
A Prototype of an Electronic Pegboard Test to Measure Hand-Time Dexterity with Impaired Hand Functionality

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
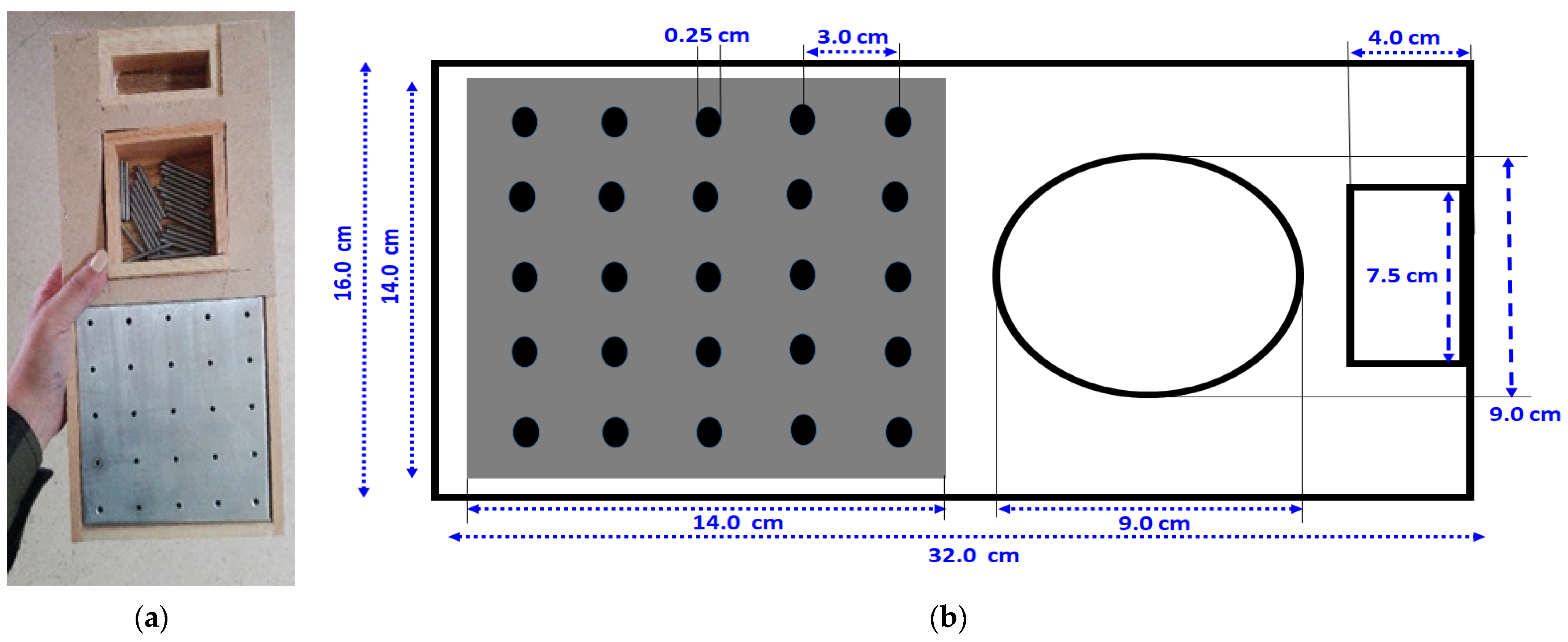
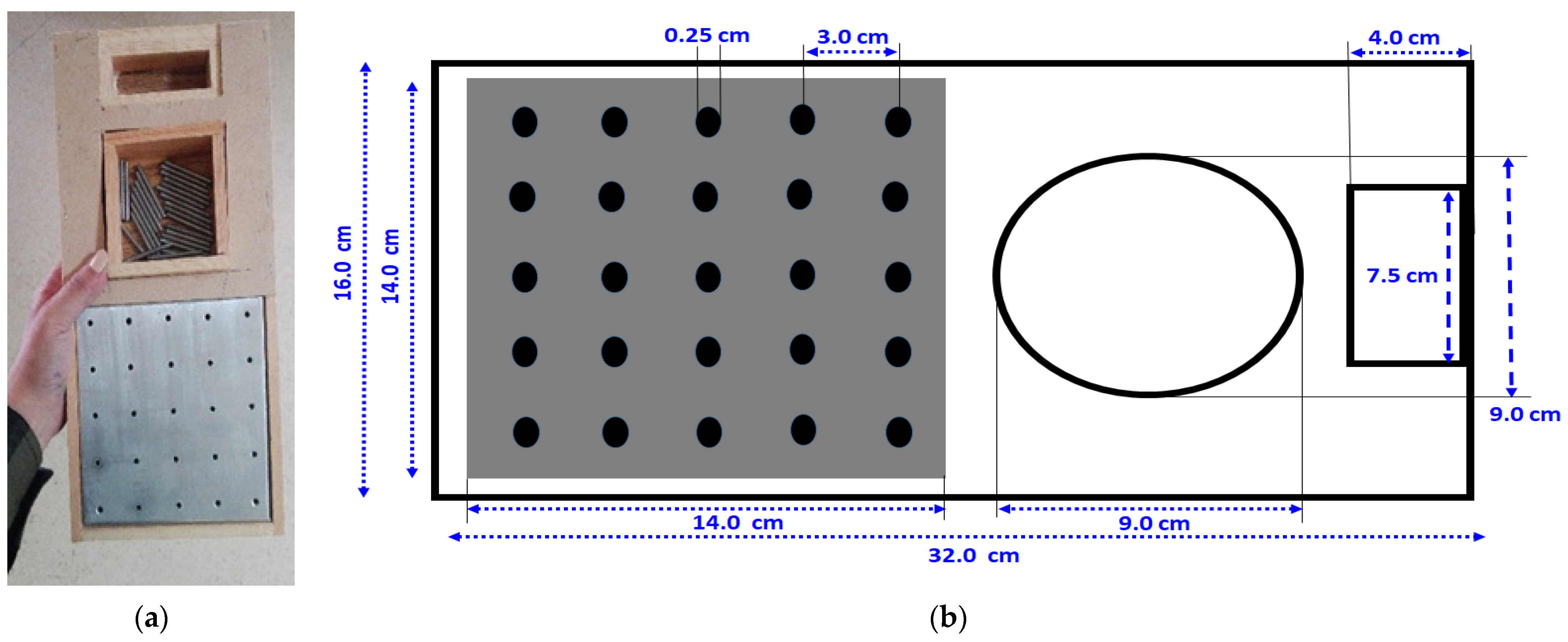
2.1. Pegboard Construction
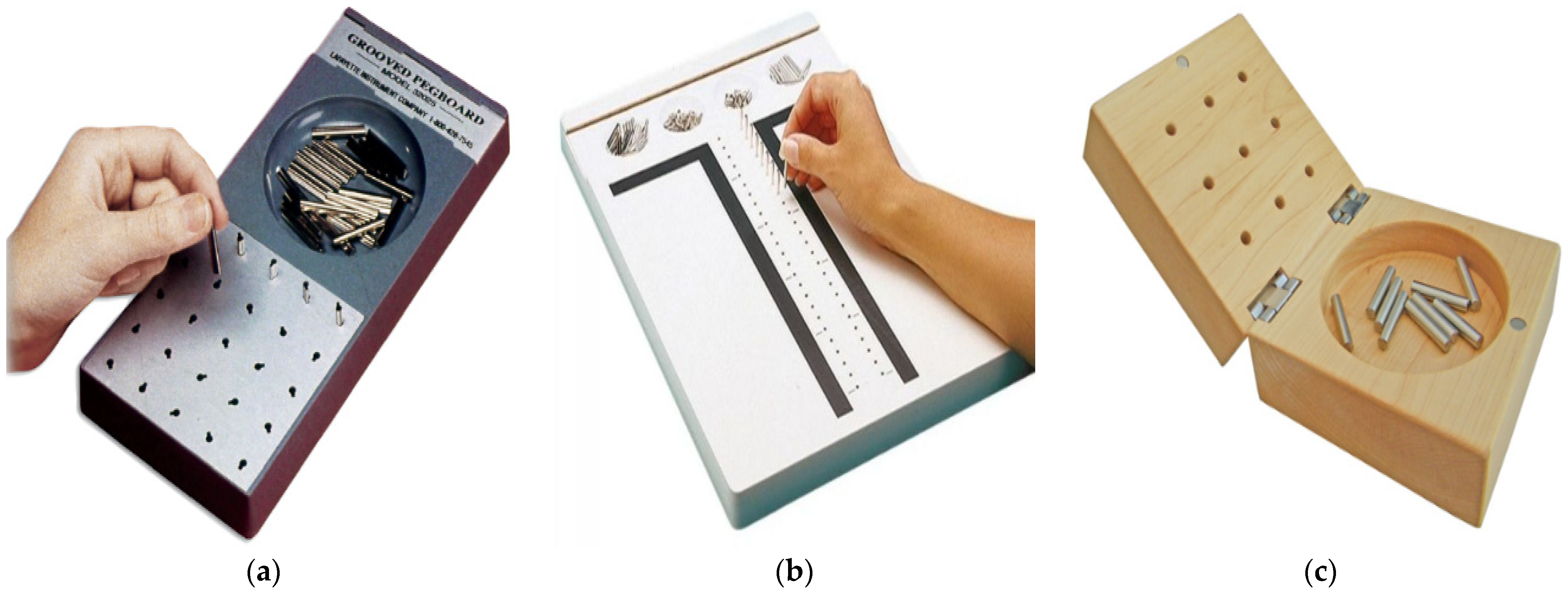
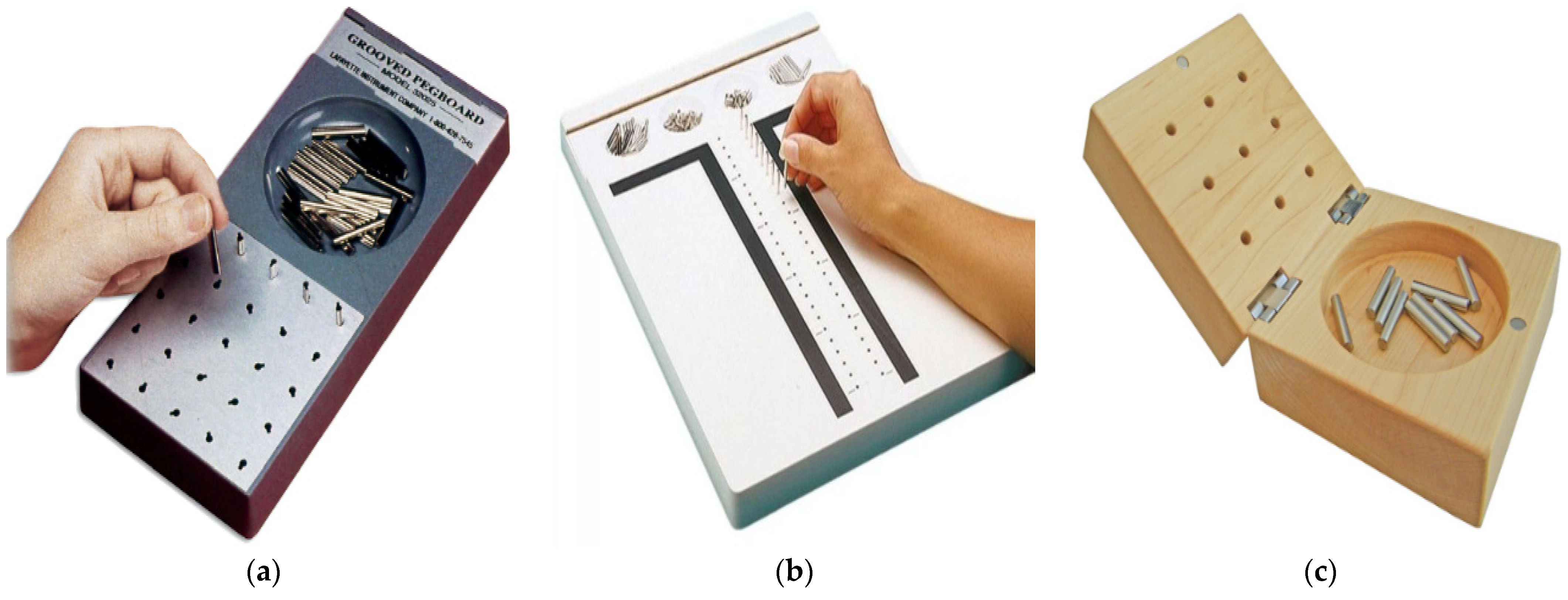
2.2. The GPT Board
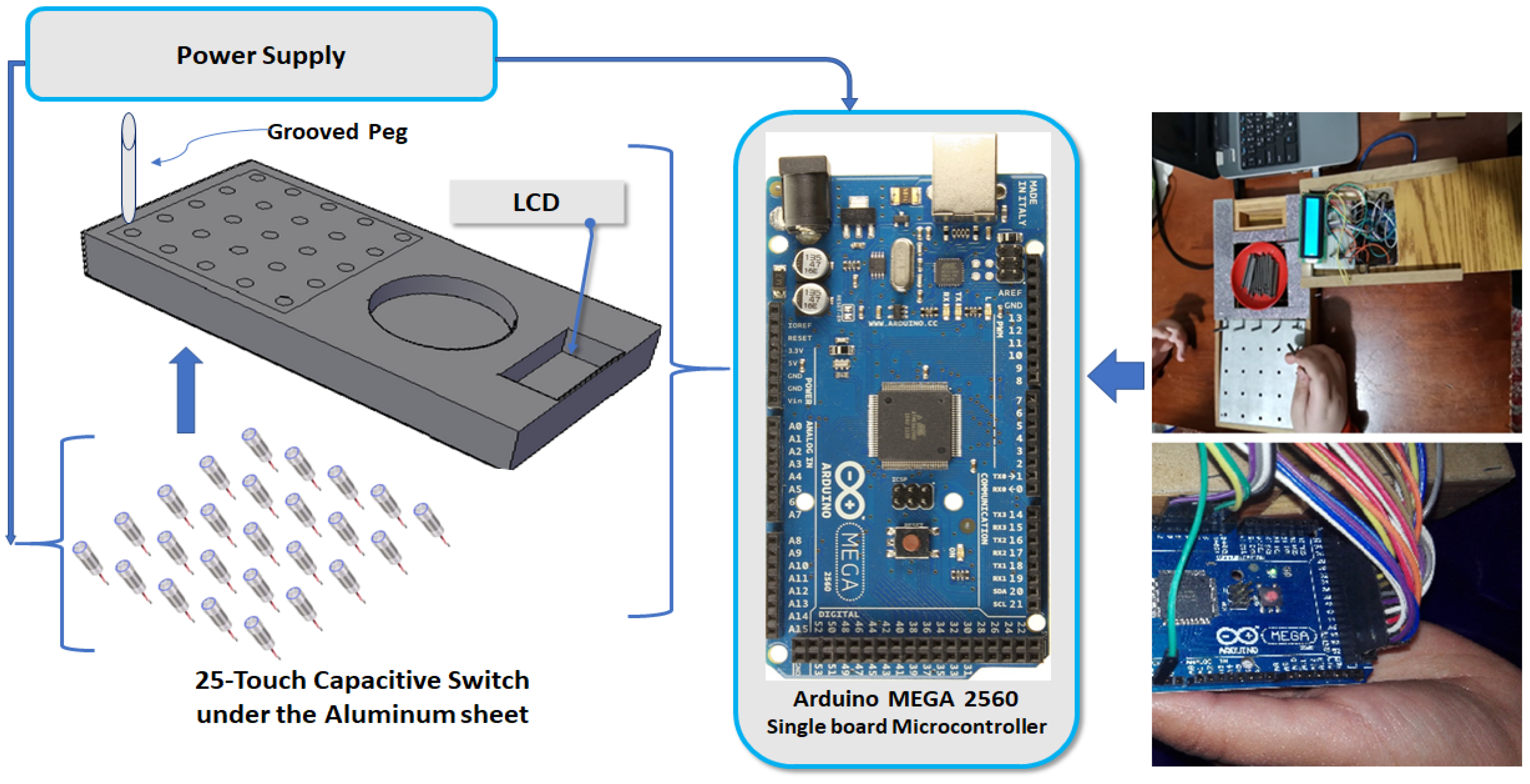
2.3. Electric Circuit
2.4. Participants
2.5. Procedures
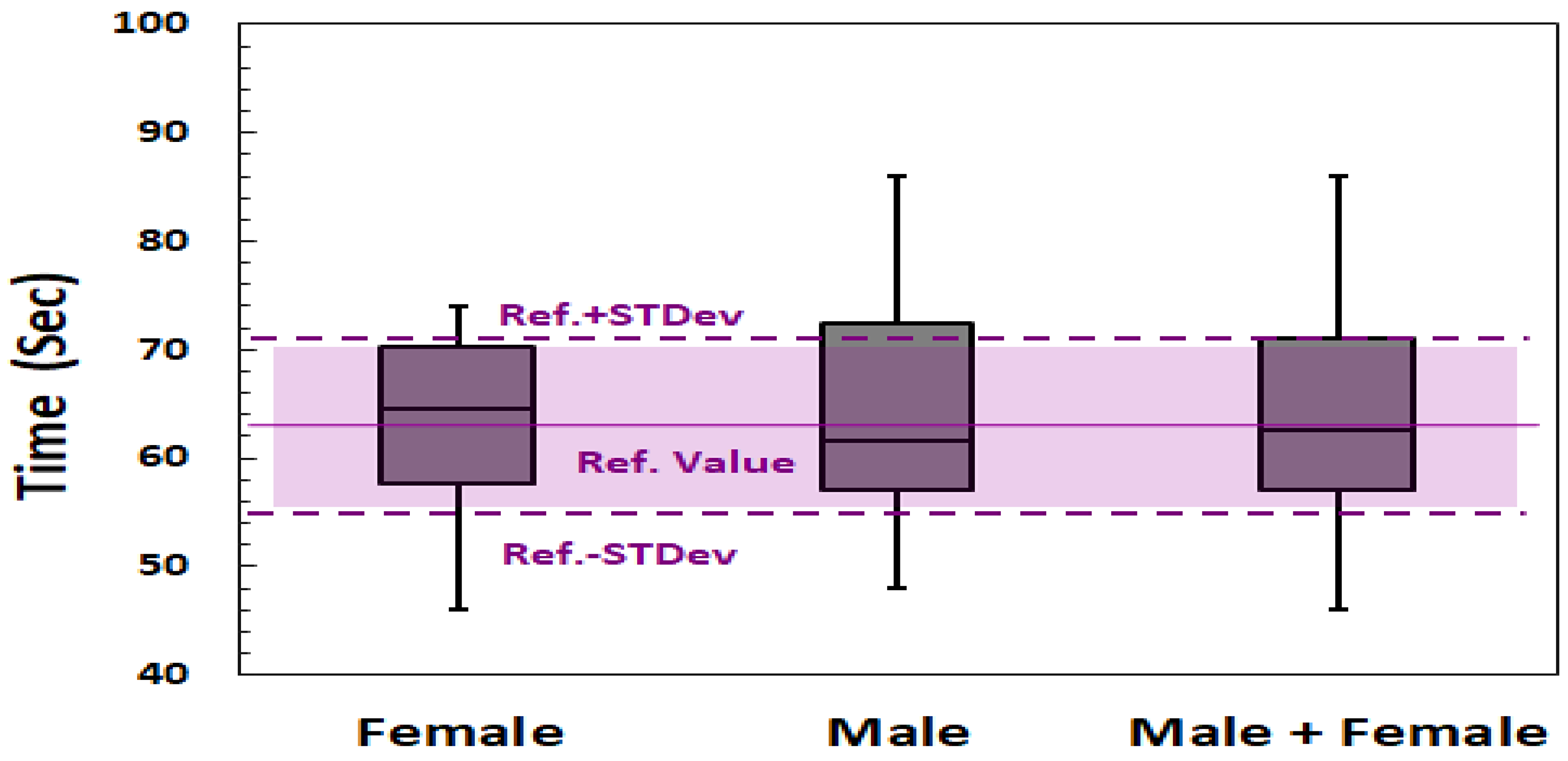
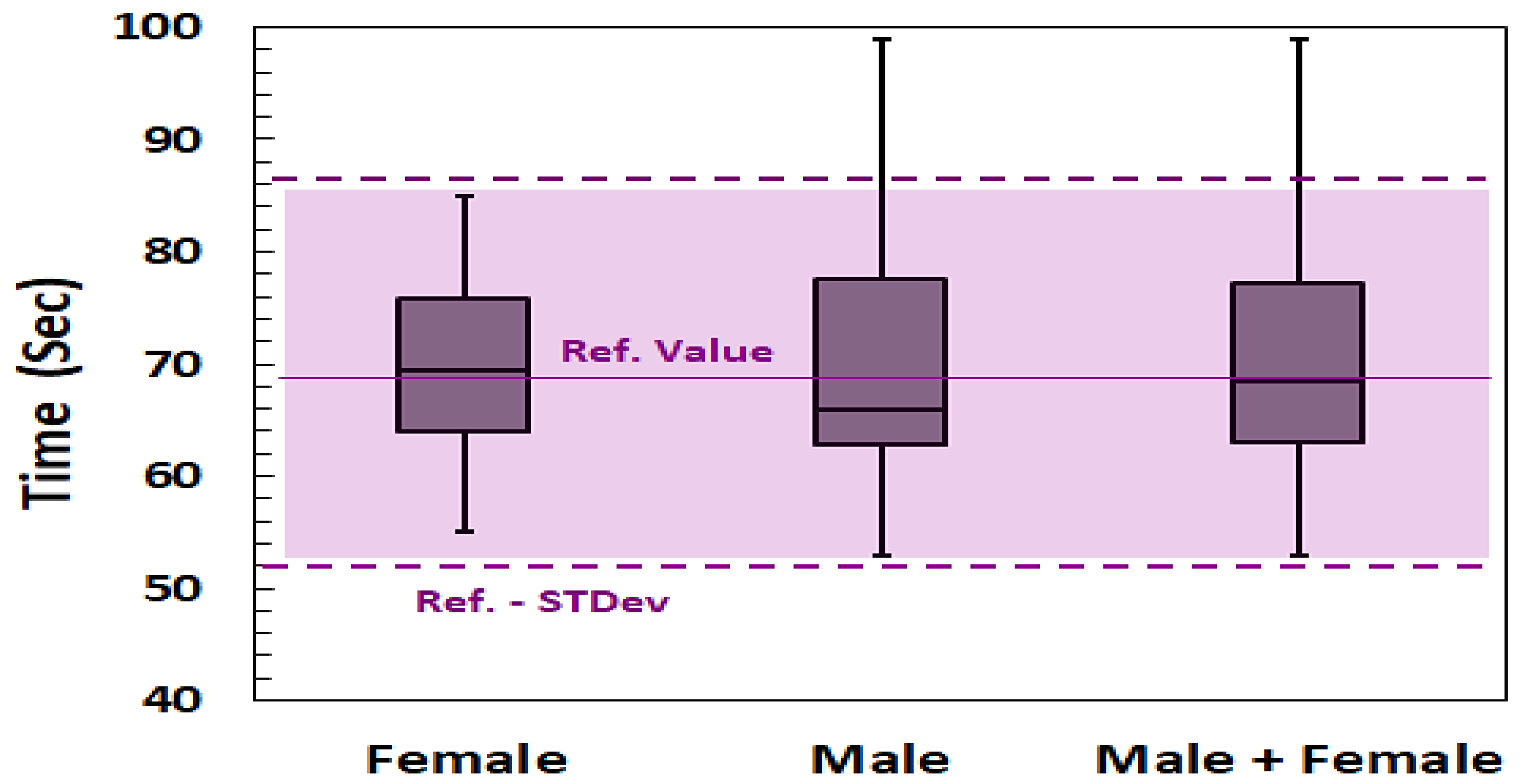
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Definition | Abbreviation |
|---|---|
| Grooved Pegboard Test | GPT |
| Liquid Crystal Display | LCD |
| Purdue Pegboard Test | PPT |
| Nine Holes Peg Test | NHPT |
| Institutional Review Board | IRB |
| Average | AVG |
| Standard Deviation | STDev |
| Cerebro-Vascular Accident | CVA |
| Cerebral Palsy | CP |
| Reference | Ref. |
References
- Lafayette Human Evaluation—Instruments. Available online: https://lafayetteevaluation.com/ (accessed on 7 June 2021).
- Amirjani, N.; Ashworth, N.L.; Olson, J.L.; Morhart, M.; Chan, K.M. Validity and reliability of the Purdue Pegboard Test in carpal tunnel syndrome. Muscle Nerve 2011, 43, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Desrosiers, J.; Hébert, R.; Bravo, G.; Dutil, E. The Purdue Pegboard Test: Normative data for people aged 60 and over. Disabil. Rehabil. 1995, 17, 217–224. [Google Scholar] [CrossRef] [PubMed]
- İnal, E.E.; Çarlı, A.B.; Çanak, S.; Aksu, O.; Köroğlu, B.K.; Savaş, S. Effects of hyperthyroidism on hand grip strength and function. J. Rehabil. Res. Dev. 2015, 52, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.; Neves, L.; Rodrigues, P.; Vasconcelos, O.; Castro, S.L. Orff-based music training enhances children’s manual dexterity and bimanual coordination. Front. Psychol. 2018, 9, 2616. [Google Scholar] [CrossRef] [PubMed]
- Servatius, R.J.; Spiegler, K.M.; Handy, J.D.; Pang, K.C.; Tsao, J.W.; Mazzola, C.A. Neurocognitive and fine motor deficits in asymptomatic adolescents during the subacute period after concussion. J. Neurotrauma 2018, 35, 1008–1014. [Google Scholar] [CrossRef]
- Lee, S.; Kim, Y.; Lee, B.H. Effect of virtual reality-based bilateral upper extremity training on upper extremity function after stroke: A randomized controlled clinical trial. Occup. Ther. Int. 2016, 23, 357–368. [Google Scholar] [CrossRef] [Green Version]
- Martirosov, S.; Bureš, M.; Zítka, T. Cyber sickness in low-immersive, semi-immersive, and fully immersive virtual reality. Virtual Real. 2021, 1–18. [Google Scholar] [CrossRef]
- Varley, B.J.; Shiner, C.T.; Johnson, L.; McNulty, P.A.; Thompson-Butel, A.G. Revisiting Poststroke Upper Limb Stratification: Resilience in a Larger Cohort. Neurorehabilit. Neural Repair 2021, 35, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Gaetani, F.; Primiceri, P.; Zappatore, G.A.; Visconti, P. Hardware design and software development of a motion control and driving system for transradial prosthesis based on a wireless myo-electric armband. IET Sci. Meas. Technol. 2019, 13, 354–362. [Google Scholar] [CrossRef]
- Petracca, M.; Droby, A.; El Mendili, M.M.; Paduri, S.; Graziano, N.; Saba, N.; Falcone, A.; Kurz, D.; Riley, C.; Howard, J.; et al. Sociodemographic features and disability in african-american and caucasian patients with multiple sclerosis. Mult. Scler. J. 2020, 26, 197–198. [Google Scholar] [CrossRef]
- Gogola, G.R.; Velleman, P.F.; Xu, S.; Morse, A.M.; Lacy, B.; Aaron, D. Hand dexterity in children: Administration and normative values of the functional dexterity test. J. Hand Surg. 2013, 38, 2426–2431. [Google Scholar] [CrossRef]
- Lafayette Instrument Grooved Pegboard Test. Available online: https://www.advys.be/docs/GroovedPegboardTestManual.pdf (accessed on 25 August 2021).
- Hamilton, L.D.; Mazzo, M.R.; Petrigna, L.; Ahmed, A.A.; Enoka, R.M. Poor Estimates of Motor Variability Are Associated with Longer Grooved Pegboard Times for Middle-Aged and Older Adults. J. Neurophysiol. 2019, 121, 588–601. [Google Scholar] [CrossRef]
- Petrigna, L.; Pajaujiene, S.; Iacona, G.M.; Thomas, E.; Paoli, A.; Bianco, A.; Palma, A. The Execution of the Grooved Pegboard Test in a Dual-Task Situation: A Pilot Study. Heliyon 2020, 6, e04678. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Magasi, S.R.; Bohannon, R.W.; Reuben, D.B.; McCreath, H.E.; Bubela, D.J.; Gershon, R.C.; Rymer, W.Z. Assessing Dexterity Function: A Comparison of Two Alternatives for the NIH Toolbox. J. Hand Ther. 2011, 24, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Almuklass, A.M.; Capobianco, R.A.; Feeney, D.F.; Alvarez, E.; Enoka, R.M. Sensory Nerve Stimulation Causes an Immediate Improvement in Motor Function of Persons with Multiple Sclerosis: A Pilot Study. Mult. Scler. Relat. Disord. 2020, 38, 101508. [Google Scholar] [CrossRef]
- Agarwal, S.; Pawlak, N.; Cucca, A.; Sharma, K.; Dobbs, B.; Shaw, M.; Charvet, L.; Biagioni, M. Remotely-Supervised Transcranial Direct Current Stimulation Paired with Cognitive Training in Parkinson’s Disease: An Open-Label Study. J. Clin. Neurosci. 2018, 57, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Mathiowetz, V.; Rogers, S.L.; Dowe-Keval, M.; Donahoe, L.; Rennells, C. The Purdue Pegboard: Norms for 14- to 19-Year-Olds. Am. J. Occup. Ther. 1986, 40, 174–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, A.J.; Miller, E.N.; Becker, J.T.; Selnes, O.A.; Cohen, B.A. Normative Data for Determining Significance of Test-Retest Differences on Eight Common Neuropsychological Instruments. Clin. Neuropsychol. 2004, 18, 373–384. [Google Scholar] [CrossRef]
- Hyngstrom, A.S.; Cho, C.C.; Barillas, R.B.; Joshi, M.; Rowley, T.W.; Keenan, K.G.; Staudenmayer, J.; Swartz, A.M.; Strath, S.J. Identification of Latent Classes of Motor Performance in a Heterogenous Population of Adults. Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100080. [Google Scholar] [CrossRef]
- Waliño-Paniagua, C.N.; Gómez-Calero, C.; Jiménez-Trujillo, M.I.; Aguirre-Tejedor, L.; Bermejo-Franco, A.; Ortiz-Gutiérrez, R.M.; Cano-De-La-Cuerda, R. Effects of a Game-Based Virtual Reality Video Capture Training Program Plus Occupational Therapy on Manual Dexterity in Patients with Multiple Sclerosis: A Randomized Controlled Trial. J. Healthc. Eng. 2019, 9780587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feys, P.; Lamers, I.; Francis, G.; Benedict, R.; Phillips, G.; Larocca, N.; Hudson, L.D.; Rudick, R. The Nine-Hole Peg Test as a Manual Dexterity Performance Measure for Multiple Sclerosis. Mult. Scler. 2017, 23, 711–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grice, K.O.; Vogel, K.A.; Le, V.; Mitchell, A.; Muniz, S.; Vollmer, M.A. Adult Norms for a Commercially Available Nine Hole Peg Test for Finger Dexterity. Am. J. Occup. Ther. 2003, 57, 570–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlova, E.L.; Borg, J. Impact of Tactile Sensation on Dexterity: A Cross-Sectional Study of Patients with Impaired Hand Function After Stroke. J. Mot. Behav. 2018, 50, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Jobbágy, Á.; Marik, A.R.; Fazekas, G. Quantification of the Upper Extremity Motor Functions of Stroke Patients Using a Smart Nine-Hole Peg Tester. J. Healthc. Eng. 2018, 7425858. [Google Scholar] [CrossRef] [Green Version]
- Arduino-Mega-2560. Arduino Company. Available online: https://www.arduino.cc/en/Guide/ArduinoMega2560 (accessed on 30 June 2021).
- Yang, L.; Zhang, F.; Zhu, J.; Fu, Y. A Portable Device for Hand Rehabilitation with Force Cognition: Design, Interaction and Experiment. IEEE Trans. Cogn. Dev. Syst. 2021. [Google Scholar] [CrossRef]
- Pawar, S.S.; Chougule, S.R. Predication and Analysis of Epileptic Seizure Neurological Disorder Using Intracranial Electroencephalography (IEEG). WSEAS Trans. Signal Process. 2021, 16, 197–205. [Google Scholar] [CrossRef]
- Davis Ojie, O.; Saatchi, R. Principal Component Analysis of the Modified Clinical Test Of sensory Interaction in Healthy Adult Humans. WSEAS Trans. Biol. Biomed. 2020, 17, 125–142. [Google Scholar] [CrossRef]

| Normal Participants | Abnormal Participants | ||
|---|---|---|---|
| Pathology | Normal | Neurology Disorders | Bone accidents |
| Women | 20 | 2 | 1 |
| Men | 20 | 2 | 1 |
| Total | 40 | 4 | 2 |
| Dominant Hands (s) | Non Dominant Hands (s) | |||
|---|---|---|---|---|
| AVG | STDev | AVG | STDev | |
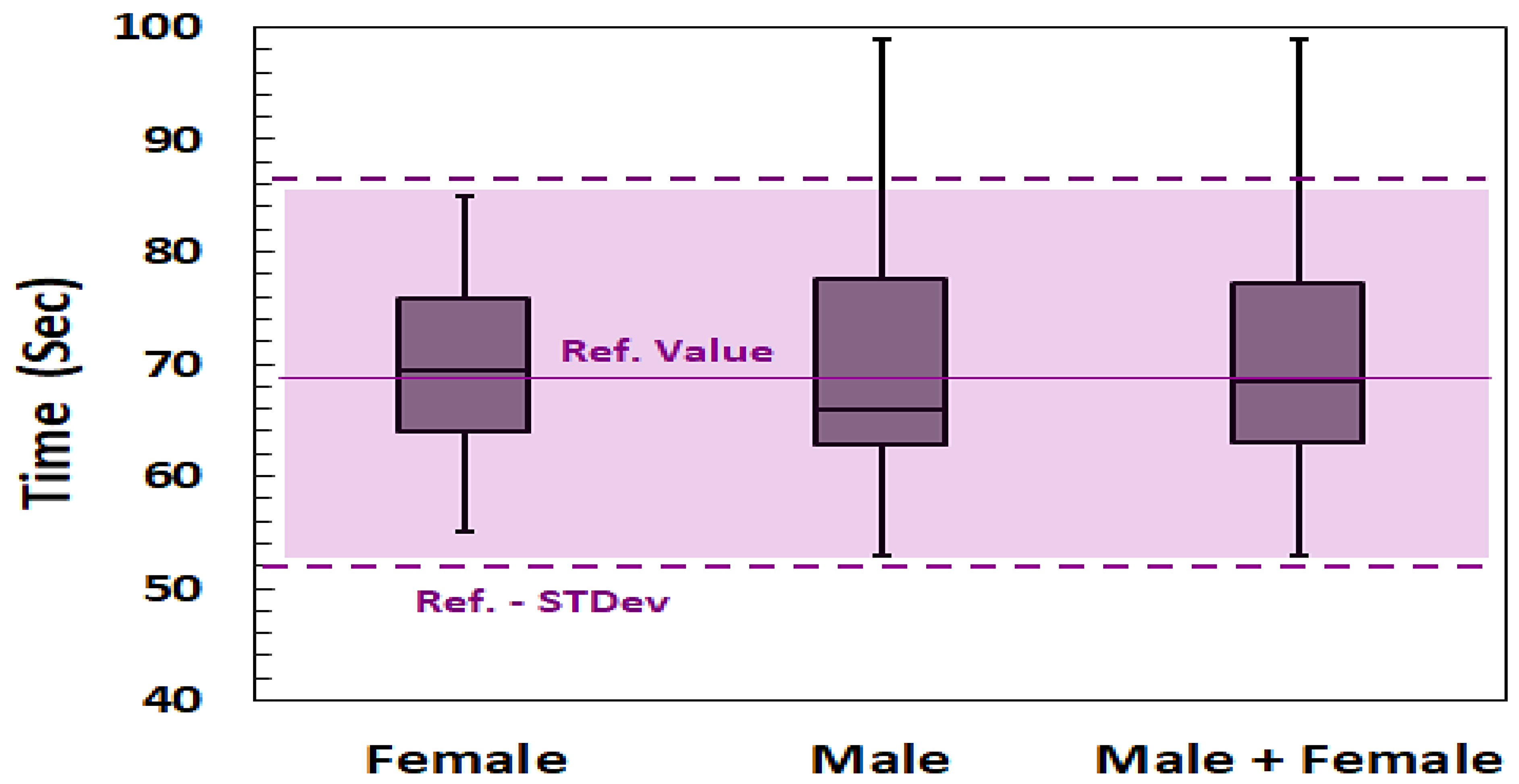
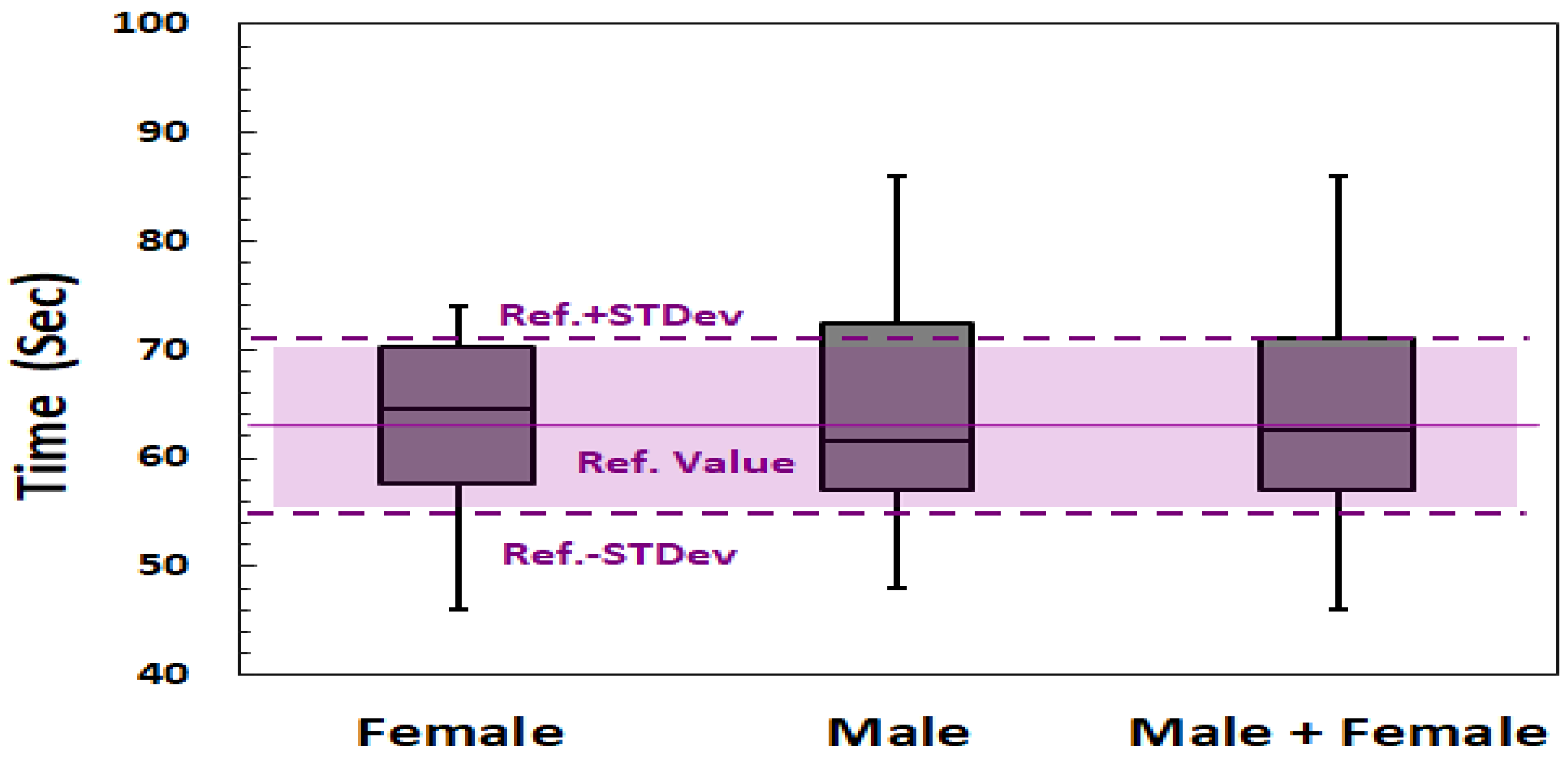
| Women (No. 20 participants) | 63.2 | 7.6 | 69.8 | 8.7 |
| Men (No. 20 participants) | 64.0 | 10.5 | 70.1 | 12.4 |
| Total (No. 40 Participants) | 63.6 | 9.1 | 69.9 | 10.6 |
| Population Mean Value [2] | 63.4 | 7.9 | 69.05 | 18.7 |
| p-value (Women) | 0.91 | 0.72 | ||
| p-value (Men) | 0.82 | 0.74 | ||
| p-value (Women + Men) | 0.90 | 0.62 | ||
| Medical Condition | Right Hand (s) | Left Hand (s) |
|---|---|---|
| Ataxia (in right hand) | 441 | 165 |
| Autism | 586 | 333 |
| Cerebrovascular accident (CVA) (Stroke in right hand) | 171 | 96 |
| Cerebral Palsy (CP) (in Right hand) | 567 | 421 |
| Patient no. 1: Bone Fracture (in left Hand) | 99 | 109 |
| Patient no. 2: Bone Fracture (in left Hand) | 85 | 184 |
| Limits of Population Mean Values from GPT devices [2] | Dominant Hand: 60.96–82.7 s Non-dominant hand: 65.61–87.95 s | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Naami, B.; Al-Naimat, F.; Almalty, A.-M.R.M.; Visconti, P.; Al-Hinnawi, A.-R. A Prototype of an Electronic Pegboard Test to Measure Hand-Time Dexterity with Impaired Hand Functionality. Appl. Syst. Innov. 2022, 5, 2. https://doi.org/10.3390/asi5010002
Al-Naami B, Al-Naimat F, Almalty A-MRM, Visconti P, Al-Hinnawi A-R. A Prototype of an Electronic Pegboard Test to Measure Hand-Time Dexterity with Impaired Hand Functionality. Applied System Innovation. 2022; 5(1):2. https://doi.org/10.3390/asi5010002
Chicago/Turabian StyleAl-Naami, Bassam, Feras Al-Naimat, Abdul-Majeed Raja M. Almalty, Paolo Visconti, and Abdel-Razzak Al-Hinnawi. 2022. "A Prototype of an Electronic Pegboard Test to Measure Hand-Time Dexterity with Impaired Hand Functionality" Applied System Innovation 5, no. 1: 2. https://doi.org/10.3390/asi5010002
APA StyleAl-Naami, B., Al-Naimat, F., Almalty, A.-M. R. M., Visconti, P., & Al-Hinnawi, A.-R. (2022). A Prototype of an Electronic Pegboard Test to Measure Hand-Time Dexterity with Impaired Hand Functionality. Applied System Innovation, 5(1), 2. https://doi.org/10.3390/asi5010002