
A Review of Hand–Arm Vibration Studies Conducted by US NIOSH since 2000

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
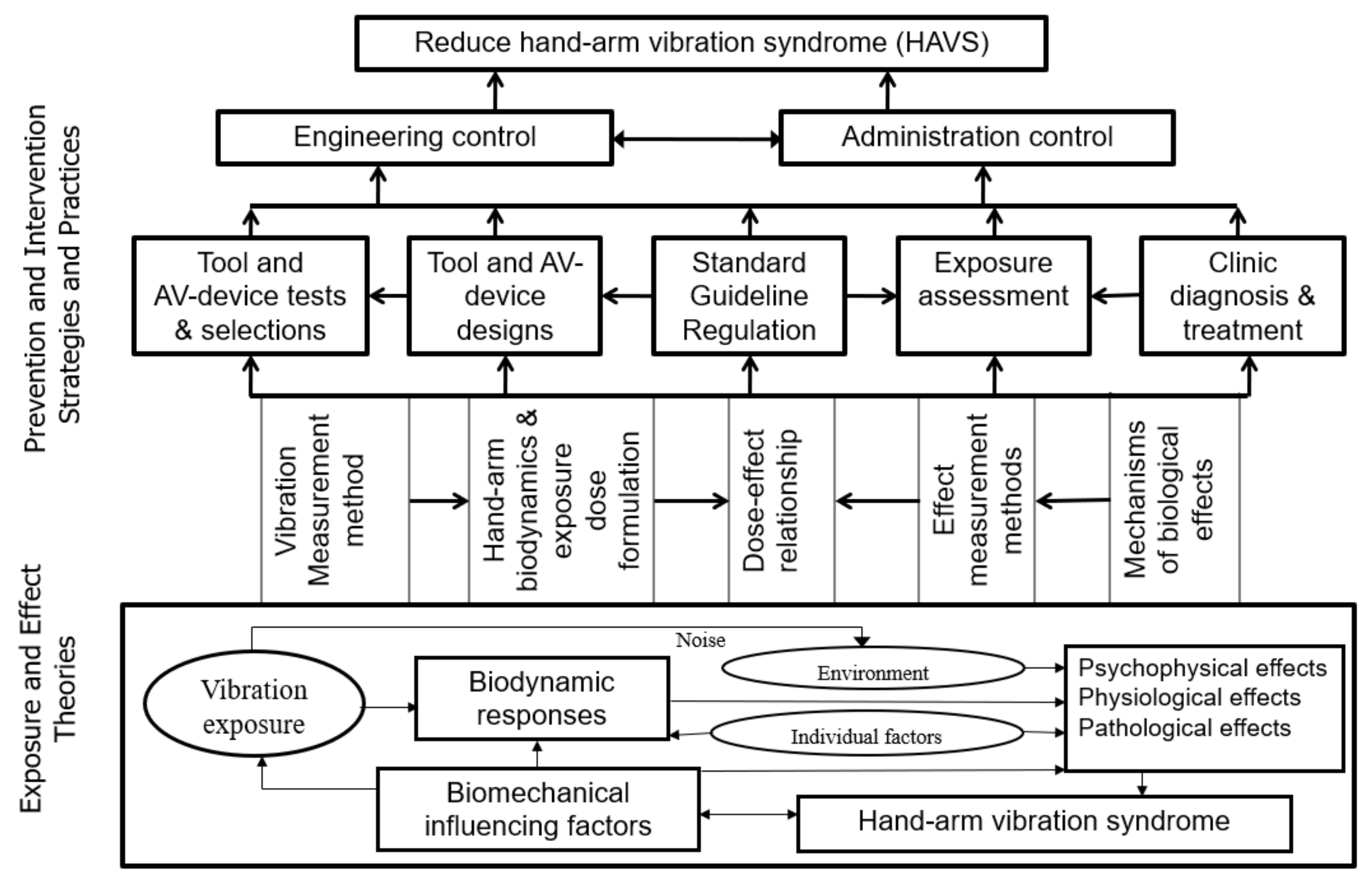
2. General Concepts and Hypotheses
3. The Standard Method for Measuring and Assessing Hand-Transmitted Vibration Exposure
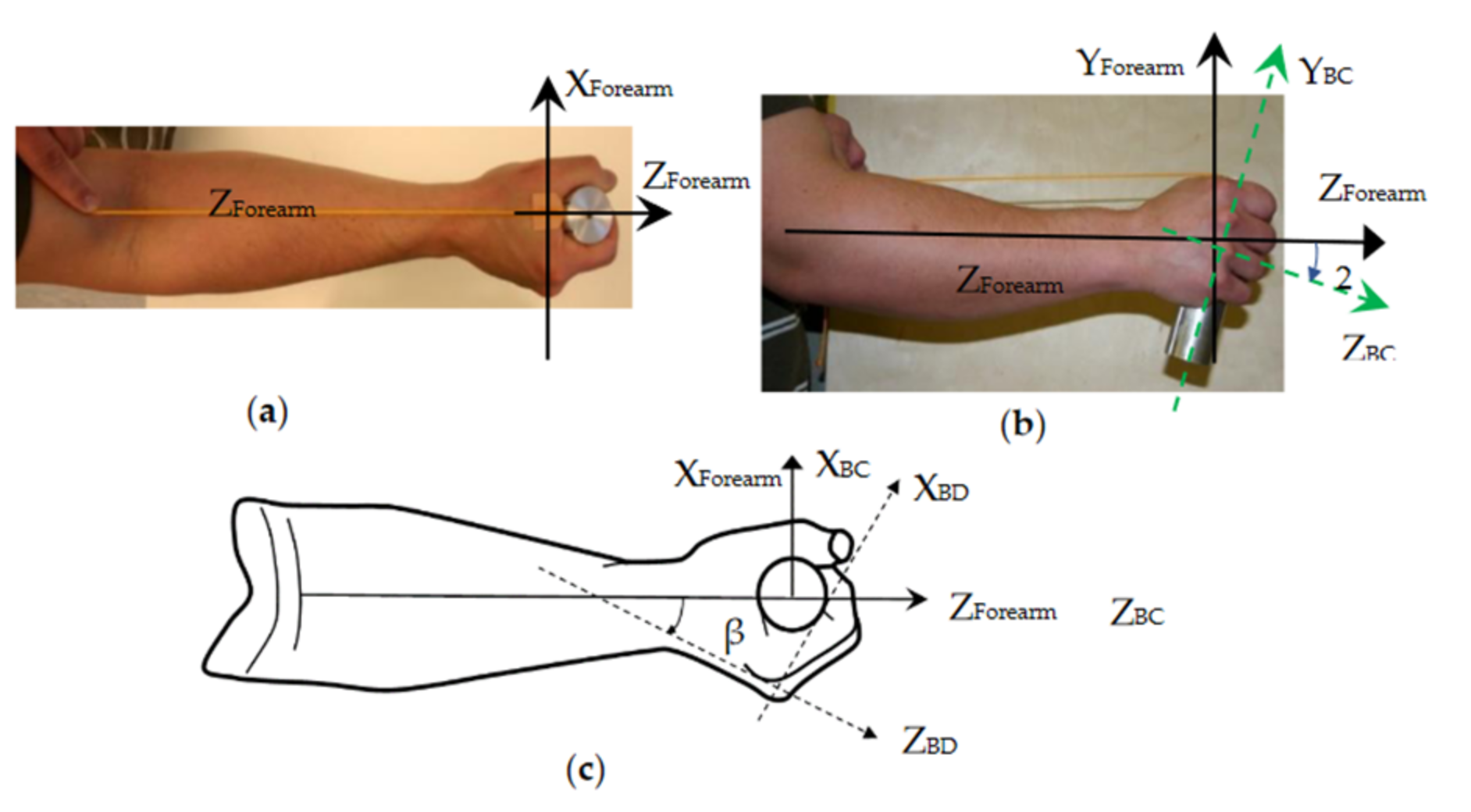
4. Vibration Biodynamics of the Hand–Arm System and Alternative Methods for Quantifying Vibration Exposure
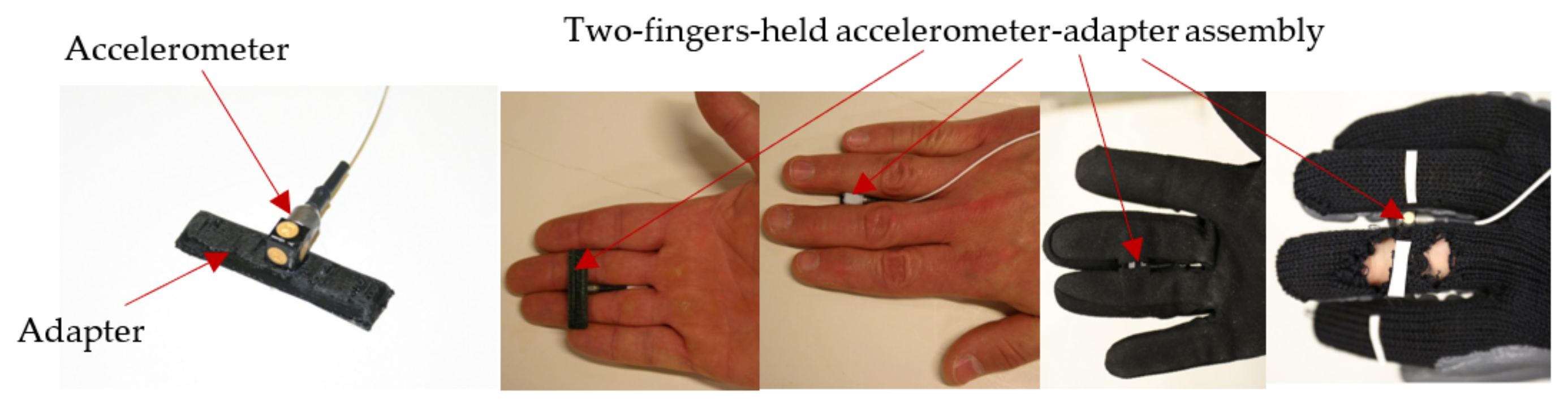
4.1. The Measurement of the Biodynamic Responses of the Hand–Arm System
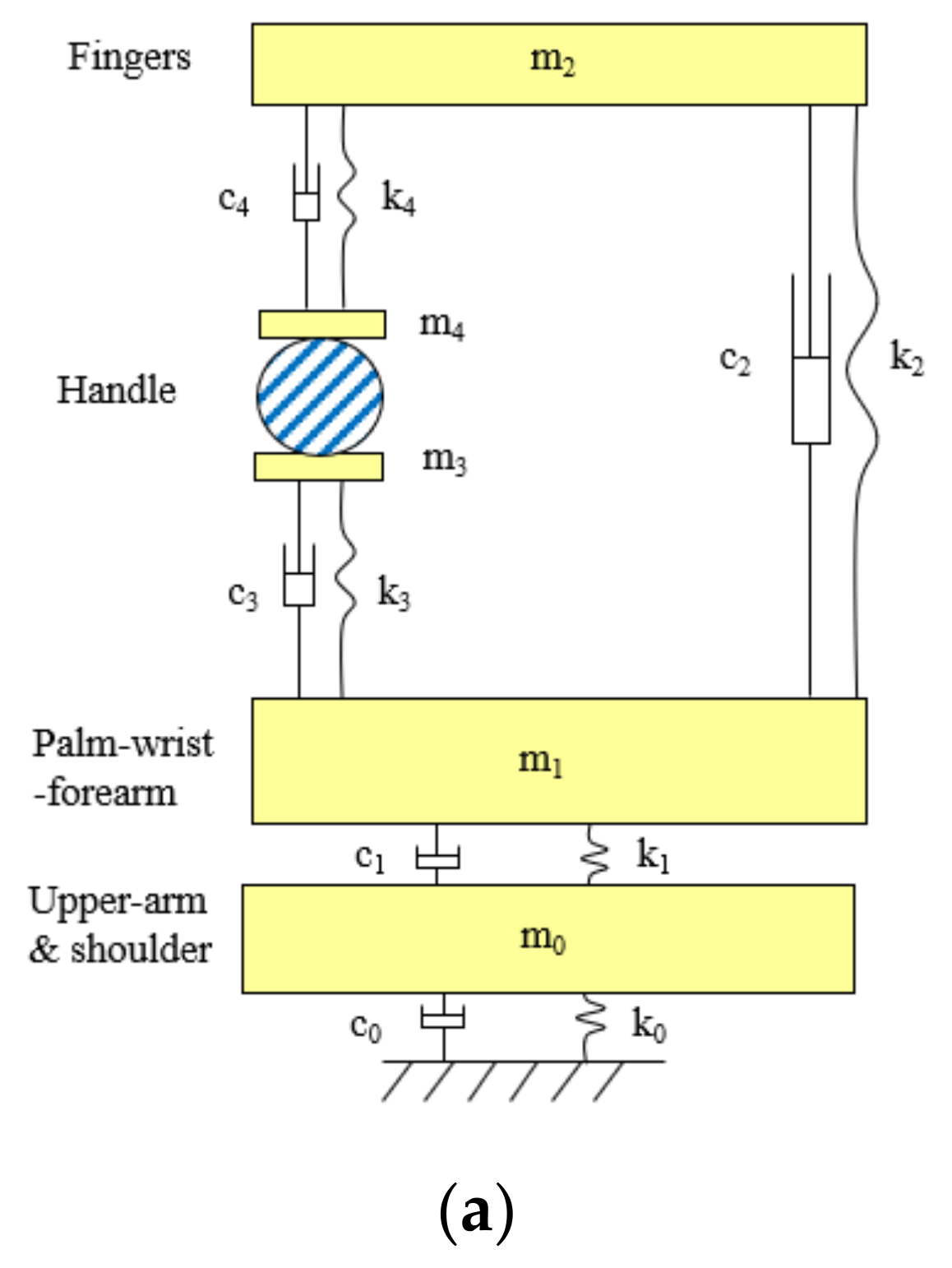
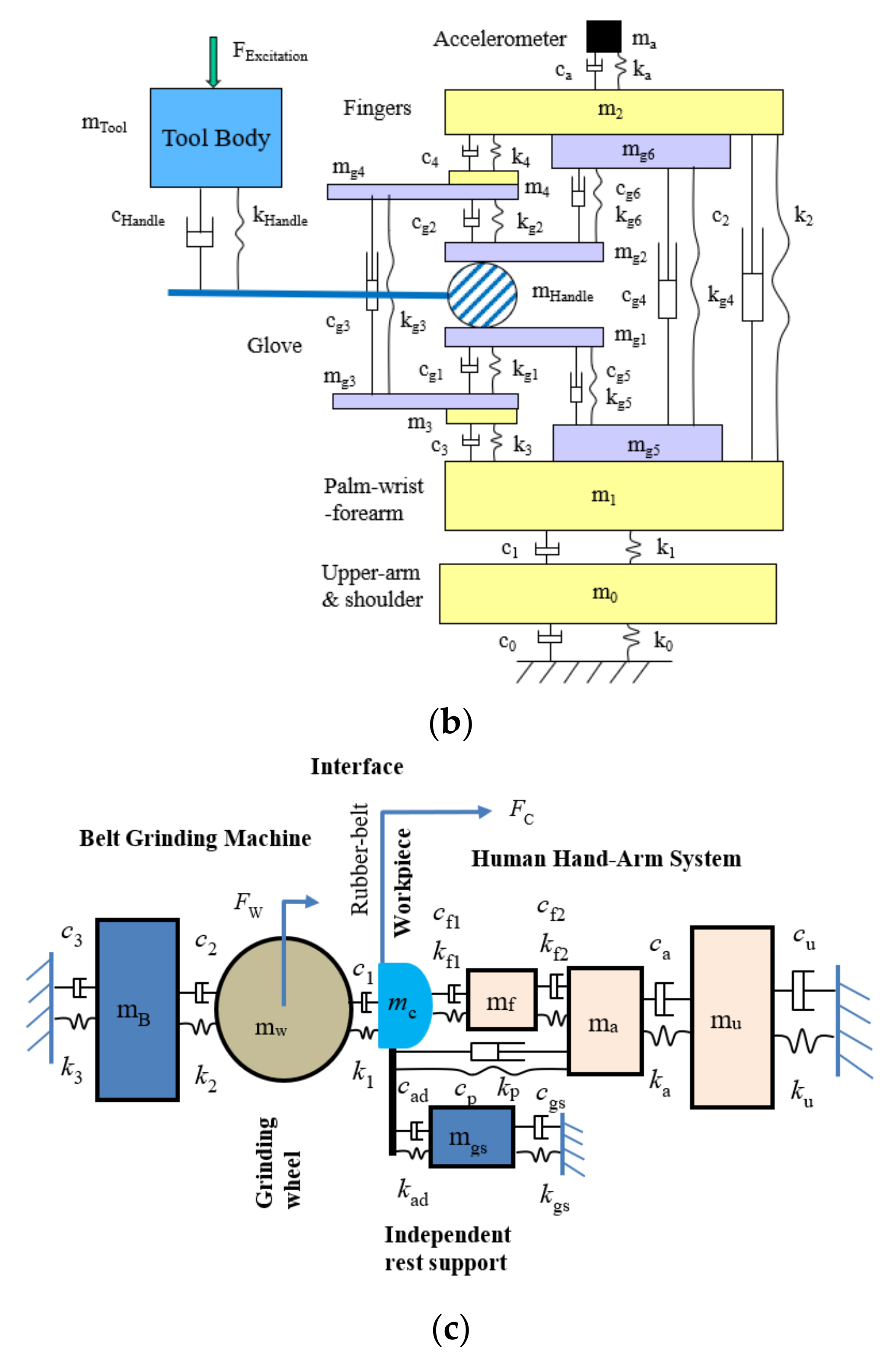
4.2. The Development of Lumped-Parameter Models of the Hand–Arm System
4.3. Alternative Measures of Vibration Exposure and Their Biodynamic Frequency Weightings
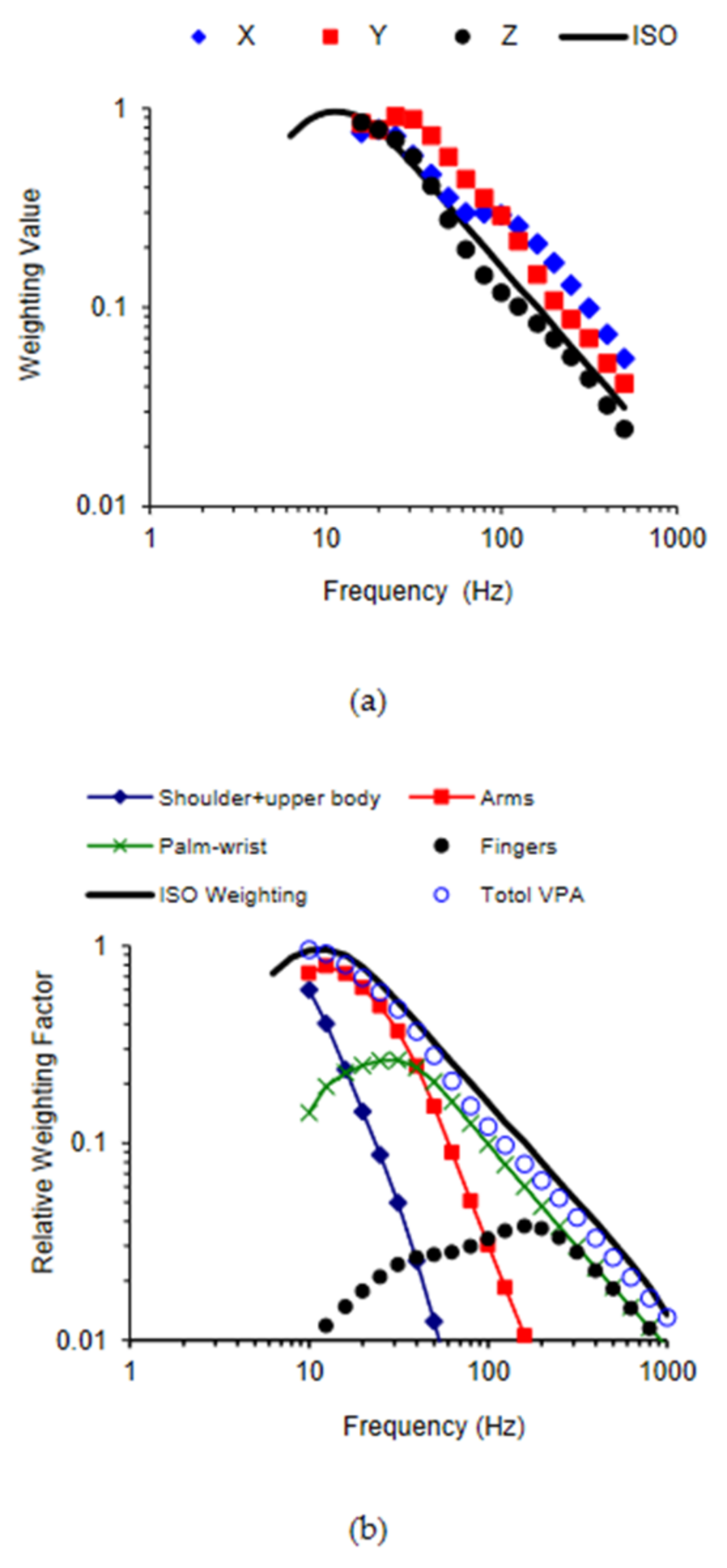
4.3.1. Vibration Acceleration on Hand and Arm Substructures
4.3.2. Vibration Force and Average Vibration Stress
4.3.3. Total Vibration Power Absorption
4.3.4. Substructure Vibration Power Absorption (VPA) and Average VPA Density
4.3.5. Time-Domain Methods
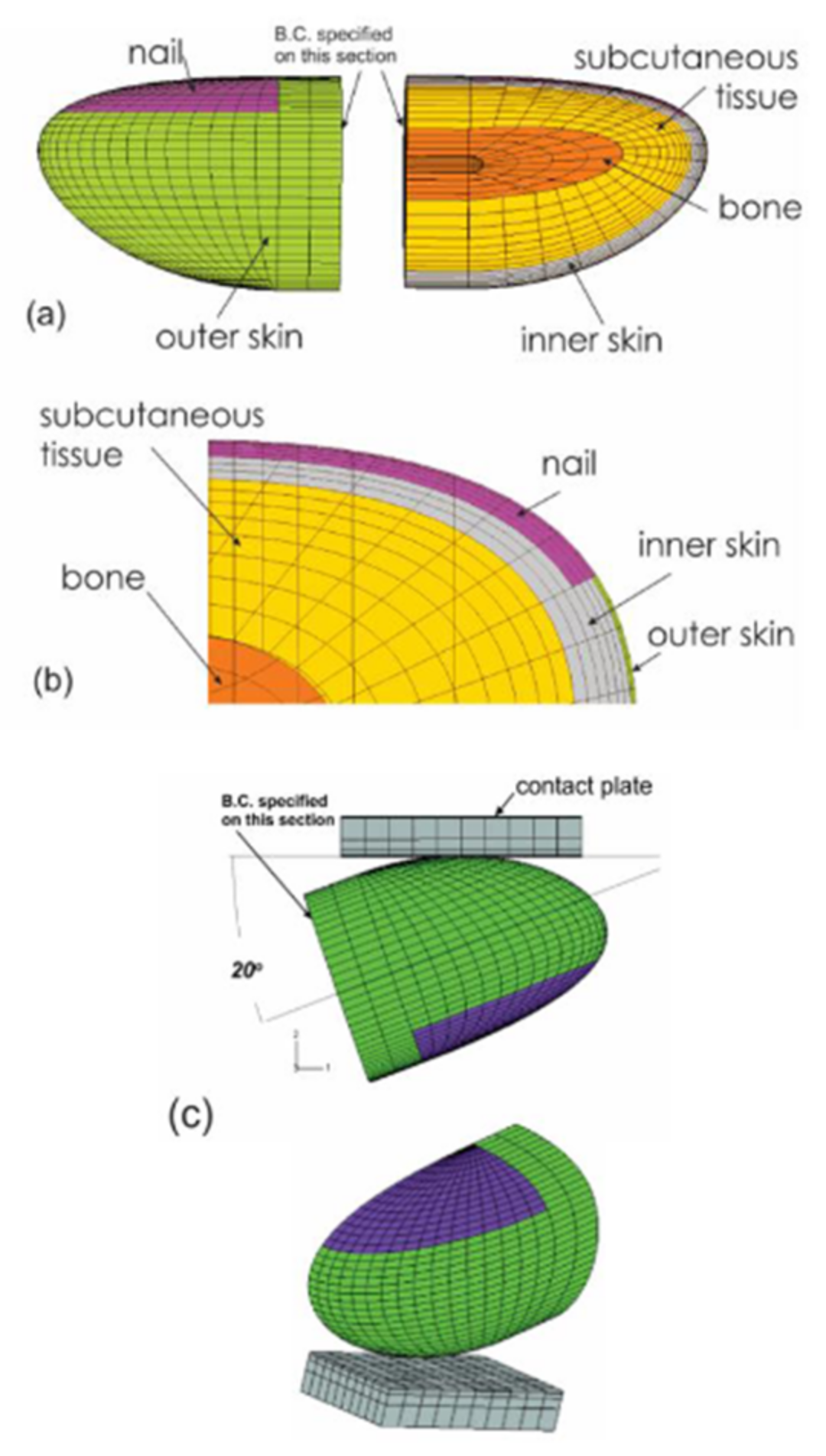
4.4. Finite Element Modeling and Applications
4.4.1. The Time-Dependent Mechanical Response of the Fingertip Subject to Dynamic Loading
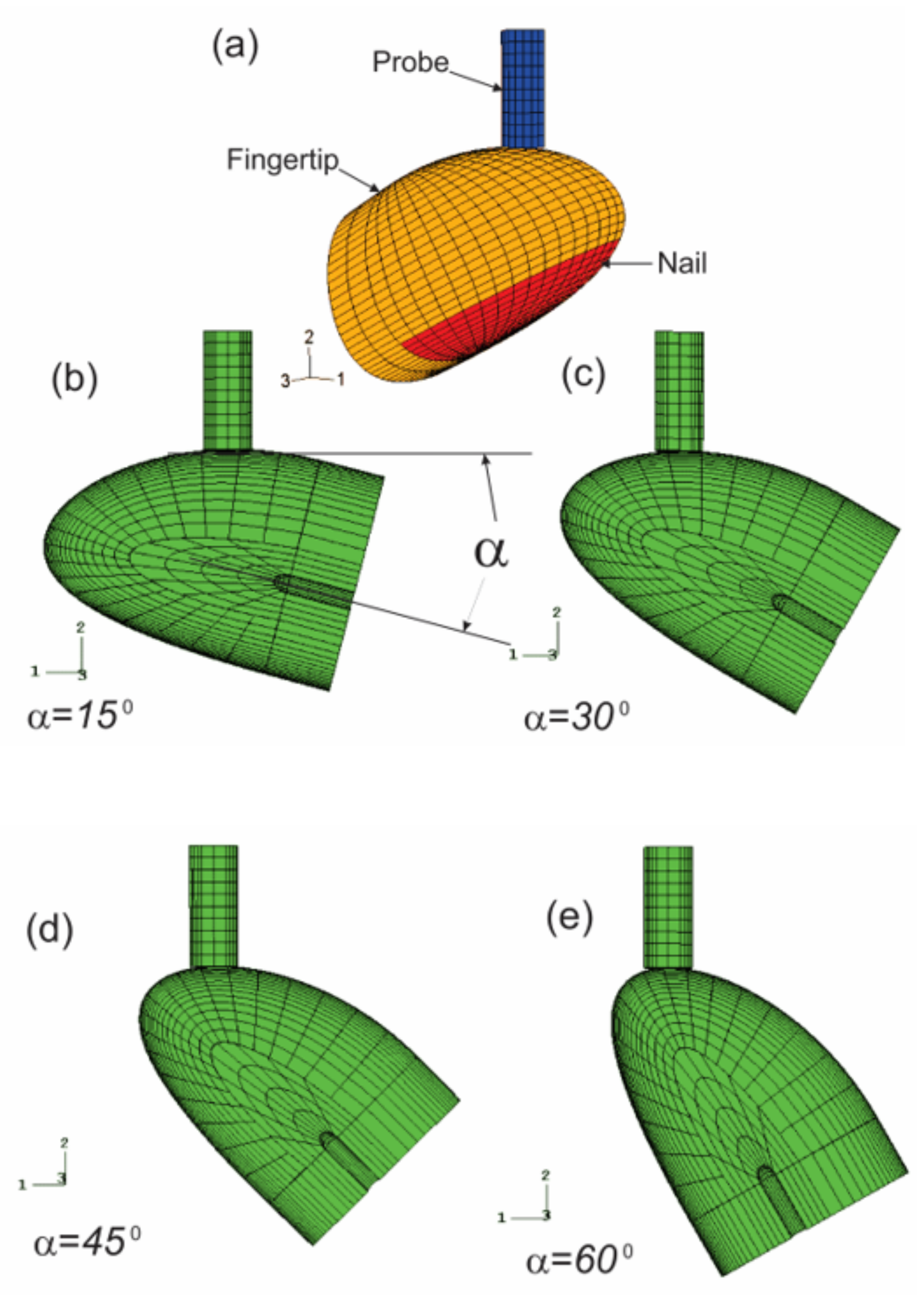
4.4.2. Probe/Fingertip Interaction in Vibrotactile Perception Threshold Testing
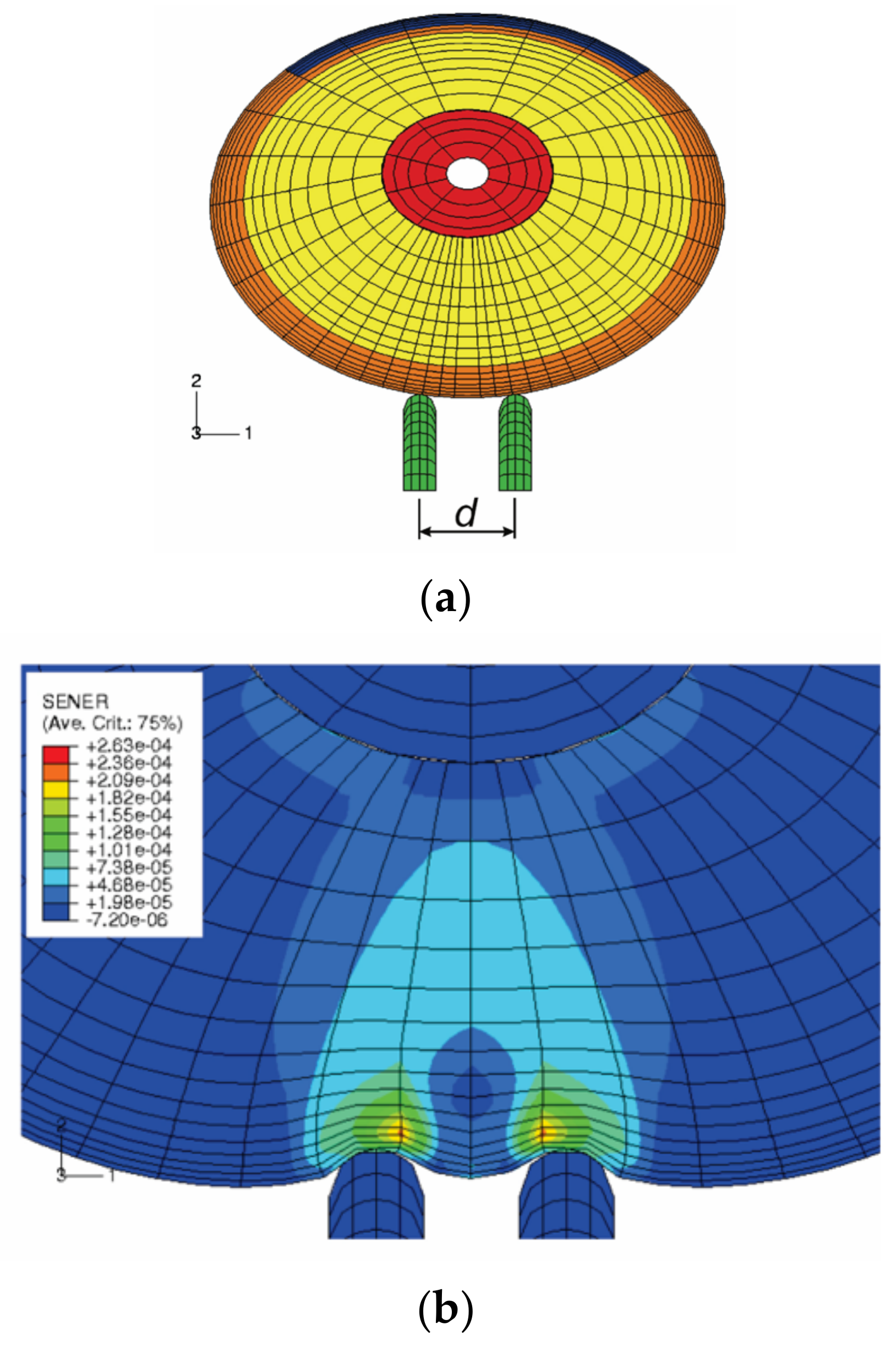
4.4.3. Simulation of Two-Point Discrimination Threshold Test
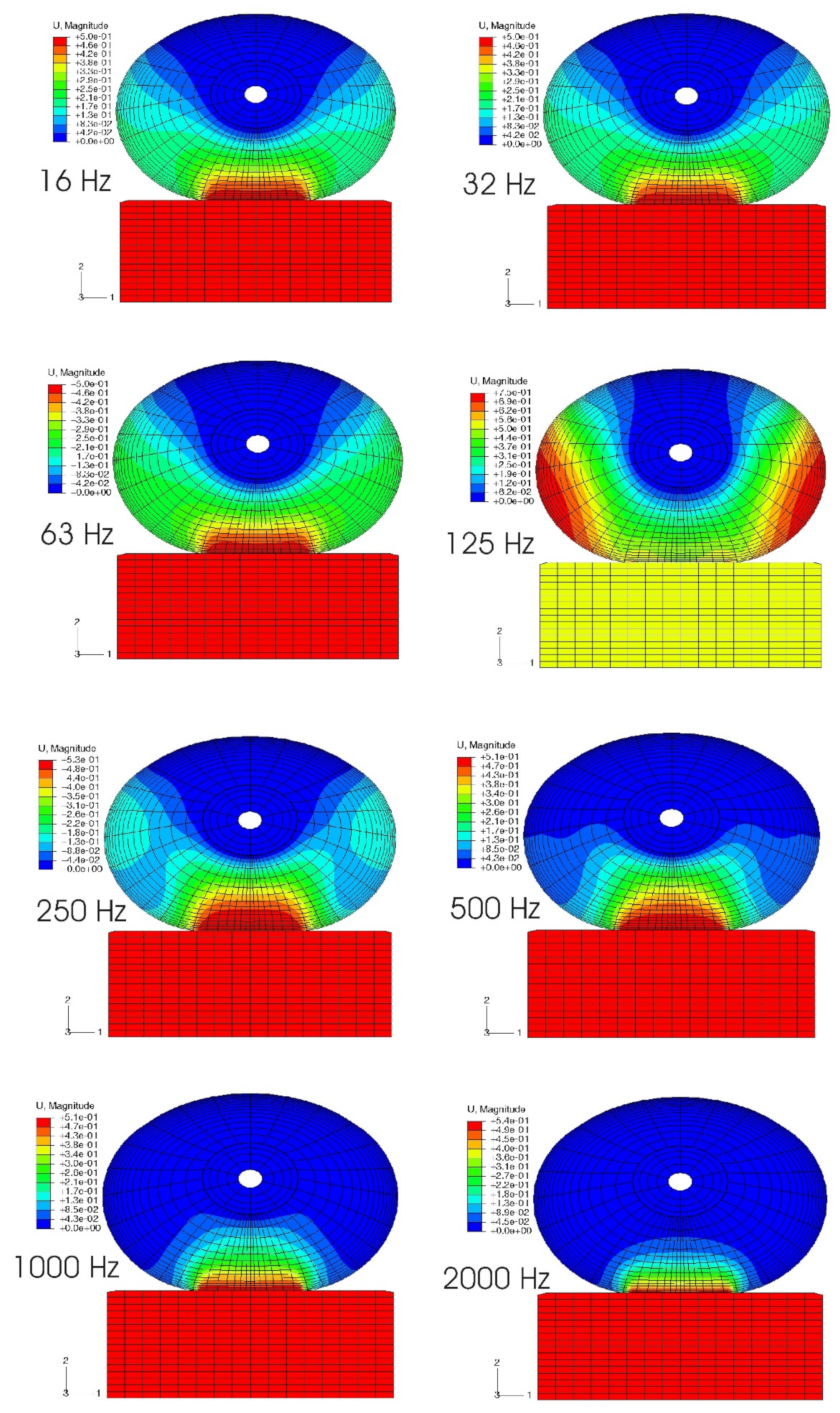
4.4.4. Vibration Modes and Vibration Penetration into the Soft Tissues of a Fingertip
4.4.5. The Effects of Shear Vibration to Soft Tissues
4.4.6. Response of Mechanoreceptors to Vibratory Stimuli
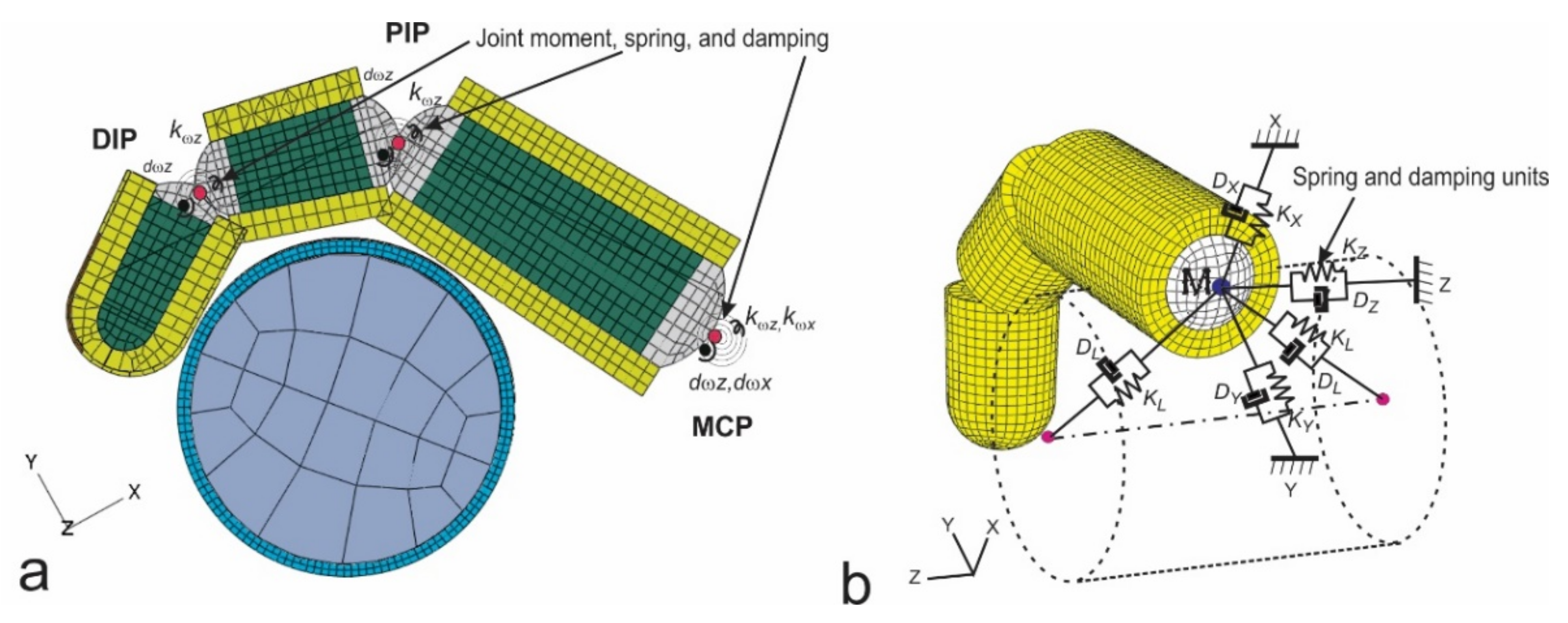
4.4.7. Interaction between Grip Force and Vibration Transmissibility
4.4.8. Biodynamic Interaction between the Fingertip and Probe in the Vibrotactile Tests
4.4.9. Further FE Model Development
5. Influencing Biomechanical Factors and Effect Assessments
6. Intervention Methods and Technologies for Controlling Hand-Transmitted Exposure
7. Biological Effects of Hand-Transmitted Vibration Exposure
7.1. Tail Model and Sinusoidal Vibration
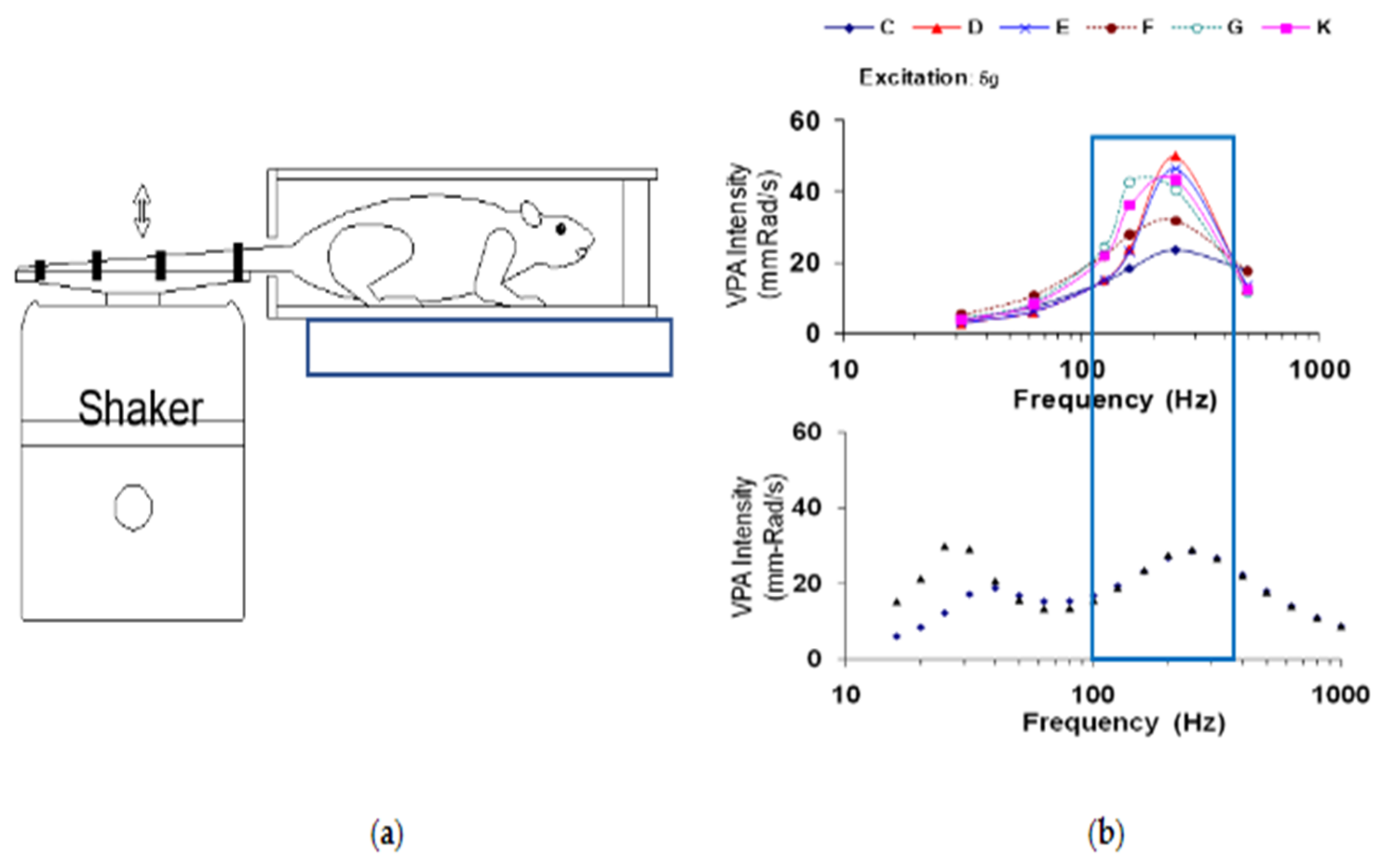
7.1.1. Biodynamic Response in an Animal Model of Vibration-Induced Injury
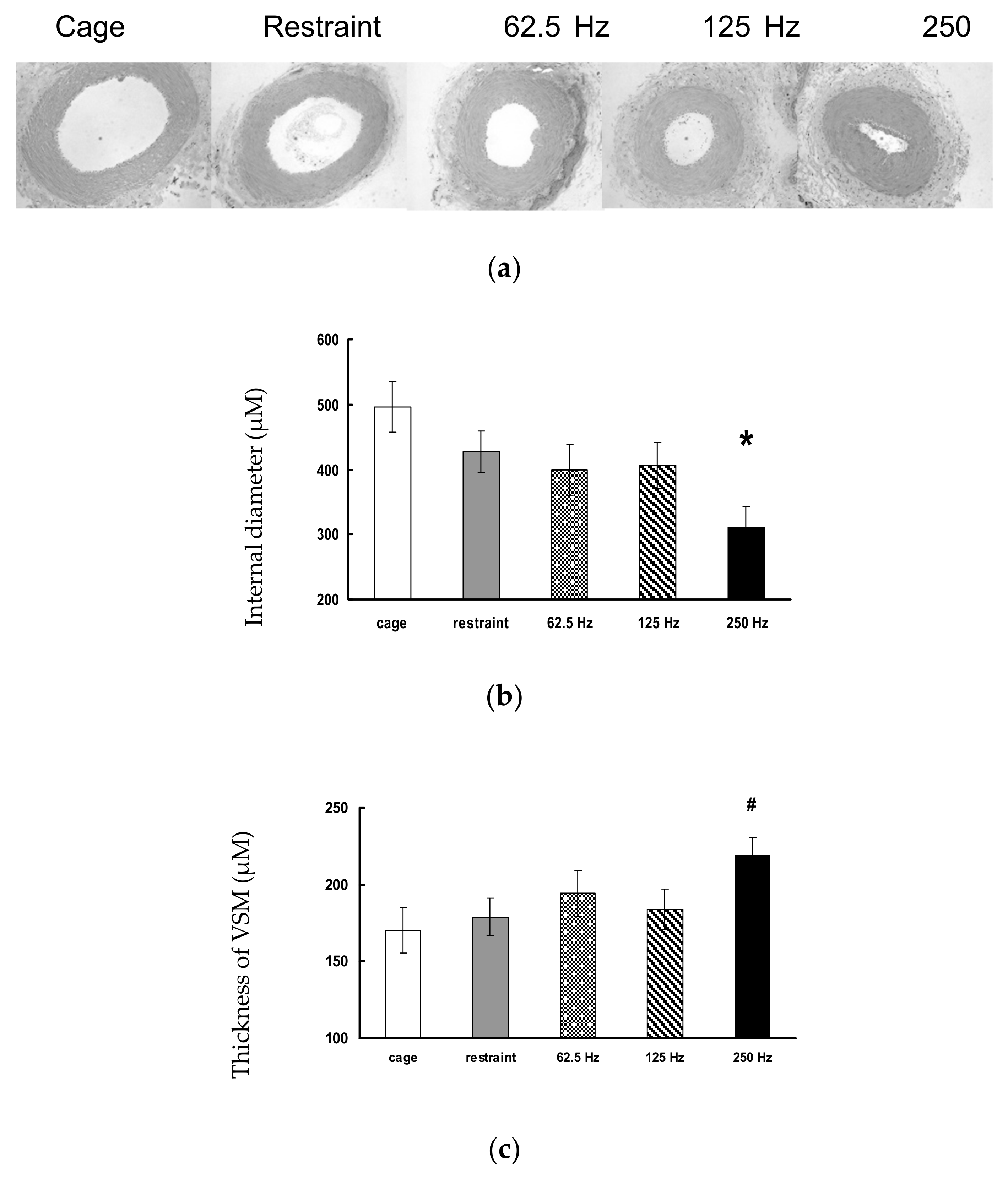
7.1.2. Frequency-Dependence of Vibration-Induced Vascular Dysfunction
7.1.3. Frequency-Dependence of Vibration-Induced Sensorineural Dysfunction
7.1.4. Potential Biomarkers of Vibration-Induced Injury
7.2. Paw Vibration Model
7.3. Models of Impact Vibration
7.4. Animal Models and Anti-Vibration Materials (VR Gloves)
7.5. Additional Studies and Data
8. Physiological Measurements of Vibration Health Effects
8.1. Animal Studies of Vascular Function Using the NIOSH Rat-Tail Model
8.2. Animal Studies of Sensorineural Function Using the NIOSH Rat-Tail Model
8.3. Automated Nail Blanching Test
8.4. Improved Thermal Perception Threshold Test
9. Summary and Major Areas for Future Research
- The fatigue-failure theory applied to vibration exposure and health effects has not been well established. While the combination of further experimental and FE modeling studies can provide reliable quantifications of various vibration dose measures, further biological studies are needed to test each of them. Most of the published biological studies examined the association between vibration exposure factors (vibration acceleration magnitude, frequency, and duration) and vibration biological effects, which includes biodynamic and biological processes. There is still a lack of information on the specific role of each process in determining the biological effects. It remains unknown what the quantitative relationship between a detailed biodynamic response (stress, strain, or VPAD) and a biological effect in the body or exposed appendage, which is the critical part of the vibration fatigue-failure theory. Biological models should be designed such that the biodynamic responses can be conveniently measured and controlled and the biological studies can focus on the second process: from biodynamic responses to the biological effects. This may require synergized efforts by biodynamic and biological researchers.
- While the overall psychophysical responses such as the vibration sensation, discomfort, and pain of the entire hand–arm system have been investigated and the results have been used as a basis to determine the standard frequency weighting of the hand-transmitted vibration exposure, few studies have examined the relationship between the location-specific vibration biodynamics and psychophysical responses [99]. Further studies in this aspect may help determine the location-specific frequency weightings of the HTV exposure.
- Applied hand forces, hand–arm postures, and vibration exposure direction may significantly affect biodynamic and physiological responses but they have not been considered in the standard method for the HTV risk assessment. Further studies are required to develop more effective devices for their measurement and to determine their specific weightings in the formulation of the HTV exposure dose.
- It is highly desired to have a reliable and convenient device to measure and monitor the vibration exposure of workers at workplaces. Further studies are required to apply advanced technologies to improve HTV dosimeters and to develop effective HTV exposure direct-reading devices.
- The current diagnosis of the hand–arm vibration syndrome depends on the use of a combined subjective survey and some measurement technologies. Some misdiagnosis may happen. Further studies are required to develop more reliable objective methods/devices for the diagnosis of HAVS. A reliable dose–effect relationship can be established only when the vibration exposure dose that truly reflects the exposure factors can be formulated and the vibration health effects can be reliably quantified.
- It remains a research challenge to develop more effective VR tools and devices without decreasing productivity and/or causing other safety concerns. Further development and application of mechanical arms and exoskeletons may help design more effective VR tools and devices. Further studies are also required to evaluate these new technologies and to minimize their adverse effects. The development and application of other new intervention methods and technologies that can decrease the required hand forces, avoid awkward hand and arm postures, and increase safe work practices (e.g., keeping hand warm and dry, and reducing noise exposure) may also help control HAVS.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Griffin, M.J. Handbook of Human Vibration; Academic Press: London, UK, 1990. [Google Scholar]
- Pelmear, P.L.; Wasserman, D.E. Hand-Arm Vibration: A Comprehensive Guide for Occupational Health Professionals, 2nd ed.; OEM Press: Beverly Farms, MA, USA, 1998. [Google Scholar]
- Raynaud, M. On Local Asphyxia and Symmetrical Gangrene at the Extremities. Master’s Thesis, Paris, France, 1862. [Google Scholar]
- International Organization for Standardization. ISO 5349-1: Mechanical Vibration—Measurement and Evaluation of Human Exposure to Hand-Transmitted Vibration—Part 1: General Requirements; International Organization for Standardization: Geneva, Switzerland, 2001. [Google Scholar]
- Loriga, G. Pneumatic tools: Occupation and health. Boll Inspett Labor 1911, 2, 35–60. [Google Scholar]
- Hamilton, A. A Study of Spastic Anemia in the Hands of Stonecutters: An Effect of the Air Hammer on the Hands of Stonecutters; Reports of Physicians for the Bureau of Labor Statistics; Industrial Accidents and Hygiene Series; Government Printing Office: Washington, DC, USA, 1918; Volume 236, pp. 53–66.
- NIOSH. Musculoskeletal Disorders and Workplace Factors: A Critical Review of Epidemiologic Evidence for Work-Related Musculoskeletal Disorders of the Neck, Upper Extremity, and Low Back; DHHS/NIOSH Publication 97-141; U.S. Department of Health and Human Services, National Institute for Occupational Safety and Health: Cincinnati, OH, USA, 1997.
- Zechmann, E.; Geiger, M.; Beamer, B. How to buy safer, quieter tools: A process management approach to reducing noise and hand-arm vibration while improving productivity and quality. Synergist 2018, 29, 26–30. [Google Scholar]
- Wasserman, D.E.; Reynold, D.D. A unique historical perspective of occupational hand-arm vibration in the U.S. from 1918–2004. In Proceedings of the 10th International Conference on Hand-Arm Vibration, Las Vegas, NV, USA, 7–11 June 2004. [Google Scholar]
- Wasserman, D.; Taylor, W.; Behrens, V.; Samueloff, S.; Reynolds, D. Vibration White Finger in U.S. Workers Using Chipping Hammers and Grinding Hand Tools. Volume I–Epidemiology; DHHS/NIOSH Publication 82-118; U.S. Department of Health and Human Services, National Institute for Occupational Safety and Health: Cincinnati, OH, USA, 1982.
- Taylor, W.; Wasserman, D.; Behrens, V.; Reynolds, D.; Samueloff, S. Effect of the air hammer on the hands of stonecutters. The limestone quarries of Bedford, Indiana, revisited. Br. J. Ind. Med. 1984, 41, 289–295. [Google Scholar] [CrossRef] [PubMed]
- NIOSH. Criteria for a Recommended Standard: Occupational Exposure to Hand-Arm Vibration; DHHS/NIOSH Publication 89-106; U.S. Department of Health and Human Services, National Institute for Occupational Safety and Health: Cincinnati, OH, USA, 1989.
- NIOSH. Current Intelligence Bulletin 38—Vibration Syndrome; DHHS/NIOSH Publication 83-110; U.S. Department of Health and Human Services, National Institute for Occupational Safety and Health: Cincinnati, OH, USA, 1983.
- International Organization for Standardization. ISO 5349: Mechanical Vibration—Guidelines for the Measurement of Human Exposure to Hand-Transmitted Vibration; International Organization for Standardization: Geneva, Switzerland, 1986. [Google Scholar]
- Acoustical Society of America. ANSI/ASA, S3.34: Guide for the Measurement and Evaluation of Human Exposure to Vibration Transmitted to the Hand; Acoustical Society of America: New York, NY, USA, 1986. [Google Scholar]
- ACGIH. Threshold Limit Values (TLV) for Hand-Arm Vibration; The American Conference of Governmental Industrial Hygienists (ACGIH): Washington, DC, USA, 1984. [Google Scholar]
- Ralph, I.; Stephens, A.F.; Stephens, R.R.; Fuchs, H.O. Metal Fatigue in Engineering; John Wiley & Sons: Hoboken, NJ, USA, 2000. [Google Scholar]
- Dong, R.G.; Welcome, D.E.; McDowell, T.W.; Xu, X.S.; Krajnak, K.; Wu, J.Z. A proposed theory on biodynamic frequency weighting for hand-transmitted vibration exposure. Ind. Health 2012, 50, 412–424. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, S.; Schall, M.C. Musculoskeletal disorders as a fatigue failure process: Evidence, implications and research needs. Ergonomics 2017, 60, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Olsen, N. Centrally and locally mediated vasomotor activities in Raynaud’s phenomenon. Scand. J. Work. Environ. Health 1987, 13, 309–312. [Google Scholar] [CrossRef]
- Olsen, N.; Fjeldborg, P.; Brchner-Mortensen, J. Sympathetic and local vasoconstrictor response to cold in vibration induced white finger. Br. J. Ind. Med. 1985, 42, 272–275. [Google Scholar] [CrossRef]
- Bovenzi, M. Exposure-response relationship in the hand-arm vibration syndrome: An overview of current epidemiology research. Int. Arch. Occup. Environ. Health 1998, 71, 509–519. [Google Scholar] [CrossRef]
- Acoustical Society of America. ANSI/ASA, S2.70: Guide for the Measurement and Evaluation of Human Exposure to Vibration Transmitted to the Hand; Acoustical Society of America: New York, NY, USA, 2006. [Google Scholar]
- European Union. Directive 2002/44/EC of the European Parliament and of the Council of 25 June 2002 on the Minimum Health and Safety Requirements Regarding the Exposure of Workers to the Risks Arising from Physical Agents (Vibration); European Union: Brussels, Belgium, 2002; pp. 13–19. [Google Scholar]
- Akesson, I.; Lundborg, G.; Horstmann, V.; Skerfving, S. Neuropathy in female dental personnel exposed to high frequency vibrations. Occup. Environ. Med. 1995, 52, 116–123. [Google Scholar] [CrossRef]
- Palmer, K.T.; Haward, B.; Griffin, M.J.; Bendall, H.; Coggon, D. Validity of self reported occupational exposure to hand transmitted and whole body vibration. Occup. Environ. Med. 2000, 57, 237–241. [Google Scholar] [CrossRef]
- Dong, R.G.; Bader, J.; Welcome, D.E.; Rakheja, S.; Schopper, A.W. An accurate method for measuring the exposure duration of hand-transmitted vibration. In Proceedings of the 36th UK Conference on Human Response to Vibration, Farnborough, UK, 12–14 September 2001. [Google Scholar]
- Xu, X.S.; Welcome, D.E.; McDowell, T.W.; Warren, C.; Dong, R.G. An investigation on characteristics of the vibration transmitted to wrist and elbow in the operation of impact wrenches. Int. J. Ind. Ergon. 2009, 39, 174–184. [Google Scholar] [CrossRef]
- Xu, X.S.; Dong, R.G.; Welcome, D.E.; Warren, C.; McDowell, T.W. An examination of an adapter method for measuring the vibration transmitted to the human arms. Measurement 2015, 73, 318–334. [Google Scholar] [CrossRef]
- Kitchener, R. The measurement of hand-arm vibration in industry. In Proceedings of the International Occupational Hand-Arm Vibration Conference, Cincinnati, OH, USA, October 1975; NIOSH: Cincinnati, OH, USA, 1975. [Google Scholar]
- Maeda, S.D.; Dong, R.G. Measurement of hand-transmitted vibration exposure. In Proceedings of the 10th International Conference on Hand-Arm Vibration, Las Vegas, NV, USA, 7–11 June 2004. [Google Scholar]
- Dong, R.G.; McDowell, T.W.; Welcome, D.E.; Rakheja, S.; Caporali, S.A.; Schopper, A.W. Effectiveness of a transfer function method for evaluating vibration isolation performance of gloves when used with chipping hammers. J. Low Freq. Noise Vib. Act. Control 2002, 21, 141–155. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO 5349-2: Mechanical Vibration—Measurement and Evaluation of Human Exposure to Hand-Transmitted Vibration—Part 2: Practical Guidance for Measurement at the Workplace; International Organization for Standardization: Geneva, Switzerland, 2001. [Google Scholar]
- Xu, X.S.; Dong, R.G.; Welcome, D.E.; McDowell, T.W.; Wu, J.Z.; Wimer, B.; Warren, C. An examination of the handheld adapter approach for measuring hand-transmitted vibration exposure. Measurement 2014, 47, 64–77. [Google Scholar] [CrossRef]
- Xu, X.S.; Welcome, D.E.; Warren, C.; McDowell, T.W.; Dong, R.G. Development of a finger adapter method for testing and evaluating vibration-reducing gloves and materials. Measurement 2019, 137, 362–374. [Google Scholar] [CrossRef] [PubMed]
- Dong, R.G.; Welcome, D.E.; Xu, X.S.; Warren, C.; McDowell, T.W.; Wu, J.Z.; Rakheja, S. Mechanical impedances distributed at the fingers and palm of the human hand in three orthogonal directions. J. Sound Vib. 2012, 331, 1191–1206. [Google Scholar] [CrossRef][Green Version]
- Welcome, D.E.; Dong, R.G.; Xu, X.S.; Warren, C.; McDowell, T.W.; Wu, J.Z. An examination of the vibration transmissibility of the hand-arm system in three orthogonal directions. Int. J. Ind. Erg. 2015, 45, 21–34. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Standardization. ISO 8727: Mechanical Vibration and Shock—Human Exposure—Biodynamic Coordinate Systems; International Organization for Standardization: Geneva, Switzerland, 1997. [Google Scholar]
- Dong, R.G.; Sinsel, E.W.; Welcome, D.E.; Warren, C.; Xu, X.S.; McDowell, T.W.; Wu, J.Z. Review and evaluation of hand-arm coordinate systems for measuring vibration exposure, biodynamic responses, and hand forces. Saf. Health Work 2015, 6, 159–173. [Google Scholar] [CrossRef][Green Version]
- International Organization for Standardization. ISO 2631-1: Mechanical Vibration and Shock -Evaluation of Human Exposure to Whole-Body Vibration—Part 1: General Requirements; International Organization for Standardization: Geneva, Switzerland, 1997. [Google Scholar]
- International Organization for Standardization. ISO 10068: Mechanical Vibration and Shock—Mechanical Impedance of the Human Hand-Arm System at the Driving Point; International Organization for Standardization: Geneva, Switzerland, 2012. [Google Scholar]
- International Organization for Standardization. ISO 10819: Mechanical Vibration and Shock—Hand-Arm Vibration—Measurement and Evaluation of the Vibration Transmissibility of Gloves at the Palm of the Hand; International Organization for Standardization: Geneva, Switzerland, 2013. [Google Scholar]
- International Organization for Standardization. ISO 15230: Mechanical Vibration and Shock—Coupling Forces at the Man—Machine Interface for Hand-Transmitted Vibration; International Organization for Standardization: Geneva, Switzerland, 2007. [Google Scholar]
- McDowell, T.W.; Dong, R.G.; Welcome, D.E.; Warren, C.; Xu, X.S. Vibration-reducing gloves: Transmissibility at the palm of the hand in three orthogonal directions. Ergonomics 2013, 56, 1823–1840. [Google Scholar] [CrossRef] [PubMed]
- Dong, R.G.; Welcome, D.E.; Wu, J.Z. Frequency weightings based on biodynamic responses of fingers-hand-arm system. Ind. Health 2005, 43, 485–494. [Google Scholar] [CrossRef]
- Dong, R.G.; Welcome, D.E.; McCormick, R. 3-D Laboratory simulation of hand-transmitted vibration. In Proceedings of the 13th Japan Group Meeting on Human Responses to Vibration, Osaka, Japan, 3–5 August 2005; pp. 41–51. [Google Scholar]
- Dong, R.G.; McDowell, T.W.; Welcome, D.E.; Wu, J.Z.; Warren, C.; Smutz, W.P.; Schopper, A.W. Mechanical energy absorption in human fingers exposed to hand-transmitted vibration. In Biomedical Engineering Recent Developments; Vossoughi, J., Ed.; Medical and Engineering Publishers, Inc.: Washington, DC, USA, 2002; pp. 159–160. [Google Scholar]
- Dong, R.G.; Rakheja, S.; Schopper, A.W.; Han, B.; Smutz, W.P. Hand-transmitted vibration and biodynamic response of the human hand-arm: A critical review. Crit. Rev. Biomed. Eng. 2001, 29, 393–439. [Google Scholar] [CrossRef] [PubMed]
- Dong, R.G.; Rakheja, S.; McDowell, T.W.; Welcome, D.E.; Wu, J.Z. Estimation of the biodynamic responses distributed at fingers and palm based on the total response of the hand-arm system. Int. J. Ind. Ergon. 2010, 40, 425–436. [Google Scholar] [CrossRef]
- Dong, R.G.; Welcome, D.E.; McDowell, T.W.; Wu, J.Z. Measurement of biodynamic response of human hand-arm system. J. Sound Vib. 2006, 294, 807–827. [Google Scholar] [CrossRef]
- Dong, R.G.; Welcome, D.E.; McDowell, T.W.; Wu, J.Z. Analysis of handle dynamics-induced errors in hand biodynamic measurements. J. Sound Vib. 2008, 318, 1313–1333. [Google Scholar] [CrossRef]
- Welcome, D.E.; Dong, R.G. Instrumented handles for studying hand-transmitted vibration exposure. In Proceedings of the 1st American Conference on Human Vibration, Morgantown, WV, USA, 5–7 June 2006. [Google Scholar]
- Dong, R.G.; McDowell, T.W.; Welcome, D.E.; Warren, C.; Wu, J.Z.; Rakheja, S. Analysis of anti-vibration gloves mechanism and evaluation methods. J. Sound Vib. 2009, 321, 435–453. [Google Scholar] [CrossRef]
- Welcome, D.E.; Dong, R.G.; Xu, X.S.; Warren, C.; McDowell, T.W. The effects of vibration-reducing gloves on finger vibration. Int. J. Ind. Erg. 2014, 44, 45–59. [Google Scholar] [CrossRef]
- Pan, D.; Xu, X.S.; Welcome, D.E.; McDowell, T.W.; Warren, C.; Wu, J.Z.; Dong, R.G. The relationships between hand forces and vibration responses of the human-arm system. Ergonomics 2018, 61, 818–830. [Google Scholar] [CrossRef]
- McDowell, T.W.; Wike, S.F.; Dong, R.G.; Welcome, D.E.; Schopper, A.W. Evaluation of psychometric estimates of vibratory hand-tool grip and push forces. Int. J. Ind. Ergon. 2006, 36, 119–128. [Google Scholar] [CrossRef]
- McDowell, T.W.; Wike, S.F.; Dong, R.G.; Welcome, D.E. Effects of vibration on grip and push force-recall performance. Int. J. Ind. Ergon. 2007, 37, 257–266. [Google Scholar] [CrossRef]
- Gillmeister, F.; Schenk, T.; Melzig-Thiel, R. A personal dosimeter for daily vibration exposure. In Proceedings of the 9th International Conference on Hand-Arm Vibration, Nancy, France, 5–8 June 2001; pp. 55–62. [Google Scholar]
- Pyykkö, I.; Färkkilä, M.; Toivanen, J.; Korhonen, O.; Hyvärinen, J. Transmission of vibration in the hand-arm system with special reference to changes in compression force and acceleration. Scand. J. Work Environ. Health 1976, 2, 87–95. [Google Scholar] [CrossRef]
- Reynolds, D.; Angevine, E.N. Hand-arm vibration, part II: Vibration transmission characteristics of the hand and arm. J. Sound Vib. 1977, 51, 255–256. [Google Scholar] [CrossRef]
- Paddan, G.S.; Griffin, M.J. Measurement of glove and hand dynamics using knuckle vibration. In Proceedings of the 9th International Conference on Hand-Arm Vibration, Nancy, France, 5–8 June 2001. [Google Scholar]
- Welcome, D.E.; Dong, R.G.; Xu, X.S.; Warren, C.; McDowell, T.W. Tool-specific performance of vibration-reducing gloves for attenuating fingers-transmitted vibration. Occup. Erg. 2016, 13, 23–44. [Google Scholar] [CrossRef]
- Dong, R.G.; McDowell, T.W.; Welcome, D.E. Biodynamic response at the palm of the human hand subjected to a random vibration. Ind. Health 2005, 43, 241–255. [Google Scholar] [CrossRef][Green Version]
- Dong, R.G.; Schopper, A.W.; McDowell, T.W.; Welcome, D.E.; Wu, J.Z.; Smutz, W.P.; Warren, C.; Rakheja, S. Vibration energy absorption (VEA) in human fingers-hand-arm system. Med. Eng. Phys. 2004, 26, 483–492. [Google Scholar] [CrossRef]
- Dong, R.G.; McDowell, T.W.; Welcome, D.E.; Wu, J.Z. Biodynamic response of human fingers in a power grip subjected to a random vibration. J. Biomech. Eng. 2004, 126, 447–457. [Google Scholar] [CrossRef]
- Dong, R.G.; Wu, J.Z.; McDowell, T.W.; Welcome, D.E.; Schopper, A.W. Distribution of mechanical impedance at the fingers and the palm of the human hand. J. Biomech. 2005, 38, 1165–1175. [Google Scholar] [CrossRef]
- Xu, X.S.; Welcome, D.E.; McDowell, T.W.; Wu, J.Z.; Wimer, B.; Warren, C.; Dong, R.G. The vibration transmissibility and driving-point biodynamic response of the hand exposed to vibration normal to the palm. Int. J. Ind. Ergon. 2011, 41, 418–427. [Google Scholar] [CrossRef]
- Xu, X.S.; Dong, R.G.; Welcome, D.E.; Warren, C.; McDowell, T.W.; Wu, J.Z. Vibrations transmitted from human hands to upper arm, shoulder, back, neck, and head. Int. J. Ind. Erg. 2017, 62, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.S.; Welcome, D.E.; Warren, C.; McDowell, T.W.; Dong, R.G. An evaluation of experimental methods for measuring the vibration transmissibility of vibration-reducing gloves at or on the fingers. In Proceedings of the 14th International Conference on Hand-Arm-Vibration, Bonn, Germany, 21–24 May 2019. [Google Scholar]
- Rakheja, S.; Wu, J.Z.; Dong, R.G.; Schopper, A.W. A comparison of biodynamic models of the human hand-arm system for applications to hand-held power tools. J. Sound Vib. 2002, 249, 55–82. [Google Scholar] [CrossRef]
- Dong, R.G.; Dong, J.H.; Wu, J.Z.; Rakheja, S. Modeling of biodynamic responses distributed at the fingers and the palm of the human hand-arm system. J. Biomech. 2007, 40, 2335–2340. [Google Scholar] [CrossRef] [PubMed]
- Dong, R.G.; Welcome, D.E.; McDowell, T.W.; Wu, J.Z. Theoretical relationship between vibration transmissibility and driving-point response functions of the human body. J. Sound Vib. 2013, 332, 6193–6202. [Google Scholar] [CrossRef][Green Version]
- Dong, R.G.; Welcome, D.E.; McDowell, T.W.; Wu, J.Z. Theoretical foundation, methods, and criteria for calibrating human vibration models using frequency response functions. J. Sound Vib. 2015, 356, 195–216. [Google Scholar] [CrossRef]
- Dong, R.G.; Welcome, D.E.; McDowell, T.W.; Wu, J.Z. Modeling of the biodynamic responses distributed at the fingers and palm of the hand in three orthogonal directions. J. Sound Vib. 2013, 232, 1125–1140. [Google Scholar] [CrossRef]
- Dong, J.H.; Dong, R.G.; Rakheja, S.; Welcome, D.E.; McDowell, T.W.; Wu, J.Z. A method for analyzing absorbed power distribution in the hand and arm substructures when operating vibrating tools. J. Sound Vib. 2008, 311, 1286–1304. [Google Scholar] [CrossRef]
- Dong, R.G.; Welcome, D.E.; McDowell, T.W.; Wu, J.Z. Methods for deriving representative biodynamic response of hand-arm system to vibration. J. Sound Vib. 2009, 325, 1047–1061. [Google Scholar] [CrossRef]
- Dong, R.G.; Xu, X.S.; Welcome, D.E.; McDowell, T.W. A method for analyzing the effectiveness of vibration-reducing gloves based on vibration power absorption. Vibration 2021, 4, 2. [Google Scholar] [CrossRef]
- Dong, R.G.; Welcome, D.E.; Xu, X.S.; Chen, Q.; Lin, H.; McDowell, T.W.; Wu, J.Z. A model for simulating vibration responses of grinding machine-workpiece-hand-arm systems. J. Sound Vib. 2018, 431, 276–294. [Google Scholar] [CrossRef]
- Dong, R.G.; Welcome, D.E.; Xu, S.X.; McDowell, T.W. Identification of effective engineering methods for controlling handheld workpiece vibration in grinding processes. Int. J. Ind. Ergon. 2020, 77, 102946. [Google Scholar] [CrossRef]
- Dong, R.G.; Welcome, D.E.; Wu, J.Z.; McDowell, T.W. Development of hand-arm system models for vibrating tool analysis and test rig construction. Noise Control Eng. J. 2008, 56, 35–44. [Google Scholar] [CrossRef]
- Wilson, C.E. Measurement problems associated with the study of segmental vibration. In Proceedings of the International Occupational Hand-Arm Vibration Conference, Cincinnati, OH, USA, October 1975. [Google Scholar]
- Maeda, S.; Ye, Y. Review of necessary risk assessment equipment for prevention of hand-arm vibration syndrome. In Proceedings of the 8th American Conference on Human Vibration, Morgantown, WV, USA, 23–25 June 2021. [Google Scholar]
- Dong, R.G.; Welcome, D.E.; Wu, J.Z. Estimation of biodynamic forces distributed on the fingers and the palm exposed to vibration. Ind. Health 2005, 43, 485–494. [Google Scholar] [CrossRef]
- Dong, R.G.; Welcome, D.E.; Wu, J.Z. A method to quantify hand-transmitted vibration exposure based on the biodynamic stress concept. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2007, 221, 847–861. [Google Scholar] [CrossRef]
- Cundiff, J.S. Energy dissipation in human hand-arm exposed to random vibration. J. Acoust. Soc. Am. 1976, 59, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Lidström, I.M. Vibration injury in rock drillers, chiselers, and grinders. Some views on the relationship between the quantity of energy absorbed and the risk of occurrence of vibration injury. In Proceedings of the International Conference on Hand-Arm Vibration, Cincinnati, OH, USA, January, 1977; NIOSH: Cincinnati, OH, USA, 1977; pp. 77–83. [Google Scholar]
- Reynolds, D.D.; Wasserman, D.E.; Basel, R.; Taylor, W. Energy entering the hands of operators of pneumatic tools used in chipping and grinding operations. In Vibration Effects on the Hand and Arm in Industry; Brammer, A.J., Taylor, W., Eds.; John Wiley & Sons: New York, NY, USA, 1982; pp. 133–146. [Google Scholar]
- Burström, L.; Lundström, R. Absorption of vibration energy in the human hand and arm. Ergonomics 1994, 37, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Sörensson, A. Energy absorption and transmission in the hand and arm during high frequency vibration and impact. In Department of Human Work Sciences, Division of Environmental Technology; National Institute of Working Life: Umea, Sweden, 1998. [Google Scholar]
- Dong, R.G.; Welcome, D.E.; McDowell, T.W.; Wu, J.Z.; Schopper, A.W. Frequency weighting derived from power absorption of fingers-hand-arm system under zh-axis vibration. J. Biomech. 2006, 39, 2311–2324. [Google Scholar] [CrossRef] [PubMed]
- Dong, R.G.; Wu, J.Z.; Welcome, D.E.; McDowell, T.W. A discussion on comparing alternative vibration measures with frequency-weighted accelerations defined in ISO standards. J. Sound Vib. 2008, 317, 1042–1050. [Google Scholar] [CrossRef]
- Miwa, T. Evaluation methods for vibration effect: Part 3. Measurements of threshold and equal sensation contours on hand for vertical and horizontal sinusoidal vibrations. Ind. Health 1967, 5, 213–220. [Google Scholar] [CrossRef]
- Miwa, T. Evaluation methods for vibration effect: Part 6. Measurements of unpleasant and tolerance limit levels for sinusoidal vibrations. Ind. Health 1968, 6, 18–27. [Google Scholar] [CrossRef]
- Brammer, A.J. Relations between vibration exposure and the development of the vibration syndrome. In Vibration Effects on the Hand and Arm in Industry; Brammer, A.J., Taylor, W., Eds.; Wiley and Sons: New York, NY, USA, 1982; pp. 283–290. [Google Scholar]
- Griffin, M.J. Frequency-dependence of psychophysical and physiological responses to hand-transmitted vibration. Ind. Health 2012, 50, 354–369. [Google Scholar] [CrossRef]
- Reynolds, D.; Standlee, K.G.; Angevine, E.N. Hand-arm vibration, Part III: Subjective response characteristics of individuals to hand-induced vibration. J. Sound Vib. 1977, 51, 267–282. [Google Scholar] [CrossRef]
- Giacomin, J.; Shayaa, M.S.; Dormegnie, E.; Richard, L. Frequency weighting for the evaluation of steering wheel rotational vibration. Int. J. Ind. Ergon. 2004, 33, 527–541. [Google Scholar] [CrossRef]
- Morioka, M.; Griffin, M.J. Magnitude-dependence of equivalent comfort contours for fore-and-aft, lateral and vertical hand-transmitted vibration. J. Sound Vib. 2006, 295, 633–648. [Google Scholar] [CrossRef]
- McDowell, T.W.; Kashon, M.L.; Welcome, D.E.; Warren, C.; Dong, R.G. Relationships between psychometrics, exposure conditions, and vibration power absorption in the hand-arm system. In Proceedings of the 11th International Conference on Hand-Arm Vibration, Bologna, Italy, 3–7 June 2007. [Google Scholar]
- Xu, Z.; Ding, H.C.; Ding, M.P.; Lin, J.C.; Wang, H. A study of dose-effect relationship for vibration-induced white finger. In Proceedings of the 5th International Conference on Hand-Arm Vibration, Kanazawa, Japan, 23–26 May 1989. [Google Scholar]
- Tominaga, Y. The relationship between vibration exposure and symptoms of vibration syndrome. J. Sci. Labour. 1993, 69, 1–14. [Google Scholar]
- Tominaga, Y. New frequency weighting of hand-arm vibration. Ind. Health 2005, 43, 509–515. [Google Scholar] [CrossRef]
- Bovenzi, M.; Franzinelli, A.; Strambi, F. Prevalence of vibration-induced white finger and assessment of vibration exposure among travertine workers in Italy. Int. Arch. Occup. Environ. Health 1988, 61, 25–34. [Google Scholar] [CrossRef]
- Starck, J.; Jussi, P.; Ilmari, P. Physical characteristics of vibration in relation to vibration-induced white finger. Am. Ind. Hyg. Assoc. J. 1990, 51, 179–184. [Google Scholar] [CrossRef]
- Nilsson, T.; Burström, L.; Hagberg, M. Risk assessment of vibration exposure and white fingers among platers. Int. Arch. Occup. Environ. Health 1989, 61, 473–481. [Google Scholar] [CrossRef]
- Dandanell, R.; Engstrom, K. Vibration from riveting tools in the frequency range 6 Hz-10 MHz and Raynaud’s phenomenon. Scand. J. Work Environ. Health 1986, 12, 338–342. [Google Scholar] [CrossRef]
- Griffin, M.; Bovenzi, M.; Nelson, C.M. Dose-response patterns for vibration-induced white finger. Occup. Environ. Med. 2003, 60, 16–26. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO/TR, 18570: Mechanical Vibration—Measurement and Evaluation of Human Exposure to Hand-Transmitted Vibration—Supplementary Method for Assessing Risk of Vascular Disorder; International Organization for Standardization: Geneva, Switzerland, 2016. [Google Scholar]
- Dong, R.G.; Wu, J.Z.; Welcome, D.E.; McDowell, T.W. Estimation of vibration power absorption density in human fingers. J. Biomech. Eng. 2005, 127, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Welcome, D.E.; Dong, R.G.; Song, W.J.; Hayden, C. Time-Frequency Characterization of Hand-Transmitted, Impulsive Vibrations Using Analytic Wavelet Transform. J. Sound Vib. 2007, 308, 98–111. [Google Scholar] [CrossRef]
- Wu, J.Z.; Dong, R.G.; Rakheja, S.; Schopper, A.W. Simulation of mechanical responses of fingertip to dynamic loading. Med. Eng. Phys. 2002, 24, 253–264. [Google Scholar] [CrossRef]
- Wu, J.Z.; Dong, R.G.; Schopper, A.W.; Smutz, W.P. Analysis of skin deformation profiles during sinusoidal vibration of fingerpad. Ann. Biomed. Eng. 2003, 31, 867–878. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.Z.; Dong, R.G.; Smutz, W.P.; Rakheja, S. Dynamic interaction between a fingerpad and a flat surface: Experiments and analysis. Med. Eng. Phys. 2003, 25, 397–406. [Google Scholar] [CrossRef]
- Wu, J.Z.; Dong, R.G.; Smutz, W.P.; Schopper, A.W. Modeling of time-dependent force response of fingertip to dynamic loading. J. Biomech. 2003, 36, 383–392. [Google Scholar] [CrossRef]
- Wu, J.Z.; Dong, R.G.; Smutz, W.P. Effects of static compression on the vibration modes of a fingertip. J. Low Freq. Noise Vib. Act. Control 2003, 21, 229–243. [Google Scholar] [CrossRef]
- Wu, J.Z.; Krajnak, K.; Welcome, D.E.; Dong, R.G. Analysis of the biodynamic interaction between the fingertip and probe in the vibrotactile tests: The influences of the probe/fingertip contact orientation and static indentation. J. Biomech. 2009, 42, 116–124. [Google Scholar] [CrossRef]
- Wu, J.Z.; Welcome, D.E.; McDowell, T.W.; Xu, X.S.; Dong, R.G. Modeling of the interaction between grip force and vibration transmissibility of a finger. Med. Eng. Phys. 2017, 45, 61–70. [Google Scholar] [CrossRef]
- Lindsell, C.; Griffin, M. Thermal thresholds, vibrotactile thresholds and finger systolic blood pressures in dockyard workers exposed to hand-transmitted vibration. Int. Arch. Occup. Environ. Health 1999, 72, 377–386. [Google Scholar] [CrossRef]
- Liu, W.; Lipsitz, L.A.; Montero-Odasso, M.; Bean, J.; Kerrigan, D.C.; Collins, J.J. Noise-enhanced vibrotactile sensitivity in older adults, patients with stroke, and patients with diabetic neuropathy. Arch. Phys. Med. Rehabil. 2002, 83, 171–176. [Google Scholar] [CrossRef]
- Christensen, N.J. Vibratory perception and blood flow in the feet of diabetics. Acta Med. Scand. 1969, 185, 553–559. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO 13091-1: Mechanical Vibration—Vibrotactile Perception Thresholds for the Assessment of Nerve Dysfunction—Part 1: Methods of Measurement at the Fingertips; International Organization for Standardization: Geneva, Switzerland, 2001. [Google Scholar]
- Goodwin, A.W.; John, K.T.; Darian-Smith, I. Skin profiles during sinusoidal vibration of the fingerpad. Exp. Brain Res. 1989, 77, 79–86. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Standardization. ISO 13091-2: Mechanical Vibration-Vibrotactile Perception Thresholds for the Assessment of Nerve Dysfunction-Part 2: Analysis and Interpretation of Measurements at the Fingertips; International Organization for Standardization: Geneva, Switzerland, 2003. [Google Scholar]
- Morrissey, S.; Winn, F.; Bittner, A. Screening for carpal tunnel syndrome with vibration threshold testing. In Proceedings of the 4th Pan Pacific Conference on Occupational Ergonomics, Taipei, Taiwan, 11-13 November 1996; Ergonomics Society of Taiwan: Hsinchu, Taiwan, 1996. [Google Scholar]
- Wu, J.Z.; Dong, R.G.; Rakheja, S.; Schopper, A.W.; Smutz, W.P. A structural fingertip model for simulating the biomechanics of tactile sensation. Med. Eng. Phys. 2004, 26, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Perez, C.A.; Holzmann, C.A.; Jaeschke, H.E. Two-point vibrotactile discrimination related to parameters of pulse burst stimulus. Med. Biol. Eng. Comput. 2000, 38, 74–79. [Google Scholar] [CrossRef]
- Wu, J.Z.; Krajnak, K.; Welcome, D.E.; Dong, R.G. Analysis of the dynamic strains in a fingertip exposed to vibration: Correlation to the mechanical stimuli on mechanoreceptors. J. Biomech. 2006, 39, 2445–2456. [Google Scholar] [CrossRef]
- Wu, J.Z.; Krajnak, K.; Welcome, D.E.; Dong, R.G. Three-dimensional finite element simulations of the dynamic response of a fingertip to vibration. ASME J. Biomech. Eng. 2008, 130, 054501. [Google Scholar] [CrossRef]
- Lundström, R. Effects of local vibration transmitted from ultrasonic devices on vibro-tactile perception in the hands of therapists. Ergonomics 1985, 28, 793–803. [Google Scholar] [CrossRef]
- Lundström, R.; Lindmark, A. Effects of local vibration on tactile perception in the hands of dentists. J. Low Freq. Noise Vib. 1982, 1, 1–11. [Google Scholar] [CrossRef]
- Wu, J.Z.; Welcome, D.E.; Krajnak, K.; Dong, R.G. Finite element analysis of the penetrations of shear and normal vibrations into the soft tissues in a fingertip. Med. Eng. Phys. 2007, 29, 718–727. [Google Scholar] [CrossRef]
- Topp, K.; Boyd, B.S. Structure and biomechanics of peripheral nerves: Nerve responses to physical stresses and implications for physical therapist practice. Phys. Ther. 2006, 86, 92–109. [Google Scholar] [CrossRef]
- Maeda, S.; Griffin, M.J. Temporary threshold shifts in fingertip vibratory sensation from hand-transmitted vibration and repetitive shock. Br. J. Ind. Med. 1993, 50, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Harada, N.; Griffin, M.J. Factors influencing vibration sense thresholds used to assess occupational exposures to hand transmitted vibration. Br. J. Ind. Med. 1991, 48, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Aldien, Y.; Marcotte, P.; Rakheja, S.; Boileau, P.-E. Influence of hand-arm posture on biodynamic response of the human hand-arm exposed to zh-axis vibration. Int. J. Ind. Ergon. 2006, 36, 45–59. [Google Scholar] [CrossRef]
- Aldien, Y.; Marcotte, P.; Rakheja, S.; Boileau, P.-E. Mechanical impedance and absorbed power of hand-arm under xh-axis vibration and role of hand forces and posture. Ind. Health 2005, 43, 495–508. [Google Scholar] [CrossRef] [PubMed]
- Welcome, D.E.; Rakheja, S.; Dong, R.G.; Wu, J.Z.; Schopper, A.W. An investigation on the relationship between grip, push and contact forces applied to a tool handle. Int. J. Ind. Ergon. 2004, 34, 507–518. [Google Scholar] [CrossRef]
- Aldien, Y.; Welcome, D.E.; Rakheja, S.; Dong, R.G.; Boileau, P.-E. Contact pressure distribution at hand–handle interface: Role of hand forces and handle size. Int. J. Ind. Ergon. 2005, 35, 267–286. [Google Scholar] [CrossRef]
- Dong, R.G.; Wu, J.Z.; Welcome, D.E.; McDowell, T.W. A new approach to characterize grip force applied to a cylindrical handle. Med. Eng. Phys. 2008, 30, 20–33. [Google Scholar] [CrossRef] [PubMed]
- Wimer, B.; Dong, R.G.; Welcome, D.E.; Warren, C.; McDowell, T.W. Development of a new dynamometer for measuring grip strength applied on a cylindrical handle. Med. Eng. Phys. 2009, 31, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Wimer, B.; McDowell, T.W.; Xu, X.S.; Welcome, D.E.; Warren, C.; Dong, R.G. Effects of gloves on the total grip strength applied to cylindrical handles. Int. J. Ind. Ergon. 2010, 40, 574–583. [Google Scholar] [CrossRef]
- McDowell, T.W.; Wimer, B.; Welcome, D.E.; Warren, C.; Dong, R.G. Effects of handle size and shape on measured grip strength. Int. J. Ind. Ergon. 2012, 42, 199–205. [Google Scholar] [CrossRef]
- Dong, R.G.; McDowell, T.W.; Welcome, D.E.; Warren, C.; Schopper, A.W. An evaluation of the standardized chipping hammer test specified in ISO 8662-2. Ann. Occup. Hyg. 2004, 48, 39–49. [Google Scholar]
- McDowell, T.W.; Dong, R.G.; Xu, S.X.; Welcome, D.E.; Warren, C. An evaluation of impact wrench vibration emissions and test methods. Ann. Occup. Hyg. 2008, 52, 125–138. [Google Scholar]
- McDowell, T.W.; Marcotte, P.; Warren, C.; Welcome, D.E.; Dong, R.G. Comparing three methods for evaluating impact wrench vibration emissions. Ann. Occup. Hyg. 2009, 53, 617–626. [Google Scholar]
- McDowell, T.W.; Warren, C.; Xu, X.S.; Welcome, D.E.; Dong, R.G. Laboratory and field measurements and evaluations of vibration at the handles of riveting hammers. Ann. Occup. Hyg. 2012, 56, 911–924. [Google Scholar]
- McDowell, T.W.; Warren, C.; Xu, X.S.; Welcome, D.E.; Dong, R.G. Laboratory and workplace assessments of rivet bucking bar vibration emissions. Ann. Occup. Hyg. 2015, 59, 382–397. [Google Scholar] [PubMed]
- McDowell, T.W.; Welcome, D.; Warren, C.; Xu, X.; Dong, R.G. Assessment of hand-transmitted vibration exposure from motorized forks used for beach-cleaning operations. Ann. Occup. Hyg. 2013, 57, 43–53. [Google Scholar] [PubMed]
- McDowell, T.W.; Welcome, D.E.; Warren, C.; Xu, X.S.; Dong, R.G. The effect of a mechanical arm system on portable grinder vibration emissions. Ann. Occup. Hyg. 2016, 60, 371–386. [Google Scholar] [CrossRef] [PubMed]
- McDowell, T.W.; Xu, X.S.; Warren, C.; Welcome, D.E.; Dong, R.G. The effects of feed force on rivet bucking bar vibrations. Int. J. Ind. Erg. 2018, 67, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Geiger, M.; Ster, J. Aerospace Standard 6228 developed to support improved productivity and reduce occupational disease among powered hand tool operators. SAE Int. J. Mater. Manf. 2016, 9, 1–11. [Google Scholar] [CrossRef]
- The Society of Automotive Engineers (SAE) International. AS 6228: Safety Requirements for Procurement, Maintenance and Use of Hand-Held Powered Tools; The Society of Automotive Engineers (SAE) International: Warrendale, PA, USA, 2014. [Google Scholar]
- McKenna, K.M.; McGrann, S.; Blann, A.D.; Allen, J.A. An investigation into the acute vascular effects of riveting. Br. J. Ind. Med. 1993, 50, 160–166. [Google Scholar] [CrossRef][Green Version]
- Engstrom, K.; Dandanell, R. Exposure conditions and Raynaud’s phenomenon among riveters in the aircraft industry. Scand. J. Work Environ. Health 1986, 12, 293–295. [Google Scholar] [CrossRef]
- Dong, R.G.; Rakheja, S.; Smutz, W.P.; Schopper, A.W.; Wu, J.Z. Effectiveness of a new method (TEAT) to assess vibration transmissibility of gloves. Int. J. Ind. Ergon. 2002, 30, 33–48. [Google Scholar] [CrossRef]
- Smutz, W.P.; Dong, R.G.; Han, B.; Schopper, A.W.; Welcome, D.E.; Kashon, M. A method for reducing adaptor misalignment when testing gloves using ISO 10819. Ann. Occup. Hyg. 2002, 46, 309–315. [Google Scholar] [PubMed]
- Dong, R.G.; Rakheja, S.; Smutz, W.P.; Schopper, A.W.; Caporali, S. Dynamic characterization of instrumented handle and palm-adapter used for assessment of vibration transmissibility of gloves. J. Test. Eval. 2003, 31, 234–246. [Google Scholar]
- Welcome, D.E.; Dong, R.G.; Xu, X.S.; Warren, C.; McDowell, T.W. An evaluation of the proposed revision of the anti-vibration glove test method defined in ISO 10819 (1996). Int. J. Ind. Ergon. 2012, 42, 143–155. [Google Scholar] [CrossRef]
- Dong, R.G.; McDowell, T.W.; Welcome, D.E.; Smutz, P.W.; Schopper, A.W. Correlations between biodynamic characteristics of human hand-arm system and the isolation effectiveness of antivibration gloves. Int. J. Ind. Ergon. 2005, 35, 205–216. [Google Scholar] [CrossRef]
- Dong, R.G.; Rakheja, S.; McDowell, T.W.; Welcome, D.E.; Wu, J.Z.; Warren, C.; Barkley, J.; Washington, B.; Schopper, A.W. A method for assessing the effectiveness of anti-vibration gloves using biodynamic responses of the hand-arm system. J. Sound Vib. 2005, 282, 1101–1118. [Google Scholar] [CrossRef]
- Xu, S.X.; Welcome, D.E.; McDowell, T.W.; Warren, C.; Service, S.; Lin, H.S.; Chen, Q.S.; Dong, R.G. An investigation of the effectiveness of vibration-reducing gloves for controlling vibration exposures during grinding handheld workpieces. Appl. Ergon. 2021, 95, 103454, in press. [Google Scholar] [CrossRef]
- Wu, J.Z.; Wimer, B.; Welcome, D.E.; Dong, R.G. An analysis of contact stiffness between a finger and an object when wearing an air-cushioned glove: The effects of the air pressure. Med Eng. Phys. 2012, 34, 386–393. [Google Scholar] [CrossRef]
- Dong, R.G.; McDowell, T.W.; Welcome, D.E.; Barkley, J.; Warren, C.; Washington, B. Effects of hand-tool coupling conditions on the isolation effectiveness of air bladder anti-vibration gloves. J. Low Freq. Noise Vib. Act. Control 2004, 23, 231–248. [Google Scholar] [CrossRef]
- Dong, R.G.; Welcome, D.E.; Peterson, D.R.; Xu, X.S.; McDowell, T.W.; Warren, C.; Asaki, T.; Kudernatsch, S.; Brammer, A. Tool-specific performance of vibration-reducing gloves for attenuating palm-transmitted vibrations in three orthogonal directions. Int. J. Ind. Ergon. 2014, 44, 827–839. [Google Scholar] [CrossRef]
- Rakheja, S.; Dong, R.G.; Welcome, D.E.; Schopper, A.W. Estimation of tool-specific isolation performance of antivibration gloves. Int. J. Ind. Ergon. 2002, 30, 71–87. [Google Scholar] [CrossRef]
- Xu, X.S.; Riley, D.A.; Persson, M.; Welcome, D.E.; Krajnak, K.; Wu, J.Z.; Govindaraju, S.R.; Dong, R.G. Evaluation of anti-vibration effectiveness of glove materials using an animal model. Bio. Med. Mater. Eng. 2011, 21, 193–211. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.S.; Welcome, E.; Warren, C.; McDowell, T.W.; Dong, R.G. Identification of additional effects of vibration-reducing gloves other than cushioning functions on finger vibration responses. In Proceedings of the 8th American Conference on Human Vibration, Morgantown, VW, USA, 23–25 June 2021. [Google Scholar]
- Dong, R.G.; Smutz, W.P.; Schopper, A.W.; Warren, C.; Wu, J.Z.; Rakheja, S. On-the-hand measurement methods for assessing effectiveness of anti-vibration gloves. Int. J. Ind. Ergon. 2003, 32, 283–298. [Google Scholar] [CrossRef]
- Chen, Q.; Lin, H.; Xiao, B.; Welcome, D.E.; Lee, J.; Chen, G.; Tang, S.; Zhang, D.; Xu, G.; Yan, M.; et al. Vibration characteristics of golf club heads in their handheld grinding process and potential approaches for reducing the vibration exposure. Int. J. Ind. Erg. 2017, 62, 27–41. [Google Scholar] [CrossRef]
- Xu, X.S.; Welcome, D.E.; McDowell, T.W.; Warren, C.; Lin, H.; Xiao., B.; Chen, Q.; Dong, R.G. Characterizing vibration responses of a handheld workpiece and the hand-arm system. J. Low Freq. Noise Vib. Act. Control 2020. [Google Scholar] [CrossRef]
- Bovenzi, M.; Petronio, L.; DiMarino, F. Epidemiological survey of Shipyard workers exposed to hand-arm vibration. Int. Arch. Occup. Environ. Health 1980, 46, 251–266. [Google Scholar] [CrossRef]
- Bovenzi, M. Finger systolic pressure during local cooling in normal subjects aged 20 to 60 years: Reference values for the assessment of digital vasospasm in Raynaud’s Phenomenon of occupational origin. Int. Arch. Occup. Environ. Health 1988, 61, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Giannini, F.; Rossi, S.; Passero, S.; Bovenzi, M.; Cannavà, G.; Mancini, R.; Cioni, R.; Battistini, N. Multifocal neural conduction impairment in forestry workers exposed and not exposed to vibration. Clin. Neurophysiol. 1999, 110, 1276–1283. [Google Scholar] [CrossRef]
- Taylor, W. The hand-arm vibration syndrome (HAVS) secondary Raynaud’s phenomenon of occupational origin. Proc. R. Coll. Physicians Edinb. 1987, 19, 7–13. [Google Scholar]
- Nilsson, T.; Wahlström, J.; Burström, L. Hand-arm vibration and the risk of vascular and neurological diseases—A systematic review and meta-analysis. PLoS ONE 2017, 12, e0180795. [Google Scholar] [CrossRef]
- Wasserman, D.E.; Taylor, W. Lessons from Hand-Arm Vibration Syndrome Research. Am. J. Ind. Med. 1991, 19, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Mirbod, S.M.; Inaba, R.; Iwata, H. A study on the vibration-dose limit for Japanese workers exposed to hand-arm vibration. Ind. Health 1992, 30, 1–22. [Google Scholar] [CrossRef]
- Heaver, C.; Goonetilleke, K.S.; Ferguson, H.; Shiralkar, S. Hand-arm vibration syndrome: A common occupational hazard in industrialized countries. J. Hand Surg. 2011, 36E, 354–363. [Google Scholar] [CrossRef]
- Bongiovanni, L.G.; Hagbarth, K.-E.; Stjernberg, L. Prolonged muscle vibration reducing motor output in maximal voluntary contractions in man. J. Physiol. 1990, 423, 15–26. [Google Scholar] [CrossRef]
- Bovenzi, M.; Zadini, A.; Franzinelli, A.; Borgogni, F. Occupational musculoskeletal disorders in the neck and upper limbs of forestry workers exposed to hand arm vibration. Ergonomics 1991, 34, 547–562. [Google Scholar] [CrossRef]
- Kihlberg, S.; Kjellberg, A.; Lindbeck, L. Pneumatic tool torque reaction: Reaction forces, displacement, muscle activity and discomfort in the hand-arm system. Appl. Ergon. 1993, 24, 165–173. [Google Scholar] [CrossRef]
- Park, H.S.; Martin, B. Hand vibration exposure as a hazard factor for muscle tendon stress. Ergon. Man. Work 1993, 327–330. [Google Scholar]
- Gurram, R.; Rakheja, S.; Gouw, G.J.; Ma, S. Influence of power tool-related parameters on the response of finger flexor muscles. Int. Arch. Occup. Environ. Health 1995, 66, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Roquelaure, Y.; Ha, C.; Rouillon, C.; Fouquet, N.; Leclerc, A.; Descatha, A.; Touranchet, A.; Goldberg, M.; Imbernon, E. Risk factors for upper-extremity musculoskeletal disorders in the working population. Arthritis Care Res. 2009, 61, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- Widia, M.; Dawal, S.Z.M. The effect of vibration on muscle activity using electric drill. In Proceedings of the International Conference for Technical Postgraduates, Kuala Lumpur, Malaysia, 14–15 December 2009; IEEE: New York, NY, USA, 2009; pp. 82–86. [Google Scholar]
- Widia, M.; Dawal, S.Z.M. Investigation on upper limb muscle activity and grip strength during drilling task. In Proceedings of the IMECS 2010, Hong Kong, 17–19 March 2010; pp. 1953–1957. [Google Scholar]
- Cederlund, R.; Isacsson, A.; Lundborg, G. Hand function in workers with hand-arm vibration syndrome. J. Hand Ther. 1999, 12, 16–24. [Google Scholar] [CrossRef]
- Toibana, N.; Ishikawa, N.; Sakakibara, H. Measurement of manipulative dexterity in patients with hand-arm vibration syndrome. Int. Arch. Occup. Environ. Health 2002, 75, 106–110. [Google Scholar] [CrossRef]
- McGeoch, K.L.; Gilmour, W.H.; Taylor, W. Sensorineural objective tests in the assessment of hand-arm vibration syndrome. Occup. Environ. Med. 1994, 51, 57–61. [Google Scholar] [CrossRef]
- Pelmear, P.L.; Taylor, W. Hand-arm vibration syndrome. J. Fam. Pract. 1994, 38, 180–185. [Google Scholar] [CrossRef][Green Version]
- Pelmear, P.L.; Taylor, W. Carpal tunnel syndrome and hand-arm vibration syndrome. A diagnostic enigma. Arch. Neurol. 1994, 51, 416–420. [Google Scholar] [CrossRef]
- Flodmark, B.T.; Lundborg, G. Vibrotactile sense and hand symptoms in blue collar workers in a manufacturing industry. Occup. Environ. Med. 1997, 54, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Josty, I.C.; Tyler, M.P.; Shewell, P.C.; Roberts, A.H. Grip and pinch strength variations in different types of workers. J. Hand Surg. 1997, 22, 266–269. [Google Scholar] [CrossRef]
- Tanaka, M.; Nakamura, K.; Sato, K.; Tanaka, K. Influence of local vibration on finger functions of forest workers. Ind. Health 1997, 35, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Neitzel, R.; Yost, M. Task-based assessment of occupational vibration and noise exposures in forestry workers. AIHA J. 2002, 63, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Qamruddin, A.A.; Husain, N.R.N.; Sidek, M.Y.; Hanafi, M.H.; Ripin, Z.M.; Ali, N. Prevalence of hand-arm vibration syndrome among tyre shop workers in Kelantan, Malaysia. J. Occup. Health 2019, 61, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Merkevicius, S.; Butkus, R.; Jotautiene, E.; Vasiliauskas, C. Prognostics of vibration induced risk to operators of agricultural machinery. J. Vibroeng. 2012, 14, 381–387. [Google Scholar]
- Tamrin, S.B.M.; Jamalohdin, M.N.; Ng, Y.G.; Maeda, S.; Al, N.A.M. The characteristics of vibrotactile perception threshold among shipyard workers in a tropical environment. Ind. Health 2012, 50, 156–163. [Google Scholar] [CrossRef]
- Bovenzi, M.; Lindsell, C.J.; Griffin, M.J. Acute vascular responses to the frequency of vibration transmitted to the hand. Occup. Environ. Med. 2000, 57, 422–430. [Google Scholar] [CrossRef]
- Bovenzi, M.; Lindsell, C.J.; Griffin, M.J. Response of finger circulation to energy equivalent combinations of magnitude and duration of vibration. Occup. Environ. Med. 2001, 58, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Pacurari, M.; Waugh, S.; Krajnak, K. Acute vibration induces peripheral nerve sensitization in a rat tail model: possible role of oxidative stress and inflammation. Neuroscience 2019, 398, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Raju, S.G.; Rogness, O.; Persson, M.; Bain, J.; Riley, D. Vibration from a riveting hammer causes severe nerve damage in the rat tail model. Muscle Nerve 2011, 44, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Loffredo, M.A.; Yan, J.G.; Kao, D.; Zhang, L.L.; Matloub, H.S.; Riley, D.A. Persistent reduction of conduction velocity and myelinated axon damage in vibrated rat tail nerves. Muscle Nerve 2009, 39, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Curry, B.D.; Govindaraju, S.R.; Bain, J.L.; Yan, J.G.; Matloub, H.S.; Riley, D.A. Evidence for frequency-dependent arterial damage in vibrated rat tails. Anat. Rec. Part A Discov. Mol. Cell. Evol. Biol. 2005, 284, 511–521. [Google Scholar] [CrossRef]
- Welcome, D.E.; Krajnak, K.; Kashon, M.L.; Dong, R.G. An investigation on the biodynamic foundation of a rat tail vibration model. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2008, 222, 1127–1141. [Google Scholar] [CrossRef] [PubMed]
- Krajnak, K.; Waugh, S.; Miller, G.R.; Johnson, C.; Kashon, M.L. Vascular responses to vibration are frequency dependent. Am. Conf. Hum. Vib. 2010, 52, 25–26. [Google Scholar]
- Takeuchi, T.; Futatsuka, M.; Imanishi, H.; Yamada, S. Pathological changes observed in the finger biopsy of patients with vibration-induced white finger. Scand. J Work Environ. Health 1986, 12, 280–283. [Google Scholar] [CrossRef]
- Krajnak, K.; Dong, R.G.; Flavahan, S.; Welcome, D.E.; Flavahan, N.A. Acute vibration increases alpha2C-adrenergic smooth muscle constriction and alters thermosensitivity of cutaneous arteries. J. Appl. Physiol. 2006, 100, 1230–1237. [Google Scholar] [CrossRef]
- Krajnak, K.; Waugh, S.; Miller, G.R.; Johnson, C. Recovery of vascular function after exposure to a single bout of segmental vibration. J. Toxicol. Environ. Health A 2014, 77, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Bovenzi, M. Epidemiological evidence for new frequency weightings of hand-transmitted vibration. Ind. Health 2012, 50, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, G.; Khan, F.; McLaren, M.; Belch, J.J. Endothelial activation and response in patients with hand arm vibration syndrome. Eur. J. Clin. Investig. 1999, 29, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Pitt, B.R.; Schwarz, M.; Woo, E.S.; Yee, E.; Wasserloos, K.; Tran, S.; Weng, W.; Mannix, R.J.; Watkins, S.A.; Tyurina, Y.Y.; et al. Overexpression of metallothionein decreases sensitivity of pulmonary endothelial cells to oxidant injury. Am. J. Physiol. Heart Circ. Physiol. 1997, 273, L856–L865. [Google Scholar] [CrossRef] [PubMed]
- Langille, B.L. Arterial remodeling: Relation to hemodynamics. Can. J. Physiol. Pharmacol. 1996, 74, 834–841. [Google Scholar] [CrossRef] [PubMed]
- Stoyneva, Z.; Lyapina, M.; Tzvetkov, D.; Vodenicharov, E. Current pathophysiological views on vibration-induced Raynaud’s phenomenon. Cardiovasc. Res. 2003, 57, 615–624. [Google Scholar] [CrossRef]
- Wohlin, M.; Helmersson, J.; Sundström, J.; Arnlöv, J.; Vessby, B.; Larsson, A.; Andrén, B.; Lind, L.; Basu, S. Both cyclooxygenase- and cytokine-mediated inflammation are associated with carotid intima-media thickness. Cytokine 2007, 38, 130–136. [Google Scholar] [CrossRef]
- Krajnak, K.; Miller, G.R.; Waugh, S.; Johnson, C.; Kashon, M.L. Characterization of frequency-dependent responses of the sensorineural system to repetitive vibration. J Occup. Environ. Med. 2012, 54, 1010–1016. [Google Scholar] [CrossRef]
- Krajnak, K.; Miller, G.R.; Waugh, S. Contact area affects frequency-dependent responses to vibration in the peripheral vascular and sensorineural systems. J. Toxicol. Environ. Health Part A 2018, 81, 6–19. [Google Scholar] [CrossRef]
- Richner, M.; Ulrichsen, M.; Elmegaard, S.L.; Dieu, R.; Pallesen, L.T.; Vaegter, C.B. Peripheral nerve injury modulates neurotrophin signaling in the peripheral and central nervous system. Mol. Neurobiol. 2014, 50, 945–970. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.-Y.; Tan, C.-H. TRP channels in nociception and pathological pain. In Advances in Experimental Medicine and Biology; Springer: Singapore, 2018. [Google Scholar]
- Frias, B.; Merighi, A. Capsaicin, Nociception and Pain. Molecules 2016, 21, 797. [Google Scholar] [CrossRef] [PubMed]
- Mason, H.J.; Poole, K.; Young, C. Exposure assessment in health assessments for hand-arm vibration syndrome. Occup. Med. 2011, 61, 374–376. [Google Scholar] [CrossRef]
- Pitts, P.M.; Mason, H.J.; Poole, K.A.; Young, C.E. Relative performance of frequency weighting Wh and candidates for alternative frequency weightings when used to predict the occurrence of hand-arm vibration induced injuries. Can. Acoust. 2011, 39, 96–97. [Google Scholar]
- Lundström, R. Neurological diagnosis--aspects of quantitative sensory testing methodology in relation to hand-arm vibration syndrome. Int. Arch. Occup. Environ. Health 2002, 75, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.; Andersen, M.; Mikkelsen, S.; Nielsen, S.L. Prognosis of vibration induced white finger: A follow up study. Occup. Environ. Med. 1995, 52, 110–115. [Google Scholar] [CrossRef]
- Krajnak, K.; Raju, S.G.; Miller, G.R.; Johnson, C.; Wauigh, S.; Kashon, M.L.; Riley, D.A. Long-term daily vibration exposure alters current perception threshold (CPT) sensitivity and myelinated axons in a rat-tail model of vibration-induced injury. J. Toxicol. Environ. Health A 2016, 79, 101–111. [Google Scholar] [CrossRef]
- House, R.; Krajnak, K.; Manno, M.; Lander, L. Current perception threshold and the HAVS Stockholm sensorineural sclare. Occup. Med. 2009, 59, 476–482. [Google Scholar] [CrossRef][Green Version]
- Shadiack, A.M.; Sun, Y.; Zigmond, R.E. Nerve growth factor antiserum induces axotomy-like changes in neuropeptide expression in intact sympathetic and sensory neurons. J. Neurosci. 2001, 21, 363–371. [Google Scholar] [CrossRef]
- Hill, R.G.; Oliver, K.R. Neuropeptide and kinin antagonists. Handb. Exp. Pharmacol. 2007, 177, 181–216. [Google Scholar]
- Goldsmith, P.C.; Molina, F.A.; Bunker, C.B.; Terenghi, G.; Leslie, T.A.; Fowler, C.J.; Polak, J.M.; Dowd, P.M. Cutaneous nerve fibre depletion in vibration white finger. J. R. Soc. Med. 1994, 87, 377–381. [Google Scholar]
- Hughes, J.M.; Wirth, O.; Krajnak, K.; Miller, R.; Flavahan, S.; Berkowitz, D.E.; Welcome, D.E.; Flavahan, N.A. Increased oxidant activity mediates vascular dysfunction in vibration injury. J. Pharmacol. Exp. Ther. 2009, 328, 223–230. [Google Scholar] [CrossRef]
- Jeyaraj, S.C.; Unger, N.T.; Eid, A.H.; Mitr, S.; EI-Dahdah, N.P.; Quilliam, L.A.; Flavahan, N.A.; Chotani, M.A. Cyclic AMP-Rap1A signaling activates RhoA to induce a2C adrenoreceptor translocation to the cell surface of microvascular smooth muscles. Am. J. Physiol. Cell Physiol. 2012, 303, C499–C511. [Google Scholar] [CrossRef]
- Ekenvall, L.; Lindblad, L.E.; Norbeck, O.; Etzell, B.M. alpha-Adrenoceptors and cold-induced vasoconstriction in human finger skin. Am. J. Physiol. Heart Circ. Physiol. 1988, 255, 1000–1003. [Google Scholar] [CrossRef]
- Xu, X.S.; Riley, D.A.; Persson, M.; Welcome, D.E.; Krajnak, K.; Govindaraju, S.; Dong, R.G. Experiments characterizing impact vibration for rat tail vibration exposure. In Proceedings of the 3rd American Conference on Human Vibration, Iowa City, IA, USA, 1–4 June 2010. [Google Scholar]
- Zimmerman, J.J.; Bain, J.W.L.; Wu, C.; Lindell, H.; Grétarsson, S.L.; Riley, D.A. Riveting hammer vibration damages mechanosensory nerve endings. J. Peripher. Nerv. Syst. 2020, 25, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Krajnak, K.; Waugh, S.; Johnson, C.; Miller, G.R.; Xu, X.S.; Warren, C.; Dong, R.G. The effects of impact vibration on peripheral blood vessels and nerves. Ind. Health 2013, 51, 572. [Google Scholar] [CrossRef][Green Version]
- Ramieri, G.; Stella, M.; Calcagni, M.; Cellino, G.; Panzica, C.G. An immunohistochemical study on cutaneous sensory receptors after chronic median nerve compression in man. Acta Anat. 1995, 152, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Pinto, I.; Stacchint, N.; Bovenzi, M.; Paddan, G.S.; Griffin, M.J. Protection effectiveness of anti-vibration gloves: Field evaluation and laboratory performance assessment. In Proceedings of the 9th International Conference on Hand-Arm Vibration, Nancy, France, 5–8 June 2001. [Google Scholar]
- Krajnak, K.; Waugh, W.; Johnson, C.; Miller, R.G.; Welcome, D.E.; Xu, X.S.; Warren, C.; Sarkisian, S.; Andrew, M.; Dong, R.G. Antivibration gloves: Effects on vascular and sensorineural function, an animal model. J. Toxicol. Environ. Health A 2015, 78, 571–582. [Google Scholar] [CrossRef] [PubMed]
- Pattnaik, S.; Banerjee, R.; Kim, J. Spatial resonance in a small artery excited by vibration input as a possible mechanism to cause hand-arm vascular disorders. J. Sound Vib. 2012, 331, 1951–1960. [Google Scholar] [CrossRef]
- Bovenzi, M. Cardiovascular-responses to autonomic stimuli in workers with vibration-induced white finger. Eur. J. Appl. Physiol. Occup. Physiol. 1989, 59, 199–208. [Google Scholar] [CrossRef]
- Harada, N.; Nakamoto, M.; Kohno, H.; Kondo, H.; Tanaka, M. Hormonal responses to cold exposure in subjects with vibration syndrome. Kurume Med. J. 1990, 37, S45–S52. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Maeda, K. Autonomic and peripheral nervous system dysfunction in workers exposed to hand-arm vibration: A study of R-R interval variability and distribution of nerve conduction velocities. Int. Arch. Occup. Environ. Health 1991, 63, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Sakakibara, H.; Luo, J.; Zhu, S.K.; Hirata, M.; Abe, M. Autonomic nervous activity during hand immersion in cold water in patients with vibration-induced white finger. Ind. Health 2002, 40, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Waugh, S.; Kashon, M.L.; Li, S.Q.; Miller, G.R.; Johnson, C.; Krajnak, K. Transcriptional pathways altered in response to vibration in a model of hand-arm vibration syndrome. J. Occup. Environ. Med. 2016, 58, 344–350. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bovenzi, M.; Prodi, A.; Mauro, M. A longitudinal study of neck and upper limb musculoskeletal disorders and alternative measures of vibration exposure. Int. Arch. Occup. Environ. Health 2016, 89, 923–933. [Google Scholar] [CrossRef]
- Bovenzi, M.; Ronchese, F.; Mauro, M. Follow-up study of vascular and sensory functions in vibration-exposed shipyard workers. Can. Acoust. 2011, 39, 14–15. [Google Scholar]
- Cherniack, M.; Brammer, A.J.; Lundstrom, R.; Meyer, J.D.; Morse, T.F.; Neely, G.; Nilsson, T.; Peterson, D.; Toppila, E.; Warren, N. The hand-arm vibration international consortium (HAVIC): Prospective studies on the relationship between power tool exposure and health effects. J. Occup. Environ. Med. 2007, 49, 289–301. [Google Scholar] [CrossRef]
- Sauni, R.; Pääkkönen, R.; Virtema, P.; Toppila, E.; Uitti, J. Dose-response relationship between exposure to hand-arm vibration and health effects among metalworkers. Ann. Occup. Hyg. 2009, 53, 55–62. [Google Scholar]
- Eng, A.; Mannetje, A.; McLean, D.; Ellison-Loschmann, L.; Cheng, S.; Pearce, N. Gender differences in occupational exposure patterns. Occup. Environ. Med. 2011, 68, 888–894. [Google Scholar] [CrossRef] [PubMed]
- Burström, L. The influence of individual factors on the absorption of vibration energy in the hand and arm. Cent. Eur. J. Public Health 1996, 4, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Harada, N.; Ueda, A.; Takegata, S. Prevalence of Raynaud’s phenomenon in Japanese males and females. J. Clin. Epidemiol. 1991, 44, 649–655. [Google Scholar] [CrossRef]
- Bailey, S.R.; Mitra, S.; Flavahan, S.; Flavahan, N.A. Reactive oxygen species from smooth muscle mitochondria initiate cold-induced constriction of cutaneous arteries. Am. J. Physiol. Heart Circ. Physiol. 2005, 289, H243–H250. [Google Scholar] [CrossRef] [PubMed]
- Seah, S.A.; Griffin, M.J. Normal values for thermotactile and vibrotactile thresholds in males and females. Int. Arch. Occup. Environ. Health 2008, 81, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Kurozawa, Y.; Nasu, Y.; Oshiro, H. Finger systolic blood pressure measurements after finger cooling. Using the laser-Doppler method for assessing vibration-induced white finger. J. Occup. Med. 1992, 34, 683–686. [Google Scholar]
- Kurozawa, Y.; Nasu, Y. Inhibited cold-induced vasodilatation in patients with vibration-induced white finger. Int. Angiol. 1996, 15, 47–49. [Google Scholar]
- Mirbod, S.M.; Yoshida, H.; Jamali, M.; Miyashita, K.; Takada, H.; Inaba, R.; Iwata, H. Finger skin temperature and laser-Doppler finger blood flow in subjects exposed to hand-arm vibration. Ind. Health 1998, 36, 171–178. [Google Scholar] [CrossRef]
- Bovenzi, M.; Griffin, M.J.; Ruffell, C.M. Acute effects of vibration on digital circulatory function in healthy men. Occup. Environ. Med. 1995, 52, 834–841. [Google Scholar] [CrossRef]
- Bovenzi, M.; Griffin, M.J. Haemodynamic changes in ipsilateral and contralateral fingers caused by acute exposures to hand transmitted vibration. Occup. Environ. Med. 1997, 54, 566–576. [Google Scholar] [CrossRef]
- Bovenzi, M.; Lindsell, C.J.; Griffin, M.J. Duration of acute exposures to vibration and finger circulation. Scand. J. Work Environ. Health 1998, 24, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Bovenzi, M.; Lindsell, C.J.; Griffin, M.J. Magnitude of acute exposures to vibration and finger circulation. Scand. J. Work Environ. Health 1999, 25, 278–284. [Google Scholar] [CrossRef]
- Lindsell, C.J.; Griffin, M.J. Interpretation of the finger skin temperature response to cold provocation. Int. Arch. Occup. Environ. Health 2001, 74, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.L.; Griffin, M.J. Effect of the magnitude and frequency of hand-transmitted vibration on finger blood flow during and after exposure to vibration. Int. Arch. Occup. Environ. Health 2009, 82, 1151–1162. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Griffin, M.J. Reductions in finger blood flow induced by low magnitude hand-transmitted vibration. Can. Acoust. 2011, 39, 56–57. [Google Scholar]
- Ye, Y.; Griffin, M.J. Effect of room temperature on tests for diagnosing vibration-induced white finger: finger rewarming times and finger systolic blood pressures. Int. Arch. Occup. Environ. Health 2017, 90, 527–538. [Google Scholar] [CrossRef]
- Maeda, S.; Griffin, M.J. A comparison of vibrotactile thresholds on the finger obtained with different equipment. Ergonomics 1994, 37, 1391–1406. [Google Scholar] [CrossRef] [PubMed]
- Maeda, S.; Morioka, M. Repeatability of vibrotactile threshold measurements on the finger obtained with different equipment. In Proceedings of the United Kingdom Informal Group Meeting on Human Response to Vibration, Shrivenham, UK, 18–20 September 1996. [Google Scholar]
- Maeda, S.; Yonekawa, Y.; Kanada, K.; Takahashi, Y. Vibrotactile TTS of fingertip vibratory sensation from hand-transmitted vibration having the same equal equivalent tool vibration levels according to the JIS B 4900 determination method. Ind. Health 1996, 34, 257–266. [Google Scholar] [CrossRef]
- Lander, L.; Lou, W.; House, R. Nerve conduction studies and current perception thresholds in workers assessed for hand-arm vibration syndrome. Occup. Med. 2007, 57, 284–289. [Google Scholar] [CrossRef][Green Version]
- Stromberg, T.; Dahlin, L.B.; Rosen, I.; Lundborg, G. Neurophysiological findings in vibration-exposed male workers. J. Hand Sur. 1999, 24, 203–209. [Google Scholar] [CrossRef]
- Sakakibara, H.; Hirata, M.; Hashiguchi, T.; Toibana, N.; Koshiyama, H.; Zhu, S.K.; Yamada, S. Digital nerve conduction velocity for evaluation of peripheral nerve impairments in vibration syndrome. Cent. Eur. J. Public Health 1995, 3, 52–53. [Google Scholar]
- Nilsson, T.; Hagberg, M.; Burström, L.; Kihlberg, S. Impaired nerve-conduction in the carpal-tunnel of platers and truck assemblers exposed to hand-arm vibration. Scand. J. Work Environ. Health 1994, 20, 189–199. [Google Scholar] [CrossRef][Green Version]
- Winn, F.J.; Biersner, R.J. Nerve conduction and vibration testing for occupationally-induced entrapment syndromes: A comparison of techniques. Adv. Ind. Ergon. Saf. 1994, 505–510. [Google Scholar]
- Hayward, R.A. Temporary threshold shifts in vibrotactile sensitivity: Effects of vibration duration, intensity, and frequency. In U.K. Informal Group Meeting on Human Response to Vibration; Heriot-Watt University: Edinburgh, UK, 1984. [Google Scholar]
- Ide, H.; Akimura, H.; Obata, S. Effect of skin temperature on vibrotactile sensitivity. Med. Biol. Eng. Comput. 1985, 23, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Hayward, R.A.; Griffin, M.J. Measures of vibrotactile sensitivity in persons exposed to hand-arm vibration. Scand. J. Work Environ. Health 1986, 12, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Lundström, R.; Nilsson, T.; Burström, L.; Hagberg, M. Vibrotactile Perception Sensitivity and its Relation to Hand-Arm Vibration Exposure. Central Eur. J. Public Health 1995, 3, 62–65. [Google Scholar]
- Wenemark, M.; Lundström, R.; Hagberg, M.; Nilsson, T. Vibrotactile perception thresholds as determined by two different devices in a working population. Scand. J. Work Environ. Health 1996, 22, 204–210. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lundström, R.; Nilsson, T.; Burström, L.; Hagberg, M. Exposure-Response Relationship between Hand-Arm Vibration and Vibrotactile Perception Sensitivity. Am. J. Ind. Med. 1999, 35, 456–464. [Google Scholar] [CrossRef]
- Dick, R.B.; Steenland, K.; Krieg, E.F.; Hines, C.J. Evaluation of acute sensory--motor effects and test sensitivity using termiticide workers exposed to chlorpyrifos. Neurotoxicol. Teratol. 2001, 23, 381–393. [Google Scholar] [CrossRef]
- Poole, C.J.M.; Robinson, E.W.; Frost, G. Sensory perception testing by monofilaments in the digits of controls and workers with HAVS. Int. Arch. Occup. Environ. Health 2020, 93, 723–731. [Google Scholar] [CrossRef]
- Gerhardsson, L.; Burström, L.; Hagberg, M.; Lundström, R.; Nilsson, T. Quantitative neurosensory findings, symptoms and signs in young vibration exposed workers. J. Occup. Med. Toxicol. 2013, 8, 8. [Google Scholar] [CrossRef]
- Broadwell, D.K.; Darcey, D.J.; Hudnell, H.K.; Otto, D.A.; Boyes, W.K. Work-site clinical and neurobehavioral assessment of solvent-exposed microelectronics workers. Am. J. Ind. Med. 1995, 27, 677–698. [Google Scholar] [CrossRef]
- Haward, B.M.; Griffin, M.J. Repeatability of grip strength and dexterity tests and the effects of age and gender. Int. Arch. Occup. Environ. Health 2002, 75, 111–119. [Google Scholar] [CrossRef]
- Alaranta, H.; Seppalainen, A.M. Neuropathy and the automatic analysis of electromyographic signals from vibration exposed workers. Scand. J. Work Environ. Health 1977, 3, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Cabecas, J.M.; Milho, R.J. Anti-vibration gloves and the forearm efforts during tools operations. Enterp. Work Innov. Stud. 2009, 5, 59–67. [Google Scholar]
- Casale, R.; Ring, H.; Rainoldi, A. High frequency vibration conditioning stimulation centrally reduces myoelectrical manifestation of fatigue in healthy subjects. J. Electromyogr. Kinesiol. 2009, 19, 998–1004. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, D.S.; Barwick, D.D.; Petrie, A. Exploratory electromyography in the study of vibration-induced white finger in rock drillers. Br. J. Ind. Med. 1982, 39, 89–97. [Google Scholar] [CrossRef]
- Hagg, G.M.; Milerad, E. Forearm extensor and flexor muscle exertion during simulated gripping work—An electromyographic study. Clin. Biomech. 1997, 12, 39–43. [Google Scholar] [CrossRef]
- Marzke, M.W.; Toth, N.; Schick, K.; Reece, S.; Steinberg, B.; Hunt, K.; An, K.N. EMG study of hand muscle recruitment during hard hammer percussion manufacture of oldowan tools. Am. J. Phys. Anthropol. 1998, 105, 315–332. [Google Scholar] [CrossRef]
- Chau, N.; Remy, E.; Petry, D.; Huguenin, P.; Bourgkard, E.; Andre, J.M. Asymmetry correction equations for hand volume, grip and pinch strengths in healthy working people. Eur. J. Epidemiol. 1998, 14, 71–77. [Google Scholar] [CrossRef]
- Chatterjee, S.; Bandyopadhyay, A. Effect of vibrating steering on grip strength in heavy vehicle drivers. J. Hum. Ergol. 1991, 20, 77–84. [Google Scholar]
- Marley, R.J.; Fernandez, J.E. Psychophysical frequency and sustained exertion at varying wrist postures for a drilling task. Ergonomics 1995, 38, 303–325. [Google Scholar] [CrossRef]
- Radhakrishnan, S.; Nagaravindra, M. Analysis of hand forces in health and disease during maximum isometric grasping of cylinders. Med. Biol. Eng. Comput. 1993, 31, 372–376. [Google Scholar] [CrossRef]
- Harada, N. Cold-stress tests involving finger skin temperature measurement for evaluation of vascular disorders in hand-arm vibration syndrome: Review of the literature. Int. Arch. Occup. Environ. Health 2002, 75, 14–19. [Google Scholar] [CrossRef]
- International Organization for Standardization. ISO/CD 14835-1: Mechanical Vibration and Shock—Cold Provocation Tests for the Assessment of Peripheral Vascular Function—Part 1: Measurement and Evaluation of Finger Skin Temperature; International Organization for Standardization: Geneva, Switzerland, 2002. [Google Scholar]
- Sakakibara, H.; Maeda, S.; Yonekawa, Y. Thermotactile threshold testing for the evaluation of sensory nerve function in vibration-exposed patients and workers. Int. Arch. Occup. Environ. Health 2002, 75, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Tomida, K.; Morioka, I.; Kaewboonchoo, O.; Yamamoto, H.; Miyai, N.; Ishii, N.; Miyashita, K. Evaluation of Finger Skin Temperature by cold provocation test for diagnosis of vibration induced white finger (VWF). Ind. Health 1998, 36, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Hahn, M.; Klyscz, T.; Bohnenberger, G.; Jünger, M. A new technique for controlling the finger skin temperature in microcirculatory research demonstrated in a local cold stress test in healthy controls and patients with Raynaud’s phenomenon. Int. J. Microcirc. Clin. Exp. 1996, 16, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Furuta, M.; Sakakibara, H.; Miyao, M.; Kondo, T.; Yamada, S. Effect of vibration frequency on finger blood flow. Int. Arch. Occup. Environ. Health 1991, 63, 221–224. [Google Scholar] [CrossRef]
- Okada, A.; Naito, M.; Ariizumi, M.; Inaba, R.E. Experimental studies on the effects of vibration and noise on sympathetic-nerve activity in skin. Eur. J. Appl. Physiol. Occup. Physiol. 1991, 62, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Krajnak, K.; Waugh, S.; Sarkisian, K. Can blood flow be used to monitor changes in peripheral vascular function that occur in response to segmental vibration exposure? J Occup. Environ. Med. 2019, 61, 162–167. [Google Scholar] [CrossRef]
- Mizeva, I.; Zharkikh, E.; Dremin, V.; Zherebtsov, E.; Makovik, I.; Potapova, E.; Dunaey, A. Spectral analysis of the blood flow in the foot microvascular bed during thermal testing in patients with diabetes mellitus. Microvasc. Res. 2018, 120, 13–20. [Google Scholar] [CrossRef]
- Kent, P.; Williams, G.; Kester, R. Altered sensitivity of digital blood flow to acute vibration in patients with vasospastic disease. J. Biomed. Eng. 1991, 13, 269–271. [Google Scholar] [CrossRef]
- Kent, P.J.; McNamara, J.; Mooney, E.; Gorey, T.; Fitzpatrick, J. The vascular surgical society of great britain and ireland: Prognosis of patients with vibration-induced white finger after cessation of occupational vibration exposure. Br. J. Surg. 1995, 82, 549. [Google Scholar]
- House, R.; Krajnak, K.; Jiang, D. Factors affecting finger and hand pain in workers with HAVS. Occup. Med. 2016, 66, 292–295. [Google Scholar] [CrossRef]
- Krajnak, K. Chronic vibration reduces thresholds of A-beta and A-delta nerve fibers in the rat tail. J. Pain 2007, 8, S9. [Google Scholar] [CrossRef]
- Kurozawa, Y.; Nasu, Y. Current perception thresholds in vibration-induced neuropathy. Arch Environ. Health 2001, 56, 254–256. [Google Scholar] [CrossRef]
- Krajnak, K.; Waugh, S.; Wirth, O.; Kashon, M.L. Acute vibration reduced Aβ nerve fiber sensitivity and alters gene expression in the ventral tail nerves of rats. Muscle Nerve 2007, 36, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Krajnak, K.; Riley, D.A.; Wu, J.Z.; McDowell, T.W.; Welcome, D.E.; Xu, X.S.; Dong, R.G. Frequency-dependent effects of vibration on physiological systems: experiments with animals and other human surrogates. Ind. Health 2012, 50, 343–353. [Google Scholar] [CrossRef]
- Krajnak, K.; Waugh, S. Systemic effects of segmental vibration in an animal model of hand-arm vibration syndrome. J. Occup. Environ. Med. 2018, 60, 886–895. [Google Scholar] [CrossRef]
- Brumfield, A.M.; Schopper, A.W. User Solution: Automated Instrumentation for the Assessment of Peripheral Vascular Function. Image Acquisition and Processing with LabVIEW; CRC Press: Boca Raton, FL, USA, 2003; pp. 189–193. [Google Scholar]
- Maeda, S.; Sakakibara, H. Thermotactile perception thresholds measurement conditions. Ind. Health 2002, 40, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, T. Quantitative thermal perception thresholds relative to exposure to vibration. Occup. Environ. Med. 2001, 58, 472–478. [Google Scholar] [CrossRef]
- Bovenzi, M.; Alessandro, G.; Vanoni, O. Changes over a workshift in aesthesiometric and vibrotactile perception thresholds of workers exposed to intermittent hand transmitted vibration from impact wrenches. Occup. Environ. Med. 1997, 54, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Smutz, W.P.; Schopper, A.W.; Welcome, D.E.; Dong, R.G.; Andrew, M.E. The effects of finger force and visual distractions on the measurement of thermal perception thresholds. In Proceedings of the 10th International Conference on Hand-Arm Vibration, Las Vegas, NV, USA, 7–11 June 2004. [Google Scholar]
- International Organization for Standardization. ISO 8662/29827 (Part 1 to Part 14): Hand-Held Portable Power Tools—Test Methods for Evaluation of Vibration Emission 1988–2019; International Organization for Standardization: Geneva, Switzerland, 2009. [Google Scholar]
- International Organization for Standardization. ISO 14835-2: Mechanical Vibration and Shock—Cold Provocation Tests for the Assessment of Peripheral Vascular Function—Part 2: Measurement and Evaluation of Finger Systolic Blood Pressure; International Organization for Standardization: Geneva, Switzerland, 2005. [Google Scholar]
- ACGIH. Threshold Limit Values (TLV) for Hand-Arm Vibration; The American Conference of Governmental Industrial Hygienists (ACGIH): Cincinnati, OH, USA, 2021. [Google Scholar]
















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, R.G.; Wu, J.Z.; Xu, X.S.; Welcome, D.E.; Krajnak, K. A Review of Hand–Arm Vibration Studies Conducted by US NIOSH since 2000. Vibration 2021, 4, 482-528. https://doi.org/10.3390/vibration4020030
Dong RG, Wu JZ, Xu XS, Welcome DE, Krajnak K. A Review of Hand–Arm Vibration Studies Conducted by US NIOSH since 2000. Vibration. 2021; 4(2):482-528. https://doi.org/10.3390/vibration4020030
Chicago/Turabian StyleDong, Ren G., John Z. Wu, Xueyan S. Xu, Daniel E. Welcome, and Kristine Krajnak. 2021. "A Review of Hand–Arm Vibration Studies Conducted by US NIOSH since 2000" Vibration 4, no. 2: 482-528. https://doi.org/10.3390/vibration4020030
APA StyleDong, R. G., Wu, J. Z., Xu, X. S., Welcome, D. E., & Krajnak, K. (2021). A Review of Hand–Arm Vibration Studies Conducted by US NIOSH since 2000. Vibration, 4(2), 482-528. https://doi.org/10.3390/vibration4020030