1. Introduction
Artificial intelligence (AI) harnesses computer systems to mimic human intelligence in problem solving and decision making. It encompasses various techniques, including machine learning (ML) and deep learning (DL) [
1]. Machine learning uses traditional methods like support vector machines, logistic regression, and decision-tree algorithms that use relatively smaller datasets [
2,
3]. Deep learning, on the other hand, is a subset of ML that uses artificial neural networks inspired by and imitating the functionality of the human brain [
4,
5,
6]. These networks, like convolutional neural networks (CNNs) and recurrent neural networks (RNNs), process information from vast amounts of data through layers of interconnected nodes, achieving high learning capabilities. AI’s impact is transforming numerous industries, including facial recognition [
7,
8], object detection [
9,
10], and autonomous vehicles [
11]. Now, AI developers are building powerful models for healthcare applications as well. Major companies are heavily invested in this field, tackling diverse medical challenges [
12,
13]. One exciting area is AI-powered arrhythmia detection [
14,
15]. Arrhythmia disrupts the heart’s rhythm, causing abnormalities in electrocardiogram (ECG) readings. Early detection and treatment are crucial to preventing potentially fatal consequences, as cardiovascular disease (CVD) remains a leading cause of mortality worldwide. A staggering 931,578 deaths in the United States alone were attributed to CVD in 2021, according to the American Heart Association’s 2024 report [
16]. These alarming figures highlight the widespread impact of the disease, with approximately 127.9 million American adults living with CVD conditions such as heart disease, stroke, and hypertension.
Traditionally, ECG tests rely on 12 electrodes placed on the body, which can be inconvenient for patients. Additionally, diagnosing arrhythmias from these traces requires skilled doctors due to the complexity of identifying subtle abnormalities. This poses a risk of misdiagnosis, potentially leading to serious complications. Fortunately, alternative solutions are emerging. Single-lead ECG sensors offer a more comfortable and accessible approach. The captured signal can be analyzed by trained AI models to diagnose various heart conditions. The integration of AI and single-lead ECG technology shows immense promise for improving arrhythmia detection and potentially saving lives.
Several studies have explored various approaches using the MIT-BIH and BIDMC datasets to predict arrhythmias and other heart conditions [
17,
18,
19,
20,
21]. Notably, convolutional neural networks (CNNs) have emerged as a preferred classification method [
22,
23,
24]. These studies demonstrate the effectiveness of CNNs in classifying irregular heartbeats and various ailments from one-dimensional (time series) and two-dimensional (image) data. A key advantage of CNNs is their ability to automatically learn features from the data, eliminating the need for pre-processing or manual feature extraction. This makes them versatile tools across diverse applications, including emotion detection [
25,
26], medical data analysis [
27,
28], and education [
29]. Researchers have proposed combining CNNs with long short-term memory (LSTM) networks (e.g., [
14,
15]). This approach leverages LSTMs’ ability to retain long-term dependencies within the data, potentially improving classification accuracy. Additionally, the same studies employed the fast Fourier transform (FFT) to extract relevant features from the ECG signals.
Traditional ECG diagnostic devices face several challenges, including limited accessibility due to their bulk and stationary nature, high costs for their purchase and maintenance, lack of portability, complexity requiring trained personnel for their operation and interpretation, and difficulties integrating the data with electronic health records (EHRs). In contrast, mobile ECG devices offer significant advantages. They are lightweight and portable, making them usable in various settings such as at home and while travelling, and they enhance accessibility, particularly in remote and underserved areas. These devices are more cost-effective and user-friendly, allowing patients to conduct self-monitoring with minimal training. Mobile ECG devices can transmit data to healthcare providers in real time, facilitating prompt diagnosis and intervention. With this in mind, we developed a mobile ECG device using deep learning algorithms, such as CNNs, for detecting heart diseases. This device can help patients make quick diagnoses without visiting medical facilities. The generated ECG signals, along with simple diagnoses and comments, can easily be downloaded and sent to medical staff for further evaluation if needed.
The rest of the paper is organized as follows:
Section 2 explains the data preparation and preprocessing steps. The proposed deep learning approach is addressed in
Section 3, while
Section 4 explains the details of the developed mobile ECG prototype and its dedicated website.
Section 5 presents the simulation and real-time implementations along with a discussion. The paper is concluded in
Section 6.
2. Materials and Methods
Data gathering and preparation are crucial steps in developing any AI model. This section outlines our data acquisition process and preprocessing techniques, including the identification of the total number of classes within the dataset. Signal processing, such as denoising using IIR filters, was applied. Finally, the data were divided into training and testing sets for subsequent model development.
2.1. Database Description
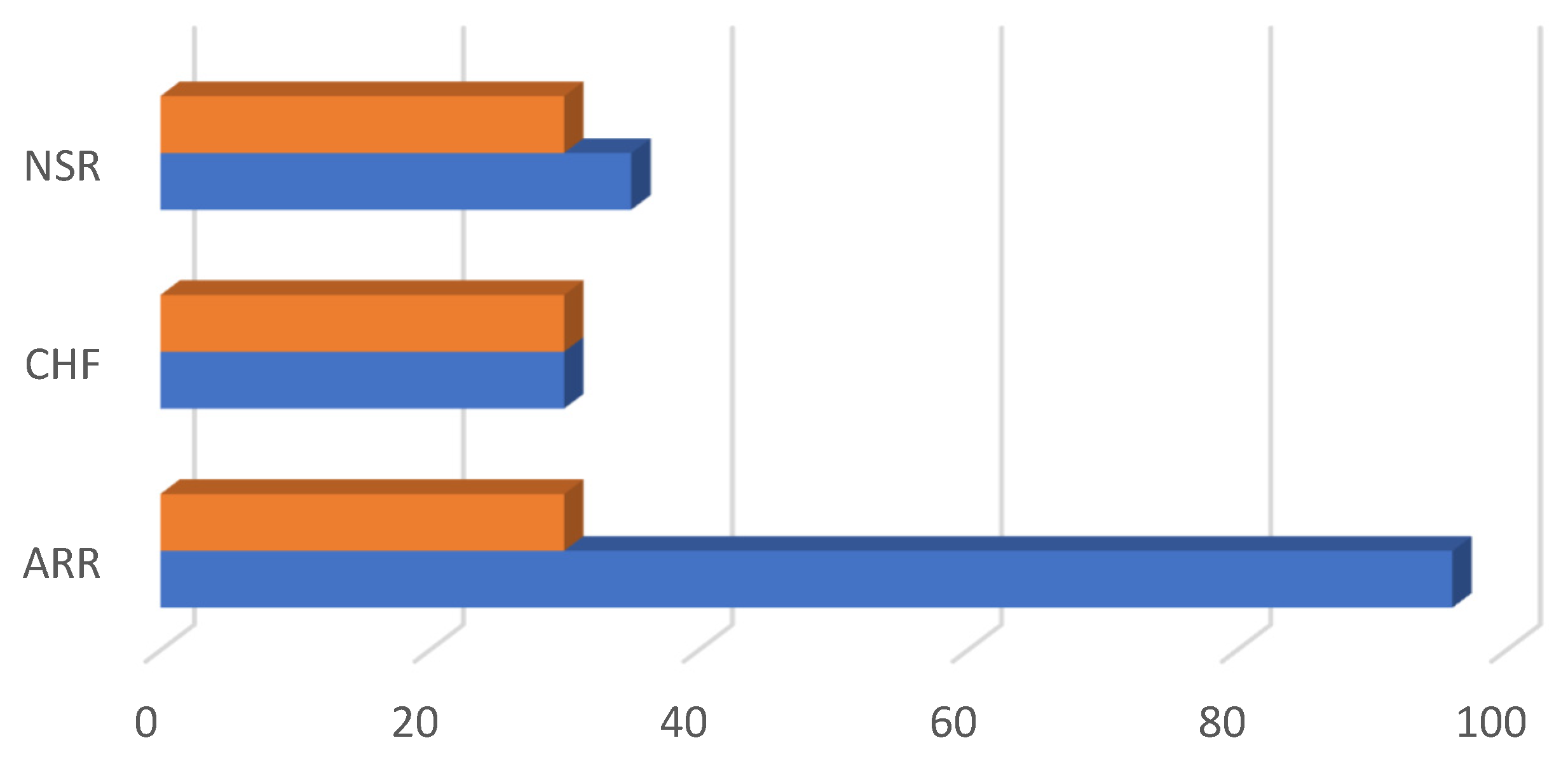
Reliable data are crucial for achieving robust performance. This study utilized two separate ECG databases from well-known PhysioNet resources, including MIT-BIH [
30] and BIDMC [
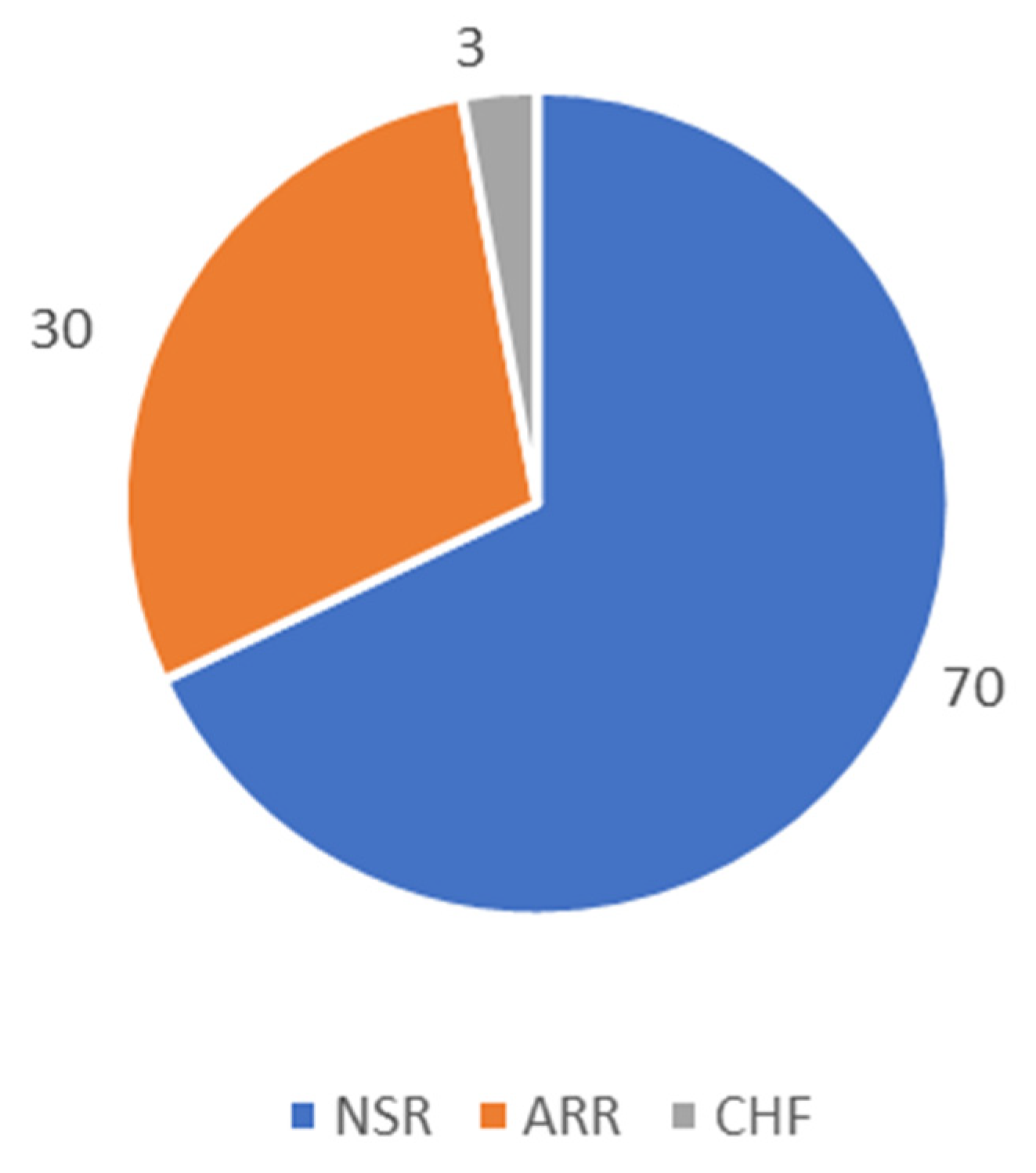
31]. The MIT-BIH database contains recordings of normal sinus rhythms (NSR) and arrhythmia (ARR), while BIDMC focuses on congestive heart failure (CHF). Originally, the data had 162 recordings (96 recordings for the ARR class, 30 recordings for the CHF class, and 36 recordings for the NSR class). To address the imbalance in the number of recordings across the different classes, we used 30 recordings for each class (NSR, ARR, and CHF), resulting in a total of 90 recordings for analysis (refer to
Figure 1). Additionally, we ensured that all recordings had a consistent sampling frequency
of 128 Hz.
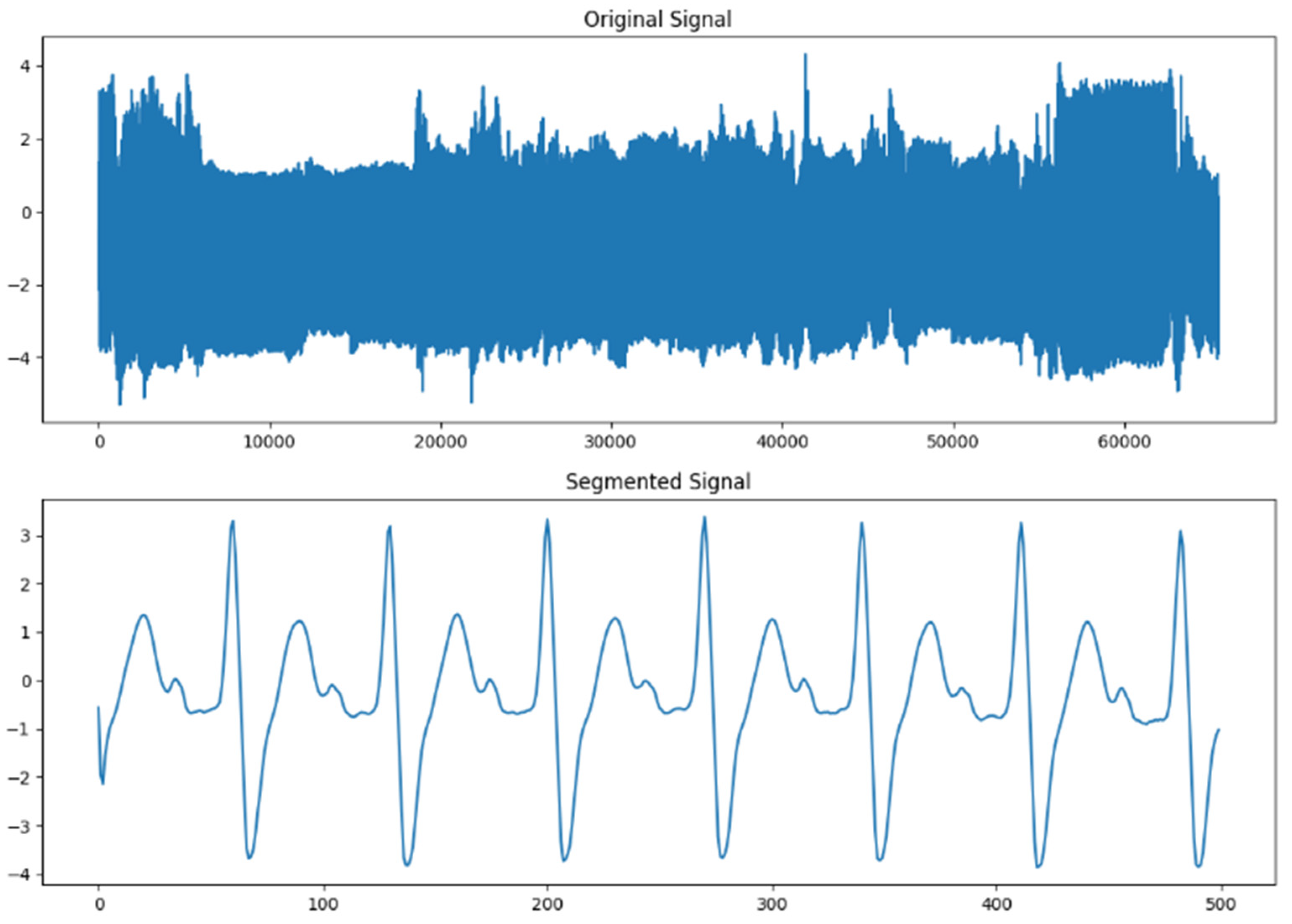
2.2. Signal Segmentation
To effectively analyze complex signals with many features, we employed signal segmentation. This method breaks down a huge signal into smaller, manageable pieces. In our case, each original ECG signal from the 90 recordings had a vast number of features (65,535 to be exact). Signal segmentation works by sliding a window of fixed size across the entire signal/recording. We set this window size to 500, meaning that each segmented piece would contain 500 specific features. This process transformed each original signal/recording into 131 segments, each with 500 features. As illustrated in
Figure 2, this segmentation significantly increased the dataset size from 90 recordings to 11,790 signals that represented the 3 classes. This expanded dataset allowed the model to learn from a wider variety of samples, potentially leading to improved performance.
2.3. Signal Denoising
ECG signals are susceptible to various noises, making accurate analysis challenging, even for experts. The original signal is corrupted by two main types of noise:
Low-frequency noise [
32]: This noise distorts the signal, making it difficult to interpret.
Baseline wander [
33]: This low-frequency noise causes the baseline of the signal to drift up and down, obscuring the heartbeats.
These noises can significantly impact prediction accuracy. To address this problem, we implemented two stages of infinite impulse response (IIR) Butterworth filters to remove noise and to improve the ECG signal for analysis. ECG signals are vulnerable to low-frequency noise from various sources. This noise can vary depending on the recording equipment and the patient’s condition. In our study, we identified a low-frequency noise range between 0.15 and 0.3 Hz. To eliminate this noise, we applied a Butterworth filter with a cut-off frequency of 0.39 Hz. This specific value effectively removed low-frequency artifacts without compromising the ECG waveform itself. Baseline wander is another type of low-frequency noise that causes the baseline of the signal to drift. This noise typically occurs above 1 Hz. To address this, we employed a 4th-order bandpass Butterworth filter. The order of 4 was chosen because it provides a good balance between reducing the noise and preserving the core ECG information. The specific cut-off frequencies for the bandpass filter were normalized as .
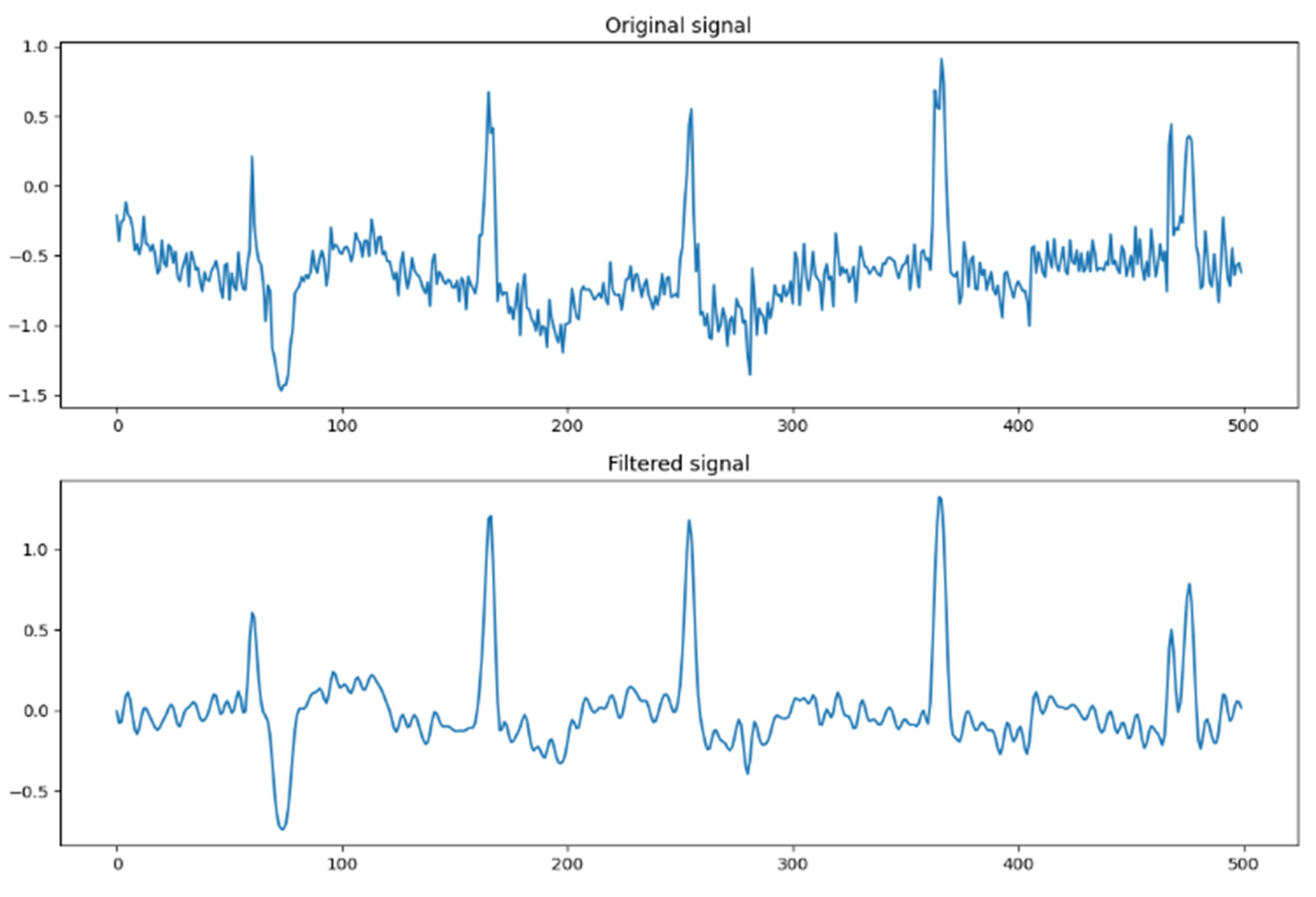
As depicted in
Figure 3, we could observe the transformation of the signal. The original signal was cluttered with noise, making it difficult to analyze the underlying ECG data. However, after applying the filters, the signal became significantly cleaner. The filters effectively removed unwanted artifacts, resulting in a signal that was much closer to the zero axis (zero crossing). This cleaner signal allowed for a more accurate analysis of the heart’s electrical activity.
2.4. Data Splitting
Data splitting is a crucial step in training AI models. It helps us to visualize and address potential imbalances in the number of samples for each class within the data. This imbalance can lead to biased patterns, where AI models can develop biases during training if one class has significantly more samples than others. This can be observed in applications like gender-biased face recognition systems [
34]. To prevent such biases, we divided our dataset (11,790 samples) into two sets, as illustrated in
Figure 4. Eighty percent of the data was allocated to the training set, which was used by the model to learn patterns from the data. The remaining 20% was used as the testing set, which helps to evaluate the model’s performance on unseen data. Furthermore, we employed a 5-fold cross-validation to obtain more robust results.
2.5. Evaluation Method
Many metrics can be used to evaluate the performance of the model using true positive (TP), true negative (TN), false positive (FP), and false negative (FN) values. One metric is the receiver operating characteristic (ROC) curve, which is a graph that shows how well a model can distinguish between positive and negative cases, considering different classification thresholds. Another metric is the area under the ROC curve (AUC), which is a single number that summarizes the overall performance of a model based on its ROC curve. A higher AUC indicates better classification ability. Other metrics used are accuracy, precision, sensitivity, specificity, and the F1-score, which can be defined as follows:
3. Proposed Approach
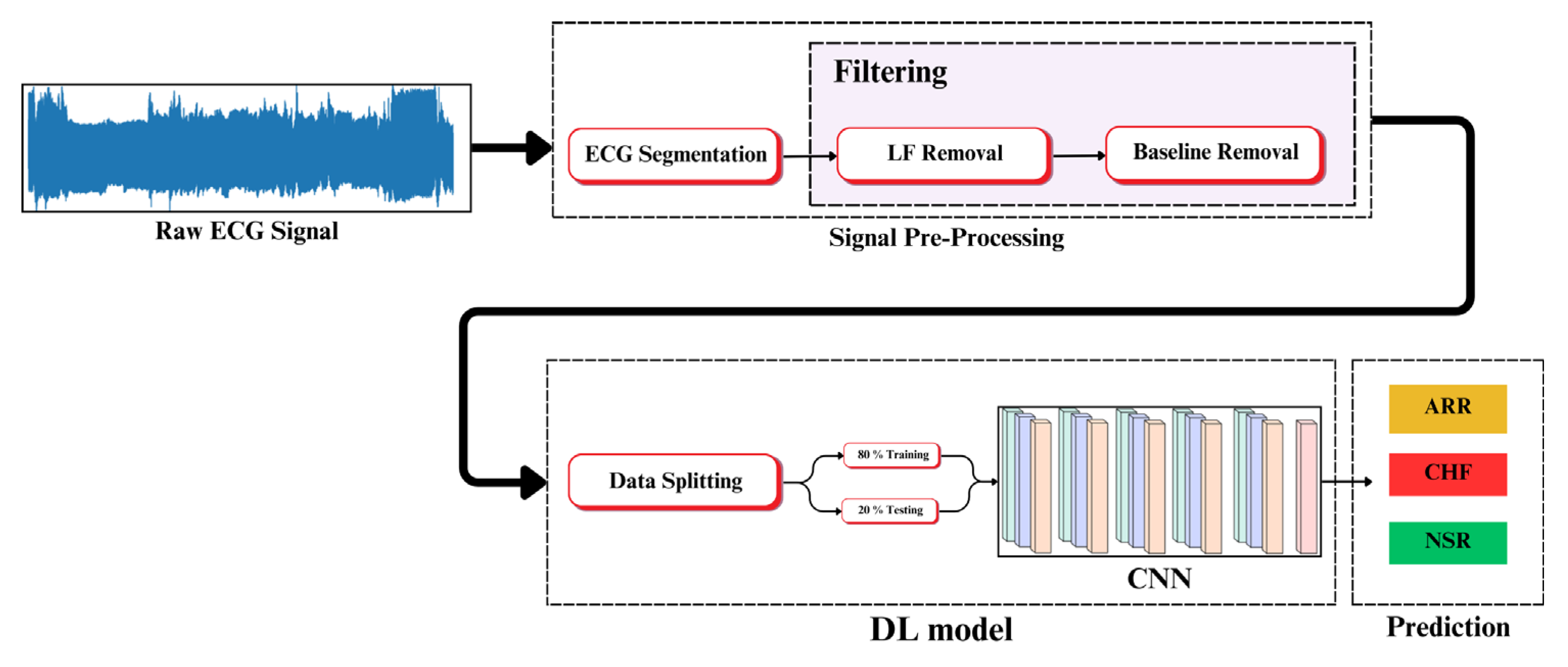
In this research, we proposed a real-time hardware implementation for ECG analysis using a deep learning model that employs a convolutional neural network (CNN) as the main classifier. The block diagram in
Figure 5 outlines the steps involved in our proposed approach. The initial signal preprocessing stage encompassed data segmentation/augmentation and noise removal. Subsequently, a deep learning (DL) model utilizing a convolutional neural network (CNN) was implemented. The final step involved predicting the correct class from the three available classes. The preprocessing stage is detailed in
Section 2, while the DL model is elaborated on in the following paragraphs.
3.1. Convolutional Neural Network
It is widely accepted that deep learning is a subfield of machine learning. Essentially, deep learning is a powerful tool within machine learning that is particularly effective for tackling complex problems with vast amounts of data. An automated classification system utilizing deep learning algorithms can significantly impact the system’s performance. Deep learning involves employing complex neural networks with numerous layers. These networks enable the system to learn diverse patterns from the input, which aids in making better decisions. Such an algorithm mimics the human brain’s functioning, as neurons transmit and process information from the environment. A convolutional neural network (CNN) is an example of a network used by deep learning algorithms for predicting and classifying different patterns across various problems [
35,
36,
37].
3.2. Model Architecture
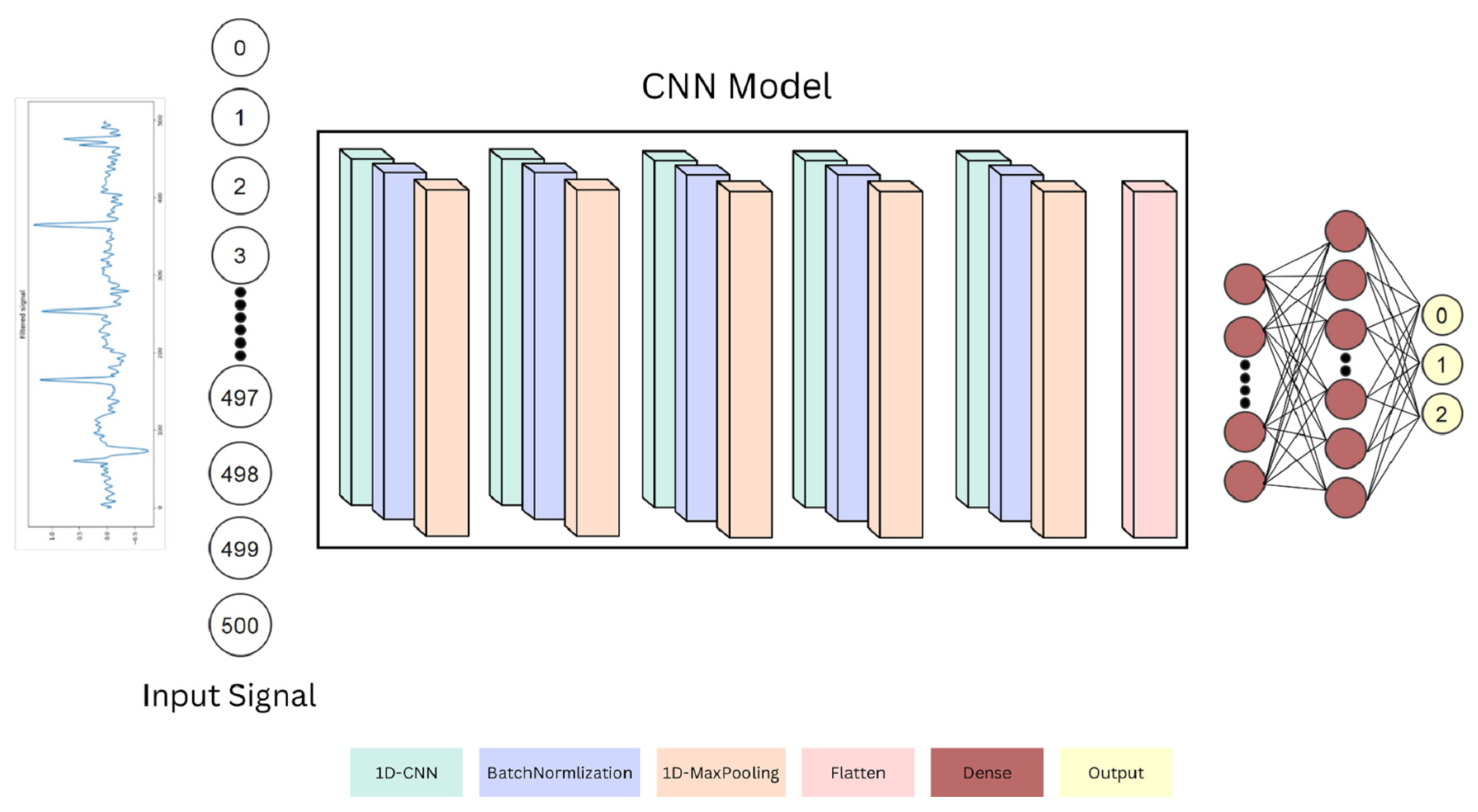
Figure 6 explains the structure of the proposed CNN model, which contains 8 layers divided into 5 CNN layers, 1 flatten layer, and 2 dense layers. Firstly, each CNN layer consists of 3 main components listed as the following: 1D CNN, batch normalization, and 1D max pooling. In the beginning, the ECG signal is passed to 500 neurons so that it can be transmitted to the other layers, and this layer is called the input signal layer. The 1D CNN is the layer that takes the input and performs the convolutional operations so that it extracts meaningful features. Next, these features are passed to a batch normalization layer that normalizes and simplifies the obtained features between 0 and 1. Finally, the features are passed to a max pooling layer, which has a kernel that locates the strongest features that have a bigger contribution (maximum values). This helps in dimensionality reduction by getting rid of unnecessary features. Thus, the same process continues through the rest of the 4 CNN layers. Moreover, the results are passed to a flatten layer that makes sure that the output of the features is a 1-dimensional column vector preparing it to be passed to the last 2 dense layers, which contain 2000 and 500 fully connected neurons, respectively, for pre-classification. Lastly, these neurons are connected to the output dense layer, which contains 3 neurons that represent the 3 target classes.
4. Prototype and Application
For this research, we employed an external ECG acquisition sensor to collect data in support of our heart disease prediction model. Additionally, we developed an application that allows users and physicians to directly upload ECG signals from the sensor to our system, enabling patients to monitor their heart health. The data acquisition mechanism and the mobile application details are explained below.
4.1. ECG Acquisition
The sensor module used in this research is called BITalino Core BT/BLE [
38]. This sensor is a portable biomedical sensor that allows ECG signals to be recorded and saved. This model is fitted with Bluetooth and/or Bluetooth Low Energy (BLE) communication. As illustrated in
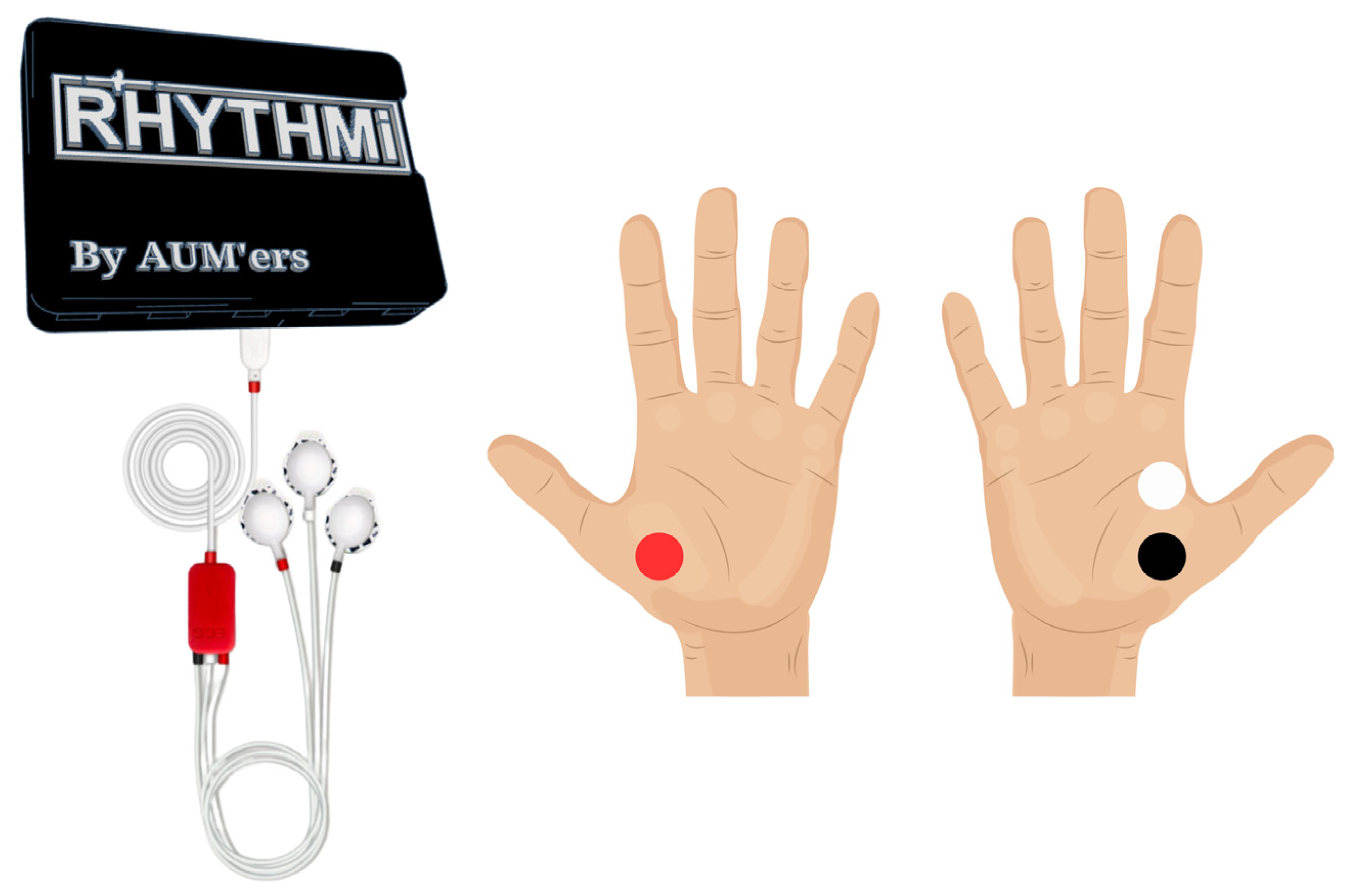
Figure 7, the developed system captures ECG signals in real time using the BITalino sensor. Electrodes are placed on the patient’s hands based on the recommendations of the manufacturer of the sensor:
The ECG signal is transmitted to the website for storage and processing. Once processed, a text file is generated containing the ECG signal data itself, the diagnosis based on the signal analysis, and feedback about the results. This text file can then be downloaded by the user for their records.
4.2. RHYTHMI’s Application
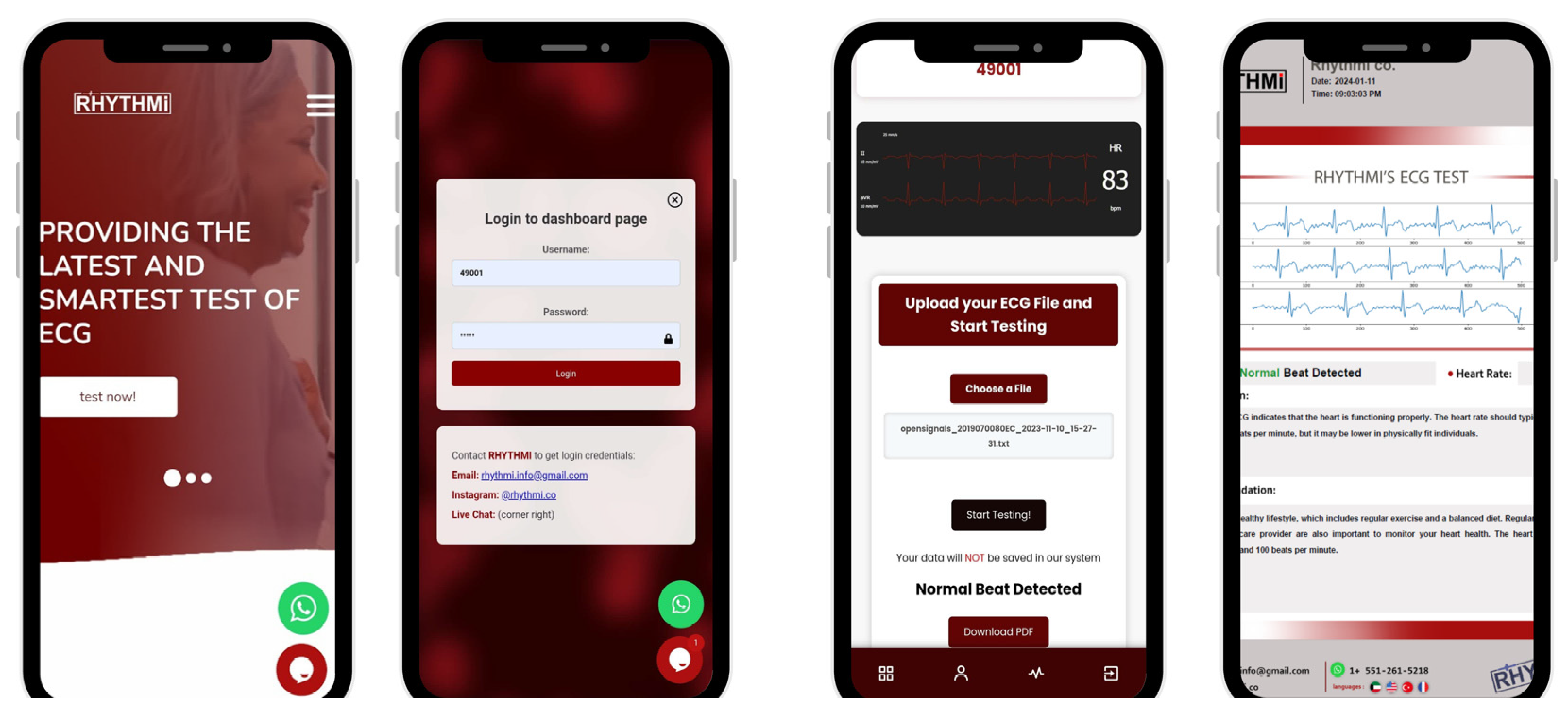
Rhythmi is a user-friendly system designed to help users monitor their heart health feasibly from their own devices. Initially built as an interactive website using HTML, CSS, and JavaScript, Rhythmi is now available as a mobile application (APK) using Median Toolbox. Python served as the backbone for the backend system hosting the deep learning model. Key libraries included NumPy for computations, Pandas for data management, Matplotlib for visualization, SciPy for signal processing, Scikit-learn for performance evaluation, Keras and TensorFlow for model development, PyPDF for report generation, and Flask for web application development. The ECG sensor has an application for recording ECG signals, which can be integrated with a mobile device via Bluetooth. To predict the heart status using Rhythmi, however, a Wi-Fi connection is required to upload readings to the dedicated website. A medical report is then generated following the prediction of the patient’s heart status, which is possible to be downloaded as a PDF file. Additionally, if the patient already has an ECG reading in a compatible format from another device, they can upload it to the website for prediction as well.
Figure 8 illustrates the intuitive layout of the Rhythmi app, guiding you through the login and testing process.
5. Results and Discussion
We employed a two-pronged approach to evaluate Rhythmi’s effectiveness:
Data-driven training and testing: As illustrated in
Figure 4, we initially trained and tested the deep learning model using the established MIT-BIH + BIDMC dataset. This dataset provided a foundation for the model’s learning process.
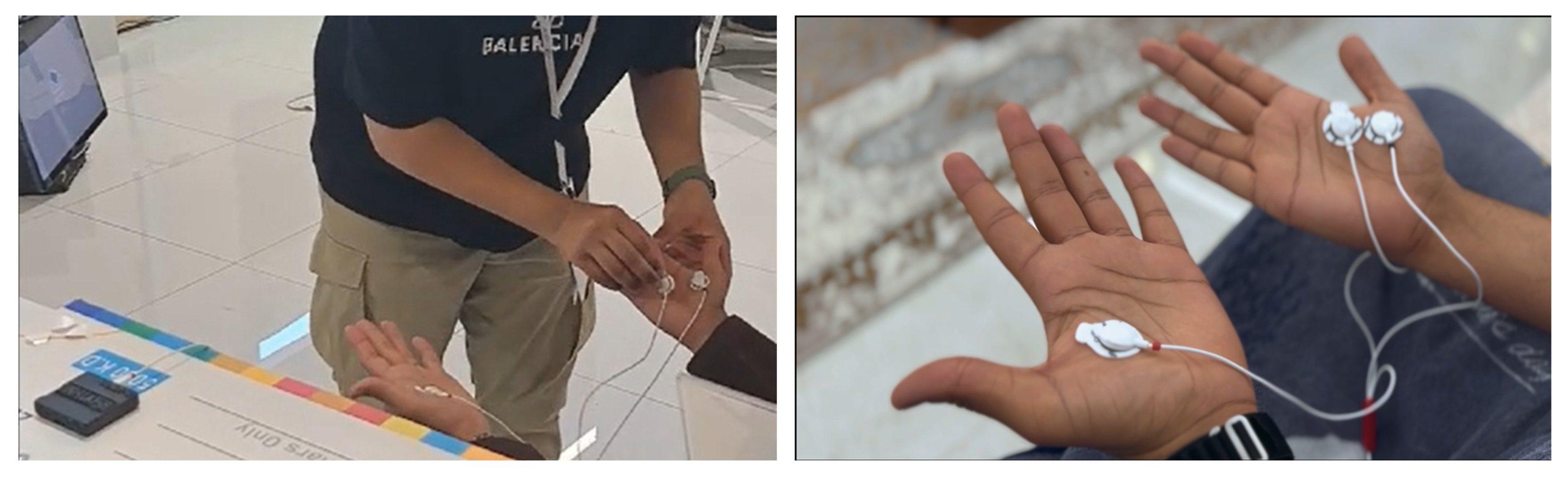
Real-world testing with human participants: Following the initial data-driven evaluation, we conducted real-time experiments to assess Rhythmi’s performance in practical scenarios. Many live tests were carried out directly on participants at exhibitions and competitions we participated in (see
Figure 9). For ethical considerations, consent for data usage from each participant was obtained. The trials conducted during our participation in exhibitions and competitions involved 82 male and 21 female participants aged between 13 and 69. Sixty-four of the tested participants were above the age of 40. This real-world testing provided valuable insights into the model’s ability to function effectively with actual users.
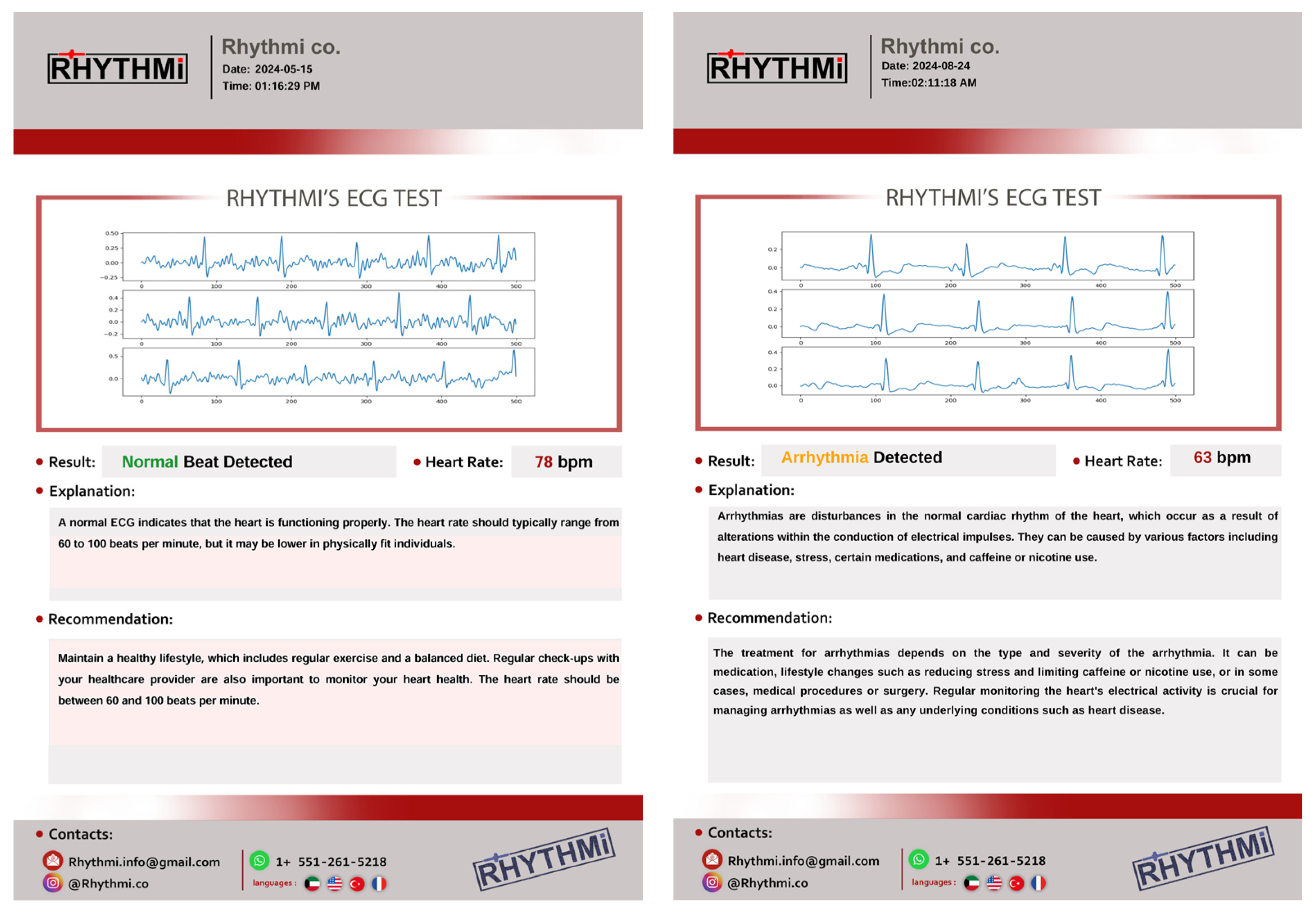
Real-time monitoring involves the ECG sensor continuously capturing and analyzing changes in the ECG signal as it is acquired. The signal is then immediately uploaded to Rhythmi for prediction, providing results within seconds, eliminating the need for prolonged wait times. The medical report is generated using only the first three heartbeats of the segmented ECG signal due to display limitations. This offers a brief overview of the cardiac activity. Heart rate variability (HRV) is calculated by identifying QRS complexes and measuring the intervals between them. It is crucial to understand that the provided recommendations and explanations based on the predicted heart condition are general in nature and cannot replace personalized medical advice. Recommendations are general guidelines based on real-world physician expertise for similar cases.
Figure 10 showcases the ECG diagnosis results obtained using the Rhythmi prototype on various individuals. It demonstrates the system’s ability to differentiate between normal and abnormal heart rhythm cases.
During real-world testing, 103 individuals participated in using Rhythmi to check their heart health. The analysis categorized 70 of these cases as normal heart rhythms, while the remaining 33 fell into the abnormal category (see
Figure 11). To assess Rhythmi’s accuracy in real-world scenarios, we compared the model’s diagnoses with evaluations by medical professionals. After consulting the generated reports from 103 participants with doctors, the results showed a 97.08% agreement between Rhythmi’s analysis and doctor diagnoses.
To assess Rhythmi’s performance using data, we conducted a rigorous testing process on the established MIT-BIH and BIDMC databases. This evaluation employed a 5-fold validation, which ensures a robust and reliable analysis.
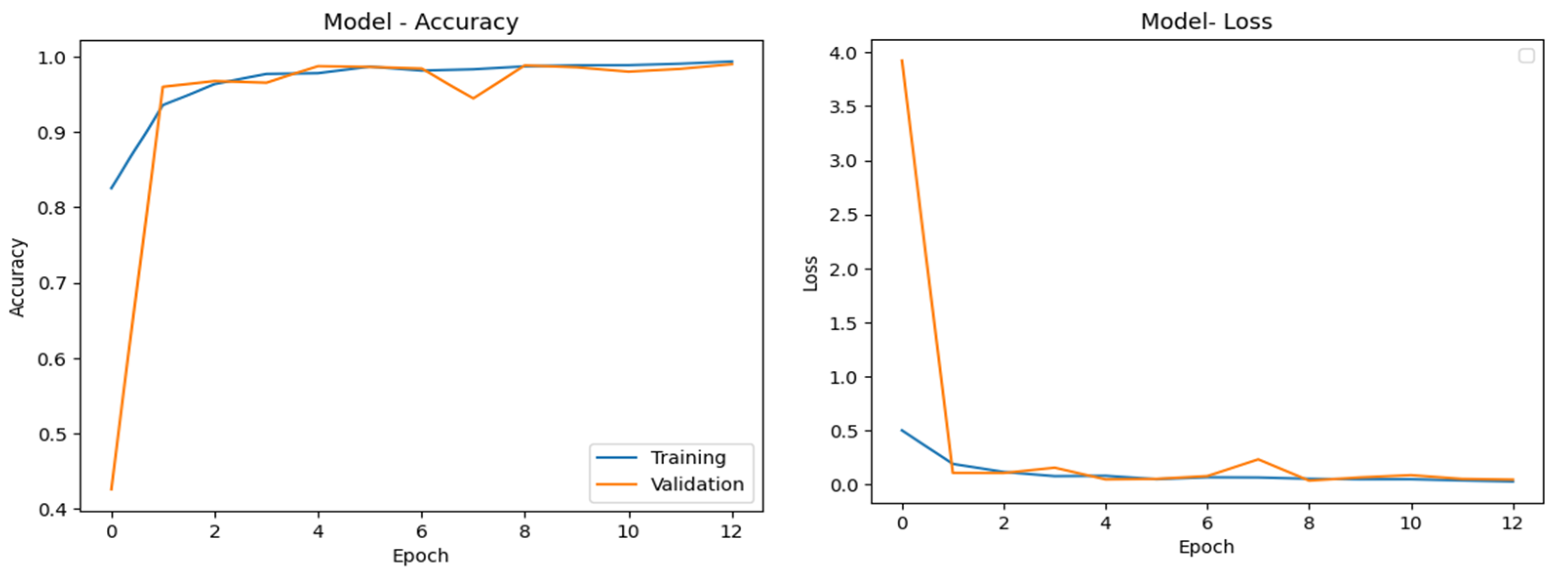
Figure 12 shows the model’s performance during training and validation. It shows both the accuracy and the loss (error) over all the training epochs (iterations). Here, you can see that the training stopped at epoch 12. This was not due to a set limit but because a technique called early stopping was employed. Early stopping is a crucial mechanism that helps prevent overfitting. This occurs when a model becomes too focused on the specific training data it sees and loses its ability to generalize well when presented with unseen data. Here is how early stopping works: We monitor the model’s performance on a separate validation set during training. If the validation loss does not improve for a certain number of epochs, the training is automatically halted. This ensures that the model learns from the general patterns in the data, not just the specifics of the training set. By preventing overfitting, early stopping also helps to avoid biased patterns. These biases can occur if the model learns to perform well on a specific type of data that might not be representative of real-world scenarios. Early stopping promotes a more robust model that can perform well on a wider range of data. The Adam optimizer was employed with a learning rate of 0.01. The model was trained for a maximum of 30 epochs using a batch size of 20. Batch size significantly impacts convergence. Smaller batch sizes generally lead to slower training but higher accuracy, as the model has more time to analyze each data point. Conversely, larger batch sizes accelerate training but can compromise accuracy due to the model’s limited exposure to individual samples.
Table 1 presents the results of our data-driven testing and compares them to the performance metrics of other relevant algorithms from the literature. These include machine learning (ML) techniques such as support vector machines (SVM), as referenced in [
39,
40], and deep learning (DL) approaches like convolutional neural networks (CNNs) and the pre-trained AlexNet model [
41]. It is important to note that some methods, such as continuous wavelet transforms (CWTs) [
42], employ feature extraction to enhance the ECG signal representation and to potentially improve performance.
The confusion matrix provided in
Figure 13 represents the performance of a classification model in predicting three classes of ECG heart disease: NSR (normal sinus rhythm), CHF (congestive heart failure), and ARR (arrhythmia). The model has high true-positive rates for all three classes, indicating strong performance in correctly classifying NSR, CHF, and ARR. Additionally, the model has low misclassification rates, with minimal instances of CHF and ARR being classified as NSR or vice versa. The model slightly struggles with distinguishing between NSR and ARR, as seen with 15 NSR instances misclassified as ARR. This could indicate some overlap or similarities in the features of these classes. With regard to the overall performance, the confusion matrix suggests that the model performs well, with high accuracy in classifying all three ECG heart disease classes. Also, the misclassifications are relatively low, implying that the model has learned to generalize well using the given data.
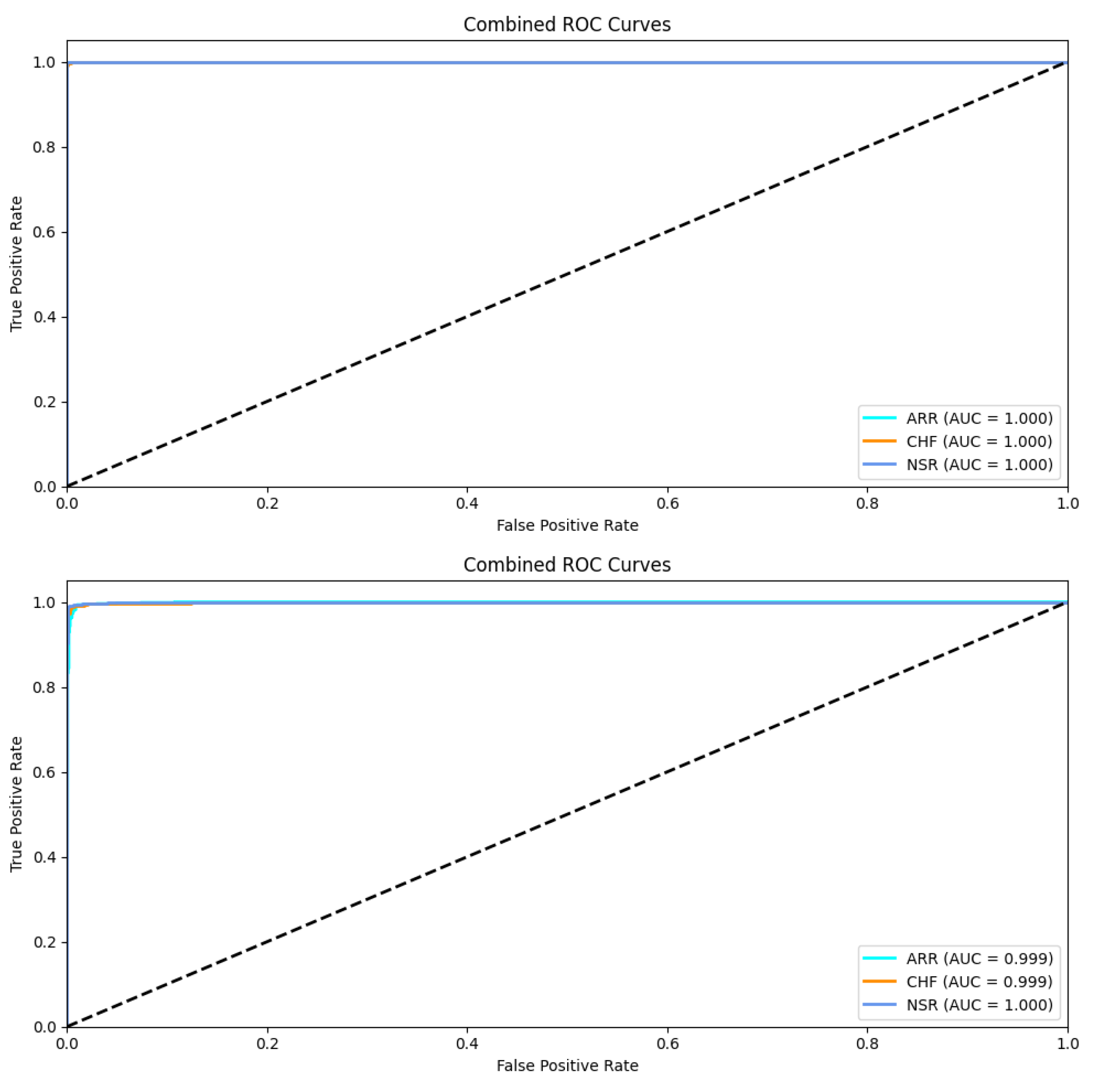
In
Figure 14, the class-wise ROC curves for the training and the test sets are shown. Class-wise AUC values are also listed in both graphs. The average AUC for testing all the classes reached 99.93% for the proposed model. This indicates the ability of the model to correctly classify signals across all possible classification thresholds.
6. Conclusions
This study aimed to introduce Rhythmi, a mobile ECG diagnosis device powered by deep learning and convolutional neural networks (CNNs) that was developed to provide accessible and accurate heart disease detection, particularly for conditions such as arrhythmia and heart failure. The device was trained using extensive medical data from reputable databases, achieving high accuracy in identifying various heart conditions. Moreover, the confusion matrix analysis demonstrated Rhythmi’s effectiveness and ability to distinguish between heart conditions with minimal errors, highlighting its robustness and reliability in real-world applications. The few misclassifications observed between NSR and ARR suggest areas for further refinement, but overall, the results indicate that the device can accurately diagnose heart diseases in real time. The impact of Rhythmi extends beyond the immediate clinical setting. By integrating AI into a mobile platform, the device addresses the significant limitations of traditional ECG diagnostic methods, including issues related to accessibility, cost, mobility, and data integration. This innovation represents a significant advancement in biomedical engineering, offering a portable, user-friendly solution that can be easily used by both healthcare professionals and patients. But, despite its strong performance and user-friendliness, the system has limitations that limit its general adoption. The use of only two databases restricts its ability to recognize diverse arrhythmias, including critical conditions such as Long QT syndrome. Additionally, the generic medical report lacks patient-specific information and is not personalized.
In the broader context of the healthcare system, Rhythmi has the potential to revolutionize the early detection and management of heart diseases, enabling timely intervention and reducing the burden on healthcare facilities. By making advanced diagnostic tools more accessible, Rhythmi contributes to the democratization of healthcare, ensuring that high-quality cardiac care is available to a wider population, particularly in remote or underserved areas. Our plans include expanding the ECG dataset to encompass diverse heart conditions, enhancing medical reports with AI-generated insights and blood pressure data, and improving application accessibility through an AI-powered chatbot.
Author Contributions
Conceptualization, A.E. and E.A.; Data curation, E.A., A.A. (Abdulwahab AlShatti), A.A. (Ahmad AlSultan) and D.A.; Formal analysis, A.E. and E.A.; Funding acquisition, A.E.; Investigation, A.A. (Abdulwahab AlShatti) and A.A. (Ahmad AlSultan); Methodology, A.E.; Project administration, A.E.; Resources, A.A. (Ahmad AlSultan) and D.A.; Software, E.A. and A.A. (Abdulwahab AlShatti); Supervision, A.E.; Validation, E.A., A.A. (Abdulwahab AlShatti) and D.A.; Visualization, E.A.; Writing—original draft, E.A., A.A. (Abdulwahab AlShatti), A.A. (Ahmad AlSultan) and D.A.; Writing—review and editing, A.E. and E.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Conflicts of Interest
The authors are the inventors of patent No. 20 2024 100 997. IPC: G16H 50/20.
References
- Russell, S.; Norvig, P. Artificial Intelligence: A Modern Approach, 4th ed.; Pearson: London, UK, 2021. [Google Scholar]
- Alzubi, J.; Nayyar, A.; Kumar, A. Machine Learning from Theory to Algorithms: An Overview. J. Phys. Conf. Ser. 2018, 1142, 012012. [Google Scholar] [CrossRef]
- Santosh, K.C.; Das, N.; Ghosh, S. (Eds.) Chapter 1—Introduction. In Primers in Biomedical Imaging Devices and Systems: Deep Learning Models for Medical Imaging; Academic Press: Cambridge, MA, USA, 2022; pp. 1–27. [Google Scholar]
- Silver, D.; Huang, A.; Maddison, C.J.; Guez, A.; Sifre, L.; Schrittwieser, D.; Antonoglou, I.; Panneershelvam, V.; Lanctot, M.; Dieleman, S.; et al. AlphaGo: Mastering the game of Go with deep neural networks and tree search. Nature 2016, 529, 484–489. [Google Scholar] [CrossRef]
- Srinivas, S.; Sarvadevabhatla, R.K.; Mopuri, K.R.; Prabhu, N.; Kruthiventi, S.S.S.; Babu, R.V. Chapter 2—An Introduction to Deep Convolutional Neural Nets for Computer Vision. In Deep Learning for Medical Image Analysis; Zhou, S.K., Greenspan, H., Shen, D., Eds.; Academic Press: Cambridge, MA, USA, 2017; pp. 25–52. [Google Scholar] [CrossRef]
- Zhang, H.; Qie, Y. Applying deep learning to medical imaging: A review. Appl. Sci. 2023, 13, 10521. [Google Scholar] [CrossRef]
- Eleyan, A. Statistical local descriptors for face recognition: A comprehensive study. Multimed. Tools Appl. 2023, 82, 32485–32504. [Google Scholar] [CrossRef]
- Eleyan, A. Face recognition using ensemble statistical local descriptors. J. King Saud Univ.-Comput. Inf. Sci. 2023, 35, 101729. [Google Scholar] [CrossRef]
- Yanagisawa, H.; Yamashita, T.; Watanabe, H. A study on object detection method from manga images using CNN. In Proceedings of the 2018 International Workshop on Advanced Image Technology (IWAIT), Chiang Mai, Thailand, 7–9 January 2018; pp. 1–4. [Google Scholar] [CrossRef]
- Vinod, G.; Padmapriya, G. An adaptable real-time object detection for traffic Surveillance using R-CNN over CNN with improved accuracy. In Proceedings of the 2022 International Conference on Business Analytics for Technology and Security (ICBATS), Dubai, UAE, 16–17 February 2022; pp. 1–4. [Google Scholar] [CrossRef]
- Hao, C.; Zhang, W.; He, W.; Chen, J.; Shao, L.; Li, Z. A hybrid GPU + FPGA system design for autonomous driving cars. In Proceedings of the 2019 IEEE International Workshop on Signal Processing Systems (SiPS), Nanjing, China, 20–23 October 2019; pp. 121–126. [Google Scholar] [CrossRef]
- Davidian, M.; Lahav, A.; Joshua, B.-Z.; Wand, O.; Lurie, Y.; Mark, S. Exploring the interplay of dataset size and imbalance on CNN performance in healthcare: Using X-rays to identify COVID-19 patients. Diagnostics 2024, 14, 1727. [Google Scholar] [CrossRef]
- Ismael, A.M.; Sengür, A. Deep learning approaches for COVID-19 detection based on chest X-ray images. Expert Syst. Appl. 2021, 164, 114054. [Google Scholar] [CrossRef] [PubMed]
- Eleyan, A.; Alboghbaish, E. Multi-classifier deep learning based system for ECG classification using fourier transform. In Proceedings of the 2023 5th International Conference on Bio-Engineering for Smart Technologies (BioSMART), Paris, France, 7–9 June 2023; pp. 1–4. [Google Scholar] [CrossRef]
- Eleyan, A.; Alboghbaish, E. Electrocardiogram signals classification using deep-learning-based incorporated convolutional neural network and long short-term memory framework. Computers 2024, 13, 55. [Google Scholar] [CrossRef]
- Martin, S.S.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Gibbs, B.B.; Beaton, A.Z.; Boehme, A.K.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. 2024 Heart disease and stroke statistics: A report of US and global data from the american heart association. Circulation 2024, 149, e347–e913. [Google Scholar] [CrossRef]
- Mironovova, M.; Bíla, J. Fast Fourier transform for feature extraction and neural network for classification of electrocardiogram signals. In Proceedings of the Fourth International Conference on Future Generation Communication Technology (FGCT), Luton, UK, 29–31 July 2015; pp. 1–6. [Google Scholar] [CrossRef]
- Sabor, N.; Gendy, G.; Mohammed, H.; Wang, G.; Lian, Y. Robust arrhythmia classification based on QRS detection and a compact 1D-CNN for wearable ECG devices. IEEE J. Biomed. Health Inform. 2022, 26, 59185929. [Google Scholar] [CrossRef]
- Satija, U.; Ramkumar, B.; Manikandan, M.S. A new automated signal quality-aware ECG beat classification method for unsupervised ECG diagnosis environments. IEEE Sens. J. 2019, 1, 277–286. [Google Scholar] [CrossRef]
- Malik, J.; Devecioglu, O.C.; Kiranyaz, S.; Ince, T.; Gabbouj, M. Real-time patient-specific ECG classification by 1D self-operational neural networks. IEEE Trans. Biomed. Eng. 2022, 69, 1788–1801. [Google Scholar] [CrossRef]
- Sun, Z.; Wang, C.; Zhao, Y.; Yan, C. Multi-label ECG signal classification based on ensemble classifier. IEEE Access 2020, 8, 117986–117996. [Google Scholar] [CrossRef]
- Wang, B.; Sun, H.; Yao, J.; Li, Y.; Liu, J.; Zhang, Y. Arrhythmia disease diagnosis based on ECG time–frequency domain fusion and convolutional neural network. IEEE J. Transl. Eng. Health Med. 2023, 11, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Thalluri, L.N.; Koripalli, H.; Nukala, P.K.N.; Mandava, V.N.S.R.; Gudapati, G.; Yaswanth, V.V.N. ECG signal classification using deep neural networks with ensemble techniques. In Proceedings of the 2022 7th International Conference on Communication and Electronics Systems (ICCES), Coimbatore, India, 22–24 June 2022; pp. 273–280. [Google Scholar] [CrossRef]
- Zhu, J.; Zeng, Y.; Zhou, J.; Dong, X. ECG heartbeat classification based on combined features extracted by PCA, KPCA, AKPCA and DWT. In Proceedings of the 2022 IEEE 35th International Symposium on Computer-Based Medical Systems (CBMS), Shenzen, China, 21–23 July 2022; pp. 155–159. [Google Scholar] [CrossRef]
- Ding, H.; Zhou, S.K.; Chellappa, R. FaceNet2ExpNet: Regularizing a deep face recognition net for expression recognition. In Proceedings of the 2017 12th IEEE International Conference on Automatic Face & Gesture Recognition (FG 2017), Washington, DC, USA, 30 May 2017–3 June 2017; pp. 118–126. [Google Scholar]
- Sai Mani Teja, B.; Anita, C.S.; Rajalakshmi, D.; Berlin, M.A. A CNN-based facial expression recognizer. Mater. Today Proc. 2021, 37, 2578–2581. [Google Scholar] [CrossRef]
- Bayram, F.; Eleyan, A. COVID-19 detection on chest radiographs using feature fusion based deep learning. Signal Image Video Process. 2022, 16, 1455–1462. [Google Scholar] [CrossRef] [PubMed]
- Dai, L.; Zhou, M.; Liu, H. Recent applications of convolutional neural networks in medical data analysis. In Federated Learning and AI for Healthcare 5.0; Advances in Healthcare Information Systems and Administration book series; IGI Global: Hershey, PA, USA, 2024; pp. 119–131. [Google Scholar] [CrossRef]
- Silva, L.C.; Sobrinho, A.; Cordeiro, T.D.; Melo, R.F.; Bittencourt, I.I.; Marques, L.B.; da Cunha, D.D.M.; da Silva, A.P.; Isotani, S. Applications of convolutional neural networks in education: A systematic literature review. Expert Syst. Appl. 2023, 231, 120621. [Google Scholar] [CrossRef]
- PhysioNet. MIT-BIH Arrhythmia Database. Available online: https://www.physionet.org/content/mitdb/1.0.0/ (accessed on 1 March 2024).
- PhysioNet. BIDMC Congestive Heart Failure Database. Available online: https://physionet.org/content/chfdb/1.0.0/ (accessed on 1 March 2024).
- Basu, S.; Mamud, S. Comparative study on the effect of order and cut off frequency of butterworth low pass filter for removal of noise in ecg signal. In Proceedings of the 2020 IEEE 1st International Conference for Convergence in Engineering (ICCE), Kolkata, India, 5–6 September 2020; pp. 156–160. [Google Scholar] [CrossRef]
- Chang, C.-H.; Wang, T.-M.; Hsu, H.-L. Denoising of mixed noises in ECG with separate noise estimators based on discrete wavelet transform. In Proceedings of the 2016 International Conference on Advanced Materials for Science and Engineering (ICAMSE), Tainan, Taiwan, 12–13 November 2016; pp. 562–564. [Google Scholar] [CrossRef]
- Atay, M.; Gipson, H.; Gwyn, T.; Roy, K. Evaluation of gender bias in facial recognition with traditional machine learning algorithms. In Proceedings of the 2021 IEEE Symposium Series on Computational Intelligence (SSCI), Orlando, FL, USA, 5–7 December 2021; pp. 1–7. [Google Scholar] [CrossRef]
- Li, W.; Xia, H.; Zhang, J.; Wang, Y.; Jia, Y.; He, Y. Complex-valued 2D-3D hybrid convolutional neural network with attention mechanism for POLSAR image classification. Remote Sens. 2024, 16, 2908. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, H.; Sun, W.; Bai, R. Intelligent fault diagnosis method for rotating machinery based on recurrence binary plot and DSD-CNN. Entropy 2024, 26, 675. [Google Scholar] [CrossRef]
- Huang, X.; Yuan, Y.; Li, J. MIMO Signal Detection Based on IM-LSTMNet Model. Electronics 2024, 13, 3153. [Google Scholar] [CrossRef]
- Bitalino Sensor. BITalino. Available online: https://www.pluxbiosignals.com/collections/bitalino (accessed on 9 August 2024).
- Lal, B.; Li, Q.; Corsonello, P.; Gravina, R. Abnormal ECG detection in wearable devices using compressed learning. In Proceedings of the 2023 International Conference on Networking, Sensing and Control (ICNSC), Marseille, France, 25–27 October 2023; pp. 1–6. [Google Scholar] [CrossRef]
- Kumari, C.U.; Ankita, R.; Pavani, T.; Vignesh, N.A.; Varma, N.T.; Manzar, M.A.; Reethika, A. Heart rhythm abnormality detection and classification using machine learning technique. In Proceedings of the 4th International Conference on Trends in Electronics and Informatics (ICOEI), Marseille, France, 25–27 October 2020; pp. 580–584. [Google Scholar] [CrossRef]
- Rahuja, N.; Valluru, S.K. A deep neural network approach to automatic multi-class classification of electrocardiogram signals. In Proceedings of the 2021 International Conference on Intelligent Technologies (CONIT), Hubli, India, 25–27 June 2021; pp. 1–4. [Google Scholar] [CrossRef]
- Katal, N.; Gupta, S.; Verma, P.; Sharma, B. Deep-learning-based arrhythmia detection using ecg signals: A comparative study and performance evaluation. Diagnostics 2023, 13, 3605. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Published by MDPI on behalf of the International Institute of Knowledge Innovation and Invention. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}