool for Neurologic Sequels after Spinal Cord Surgery: A Report of Two Cases" Reports 5, no. 4: 43. https://doi.org/10.3390/reports5040043
APA StyleZurita, M., Bonilla, C., Aguayo, C., Fernández-Mateos, C., Martínez, P., De La Calle, S., Repollés, N., & Moñivas, E. (2022). Intrathecal Cell Therapy with Autologous Bone Marrow Stromal Cells as a New Tool for Neurologic Sequels after Spinal Cord Surgery: A Report of Two Cases. Reports, 5(4), 43. https://doi.org/10.3390/reports5040043