
A Unique Case of the Transformation of a Hepatic Leiomyoma into Leiomyosarcoma with Pancreatic Metastases: Review of the Literature with Case Presentation

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Material and Methods
3. Results
3.1. Case Presentation
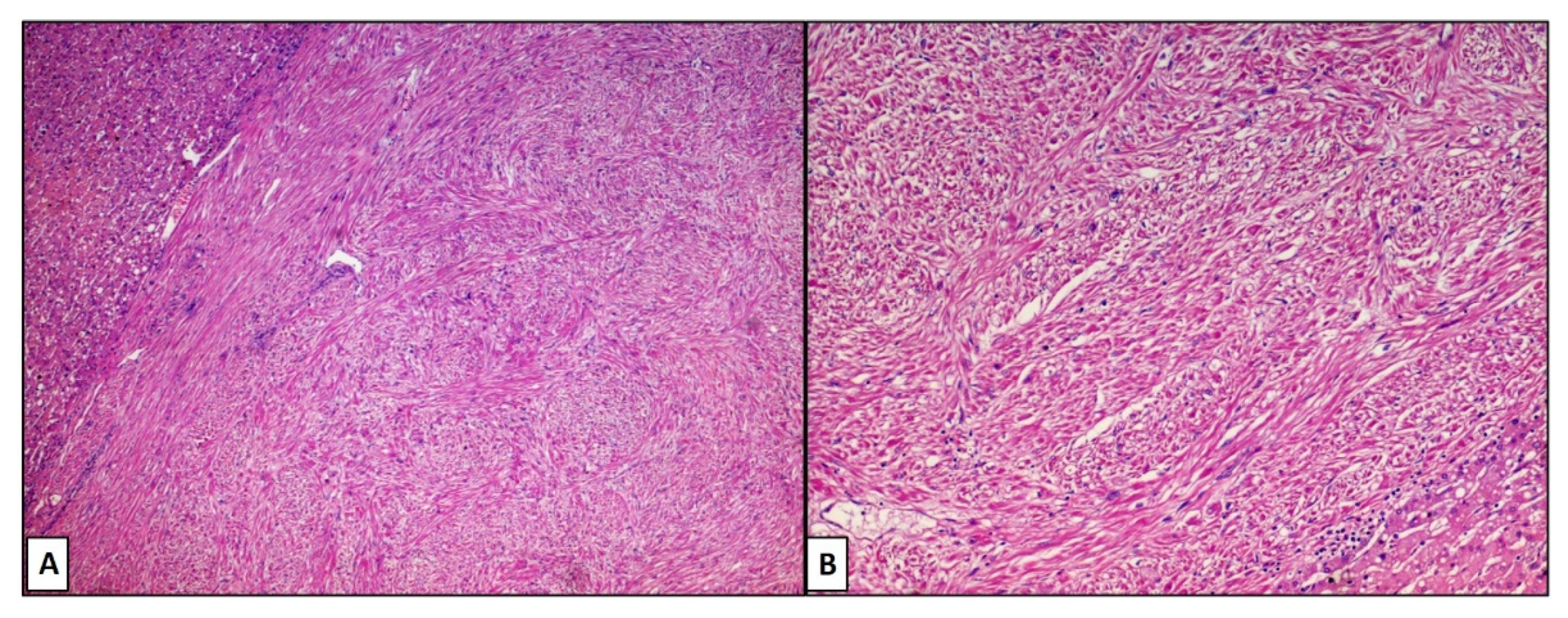
3.2. Histological Features
3.3. Review of Literature
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Digestive System Tumours: WHO Classification of Tumours; World Health Organization (WHO): Geneva, Switzerland, 2019; Volume 1.
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef]
- Demel, R. Ein operierter Fall von Leber-Myom. Virchows Arch. Pathol. Anat. Physiol. Klin. Med. 1926, 261, 881–884. [Google Scholar] [CrossRef]
- Beaird, J.B.; Scofield, G.F. Budd-Chiari syndrome. Hepatic vein occlusion due to leiomyosarcoma primary in the inferior vena cava. Arch. Intern. Med. 1962, 110, 435–441. [Google Scholar] [CrossRef]
- Rios-Dalenz, J.L. Leiomyoma of the Liver. Arch Pathol. 1965, 79, 54–56. [Google Scholar]
- Masur, H.; Sussman, E.B.; Molander, D.W. Primary hepatic leiomyosarcoma: A report of two cases. Gastroenterology 1975, 69, 994–997. [Google Scholar] [CrossRef]
- Bloustein, P.A. Hepatic leiomyosarcoma: Ultrastructural study and review of the differential diagnosis. Hum. Pathol. 1978, 9, 713–715. [Google Scholar] [CrossRef]
- Maki, H.S.; Hubert, B.C.; Sajjad, S.M.; Kirchner, J.P.; Kuehner, M.E. Primary hepatic leiomyosarcoma. Arch. Surg. 1987, 122, 1193–1196. [Google Scholar] [CrossRef]
- Griffin, A.S.; Sterchi, J.M. Primary leiomyosarcoma of the inferior vena cava: A case report and review of the literature. J. Surg. Oncol. 1987, 34, 53–60. [Google Scholar] [CrossRef]
- Shurbaji, M.S.; Olson, J.L.; Kuhajda, F.P. Thorotrast-associated hepatic leiomyosarcoma and cholangiocarcinoma in a single patient. Hum. Pathol. 1987, 18, 524–526. [Google Scholar] [CrossRef]
- Kinoshita, A.; Sakon, M.; Monden, M.; Gotoh, M.; Kobayashi, K.; Okuda, H.; Kuroda, C.; Sakurai, M.; Okamura, J.; Mori, T. Triple synchronous malignant tumors. Hepatic leiomyosarcoma, splenic hemangiosarcoma and sigmoid colon cancer. Case report. Acta Chir. Scand. 1988, 154, 477–479. [Google Scholar]
- Rummeny, E.; Weissleder, R.; Stark, D.D.; Saini, S.; Compton, C.C.; Bennett, W.; Hahn, P.F.; Wittenberg, J.; Malt, R.A.; Ferrucci, J.T. Primary liver tumors: Diagnosis by MR imaging. AJR Am. J. Roentgenol. 1989, 152, 63–72. [Google Scholar] [CrossRef]
- Herzberg, A.J.; MacDonald, J.A.; Tucker, J.A.; Humphrey, P.A.; Meyers, W.C. Primary leiomyoma of the liver. Am. J. Gastroenterol. 1990, 85, 1642–1645. [Google Scholar]
- Little, J.M.; Kenny, J.; Hollands, M.J. Hepatic incidentaloma: A modern problem. World J. Surg. 1990, 14, 448–451. [Google Scholar] [CrossRef]
- Lee, P.K.; Teixeira, O.H.; Simons, J.A.; Goodman, R.L.; Brais, M.P.; Barber, G.G.; Dunlap, H.J.; Walley, V.M. Atypical hepatic vein leiomyoma extending into the right atrium: An unusual cause of the Budd-Chiari syndrome. Can. J. Cardiol. 1990, 6, 107–110. [Google Scholar]
- Spagliardi, E.; Longo, A.; Blanco, G.F.; Ruggeri, C.; Buscaglia, M.; Torelli, P. Rare primary hepatic neoplasms. Our experience in 2 cases: A primary lymphoma and a leiomyosarcoma of the liver. Minerva Chir. 1990, 45, 95–102. [Google Scholar]
- Sundaresan, M.; Kelly, S.B.; Benjamin, I.S.; Akosa, A.B. Primary hepatic vascular leiomyosarcoma of probable portal vein origin. J. Clin. Pathol. 1990, 43, 1036. [Google Scholar] [CrossRef]
- Bartoli, S.; Alò, P.; Leporelli, P.; Puce, E.; Di Tondo, U.; Thau, A. Primary hepatic leiomyoma. Minerva Chir. 1991, 46, 777–779. [Google Scholar]
- Ishii, H.; Nakayama, T.; Hiyama, Y. Primary hepatic leiomyosarcoma: The investigation of domestic and foreign 34 cases. Nihon Shokakibyo Gakkai Zasshi 1991, 88, 1256–1263. [Google Scholar]
- Korbi, S.; Aouini, M.T.; Remadi, S.; el Ajmi, S.; Mokni, M.; Ben Ayed, F.; Gannouni, A. Primary hepatic leiomyosarcoma. A case report with immunohistochemical studies and review of the literature. J. Submicrosc. Cytol. Pathol. 1991, 23, 643–647. [Google Scholar]
- Reinertson, T.E.; Fortune, J.B.; Peters, J.C.; Pagnotta, I.; Balint, J.A. Primary leiomyoma of the liver. A case report and review of the literature. Dig. Dis. Sci. 1992, 37, 622–627. [Google Scholar] [CrossRef]
- Ross, J.S.; Del Rosario, A.; Bui, H.X.; Sonbati, H.; Solis, O. Primary hepatic leiomyosarcoma in a child with the acquired immunodeficiency syndrome. Hum. Pathol. 1992, 23, 69–72. [Google Scholar] [CrossRef]
- Baur, M.; Pötzi, R.; Lochs, H.; Neuhold, N.; Walgram, M.; Gangl, A. Primary leiomyosarcoma of the liver—A case report. Z. Gastroenterol. 1993, 31, 20–23. [Google Scholar]
- Saint-Paul, M.C.; Gugenheim, J.; Hofman, P.; Arpurt, J.P.; Fabiani, P.; Michiels, J.F.; Fujita, N.; Goubeaux, B.; Loubière, R.; Delmont, J.; et al. Leiomyosarcoma of the liver: A case treated by transplantation. Gastroenterol. Clin. Biol. 1993, 17, 218–222. [Google Scholar]
- Prévot, S.; Néris, J.; de Saint Maur, P.P. Detection of Epstein Barr virus in an hepatic leiomyomatous neoplasm in an adult human immunodeficiency virus 1-infected patient. Virchows Arch. 1994, 425, 321–325. [Google Scholar] [CrossRef]
- Hiyama, Y. Primary hepatic leiomyosarcoma and rhabdomyosarcoma. Ryoikibetsu Shokogun Shirizu 1995, 7, 463–466. [Google Scholar]
- Abdelli, N.; Thiefin, G.; Diebold, M.D.; Bouche, O.; Aucouturier, J.P.; Zeitoun, P. Primary leiomyosarcoma of the liver 37 years after successful treatment of hereditary retinoblastoma. Gastroenterol. Clin. Biol. 1996, 20, 502–505. [Google Scholar]
- Davidoff, A.M.; Hebra, A.; Clark, B.J.; Tomaszewski, J.E.; Montone, K.T.; Ruchelli, E.; Lau, H.T. Epstein-Barr virus-associated hepatic smooth muscle neoplasm in a cardiac transplant recipient. Transplantation 1996, 61, 515–517. [Google Scholar] [CrossRef] [PubMed]
- Yoon, G.S.; Kang, G.H.; Kim, O.J. Primary myxoid leiomyoma of the liver. Arch. Pathol. Lab. Med. 1998, 122, 1112–1115. [Google Scholar] [PubMed]
- Yanase, M.; Ikeda, H.; Ogata, I.; Ohno, A.; Moriya, A.; Miura, N.; Kimura, S.; Mori, M.; Oka, T.; Ohtomo, K.; et al. Primary smooth muscle tumor of the liver encasing hepatobiliary cystadenoma without mesenchymal stroma. Am. J. Surg. Pathol. 1999, 23, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Enoki, T.; Hayashi, D.; Inokuchi, T.; Okamura, K.; Takahashi, T.; Noshima, S.; Morita, N.; Esato, K. Combined right hepatic and retrohepatic caval resection with reconstruction using a polytetrafluoroethylene graft for primary leiomyosarcoma of the liver: Report of case. Surg. Today 1999, 29, 67–70. [Google Scholar] [CrossRef]
- Mesenas, S.J.; Ng, K.Y.; Raj, P.; Ho, J.M.; Ng, H.S. Primary leiomyoma of the liver. Singap. Med. J. 2000, 41, 129–131. [Google Scholar]
- Tsuji, M.; Takenaka, R.; Kashihara, T.; Hadama, T.; Terada, N.; Mori, H. Primary hepatic leiomyosarcoma in a patient with hepatitis C virus-related liver cirrhosis. Pathol. Int. 2000, 50, 41–47. [Google Scholar] [CrossRef]
- Belli, G.; Ciciliano, F.; Lannelli, A.; Marano, I. Hepatic resection for primary giant leiomyoma of the liver. HPB 2001, 3, 11–12. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Linares Torres, P.; Vivas Alegre, S.; Castañón López, C.; Domínguez Carbajo, A.B.; Honrado Franco, E.; Espinel Díez, J.; Jorquera Plaza, F.; Olcoz Goñi, J.L. Primary hepatic leiomyosarcoma in a patient with gastric non-Hodgkin lymphoma. Gastroenterol. Hepatol. 2002, 25, 452–454. [Google Scholar] [CrossRef]
- Fujita, H.; Kiriyama, M.; Kawamura, T.; Ii, T.; Takegawa, S.; Dohba, S.; Kojima, Y.; Yoshimura, M.; Kobayashi, A.; Ozaki, S.; et al. Primary hepatic leiomyosarcoma in a woman after renal transplantation: Report of a case. Surg. Today 2002, 32, 446–449. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, J.L.; Choi, W.H. A case of primary myxoid leiomyosarcoma of the liver. Korean J. Intern. Med. 2002, 17, 278–282. [Google Scholar] [CrossRef]
- Baek, I.; Kim, J.H.; Lee, M.S.; Baik, G.H.; Hahn, T.; Park, H.J.; Park, S.H.; Chang, W.K.; Kim, W.J.; Park, C.K. A case of primary leiomyosarcoma of the liver. Taehan Kan Hakhoe Chi 2002, 8, 481–485. [Google Scholar] [PubMed]
- Beuzen, F.; Roudie, J.; Moali, I.; Maitre, S.; Barthelemy, P.; Smadja, C. Primary leiomyoma of the liver: A rare benign tumor. Gastroenterol. Clin. Biol. 2004, 28, 1169–1172. [Google Scholar] [CrossRef]
- Maruta, K.; Sonoda, Y.; Saigo, R.; Yoshioka, T.; Fukunaga, H. A patient with von Recklinghausen’s disease associated with polymyositis, asymptomatic pheochromocytoma, and primary hepatic leiomyosarcoma. Nihon Ronen Igakkai Zasshi 2004, 41, 339–343. (In Japanese) [Google Scholar] [CrossRef][Green Version]
- Lee, H.L.; Sohn, J.H.; Kim, J.B.; Han, D.S.; Jeon, Y.C.; Hahm, J.S.; Lee, D.H.; Kee, C.S.; Park, Y.W. A case of primary hepatic leiomyosarcoma presenting with multiple subcutaneous scalp mass. Korean J. Gastroenterol. 2005, 46, 233–236. [Google Scholar]
- Kwon, K.M.; Jang, B.K.; Chung, W.J.; Park, K.S.; Cho, K.B.; Hwang, J.S.; Kang, K.J.; Kang, Y.N.; Kwon, J.H. A case of primary hepatic leiomyosarcoma with intrahepatic and abdominal subcutaneous metastasis in Behcet’s disease. Korean J. Hepatol. 2005, 11, 386–391. [Google Scholar] [PubMed]
- Surendrababu, N.R.; Rao, A.; Samuel, R. Primary hepatic leiomyosarcoma in an infant. Pediatr. Radiol. 2006, 36, 366. [Google Scholar] [CrossRef]
- Marin, D.; Catalano, C.; Rossi, M.; Guerrisi, A.; Di Martino, M.; Berloco, P.; Passariello, R. Gadobenate dimeglumine-enhanced magnetic resonance imaging of primary leiomyoma of the liver. J. Magn. Reson. Imaging 2008, 28, 755–758. [Google Scholar] [CrossRef] [PubMed]
- Tsiatis, A.C.; Atkinson, J.B.; Wright, J.K.; Cates, J.M. Primary hepatic myxoid leiomyosarcoma: A case report and review of the literature. Ultrastruct. Pathol. 2008, 32, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Jeong, T.Y.; Kim, Y.S.; Park, K.J.; Lee, J.S.; Huh, J.G.; Ryu, S.H.; Lee, J.H.; Moon, J.S. A case of primary leiomyosarcoma of the liver presenting with acute bleeding. Korean J. Gastroenterol. 2008, 51, 194–198. [Google Scholar]
- Giuliante, F.; Sarno, G.; Ardito, F.; Pierconti, F. Primary hepatic leiomyosarcoma in a young man after Hodgkin’s disease: Diagnostic pitfalls and therapeutic challenge. Tumori J. 2009, 95, 374–377. [Google Scholar] [CrossRef]
- Liang, X.; Shi, X.-M.; Xie, J.-P.; Yang, J.-Y.; Zhang, X.-J.; Fu, Z.-R.; Ding, G.-S.; Li, R.-D. Liver transplantation for primary hepatic leiomyosarcoma: A case report and review of the literatures. Med. Oncol. 2010, 27, 1269–1272. [Google Scholar] [CrossRef]
- Shamseddine, A.; Faraj, W.; Mukherji, D.; El Majzoub, N.; Khalife, M.; Soubra, A.; Shamseddine, A. Unusually young age distribution of primary hepatic leiomyosarcoma: Case series and review of the adult literature. World J. Surg. Oncol. 2010, 8, 56. [Google Scholar] [CrossRef]
- Santos, I.; Valls, C.; Leiva, D.; Serrano, T.; Martinez, L.; Ruiz, S. Primary hepatic leiomyoma: Case report. Abdom. Imaging 2011, 36, 315–317. [Google Scholar] [CrossRef]
- Shivathirthan, N.; Kita, J.; Iso, Y.; Hachiya, H.; Kyunghwa, P.; Sawada, T.; Kubota, K. Primary hepatic leiomyosarcoma: Case report and literature review. World J. Gastrointest. Oncol. 2011, 3, 148–152. [Google Scholar] [CrossRef]
- Tsai, P.S.; Yeh, T.C.; Shih, S.L. Primary hepatic leiomyosarcoma in a 5-month-old female infant. Acta Radiol. Short Rep. 2013, 2, 2047981613498722. [Google Scholar] [CrossRef] [PubMed]
- Raber, E.L.; Cheng, A.L.; Dong, W.F.; Sutherland, F. Primary hepatic leiomyoma in a transplant patient: Characterization with magnetic resonance imaging. Transplantation 2012, 93, e4–e5. [Google Scholar] [CrossRef] [PubMed]
- Chelimilla, H.; Badipatla, K.; Ihimoyan, A.; Niazi, M. A rare occurrence of primary hepatic leiomyosarcoma associated with epstein barr virus infection in an AIDS patient. Case Rep. Gastrointest. Med. 2013, 2013, 691862. [Google Scholar] [CrossRef]
- Metta, H.; Corti, M.; Trione, N.; Masini, D.; Monestes, J.; Rizzolo, M.; Carballido, M. Primary hepatic leiomyosarcoma—A rare neoplasm in an adult patient with AIDS: Second case report and literature review. J. Gastrointest. Cancer 2014, 45 (Suppl. S1), 36–39. [Google Scholar] [CrossRef]
- Luo, X.Z.; Ming, C.S.; Chen, X.P.; Gong, N.Q. Epstein-Barr virus negative primary hepatic leiomyoma: Case report and literature review. World J. Gastroenterol. 2013, 19, 4094–4098. [Google Scholar] [CrossRef]
- Vyas, S.; Psica, A.; Watkins, J.; Yu, D.; Davidson, B. Primary hepatic leiomyoma: Unusual cause of an intrahepatic mass. Ann. Transl. Med. 2015, 3, 73. [Google Scholar] [PubMed]
- Lv, W.F.; Han, J.K.; Cheng, D.L.; Tang, W.J.; Lu, D. Imaging features of primary hepatic leiomyosarcoma: A case report and review of literature. Oncol. Lett. 2015, 9, 2256–2260. [Google Scholar] [CrossRef]
- Navarro, C.; Hamidian Jahromi, A.; Donato, M.; Caliri, N.; Tempra, A.; Sangster, G. Primary Leiomyoma of the Liver: Case Report and Review of the Literature. J. La. State Med. Soc. 2015, 167, 129–133. [Google Scholar] [PubMed]
- Ter-Ovanesov, M.D.; Valkin, D.L.; Gaboyan, A.S.; Kukosh, M.Y.; Ronzin, A.V.; Andrianova, V.S.; Larin, A.L.; Zhuk, A.I. Hepatic leiomyosarcoma: A case report. Vopr Onkol. 2016, 62, 857–862. [Google Scholar]
- Iida, T.; Maeda, T.; Amari, Y.; Yurugi, T.; Tsukamoto, Y.; Nakajima, F. Primary hepatic leiomyosarcoma in a patient with autosomal dominant polycystic kidney disease. CEN Case Rep. 2017, 6, 74–78. [Google Scholar] [CrossRef]
- Blas Laina, J.L.; González Ruiz, Y.; Gonzalvo González, E.; Sanz Moncasi, M.P.; Rodríguez Borobia, A. Primary hepatic leiomyoma: A rare liver mass. Gastroenterol. Hepatol. 2017, 40, 617–619. [Google Scholar] [CrossRef] [PubMed]
- Feretis, T.; Kostakis, I.D.; Damaskos, C.; Garmpis, N.; Mantas, D.; Nonni, A.; Kouraklis, G.; Dimitroulis, D. Primary Hepatic Leiomyosarcoma: A Case Report and Review of the Literature. Acta Med. 2018, 61, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Jia, B.; Jin, Z.; Gao, P.; Liu, Y. Primary hepatic leiomyoma in a Chinese female patient without underlying disease: A case report. BMC Surg. 2019, 19, 140. [Google Scholar] [CrossRef] [PubMed]
- Fraga, J.; Caetano Oliveira, R.; Terracciano, L.; Silva, M.R.; Cipriano, M.A. Hepatic Myxoid Leiomyoma: A Very Rare Tumor. GE Port. J. Gastroenterol. 2020, 27, 352–355. [Google Scholar] [CrossRef] [PubMed]
- Coletta, D.; Parrino, C.; Nicosia, S.; Manzi, E.; Pattaro, G.; Oddi, A.; D’Annibale, M.; Marino, M.; Grazi, G.L. Primary leiomyoma of the liver in an immunocompetent patient. Intractable Rare Dis. Res. 2020, 9, 251–255. [Google Scholar] [CrossRef]
- Chi, M.; Dudek, A.Z.; Wind, K.P. Primary hepatic leiomyosarcoma in adults: Analysis of prognostic factors. Onkologie 2012, 35, 210–214. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Author | Localization, Measure (cm) | Symptoms | Histological Diagnosis |
|---|---|---|---|---|
| 1926 | Demel [3] | RL/12 | RUQ pain | Leiomyoma |
| 1962 | BEAIRD JB [4] | Portal vein | RUQ pain | Leiomyosarcoma |
| 1965 | Dalenz [5] | LL/NS | RUQ pain | Leiomyoma |
| 1975 | Masur [6] | RL/NS | NS | Leiomyosarcoma (2) |
| 1978 | Bloustein [7] | RL/3.3 | RUQ pain | Leiomyosarcoma |
| 1987 | Maki [8] | RL/NS | NS | Leiomyosarcoma |
| 1987 | Griffin [9] | Cava vein | NS | Leiomyosarcoma |
| 1987 | Shurbaji [10] | RL/NS | RUQ pain | Leiomyosarcoma |
| 1988 | Kinoshita [11] | RL/NS | RUQ pain | Leiomyosarcoma |
| 1989 | Rummeny [12] | NS | NS | Leiomyoma |
| 1990 | Herzberg AJ [13] | RL/19 | RUQ pain | Leiomyoma |
| 1990 | Little [14] | LL/NS | NS | Leiomyoma |
| 1990 | Lee [15] | Hepatic vein | RUQ pain | Atypical Leiomyoma |
| 1990 | Spagliardi [16] | RL/NS | None | Leiomyosarcoma |
| 1990 | Sundaresan [17] | Portal vein | RUQ pain | Leiomyosarcoma |
| 1991 | Bartoli [18] | RL/NS | NS | Leiomyoma |
| 1991 | Ishii [19] | 34 cases | / | Leiomyosarcoma |
| 1991 | Korbi [20] | RL/2.1 | None | Leiomyosarcoma |
| 1992 | Reinertson [21] | LL/10 | RUQ pain | Leiomyoma |
| 1992 | Ross J S [22] | RL/3.3 | RUQ pain | Leiomyosarcoma (HIV) |
| 1993 | Baur [23] | RL/NS | RUQ pain | Leiomyosarcoma |
| 1993 | Saint-Paul [24] | RL/9.3 | RUQ pain | Leiomyosarcoma |
| 1994 | Prévot S [25] | RL/NS | RUQ pain | Leiomyoma in HIV |
| 1995 | Hiyama [26] | RL/NS | None | Leiomyosarcoma |
| 1996 | Abdelli [27] | RL/NS | RUQ pain and fever | Leiomyosarcoma |
| 1996 | Davidoff [28] | RL/NS | RUQ pain | Leiomyoma in transplantation |
| 1998 | Yoon [29] | RL/NS | RUQ pain | Myxoid Leiomyoma |
| 1999 | Yanase [30] | RL/12 | RUQ pain | Leiomyoma with Cystoadenoma |
| 1999 | Enoki [31] | Hepatic vein | RUQ pain | Leiomyosarcoma |
| 2000 | Mesenas [32] | RL/3.6 | None | Leiomyoma |
| 2000 | Tsuji [33] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2001 | Belli [34] | RL and LL/30 | Obstruction | Giant leiomyoma |
| 2002 | Torres [35] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2002 | Fujiita [36] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2002 | Lee [37] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2002 | Baek [38] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2004 | Beunzen [39] | RL/6 | RUQ pain | Leiomyoma |
| 2004 | Maruta [40] | RL/13 | RUQ pain | Leiomyosarcoma |
| 2005 | Lee [41] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2005 | Kwon [42] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2006 | Surendrababu [43] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2008 | Marin [44] | RL/3 | RUQ pain | Leiomyoma |
| 2008 | Tsiatis [45] | RL/9.9 | RUQ pain | Leiomyosarcoma |
| 2008 | Jeong [46] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2009 | Giuliante [47] | RL/2.5 | RUQ pain | Leiomyosarcoma |
| 2010 | Liang [48] | RL/5 | RUQ pain | Leiomyosarcoma |
| 2010 | Shamseddine [49] | RL/3 cases | RUQ pain | Leiomyosarcoma (3) |
| 2011 | Santos [50] | RL/5.5 | RUQ pain | Leiomyoma |
| 2011 | Shivathirthan [51] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2012 | Tsai [52] | RL/2.8 | RUQ pain | Leiomyoma |
| 2013 | Raber [53] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2013 | Chelimilla [54] | RL/4.6 | RUQ pain | Leiomyoma |
| 2013 | Metta [55] | RL/3.5 | RUQ pain | Leiomyosarcoma |
| 2014 | Luo [56] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2015 | Vyas [57] | RL/8 | RUQ pain | Leiomyoma |
| 2015 | Wei-Fu Lv [58] | RL/NS | None | Leiomyoma |
| 2015 | Navarro [59] | RL/9.1 | RUQ pain | Leiomyosarcoma |
| 2016 | Ovanesov [60] | RL/NS | None | Leiomyoma |
| 2016 | Takashi Iida [61] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2017 | Blas Laina [62] | RL/NS | RUQ pain | Leiomyosarcoma |
| 2018 | Feretis [63] | RL/13 | RUQ pain | Leiomyosarcoma |
| 2019 | Jia [64] | RL/7.2 | RUQ pain | Leiomyoma |
| 2020 | Fraga [65] | RL/19 | RUQ pain | Leiomyoma |
| 2020 | Coletta [66] | RL/9 | RUQ pain | Leiomyoma |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colagrande, A.; Cazzato, G.; Fedele, S.; Andriola, V.; Ingravallo, G.; Resta, L.; Vincenti, L. A Unique Case of the Transformation of a Hepatic Leiomyoma into Leiomyosarcoma with Pancreatic Metastases: Review of the Literature with Case Presentation. Reports 2022, 5, 2. https://doi.org/10.3390/reports5010002
Colagrande A, Cazzato G, Fedele S, Andriola V, Ingravallo G, Resta L, Vincenti L. A Unique Case of the Transformation of a Hepatic Leiomyoma into Leiomyosarcoma with Pancreatic Metastases: Review of the Literature with Case Presentation. Reports. 2022; 5(1):2. https://doi.org/10.3390/reports5010002
Chicago/Turabian StyleColagrande, Anna, Gerardo Cazzato, Salvatore Fedele, Valeria Andriola, Giuseppe Ingravallo, Leonardo Resta, and Leonardo Vincenti. 2022. "A Unique Case of the Transformation of a Hepatic Leiomyoma into Leiomyosarcoma with Pancreatic Metastases: Review of the Literature with Case Presentation" Reports 5, no. 1: 2. https://doi.org/10.3390/reports5010002
APA StyleColagrande, A., Cazzato, G., Fedele, S., Andriola, V., Ingravallo, G., Resta, L., & Vincenti, L. (2022). A Unique Case of the Transformation of a Hepatic Leiomyoma into Leiomyosarcoma with Pancreatic Metastases: Review of the Literature with Case Presentation. Reports, 5(1), 2. https://doi.org/10.3390/reports5010002