Abstract
After studying the professional practices related to the management of medical records in Kuwaiti hospitals, it became utterly evident that there is inadequate understanding about maintaining the health information of patients. This dire situation is further compounded by the absence of official regulations established by the Ministry of Health for hospitals to effectively assess and manage medical records. Through this study, the researchers aimed to assess the medical records system in multiple healthcare settings in Kuwait, comprising government, private, and oil sectors. The study was carried out from May 2019 to July 2020 and used a self-developed, pilot-tested questionnaire measuring various aspects of the medical records management system. A total of 98 participants responded to the survey. The study results revealed that 43% of hospitals were using paper-based medical records, as compared to 53% that used both paper-based and electronic media. Moreover, 40% of hospitals in Kuwait did not adhere to the Ministry of Health policies regarding medical records disposition; instead, they developed their own hospital-based disposition policy. Moreover, the study findings showed that there were clear discrepancies in record retention policies among the participating hospitals, and the duration of record retention varied from 2 years, 5 years, 10 years, and more than 20 years across hospitals in Kuwait. In conclusion, national policies and guidelines need to be established to monitor the medical record systems in Kuwaiti hospitals to further enable better patient care and improve healthcare facilities. Furthermore, it has become indispensable to develop and maintain electronic health records as they constitute an integral part of modern healthcare.
1. Introduction
In the present medical environment comprising a multidisciplinary team that provides care to a single patient, medical records or health information (paper or electronic) have become an indispensable part of clinical decision making [1]. Medical records are vital communication tools that include but are not limited to, data on laboratory or diagnostic tests, treatment plans, pre- and post-operative care, consent forms, discharge records, etc. [2]. Along with facilitating uninterrupted and smooth patient-centered care, medical records serve other equally imperative purposes, such as litigation cases that, for instance, may arise due to malpractice allegations, and reimbursement by third-party payers [2,3,4]. Despite health records being a crucial aspect of healthcare, poor clinical documentation practices have been reported in certain countries [5,6]. As stated by the World Health Organization (WHO), to boost the quality of any healthcare system, it is of paramount importance to ensure that a robust system for medical records management is in place [7].
The State of Kuwait comprises six governorates that are composed of primary, secondary, and tertiary healthcare centers [8]. Although medical records are maintained in all healthcare settings, their quality is poor, despite national standards established by the Ministry of Health (MoH) [9,10], and is further exacerbated by inadequate regulatory bodies overseen by the MoH. A case in point is a study conducted in 1985 to assess the medical records in Kuwaiti hospitals, which revealed significant deficiencies in the quality of the medical records system, such as incomplete documentation, lost patient records, misfiled diagnostic reports, and unskilled workforces [10]. A later study conducted by Moghli confirmed that the identified gaps in the medical records system were still persisting in Kuwaiti hospitals [11].
Other factors contributing towards a weak medical record system include an inadequate workforce and a decentralized medical records management, leading to the development of certain units, offices, and taskforce teams that are not officially processed by the MoH.
In a 2015 evaluation of the quality of the health information system (HIS) of Kuwait, the MoH deemed this system ‘inadequate’, highlighting the need for further improvement. Although significant steps have now been taken, such as the introduction of electronic health records (EHRs) across all primary healthcare centers, there remain several gaps in the EHR system in Kuwait’s healthcare settings. For instance, of the six secondary care centers, only three have employed an EHR system, despite EHRs receiving unprecedented global attention [8,9]. The benchmark for measuring the quality of medical records systems is set by professional organizations belonging to the health information management discipline.
A national strategic plan that aims to transform the State of Kuwait by 2035 is underway [12,13], which identifies ‘high quality healthcare’ as one of its seven pillars [13,14]. This strategic plan, along with establishing new healthcare centers, is focused on promoting interdisciplinary research to create and disseminate research-oriented knowledge. To achieve this, Kuwait urgently requires an integrated and ubiquitous platform to allow access to health information and render benefits for research, policymaking, and evidence-based decision-making [9,15]. Thus, it is indispensable that Kuwait’s healthcare centers not only improve their HIS but also undergo a complete transition from paper-based records to EHRs [9,16,17].
The literature on the medical record systems in Kuwait is extremely scarce [10]. While one study focused on specific aspects of medical records in a healthcare setting [18], another concentrated on patient satisfaction before and after the implementation of EHR [19]. In Karnataka, a large state in India, a systematic analysis was performed to study the health record management system in private hospitals. The study found that health data or information was unavailable for decision-making by public health managers, policymakers, and researchers. Although the government of India has regulations and policies in place to ensure proper data capture, analysis, and dissemination in a reliable and timely manner to enable effective decision-making, the study found discrepancies in data availability. The existing staff in most of the public health sector are burned out as they lack training in data collection and reporting. The study concluded that such challenges impeded the shift to EHRs [20].
A similar study conducted in Jordan assessed the structure and functions of the existing medical records system in 11 Ministry of Health hospitals, and found that there is a need to improve the work environment of the medical records department; address the shortage of qualified personnel; and offer training programs for medical records personnel, residents, interns, doctors, and head nurses. Additionally, a manual containing medical records policies and procedures should be prepared and disseminated, and medical records forms should be reviewed and updated. A national patient numbering system, terminal-digit filing system, record tracing system, and management system for active and inactive records must also be established. Additionally, several more medical records processes were delineated by the paper and recommended to be enhanced [21].
These findings are consistent with a study conducted in Egypt that was designed as a situation analysis of the quality of documentation of medical records in some Egyptian healthcare facilities. This study found that fundamental basic forms, such as general consent and discharge summaries, were missing in more than half of the reviewed records. Additional findings highlighted weaknesses like incorrect data, duplication of patient records, and illegible entries. The researchers concluded that such unreliable and poor quality of data should not be used in healthcare settings for decision-making. These results were in accordance with several common problems in documentation systems around the globe, where a lack of timely and quality data can lead to poor choices in clinical practice, medication errors, inappropriate repeating of tests, unnecessary referrals, and wastage of time and other resources [22].
With a focus on contributing significantly to the literature, our study aimed to investigate, explore, and assess the existing status of the medical records system in Kuwait’s six general, 17 tertiary, eight private hospitals, and one oil sector hospital. The objectives of the present study were to:
- Evaluate the existing condition of medical records in Kuwait’s healthcare centers;
- Establish whether medical records policies, procedures, and filing systems have been appropriately implemented and followed;
- Assess the disparity of the medical record system among the hospitals being studied;
- Assess the level of top management support for the management of medical records.
2. Materials and Methods
This was a mixed-methods, descriptive, and explanatory study conducted between May 2019 and July 2020, wherein the focus was to review the status of the medical records operations in Kuwait. As this was a mixed-methods study, we applied both quantitative and qualitative methodology for data analysis. This study was approved by two ethical committees; one was within the Kuwait University’s Health Sciences Centre (HSC) and the second through the MoH (Reference 8621) in January 2019.
2.1. Study Population
Regional directors from 38 hospitals were approached to participate in this study. The participating hospitals were classified into six general hospitals, 17 tertiary hospitals, eight private hospitals, and one oil sector hospital. Regional directors were invited via an invitation letter detailing the process of participation and data collection. The respondents to the survey were those occupying various positions primarily in the health information management departments. Most of them were medical records directors, deputy directors, and supervisors. We specifically selected this population as they are directly involved in the creation, maintenance, storage, management, and disposal of medical records; these professional practices and relevant decisions compose a significant part of our respondents’ daily work.
2.2. Data Collection Instrument
The research instrument was a self-developed questionnaire formed after an extensive literature review [10,18,21,23,24,25]. The theoretical basis of the questionnaire was the management of health record content and health record life cycle, as established in the health information management professional literature [11,26]. In regard to the practical basis of the quantitative and qualitative methodology for data analysis, existing MoH regulations and medical records practices in Kuwaiti hospitals were also considered.
The survey comprised 28 questions, categorized into seven sections. Part one of the survey included six questions concerning the participants’ demographics; Part two had four questions gauging the management processes of medical records in hospitals; Part three had seven questions related to the policies and procedures of the medical records management system; Part four had five questions related to medical records workforce; Part five had two questions on data access and confidentiality; Part six had three questions on data storage and disposal; Part seven had one closed question measuring the perception of the respondents’ vis-à-vis a pre-established list of 12 commonly expressed problems involving the existing HIS. We established the face validity of the research instrument by carrying out multiple rounds of reviews to ensure that it effectively addressed the research questions and closely reflected our interests. In specific, two ethical committees, one at the Kuwait University’s Health Science Centre and the second at the MoH, reviewed the questionnaire and recommended certain modifications that we incorporated. For example, certain terms were changed, additional private hospitals were included, and typographic errors were corrected, as recommended by the ethical committees.
Moreover, the researchers incorporated comments and feedback into the last version of the survey, and pilot tested the tool. The final version of the survey instrument was found to be comprehensible with a logical flow, ascertaining the instrument’s face validity.
2.3. Conducting the Survey
First, two researchers distributed the invitation letters and surveys to all six health districts directors, who in turn forwarded them to hospital directors, and subsequently to the medical records directors. The researchers then met with the medical records directors to hand in a copy of the study approval, brief them on the study objectives, and set deadlines for collecting the answered surveys. The survey was self-administered, and the data collection lasted for approximately 14 months with the following experienced difficulties:
- Delays in sending the original invitations from the health district headquarters to targeted hospitals.
- Rejection to participate in the study by certain sites without receiving the original invitations.
- Delays in returning the completed surveys, which were self-administered by the respondents.
- The process of data collection was interrupted for four months due to the government shutdown in Kuwait during the peak of the coronavirus disease (COVID-19) pandemic (February–June 2020).
The researchers decided to avoid using a web-based survey due to a lack of internet connection in general hospitals in Kuwait and because the survey design included certain complex questions that may compromise the accuracy of the collected data [27]. Moreover, to improve the response rate, researchers personally visited the participating hospitals multiple times to collect the completed surveys.
2.4. Statistical Analysis
The study results were analyzed using IBM SPSS Statistics for Windows, Version 27.0 (Armonk, NY, USA) and Microsoft Excel (Redmond, WA, USA). Univariate, cross tabulation, and Pearson correlation statistics were performed. Compatible with the study objectives and design, descriptive statistics and explanatory analysis were used to describe the collected data. The research team began with verifying the accuracy of the data and examined an overview of the respondents. Although we collected responses on the medical records workforce (part 4 of the survey) and data access & confidentiality (part 5 of the survey), they were not included in the data analysis and are not reported in the study. The research team later deemed it unfitting to incorporate issues related to the workforce and data access and confidentiality in a study that is focused on operational issues of the HIS departments; Therefore, we decided to address these aspects in a more in-depth study in the future.
3. Results
3.1. Response Rate
A total of 38 hospitals were invited to participate in the study. The response rate to the invitation was 78.94%. In addition, a total of 132 surveys were distributed to medical records directors, deputy directors, and supervisors. Of which, a total of 98 completed surveys were received, for a total response rate of 74.24%. Results showed that the response rate was significantly higher in government hospitals as compared to private hospitals. Reasons for the low response rate of private hospitals included no response/no contact (50%), declined/refused (25%), demanded more forms, incomplete or delayed responses (25%). Characteristics of the target population are shown in Table 1. A total of 124 participants were categorized into 21 medical records directors, 10 deputy directors, 15 assistant directors, and 78 supervisors.
Table 1.
Characteristics of the Target Population.
3.2. Demographics of the Survey Participants
The results showed that 80.6% of the participants were Kuwaiti whereas 19.4% were non-Kuwaiti. Of the participants, 82.7% were females and 16.3% were males.
3.3. Charectaristics of the Medical Records Management System
Table 2 shows the characteristics of the medical records management system. Respondents were asked four questions concerning different aspects of managing medical records. The first question was on the media of medical records, which asked respondents to specify in what media the medical records were stored.
Table 2.
Characteristics of the Medical Records Management System in Kuwait.
The second question was about the type of medical records used in the department, such as manual, electronic, or a combination of manual and electronic (hybrid) systems. In terms of storage, most hospitals mentioned that their medical records were kept in the on-site filing room, while oil sector hospital stated that they used a HIS and archived their inactive medical records off-site via outsourcing. Considering the filing system, most healthcare facilities used the terminal digit filing system (77%), while some employed serial numeric filing (20%), and 3% used the employee ID number.
3.4. Policies and Procedures of the Medical Records Management Department
Table 3 shows responses to questions on the policies and procedures of the medical records management system and the frequency of updating them. Moreover, we also asked the respondents whether their employees are aware of such policies and procedures, and what methods are used to keep the employees updated. Through the survey, we also inquired about how the employees become aware of their roles and responsibilities, and whether they are provided a copy of their roles and responsibilities.
Table 3.
Policies and Procedures of the Medical Records Management System in Kuwait.
3.5. Storage, Retention, and Disposition of the Medical Records
The main question that health information professionals are frequently asked is “For how long are the medical records retained?” Table 4 shows that there were different considerations for record storage, retention, and disposition based on the nationality of the patients. Among general hospitals, 83.3% keep the inactive records of Kuwaiti patients for 10 years, whereas 68% of tertiary hospitals do so. Whereas the oil sector hospital has an outsourced storage facility and all inactive records are archived by the outsourcing company. Regarding the medical records of non–Kuwaiti patients, most of them are archived for five years in both general and tertiary hospitals.
Table 4.
Storage Retention, and Disposal of Medical Records.
As shown in Table 4, concerning the availability of storage space, 78.9% of tertiary hospitals stated an absence of enough space for storage within their departments. Whereas most of the general hospitals agreed that there is not enough space for the storage of medical records.
The results of the data analysis concerning who authorizes patient record disposition showed that 66.7% and 8.4% of general and tertiary hospitals adhere to the MoH’s disposition policy, respectively. On the other hand, as per our results, 33.3% of general hospitals follow their own disposition policy. Similarly, results to the same question show that 33% of medical records departments follow their own policies for record disposal.
3.6. Problems in the Existing Medical Records Management Systems
Respondents were asked to identify the top five problems faced while managing medical records from a pre-established list of 12 problems. The most prevalent problems cited by the respondents were: missing medical records, lack of storage facilities, slow retrieval of records, and duplication of patients’ records. Figure 1 represents the major problems in the existing manual management system, as indicated by the respondents.
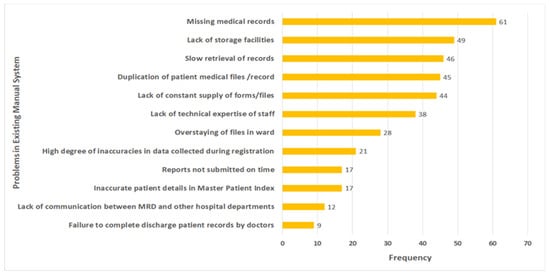
Figure 1.
Top problems in the existing manual management system.
3.7. Correlation Analysis
Correlation between three variables, i.e., years of service, availability of updated policies, and awareness of the staff showed a significant correlation (0.213) at the 0.05 level (Table 5). However, no significant correlation was found between missing medical records, lack of storage area, and the system of filing records (Table 6).
Table 5.
Correlations between Years in Service and Availability of Updated Policies and Staff Awareness.
Table 6.
Correlation between Missing Medical Records, Lack of Storage Area, and Filing of the Records.
4. Discussion
This study aimed to determine the existing functions of the medical records system of Kuwait and provide recommendations for reforming and strengthening the health information management system (HIMS). The following four main aspects of Kuwait’s HIMS were assessed: (1) Characteristics of the medical records management system; (2) Medical records policies and procedures; (3) Storage, retention, and disposal of the medical records; and (4) Existing problems in the HIMS. The results of this study reveal that the policies and procedures of the HIMS in Kuwait’s healthcare settings are nonuniform and withhold major gaps, additionally lacking sufficiently trained staff for managing health information.
The manual, paper-based method of medical record keeping is the traditional method that poses serious limitations, a few of which are challenges with accessibility, accuracy, storage, and retrieval of data [2,18]. Paper-based medical records cause additional issues, such as lost charts, ineffective record management, and writing errors, raising serious challenges in collecting, validating, and analyzing data [18]. EHRs are tools that enable healthcare practitioners to collect, manage, store, and retrieve health-related information of patients in an electronic format, thereby enabling easy access and sharing of records between different authorized individuals at any given location. EHRs can thus enable healthcare personnel to improve coordination in providing care, further eliminating duplication of patient records and diagnostic tests, by efficiently making the previous results of laboratory tests and interventions available to different points of care [26].
In regard to the format of patient records (Table 2), our study showed that patient records were predominantly stored as both paper and EHRs (53%) and as paper records alone (43%). Although all primary healthcare centers in Kuwait have implemented an EHR system, there seems to be a great gap between the maturity and adoption of this system across different facilities [28]; these statements are consistent with our results as we found that almost half of the hospitals still use paper records alone.
HIS is an integrated system that enables the effective management of clinical, administrative, and financial information in healthcare settings, including the management of healthcare data, such as collecting, storing, and transferring EHRs. According to LaTour [29] and Abdelhak [30], there are several technical functions within the scope of HIS practice, such as coding, abstracting, releasing information, and analyzing the documents qualitatively and quantitatively. Based on our results, most hospitals (70%) in Kuwait have employed a hybrid system, comprising both manual and HIS, while 20% and 10% of the hospitals use a manual system and the HIS, respectively, to process and manage the technical functions of HIS.
The MoH is the guiding force of the medical records standards, policies, and procedures represented by the National Center for Health Information (NCHI), which follows the WHO standards for quality of services in the medical records departments in developing countries; its role is similar to that of The American Health Information Management Association, The Healthcare Information and Management Systems Society, The American Medical Informatics Association, and many more [31]. However, the lack of uniform standards is reportedly a major barrier that affects the implementation of EHRs in Kuwait, as stated by Almutairi [18]. Although this report [18], which examined and identified measures for improving the adoption of EHRs in Kuwait, stated that the quality and delivery of patient care can be enhanced by increasing access to patient information, a HIS that is not efficiently managed can be counterproductive. Health information that is not appropriately maintained, managed, updated, and secured can have an opposing effect; rather than being beneficial to healthcare reforms, inadequately managed health information can create problems and barriers [26].
The implementation of policies and procedures is of paramount importance; however, the reality of this domain within the HIMS of Kuwait, as revealed by the respondents, seems unorganized at best and arbitrary at worst. Although all respondents claim that their medical records policies and procedures are updated, and almost half of them claim that they are reviewed annually, our results (Table 3) show professional negligence regarding the awareness of these policies and procedures. Supported by the findings of Chun and Salman in a policy paper for health reforms in Kuwait [9,15], the medical record system in Kuwait not only needs to be improved but also needs to undergo a complete transition from paper-based records to EHRs.
A study by Gupta et al. [32] showed disorganization in an apex tertiary care center of New Delhi, wherein poorly filed medical records with missing consent forms depicted increased lengths of hospital stay, higher cases of morbidity and mortality, along with patient dissatisfaction. In our study, the responses on making the staff aware of policies and procedures seem dissatisfactory, and the efforts are majorly insufficient. To avoid such adverse events, it is crucial to standardize medical records and train the hospital staff to meet these documentation standards, by circulating guidelines and facilitating workshops to update the staff and the doctors about their role in medical records documentation [32].
Major processes in the management of paper-based and hybrid health records are the storage, retention, and disposal of records [29,30]. Considering the responses obtained in this study, it was evident that all participating hospitals stored their health records on-site, whereas the one oil-sector hospital included used HIS for storing active records and archived inactive records by outsourcing them.
Tavakoli and Johanbkhs [33] have emphasized that the retention of medical records is an important aspect of a health care facility. Medical records must be maintained by a facility to support patient care; meet legal and regulatory requirements; achieve accreditation; support research, education, and reimbursement, and facilitate hospital administration. The duration of record retention differs based on the type of records, such as laboratory data, radiology reports and films, fetal monitor strips, birth certificates, and patient master index. Medical records retention and the disposal of unnecessary records is extremely important considering the challenges commonly confronted with limited space for storage of these records.
In our study, the stark discrepancy between the retention of medical records of Kuwaiti versus non-Kuwaiti patients shows that the retention and disposal of health records is handled arbitrarily. The retention of medical records is disproportionate across the population as the retention period is 10 years for roughly 73% of Kuwaiti patients and 5 years for 80% of non-Kuwaiti patients. This 5-year gap between the Kuwaiti and non-Kuwaiti patients is striking and unjustified, especially considering that 70% of the population of Kuwait comprises expatriates [8]. No specific rationale was provided to validate the reason behind this discrepancy in the retention policy based on the ethnicity of patients. Making matters seem even more random is the realization that there is no distinct correlation between retention policy and clinical outcomes. Our study findings state that the process of health records storage, retention, and disposal is largely inconsistent among hospitals in Kuwait.
In terms of compliance with central policies established by the MoH, although most hospitals adhere to the MoH’s policy concerning the retention and disposal of health records, 33% of hospitals tend to follow their own disposal policies. The fact that most hospitals adhere to the MoH policies indicates compliance with ministerial direction; hence, the impetus falls upon the MoH to formulate and enforce effective policies for record retention and disposal in hospitals. However, policies regarding the storage, retention and disposal of medical records require uniformity across all healthcare settings and accreditation by authorized bodies, perhaps by the National Accreditation Program for Hospitals (NAPH) in collaboration with the MoH.
Finally, our study examined the problems in the existing medical records management system. As per our findings, the top six problems were missing medical records, lack of storage facilities, slow retrieval of records, duplication of patient’s medical files, lack of supply of forms or files, and lack of technical expertise of the staff. These problems can be solved by implementing an EHR system that would provide quantitative benefits, which would help save time and cost; qualitative benefits, which would ensure data accuracy, easy accessibility, and efficient transfer of information; and strategic benefits, which would enable health research and policymaking [34]. Moreover, the overall negative impact of the COVID-19 pandemic in Kuwait necessitates the need for targeted interventions through the provision of accessible and acceptable services using health information tools [35,36].
The socio-economic status of Kuwait allows a sedentary lifestyle and a high-caloric diet, causing a rise in non-communicable diseases (NCDs), such as hypertension and diabetes [13,15]. Kuwait’s current healthcare system cannot sustain the growing burden of NCDs, making healthcare reform efforts, such as better-quality healthcare and reduced costs, a top priority. In order to achieve these milestones, it is of paramount importance that the healthcare system of Kuwait adopts effective health information technology, such as EHRs [37].
The aforementioned factors, along with the study results, clearly depict that the HIMS practiced in hospitals of Kuwait call for an urgent intervention for the improvement of medical records [32,38]. To reap the clinically-relevant benefits of the medical record system, healthcare settings must ensure the documentation of complete, accurate, timely, accessible, safe, secure, and legible medical records [29,30]. Certain accreditation practices must be implemented to establish a baseline for the required minimum expectations, if not superior quality [26]. The ripple effect of this will eventually lead to improved quality of care in Kuwaiti hospitals.
Considering the study findings, the MoH and the NCHI must lead HIM practices in Kuwaiti hospitals by establishing, enforcing, and monitoring national and international standards, guidelines, and policies for the medical record management system, based on previously published literature. Moreover, the NCHI should institutionalize a robust mechanism to monitor adherence to the established national policies and guidelines in Kuwaiti healthcare settings. Communication channels or networks between NCHI and satellite HIM departments in various hospitals must be improved to facilitate a smooth and continuous exchange of reports and guidelines. Furthermore, corrective measures should be developed when there is incompliance with national policies and procedures.
Finally, we believe that hospitals must invest in extensive training and providing mentorship to professionals in their medical record departments on the important aspects of information management to reap benefits [37]. Moreover, a clear hierarchy must be maintained in these departments, and knowledgeable individuals must be hired to strengthen the workforce.
Our study has several strengths. Since it was a mixed-methods study, it applied both quantitative and qualitative methodology, providing a better understanding of research problems than either of the approach alone. This is an up-to-date study and, to our knowledge, is the first study addressing the existing medical records management system of Kuwait, which is an invaluable addition to the limited body of work in this field. However, this study is limited because it lacks questions related to other health information management operations, such as quality of documentation. This study also lacks information on the reasons why hospitals do not comply with certain policies and procedures. Since this is a self-administered questionnaire, the information provided by the participants could be subject to recall bias. Finally, the small sample size, along with other factors, limits the generalizability of this study.
5. Conclusions
Our study found major gaps in the HIMS of Kuwaiti hospitals. To tackle these issues, we recommend the implementation of EHRs, health information training for staff members, establishing strict guidelines and policies to oversee the HIMS in hospitals, and accreditation practices to monitor adherence to these guidelines. Through our research, we aim to benefit stakeholders, researchers, policymakers, hospital healthcare management professionals, and ultimately patients and healthcare providers. Owing to the limited literature on the HIMS of Kuwaiti hospitals, we believe further studies are needed to improve practices and strengthen health information practices.
Author Contributions
Conceptualization, M.A.; Formal analysis, M.A.; Investigation, M.A.; Methodology, M.A.; Supervision, M.A.; Validation, M.A., A.S., H.A., M.Y. and N.A.-E.; Visualization, M.A.; Writing—original draft, M.A.; Writing—review & editing, M.A., A.S. and M.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank Dalal Al-Sabhan, Nabeel Akhtar and Lubaina Koti for their support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mathioudakis, A.; Rousalova, I.; Gagnat, A.A.; Saad, N.; Hardavella, G. How to keep good clinical records. Breathe 2016, 12, 369–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, J. Medical records and issues in negligence. Indian J. Urol. 2009, 25, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Gillum, R.F. From Papyrus to the Electronic Tablet: A Brief History of the Clinical Medical Record with Lessons for the Digital Age. Am. J. Med. 2013, 126, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahman, W.; Abdelmageed, A. Medical record keeping: Clarity, accuracy, and timeliness are essential. BMJ 2014, 348, f7716. [Google Scholar] [CrossRef]
- McFall, W.J., Jr.; Bader, J.D.; Rozier, R.G.; Ramsey, D. Presence of Periodontal Data in Patient Records of General Practitioners. J. Periodontol. 1988, 59, 445–449. [Google Scholar] [CrossRef]
- Brown, L.F.; Keily, P.A.; Spencer, A.J. Hygienist employment and the presence of periodontal notations in general dental practice patient records. Aust. Dent. J. 1994, 39, 45–49. [Google Scholar] [CrossRef]
- WHO. Everybody Business—Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Mossialos, E.; Cheatley, J.; Reka, H.; Alsabah, A.; Patel, N. Kuwait Health System Review; London School of Economics and Political Science: London, UK, 2018. [Google Scholar]
- Chun, S.; Salman, A. Policy Paper for the Health Pillar: Overview of Gaps, Challenges, and Way Forward in Kuwait National Development Plan 2015–2020; Kuwait Public Policy Center, General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019.
- Medical Records Working Party. Medical Records in Kuwait; Ministry of Public Health: Kuwait City, Kuwait, 1985.
- Mogli, G.D. Medical Records Role in Healthcare Delivery in 21st Century. Acta Inform. Med. 2009, 17, 209–212. [Google Scholar]
- Salman, A.; Al-Hemoud, A.; Fakhraldeen, S.; Al-Nashmi, M.; AlFadhli, S.; Chun, S. Research and Development as a Moderating Variable for Sustainable Economic Performance: The Asian, European, and Kuwaiti Models. Sustainability 2020, 12, 7525. [Google Scholar] [CrossRef]
- Salman, A.; Fakhraldeen, S.; Chun, S.; Jamil, K.; Gasana, J.; Al-Hunayan, A. Enhancing Research and Development in the Health Sciences as a Strategy to Establish a Knowledge-Based Economy in the State of Kuwait: A Call for Action. Healthcare 2020, 8, 264. [Google Scholar] [CrossRef]
- National Sustainable Development Goals Implementation Committee in Kuwait. Kuwait Voluntary National Review 2019: Report on the Implementation of the 2030 Agenda to the UN High-Level Political Forum on Sustainable Development; General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019.
- Salman, A.; Tolma, E.; Chun, S.; Sigodo, K.; Al-Hunayan, A. Health Promotion Programs to Reduce Noncommunicable Diseases: A Call for Action in Kuwait. Healthcare 2020, 8, 251. [Google Scholar] [CrossRef]
- Chun, S.; Salman, A. Research Agenda for the Health Pillar; Kuwait Public Policy Center, General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019. [CrossRef]
- Chun, S.; Salman, A. White Paper for the Health Pillar National Health Policy Framework: Ensuring Healthy Lives and Wellbeing; Kuwait Public Policy Center, General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019. [CrossRef]
- Almutairi, B. A Strategic Roadmap for Achieving the Potential Benefits of Electronic Health Record System in the State of Kuwait. Ph.D. Thesis, University College London, London, UK, 2011. [Google Scholar]
- Al-Jafar, E. Exploring patient satisfaction before and after electronic health record (EHR) implementation: The Kuwait experience. Perspect. Health Inf. Manag. 2013, 10, 1c. [Google Scholar] [PubMed]
- Johar, S.; Patagundi, B. Analysis of Health Record Management System in Private Hospitals. Ph.D. Thesis, Cambridge Institute of Technology, Ranchi, India, 2021. [Google Scholar]
- Ajlouni, M. Assessment of Medical Records Services at Ministry of Health Hospitals in Jordan; Abt Associates Inc.: Bethesda, MD, USA, 2006. [Google Scholar]
- Ahmed, H.A.A.; El-Salami, R.M.; Ayad, K.M.; El-Deeb, A.E.-A.F. Assessment of Medical Records Documentation in Secondary Health Care Facilities in Kafr El-Sheikh and El-Mahalla El-Kubra Cities. Med. J. Cairo Univ. 2019, 87, 183–194. [Google Scholar]
- Moghaddasi, H.; Hosseini, A.; Sheikhtaheri, A. A new model for the organizational structure of medical record departments in hospitals in Iran. Perspect. Health Inf. Manag. 2006, 3, 4. [Google Scholar]
- Hajavi, A.; Haqani, H.; Akhlaqi, F.; Pur, U.M. Evaluating the Performance of the Medical Records Departments of Mashhad medical University teaching hospital (1381). J. Health Adm. 2005, 7, 7–13. [Google Scholar]
- Ngidi, T. Management of Medical Records: A Study at Princes Marina Hospital, Gaborone, Botswana. Master’s Thesis, University of Botswana, Gaborone, Botswana, 2016. [Google Scholar]
- Alhuwail, D. Understanding health information management practices in public hospitals in Kuwait. Health Inf. Manag. J. 2019, 49, 127–136. [Google Scholar] [CrossRef]
- Fricker, R.D.J.; Schonlau, M. Advantages and Disadvantages of Internet Research Surveys: Evidence from the Literature; SAGE Internet Research Methods: London, UK, 2012. [Google Scholar]
- Weber, A.S.; Turjoman, R.; Shaheen, Y.; Al Sayyed, F.; Hwang, M.J.; Malick, F. Systematic thematic review of e-health research in the Gulf Cooperation Council (Arabian Gulf): Bahrain, Kuwait, Oman, Qatar, Saudi Arabia and United Arab Emirates. J. Telemed. Telecare 2016, 23, 452–459. [Google Scholar] [CrossRef]
- LaTour, K.M.; Maki, S.E. Health Information Management: Concepts, Principles, and Practice, 5th ed.; American Health Information Management Association: Chicago, IL, USA, 2010. [Google Scholar]
- Abdelhak, M.; Hanken, M.A. Health Information, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Kruk, M.E.; Freedman, L.P. Assessing health system performance in developing countries: A review of the literature. Health Policy 2008, 85, 263–276. [Google Scholar] [CrossRef]
- Gupta, A.; Jain, K.; Bhoi, S. Evaluation of patients record and its implications in the management of trauma patients. J. Emerg. Trauma Shock 2020, 13, 257. [Google Scholar] [CrossRef]
- Tavakoli, N.; Jahanbakhsh, M. Investigation of retention and destruction process of medical records in the hospitals and codifying appropriate guidelines. J. Educ. Health Promot. 2013, 2, 17. [Google Scholar] [CrossRef]
- Al-Shorbaji, N. Improving Healthcare Access through Digital Health: The Use of Information and Communication Technologies. In Healthcare Access; IntechOpen: London, UK, 2021. [Google Scholar]
- Salman, A.; Sigodo, K.; Al-Ghadban, F.; Al-Lahou, B.; Alnashmi, M.; Hermassi, S.; Chun, S. Effects of COVID-19 Lockdown on Physical Activity and Dietary Behaviors in Kuwait: A Cross-Sectional Study. Nutrients 2021, 13, 2252. [Google Scholar] [CrossRef]
- Salman, A.; Al-Ghadban, F.; Sigodo, K.; Taher, A.; Chun, S. The Psychological and Social Impacts of Curfew during the COVID-19 Outbreak in Kuwait: A Cross-Sectional Study. Sustainability 2021, 13, 8464. [Google Scholar] [CrossRef]
- McAlearney, A.S.; Robbins, J.; Kowalczyk, N.; Chisolm, D.J.; Song, P.H. The role of cognitive and learning theories in supporting successful EHR system implementation training: A qualitative study. Med. Care Res. Rev. 2012, 69, 294–315. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.G.; Lyle, D. Lean Integration: An Integration Factory Approach to Business Agility; Addison-Wesley Professional: Boston, MA, USA, 2010. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).