
Clinical Outcomes after Immunotherapies in Cancer Setting during COVID-19 Era: A Systematic Review and Meta-Regression





Abstract
:1. Introduction
2. Methodology
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Endpoints
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with Cancer Appear More Vulnerable to SARS-CoV-2: A Multicenter Study during the COVID-19 Outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Kalisz, K.R.; Ramaiya, N.H.; Laukamp, K.R.; Gupta, A. Immune Checkpoint Inhibitor Therapy–related Pneumonitis: Patterns and Management. RadioGraphics 2019, 39, 1923–1937. [Google Scholar] [CrossRef] [PubMed]
- Bersanelli, M. Controversies about COVID-19 and anticancer treatment with immune checkpoint inhibitors. Immunotherapy 2020, 12, 269–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, L.Y.; Cazier, J.B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Szabados, B.; Abu-Ghanem, Y.; Grant, M.; Choy, J.; Bex, A.; Powles, T. Clinical Characteristics and Outcome for Four SARS-CoV-2-infected Cancer Patients Treated with Immune Checkpoint Inhibitors. Eur. Urol. 2020, 78, 276–280. [Google Scholar] [CrossRef]
- Bersanelli, M.; Scala, S.; Affanni, P.; Veronesi, L.; Colucci, M.E.; Banna, G.L.; Cortellini, A.; Liotta, F. Immunological insights on influenza infection and vaccination during immune checkpoint blockade in cancer patients. Immunotherapy 2020, 12, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.; Lee, S.Y. Clinical Characteristics and Treatment of Immune-Related Adverse Events of Immune Checkpoint Inhibitors. Immune Netw. 2020, 20, e9. [Google Scholar] [CrossRef]
- Wang, D.Y.; Salem, J.E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal Toxic Effects Associated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.Q.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef]
- Chen, C.; Zhang, X.R.; Ju, Z.Y.; He, W.F. Advances in the research of mechanism and related immunotherapy on the cytokine storm induced by coronavirus disease 2019. Zhonghua Shao Shang Za Zhi 2020, 36, 471–475. [Google Scholar]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Artigas, C.; Lemort, M.; Mestrez, F.; Gil, T.; Flamen, P. COVID-19 Pneumonia Mimicking Immunotherapy-Induced Pneumonitis on 18F-FDG PET/CT in a Patient Under Treatment with Nivolumab. Clin. Nucl. Med. 2020, 45, e381–e382. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 March 2022).
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; Ernstoff, M.S.; Gardner, J.M.; Ginex, P.; et al. Management of Immune-Related Adverse Events in Patients Treated with Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef] [PubMed]
- Robilotti, E.V.; Babady, N.E.; Mead, P.A.; Rolling, T.; Perez-Johnston, R.; Bernardes, M.; Bogler, Y.; Caldararo, M.; Figueroa, C.J.; Glickman, M.S.; et al. Determinants of COVID-19 disease severity in patients with cancer. Nat. Med. 2020, 26, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Kim, Y.H.; Kanai, O.; Yoshida, H.; Mio, T.; Hirai, T. Emerging concerns of infectious diseases in lung cancer patients receiving immune checkpoint inhibitor therapy. Respir. Med. 2019, 146, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo, M.; Romero, F.A.; Argüello, E.; Kyi, C.; Postow, M.A.; Redelman-Sidi, G. The Spectrum of Serious Infections Among Patients Receiving Immune Checkpoint Blockade for the Treatment of Melanoma. Clin. Infect. Dis. 2016, 63, 1490–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, J.; Rizvi, H.; Egger, J.V.; Preeshagul, I.R.; Wolchok, J.D.; Hellmann, M.D. Impact of PD-1 Blockade on Severity of COVID-19 in Patients with Lung Cancers. Cancer Discov. 2020, 10, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Matrajt, L.; Leung, T. Evaluating the effectiveness of social distancing interventions to delay or flatten the epidemic curve of coronavirus disease. Emerg. Infect. Dis. 2020, 26, 1740. [Google Scholar] [CrossRef]
- Veronese, N.; Demurtas, J.; Yang, L.; Tonelli, R.; Barbagallo, M.; Lopalco, P.; Lagolio, E.; Celotto, S.; Pizzol, D.; Zou, L.; et al. Use of Corticosteroids in Coronavirus Disease 2019 Pneumonia: A Systematic Review of the Literature. Front. Med. 2020, 7, 170. [Google Scholar] [CrossRef]
- Amin, R.; Thomas, A.S.; Khurana, S.; Panneerselvam, K.; Zou, F.; Ma, W.; Chari, S.T.; Wang, Y. Management of Immune-Related Colitis During the COVID-19 Pandemic. Inflamm. Bowel Dis. 2020, 26, e110–e111. [Google Scholar] [CrossRef]
- Rotz, S.J.; Leino, D.; Szabo, S.; Mangino, J.L.; Turpin, B.K.; Pressey, J.G. Severe cytokine release syndrome in a patient receiving PD-1-directed therapy. Pediatr. Blood Cancer 2017, 64, e26642. [Google Scholar] [CrossRef] [PubMed]
- Bersanelli, M.; Giannarelli, D.; Castrignanò, P.; Fornarini, G.; Panni, S.; Mazzoni, F.; Tiseo, M.; Rossetti, S.; Gambale, E.; Rossi, E.; et al. Influenza vaccine indication during therapy with immune checkpoint inhibitors: A transversal challenge. The INVIDIa Study. Immunotherapy 2018, 10, 1229–1239. [Google Scholar] [CrossRef] [PubMed]
- Souza, I.L.; Fernandes, Í.; Taranto, P.; Buzaid, A.C.; Schvartsman, G. Immune-related pneumonitis with nivolumab and ipilimumab during the coronavirus disease 2019 (COVID-19) pandemic. Eur. J. Cancer 2020, 135, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Wang, H.; Shen, H.; Li, Z.; Geng, J.; Han, H.; Cai, J.; Li, X.; Kang, W.; Weng, D.; et al. The clinical pathology of severe acute respiratory syndrome (SARS): A report from China. J. Pathol. A J. Pathol. Soc. Great Br. Irel. 2003, 200, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Stroud, C.R.; Hegde, A.; Cherry, C.; Naqash, A.R.; Sharma, N.; Addepalli, S.; Cherukuri, S.; Parent, T.; Hardin, J.; Walker, P. Tocilizumab for the management of immune mediated adverse events secondary to PD-1 blockade. J. Oncol. Pharm. Pract. 2019, 25, 551–557. [Google Scholar] [CrossRef]
- Horisberger, A.; La Rosa, S.; Zurcher, J.P.; Zimmermann, S.; Spertini, F.; Coukos, G.; Obeid, M. A severe case of refractory esophageal stenosis induced by nivolumab and responding to tocilizumab therapy. J. Immunother. Cancer 2018, 6, 156. [Google Scholar] [CrossRef] [PubMed]
- Hadadi, A.; Mortezazadeh, M.; Kolahdouzan, K.; Alavian, G. Does recombinant human erythropoietin administration in critically ill COVID-19 patients have miraculous therapeutic effects? J. Med. Virol. 2020, 92, 915–918. [Google Scholar] [CrossRef] [Green Version]
- Sereno, M.; Gutiérrez-Gutiérrez, G.; Sandoval, C.; Falagan, S.; Jimenez-Gordo, A.M.; Merino, M.; López-Menchaca, R.; Martínez-Martin, P.; Roa, S.; Casado, E.; et al. A favorable outcome of pneumonia COVID 19 in an advanced lung cancer patient with severe neutropenia: Is immunosuppression a risk factor for SARS-CoV2 infection? Lung Cancer 2020, 145, 213–215. [Google Scholar] [CrossRef]
- Vivarelli, S.; Falzone, L.; Grillo, C.M.; Scandurra, G.; Torino, F.; Libra, M. Cancer Management during COVID-19 Pandemic: Is Immune Checkpoint Inhibitors-Based Immunotherapy Harmful or Beneficial? Cancers 2020, 12, 2237. [Google Scholar] [CrossRef]
- Wu, Q.; Chu, Q.; Zhang, H.; Yang, B.; He, X.; Zhong, Y.; Yuan, X.; Chua, M.L.; Xie, C. Clinical outcomes of coronavirus disease 2019 (COVID-19) in cancer patients with prior exposure to immune checkpoint inhibitors. Cancer Commun. 2020, 40, 374–379. [Google Scholar] [CrossRef]
- Goldstein, D.A.; Ratain, M.J.; Saltz, L.B. Weight-Based Dosing of Pembrolizumab Every 6 Weeks in the Time of COVID-19. JAMA Oncol. 2020, 6, 1694–1695. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.; Goel, S.; Kabarriti, R.; Cole, D.; Goldfinger, M.; Acuna-Villaorduna, A.; Pradhan, K.; Thota, R.; Reissman, S.; Sparano, J.A.; et al. Case Fatality Rate of Cancer Patients with COVID-19 in a New York Hospital System. Cancer Discov. 2020, 10, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Rizvi, H.; Preeshagul, I.R.; Egger, J.V.; Hoyos, D.; Bandlamudi, C.; McCarthy, C.G.; Falcon, C.J.; Schoenfeld, A.J.; Arbour, K.C.; et al. COVID-19 in patients with lung cancer. Ann. Oncol. 2020, 31, 1386–1396. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Author | Year | Institution | Country | Study Type | N | Mean Age | Male | Smoking History | HTN | DM | Dyslipidemia | CKD | Respiratory Conditions | CVA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yu | 2020 | Zhongnan Hospital of Wuhan University | China | Case series | 2 | NA | 2 | NA | NA | NA | NA | NA | NA | NA |
| Figuero-Perez | 2020 | University of Salamanca | Spain | Case report | 1 | 76 | 1 | NA | NA | NA | NA | NA | 1 | NA |
| Damato | 2020 | Oncologico e Tecnologie Avanzate, Azienda USL—IRCCS Reggio Emilia | Italy | Case series | 3 | 60.3 | 2 | 2 | NA | NA | NA | NA | NA | NA |
| Schmidle | 2020 | Technical University of Munich | Germany | Case report | 1 | 47 | 0 | NA | NA | NA | NA | NA | NA | NA |
| Kalinsky | 2020 | Columbia University Irving Medical Center | USA | Case report | 1 | 32 | 0 | 0 | NA | NA | NA | NA | NA | NA |
| Shaverdian | 2020 | Memorial Sloan Kettering Cancer Center | USA | Case series | 1 | 73 | 0 | NA | NA | NA | NA | NA | NA | NA |
| Ning | 2020 | The University of Texas MD Anderson Cancer Center | USA | Case series | 2 | 61.5 | 1 | NA | NA | NA | NA | NA | NA | NA |
| Rolfo | 2020 | Marlene and Stewart Comprehensive Cancer Center | USA | Case series | 2 | 65 | 1 | 2 | NA | NA | NA | NA | NA | NA |
| Spoto | 2020 | University Campus Bio-Medico of Rome | Italy | Case report | 1 | 55 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Di Giacomo | 2020 | University Hospital of Siena | Italy | Case series | 2 | 62.5 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Wei | 2020 | Huazhong University of Science and Technology | China | Case series | 1 | 30 | 1 | NA | NA | NA | NA | NA | NA | NA |
| OKelly | 2020 | Mater Misericordiae University Hospital | Ireland | Case report | 1 | 22 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Souza | 2020 | Hospital Israelita Albert Einstein | Brazil | Case series | 2 | 78.5 | 1 | NA | NA | NA | NA | NA | NA | NA |
| Di Noia | 2020 | Cliniche Humanitas Gavazzeni | Italy | Case report | 1 | 53 | 1 | NA | NA | NA | NA | NA | NA | NA |
| Guerini | 2020 | Università degli Studi di Brescia | Italy | Case report | 1 | 75 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 |
| da Costa | 2020 | Brazil | Case report | 1 | 66 | 1 | 1 | NA | NA | NA | NA | NA | NA | |
| Yekedüz | 2020 | Turkey | Case report | 1 | 75 | 1 | NA | 1 | 1 | 0 | 0 | 1 | 1 | |
| Szabados | 2020 | UK | Case series | 4 | 64.5 | 4 | 2 | 4 | 1 | 0 | 0 | 0 | 0 | |
| Bersanelli | 2020 | 82 Italian centers | Italy | Case series | 3 | 71.7 | 3 | 3 | 2 | NA | NA | NA | 2 | 1 |
| Grover | 2020 | USA | Case report | 1 | 54 | 0 | NA | NA | NA | NA | NA | NA | NA | |
| Wu | 2020 | Zhongnan Hospital of Wuhan University and the Tongji Hospital of Huazhong University of Science and Technology | China | Case series | 11 | 56 | 8 | 5 | NA | NA | NA | NA | NA | NA |
| Smith | 2021 | Baylor College of Medicine | USA | Case report | 1 | 23 | 0 | NA | NA | NA | NA | NA | NA | NA |
| Outcome | No. of Studies | Estimate | 95% CI | Heterogeneity: I2, p-Value | Egger Test (p-Value) |
|---|---|---|---|---|---|
| Steroid use | 14 | 51.36% | 34.99–67.44 | 0%, p = 0.757 | p = 0.6754 |
| Antiviral use | 10 | 62.10% | 41.04–79.41 | 0%, p = 0.5467 | p = 0.1625 |
| Antibiotics use | 13 | 57.12% | 37.03–75.10 | 0%, p = 0.9824 | p = 0.0017 |
| Convalescent plasma use | 8 | 26.48% | 10.59–52.28 | 0%, p = 0.9470 | NA |
| Prophylactic anticoagulant use | 10 | 41.90% | 21.35–65.72 | 0%, p = 0.7297 | p = 0.6215 |
| Antibody treatment | 6 | 0% | NA | NA | NA |
| Readmission to hospital | 5 | 0% | NA | NA | NA |
| ER visit | 9 | 40.75% | 19.16–65.95 | 0%, p = 0.8221 | NA |
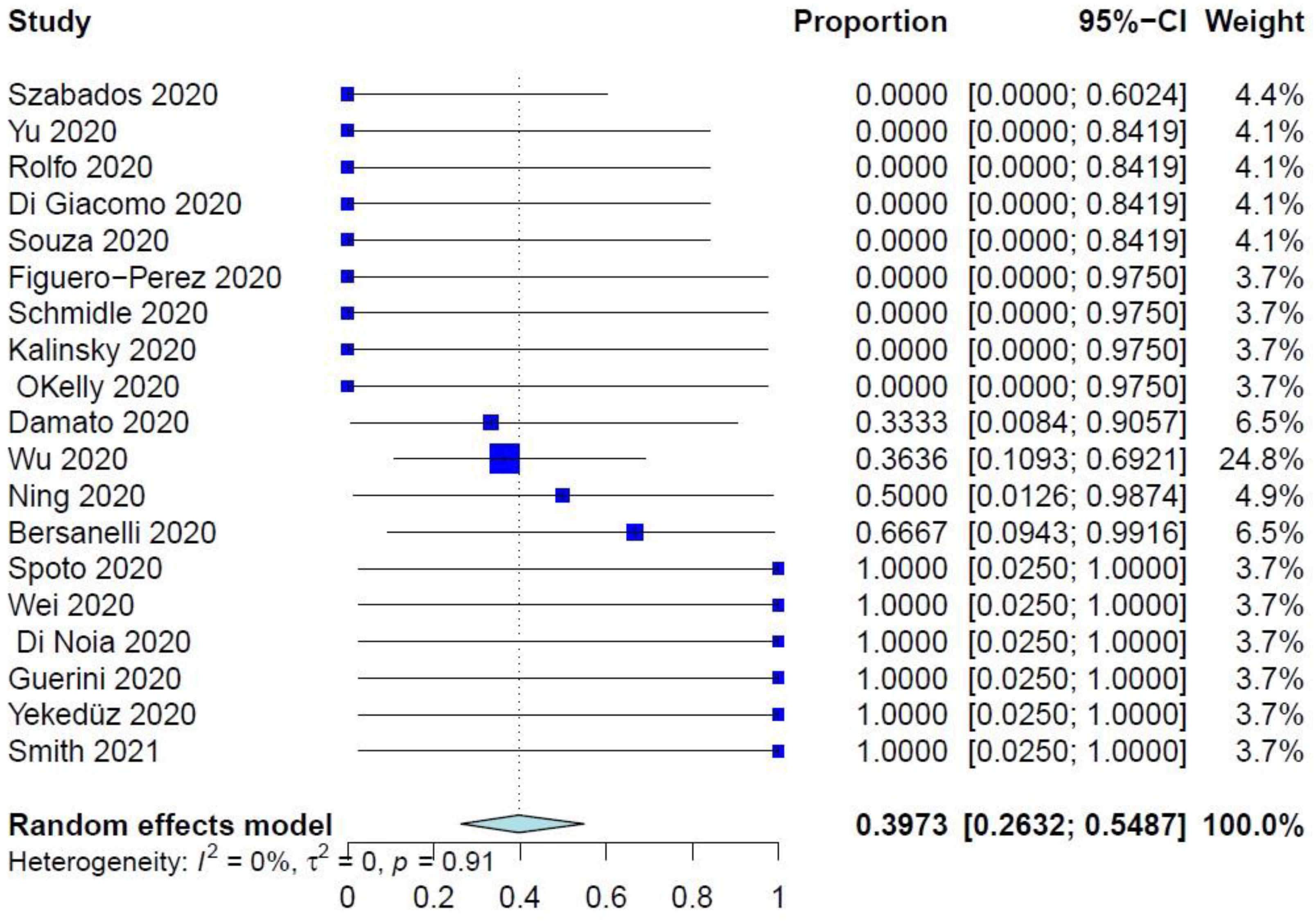
| COVID-19–related mortality | 19 | 39.73 | 26.32–54.87 | 0%, p = 0.9077 | p = 0.7214 |
| Airway problem | 9 | 27.28% | 11.79–51.30 | 0%, p = 0.8272 | NA |
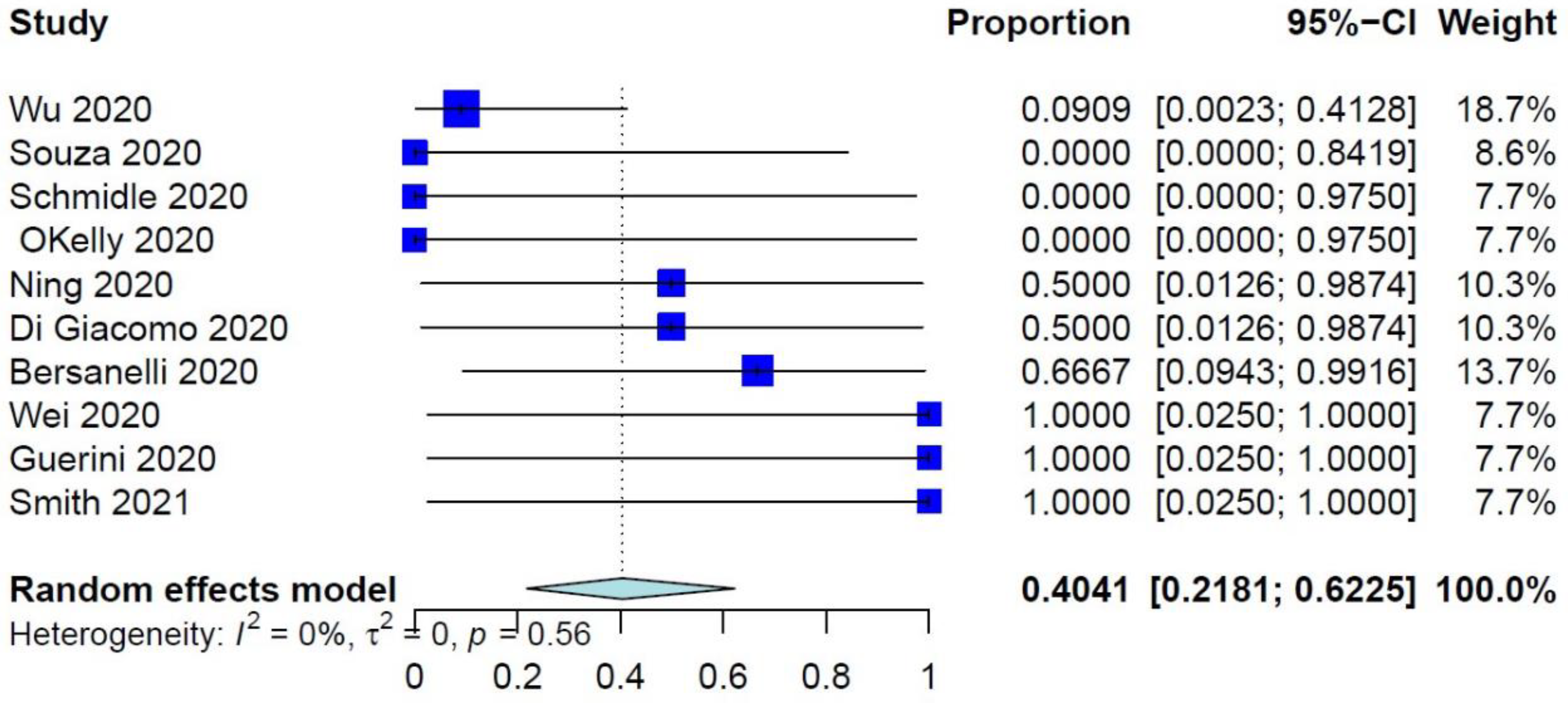
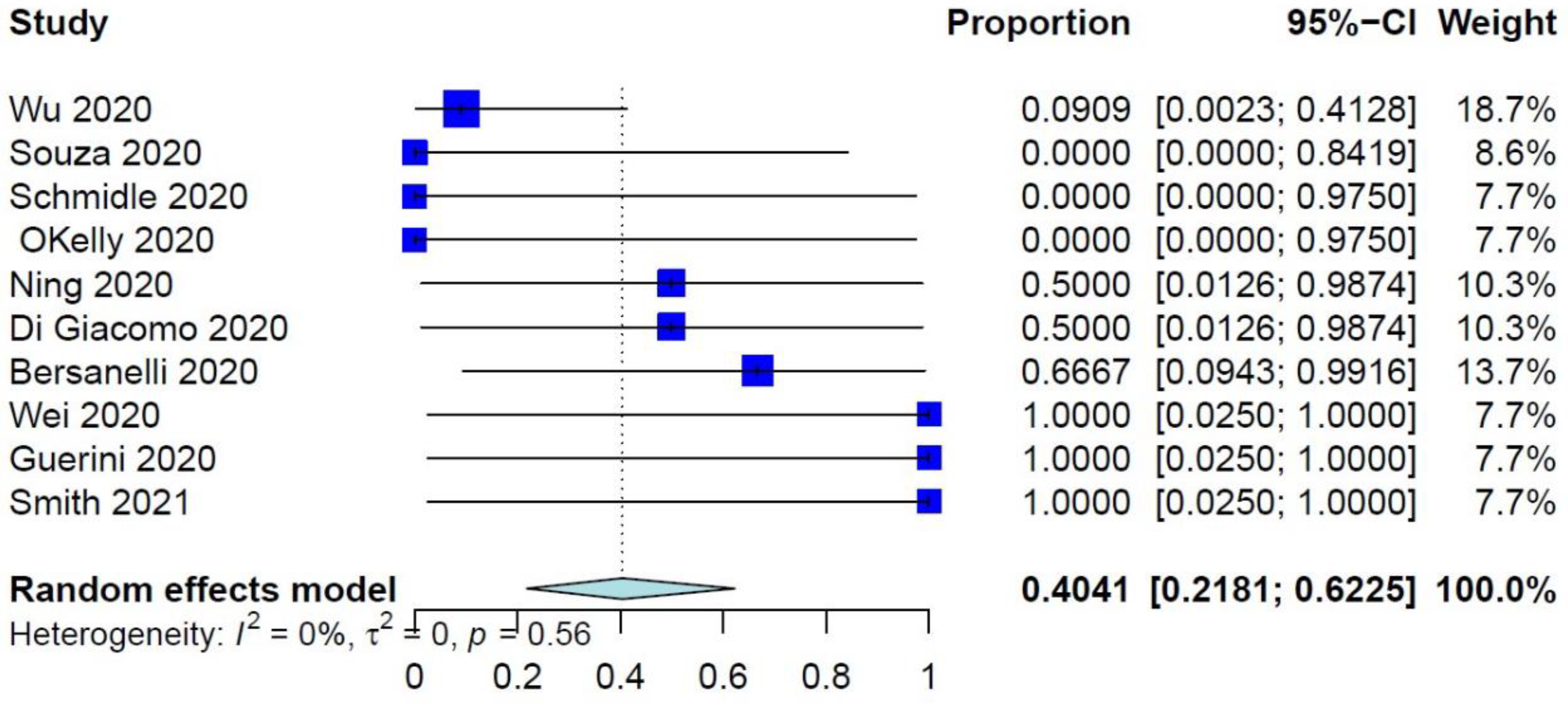
| Pulmonary complication | 10 | 40.41% | 21.81–62.25 | 0%, p = 0.5596 | |
| Need for ventilator | 11 | 34.92% | 17.34–57.86 | 0%, p = 0.7252 | p = 0.0030 |
| Need for tracheostomy | 9 | 0% | NA | NA | NA |
| Thrombo-embolic event | 8 | 0% | NA | NA | NA |
| Opportunistic infection | 9 | 29.45% | 12.84–54.18 | 0%, p = 0.8681 | NA |
| Variable | No. of Studies | Beta ± SE | p-Value |
|---|---|---|---|
| Mean age | 18 | −0.0073 ± 0.0211 | 0.7300 |
| Male sex | 19 | 0.0034 ± 0.0089 | 0.7009 |
| Respiratory disease | 7 | 0.0220 ± 0.0128 | 0.0861 |
| History of smoking | 10 | 0.0078 ± 0.0114 | 0.4917 |
| Diabetes | 5 | 0.0166 ± 0.0189 | 0.3813 |
| Hypertension | 6 | 0.0131 ± 0.0144 | 0.3634 |
| Dyslipidemia | 5 | −0.6263 ± 0.7086 | 0.3768 |
| Chronic kidney disease | 5 | −0.6263 ± 0.7086 | 0.3768 |
| Cerebrovascular accident | 6 | 0.0236 ± 0.0178 | 0.1858 |
| Previous cancer treatment | 8 | 0.0043 ± 0.0121 | 0.7194 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamal, M.; Baudo, M.; Joseph, J.; Geng, Y.; Qdaisat, A. Clinical Outcomes after Immunotherapies in Cancer Setting during COVID-19 Era: A Systematic Review and Meta-Regression. Reports 2022, 5, 31. https://doi.org/10.3390/reports5030031
Kamal M, Baudo M, Joseph J, Geng Y, Qdaisat A. Clinical Outcomes after Immunotherapies in Cancer Setting during COVID-19 Era: A Systematic Review and Meta-Regression. Reports. 2022; 5(3):31. https://doi.org/10.3390/reports5030031
Chicago/Turabian StyleKamal, Mona, Massimo Baudo, Jacinth Joseph, Yimin Geng, and Aiham Qdaisat. 2022. "Clinical Outcomes after Immunotherapies in Cancer Setting during COVID-19 Era: A Systematic Review and Meta-Regression" Reports 5, no. 3: 31. https://doi.org/10.3390/reports5030031
APA StyleKamal, M., Baudo, M., Joseph, J., Geng, Y., & Qdaisat, A. (2022). Clinical Outcomes after Immunotherapies in Cancer Setting during COVID-19 Era: A Systematic Review and Meta-Regression. Reports, 5(3), 31. https://doi.org/10.3390/reports5030031