Abstract
Background/Objectives: The management of localized prostate cancer with regional lymph node involvement (N1M0) presents significant clinical challenges. While once considered indicative of systemic disease, improved imaging and evolving treatment paradigms have redefined node-positive disease as potentially curable. This systematic review aims to assess current evidence regarding treatment modalities and outcomes for patients with localized N1M0 prostate cancer. Methods: A systematic review was conducted to identify studies evaluating therapeutic strategies for N1M0 prostate cancer. Eligible studies included randomized controlled trials, retrospective analyses, and consensus guidelines. Treatment approaches reviewed included radical prostatectomy (RP) with pelvic lymph node dissection (PLND), whole pelvic radiotherapy (WPRT), prostate-only radiotherapy (PORT), androgen deprivation therapy (ADT), and metastasis-directed therapy (MDT), including stereotactic body radiotherapy (SBRT). Key outcomes included overall survival (OS), biochemical recurrence-free survival (bRFS), disease-free survival (DFS), and treatment-related toxicity. Results: Multimodal approaches—particularly the combination of ADT with WPRT or adjuvant radiotherapy following RP—were associated with improved survival outcomes. Patients with limited nodal burden and undetectable postoperative prostate-specific antigen (PSA) levels derived the most benefit. The use of prostate-specific antigen membrane positron-emission tomography/computed tomography (PSMA PET/CT) enhanced detection and guided MDT in oligorecurrent disease. SBRT, simultaneous integrated boost (SIB), and hypofractionated regimens demonstrated promising efficacy with acceptable toxicity profiles. Conclusions: Node-positive localized prostate cancer is optimally managed with individualized, multidisciplinary strategies. Combining systemic and locoregional treatments improves outcomes in selected patients. Ongoing prospective studies are warranted to refine patient selection, optimize treatment sequencing, and integrate novel imaging and systemic agents.
1. Introduction
With advancements in imaging modalities, localized prostate cancer with nodal involvement is increasingly treated now as a locoregional spread of prostate cancer rather than a systemic disease.
Uniquely, for prostate cancer, there are numerous nomograms based primarily on prostate-specific antigen (PSA) levels, Gleason score (GS), clinical stage, and sometimes the percentage of positive biopsies to predict the probability of pelvic nodal metastasis according to risk stratification, which physicians can use to select patients for prophylactic nodal treatment when their risk exceeds a certain level (e.g., ≥15%) [1,2].
The Definition of Positive Lymph Nodes
The definition of positive lymph nodes in prostate cancer is grouped into three categories:
- Pathologically positive (pN+) lymph node metastasis, confirmed by pathology after Pelvic Lymph Node Dissection (PLND), which is considered the standard of care (SOC) for the diagnosis of positive lymph node disease in prostate cancer, or in rare cases, through nodal sampling;
- Clinically positive (cN+) lymph node metastasis suggested by imaging, with the advent of new nuclear imaging techniques, improves identification in this category. Unfortunately, despite these advances, up to one-third of lymph node metastases are still missed;
- Clinically negative (cN−) patients with high-risk features for lymph node involvement (LNI) can be readily identified using a host of validated formulas and nomograms.
2. Management of Pelvic Lymph Node Involvement
The selection of treatment modality for pelvic nodal involvement of prostate cancer is influenced by the management approach chosen for the primary tumors:
- In patients undergoing radical prostatectomy (RP), surgical options include either PLND or Extended Pelvic Lymph Node Dissection (ePLND);
- When radiation is the main treatment modality, whole pelvic radiotherapy (WPRT) with or without a nodal boost is considered the standard of care.
- (a)
- Surgical staging management
2.1. PLND vs. ePLND
The European Association of Urology (EAU) guidelines recommend ePLND for accurately staging the pelvis in patients with clinically confined prostate cancer (PCa) with a risk of nodal metastasis greater than 7% [3]. According to the American Urological Association (AUA) guidelines, PLND is advised for all patients at medium to high risk of nodal metastasis [4].
Fossati et al. [5] classified PLND into four types:
- Limited PLND (LPLND): Involves the obturator nodes;
- Standard PLND (SPLND): Involves the obturator and external iliac nodes; as shown in Figure 1
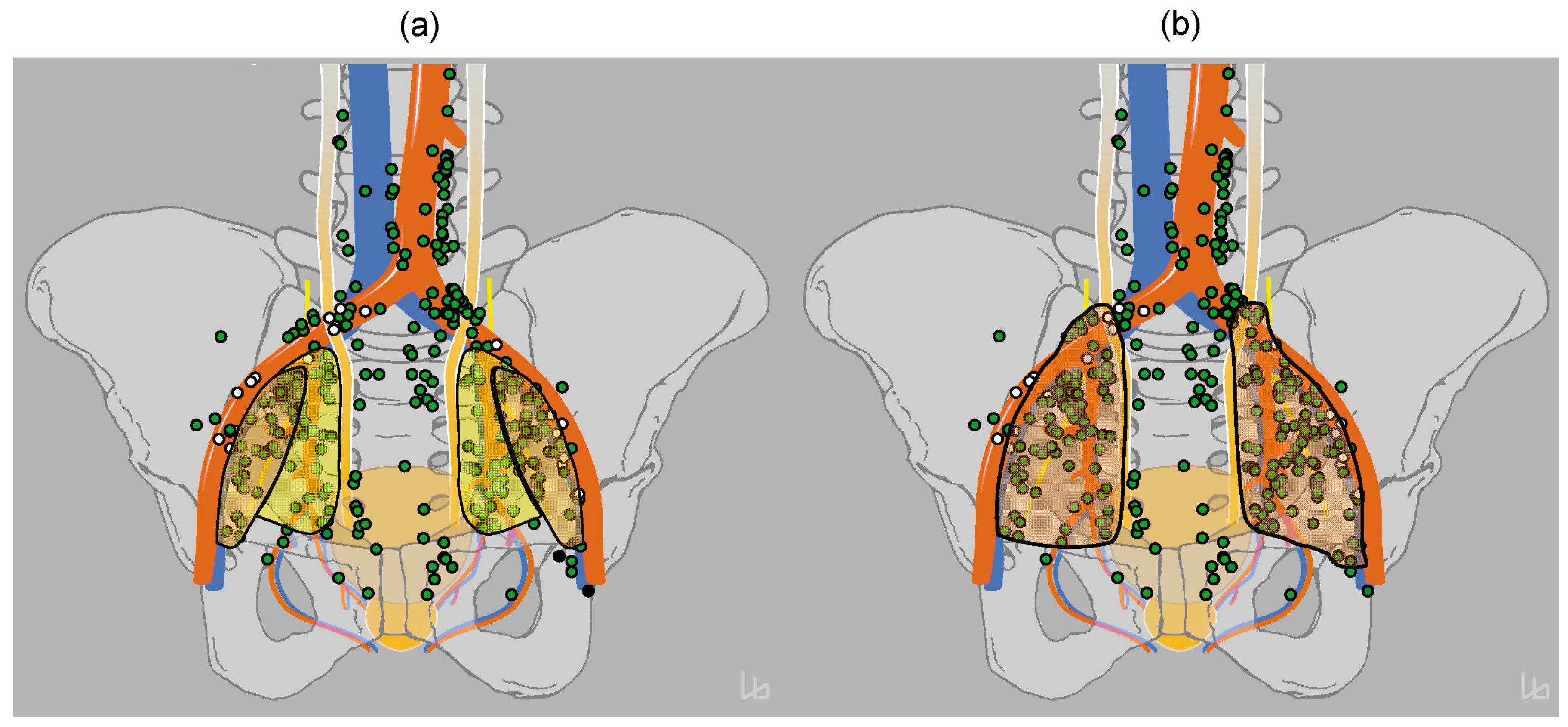
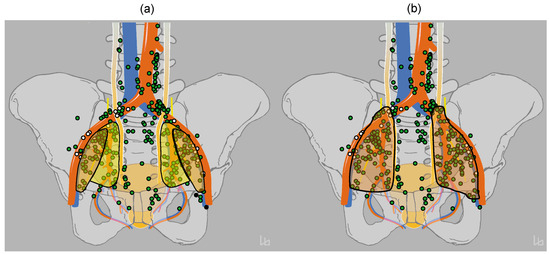 Figure 1. (a) Anatomical extent of classical extended pelvic lymphadenectomy (PLND) encompassing the nodes along the major pelvic vessels including the internal iliac, external iliac and obturator regions to the iliac bifurcation (yellow and orange areas). (b) Anatomical extent of proposed (new) extended PLND by Matti and colleagues extending along the common iliac vessels to the ureteric crossing (pale red area). From Mattei et al. [6].
Figure 1. (a) Anatomical extent of classical extended pelvic lymphadenectomy (PLND) encompassing the nodes along the major pelvic vessels including the internal iliac, external iliac and obturator regions to the iliac bifurcation (yellow and orange areas). (b) Anatomical extent of proposed (new) extended PLND by Matti and colleagues extending along the common iliac vessels to the ureteric crossing (pale red area). From Mattei et al. [6]. - ePLND: Involves the obturator, external, and internal iliac nodes;
- Super-extended PLND (SePLND): Encompasses ePLND plus common iliac, presacral, and/or other nodes.
The oncologic benefits of PLND for prostate cancer remain controversial, particularly due to the increased risks and complications associated with ePLND. While ePLND is more accurate in detecting metastatic lymph node involvement, it may not improve the oncologic outcomes and is associated with an increased risk of complications, particularly lymphocele.
Although in general, the surgical management of node-positive disease has been rather disappointing, it is now understood that in selected patients, more favorable outcomes have been reported, and surgical management appears to be feasible in reducing morbidity without compromising efficacy in patients undergoing unilateral resection of nodes, provided they have only unilateral disease as identified by prostate-specific antigen membrane positron-emission tomography (PSMA PET) [7,8,9].
An overview of the available guidelines for managing N1 disease is shown in Table 1.

Table 1.
Overview of available guidelines for management of N+ prostate cancer:
- (b)
- Nonsurgical management: (radiation therapy + systemic treatment):
- 1.
- Non-surgical management for patients with clinically node negative (cN0) at High Risk of lymph node metastasis (LNM) (i.e., Elective Nodal Irradiation)
For most solid tumors, prophylactic lymph node irradiation is considered a standard of care; however, in high-risk prostate cancer, it remains debatable practice with no universal consensus. Table 2 summarizes selected trials comparing prophylactic elective nodal irradiation (ENI) with prostate-only radiotherapy (PORT).
Table 2.
RCTs studied WPRT in cN0 disease in the primary setting evaluating prophylactic nodal radiotherapy.
A significant part of this controversy comes from the misconception among many physicians that two randomized controlled trials (Radiation Therapy Oncology Group [RTOG] 9413 and French Genitourinary Study Group [GETUG] 01) yielded “negative” results in terms of both biochemical failure-free survival (BFFS) and overall survival (OS). In reality, no trials have demonstrated definitively “negative” results for “prophylactic pelvic nodal radiotherapy”. Notably, the GETUG—01 trial did not actually use “whole pelvic” radiotherapy (but rather treated only the “true pelvis”) as defined by the RTOG. Additionally, it included too many low-risk patients and was far too small a study to assess any clinically meaningful endpoints [13].
2.1.1. GETUG-01
Pommier et al. studied 446 patients with T1b-T3, N0pNx, M0 prostate carcinoma randomized to receive either pelvic node and prostate or prostate-only radiation therapy. Patients were stratified into two groups: “low risk” (T1–T2, Gleason score 6, and PSA < 3× the upper limit of normal [ULN] of the laboratory) (92 patients) versus “high risk” (T3, Gleason score > 6, or PSA > 3× the ULN of the laboratory).
The investigators concluded that at a median follow-up of 11.4 years, the 10-year OS and event-free survival (EFS) were similar in the two treatment arms [14].
2.1.2. RTOG 9413
This study enrolled 1323 patients with a risk of LNI > 15% to evaluate the efficacy of WPRT versus PORT and to compare short-term neoadjuvant with adjuvant plus concurrent hormone therapy (HT), with the primary endpoint of progression-free survival [PFS] [18].
- 2.
- Non-surgical management for patients with cN + ve disease in the primary setting: Radiotherapeutic options
Pelvic lymph node metastasis is a strong predictor of systemic spreading, and thus we typically recommend a combination of systemic and local-regional radiotherapy. This recommendation is partly supported by an early report by Granfors et al. and by the more recent Systemic Therapy for Advanced or Metastatic Prostate cancer: Evaluation of Drug Efficacy (STAMPEDE) trial results [19,20].
The inadequacy of androgen deprivation therapy (ADT) alone has been evaluated in patients with locally advanced PCa in a randomized phase 3 trial conducted by the Scandinavian Prostate Cancer Group (SPCG). The SPCG-7 study showed that combining prostate radiotherapy with long-term hormone therapy was superior to long-term hormone therapy alone in terms of overall survival [21,22].
Table 3 summarizes the results of selected studies focusing on patients with N + M0 prostate cancer.
Table 3.
Overview of selected studies on treating localized prostate disease with node positive N + M0 disease:
3. Nodal Irradiation: Simultaneous Integrated Boost (SIB) and Hypofractionation
Based on previous evidence, WPRT combined with ADT is now considered the standard of care in clinically positive nodal prostate cancer. With the advent of modern biological imaging techniques, such as prostate-specific antigen membrane positron-emission tomography/computed tomography (PSMA PET/CT), it is likely that pelvic nodes will be detected earlier and more frequently. One efficient approach to treat node-positive disease with higher doses than uninvolved nodal areas is using a SIB to PSMA (prostate-specific membrane antigen)-positive nodes.
Onishi et al. [45] retrospectively analyzed 97 patients with clinically node-positive (cN1) prostate cancer who received intensity-modulated radiation therapy with SIB (SIB-IMRT). The investigators demonstrated favorable 5-year outcomes with low incidences of toxicity.
Recently, Basu et al. reported their findings on 22 patients with National Comprehensive Cancer Network (NCCN) high-risk (HR), N+, and oligometastatic (OM) PCa staged using prostate MRI and PSMA PET-CT who received SIB-SBRT (stereotactic body radiation therapy) [46]. The investigators found that SIB-SBRT for HR, N+, and OM prostate cancer achieved good biochemical control with minimal grade 3 toxicity.
Mizowaki et al. reported their experience with 52 patients with T2a-T4N1M0 prostate cancer, who were definitively treated with whole pelvis (WP) SIB-IMRT. The investigators reported very promising results, with excellent biochemical recurrence-free survival (bRFS), distant metastasis-free survival (MFS), OS, and prostate cancer-specific survival rates (PCCS) (69%, 78%, 88%, and 92%, respectively) at 5 years. In addition, the 5-year cumulative incidence rates for grade 2–3 late genitourinary (GU) and gastrointestinal (GI) toxicities were both 2%, with no grade 4 acute or late toxicity [47].
4. Patients with pN1 Disease in the Postoperative Setting
The EAU guidelines consider ePLND the standard of care and the most accurate staging procedure after RP, despite advancements in molecular imaging techniques [10]
Several retrospective studies recommend adding postoperative WPRT to ADT [40,48] especially for patients with between two and four positive nodes after nodal dissection [49]. These studies suggest that both PCSS and OS are improved when ADT is combined with WPRT compared with ADT alone [41,49,50]. However, to date, no randomized controlled study has explicitly tested the role of adjuvant radiotherapy (RT) in node-positive patients after RP and ePLND.
5. The Postoperative Salvage Setting: N + ve Disease
Salvage radiotherapy is the only curative treatment in the setting of biochemical recurrence after prostatectomy and no evidence of distant metastasis [51,52]. As pelvic nodes are among the most common sites of recurrence after RP, WPRT is almost a standard of care in the salvage setting and is supported by numerous prospective and retrospective trials [51,52,53].
6. The Case for Nodal Recurrence (rN + ve) Patients
ADT is generally considered a gold standard in patients with nodal recurrences after primary treatment for prostate cancer [24,54]. Emerging evidence supports the use of radiation therapy in oligorecurrent nodal disease, especially when combined with molecular imaging for localization of nodal recurrences.
7. SBRT in Oligometastatic Nodal Recurrence
Oligorecurrent (or “metachronous” oligometastatic) disease typically shows better outcomes than synchronous oligometastases, likely due to its more indolent biology and more lymphotropic pattern of recurrence [55].
Clinical evidence suggests that patients who develop metastases after 2 years or more of the treatment of the primary tumor tend to have better survival rates compared to those with early recurrence, indicating slower growing.
Although no level I evidence from phase 3 randomized trials exists specifically for oligometastatic prostate cancer, several prospective phase 1 and 2 clinical trials support the use of SBRT in this setting [56,57].
Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastases (SABR-COMET) was the first phase 2 randomized trial to show a significant benefit in OS and PFS for SBRT combined with SOC compared with SOC alone, a benefit that persists with a long-term follow-up (8 yr OS, 27.2% vs. 13.6%; 8 yr PFS, 21.3% vs. 0.0%) [58]. This trial has been criticized for including only 16 patients with PCa, 14 of whom received SBRT.
Table 4 summarizes selected phase 2 clinical trials, Surveillance or metastasis-directed Therapy for OligoMetastatic Prostate cancer recurrence (STOMP) and Observation versus stereotactic ablative RadiatIon for OLigometastatic prostate CancEr (ORIOLE), which provided the best “proof-of-principle” evidence supporting the use of SBRT in oligorecurrent disease.
Table 4.
Selected trials of metastasis directed therapy (MDT) in oligorecurrent prostate cancer.
The long-term outcomes of pooled data from both trials have been published [64]. With a median follow-up time of 52.5 months for the entire group, metastasis-directed therapy (MDT) remained associated with improved PFS compared to observation (pooled HR, 0.44; 95% CI, 0.29–0.66; p = 0.001). Interestingly, the PFS beyond 4 years was 15–20% with SBRT, suggesting that a good number of patients will benefit from a durable response with MDT. Although a further follow-up is needed, these encouraging results indicate that in appropriately selected patients, MDT (and specifically SBRT) without systemic therapy might be an alternative approach in well-informed patients wishing to avoid the side effects of ADT.
Also, it should be noted that despite the significant result of the ORIOLE trial, it had only four patients, emphasizing its potential impact on the generalizability of the study’s conclusions.
It seems reasonable to suggest that if the primary goals of SBRT in nodal oligorecurrent PCa are to achieve local control, prevent further metastasis, and delay subsequent systemic treatment escalation in selected patients, we should define our endpoints accordingly. A relevant issue that deserves further investigation is whether metastases-free survival, as measured by conventional imaging, can also act as a proxy for overall survival in patients with hormone-sensitive oligorecurrent PCa detected through molecular imaging.
8. Combined RT and Systemic Therapy
Some authors have investigated the use of MDT without ADT, despite being the current SOC for nodal oligorecurrence [65].
The results of these studies suggest that this approach could be a reasonable option in well-selected subgroups of patients in whom the main objective is to delay the effects of androgen suppression. However, the omission of ADT may compromise long-term survival [66].
Preclinical studies suggest that the synergistic effects and anti-neoangiogenic effects of ADT may contribute to normalizing irradiation and oxygenation of the tumor microenvironment, thereby enhancing the effectiveness of RT [67,68,69]. Deprivation therapy (DT) clearly plays a role in controlling distant micrometastasis and, consequently, reduces the risk of distant failure and improves outcomes in oligorecurrent disease [67,68,69].
9. Volume of Treatment and RT Scheme: SBRT vs. Elective Nodal Radiotherapy (ENRT)
It can be argued that using generous lymph node coverage, like ENRT with an additional SBRT boost, can reduce the likelihood of subsequent pelvic nodal recurrences and thus improve outcomes compared to SBRT alone. Although there is no prospective randomized trial conclusively defining the optimal radiotherapy strategy in oligo-nodal recurrence, available evidence for the use of ENRT is derived from retrospective and nonrandomized prospective studies, with wide variability in radiotherapy doses and schedules.
The Salvage Treatment of OligoRecurrent nodal prostate cancer Metastases (STORM) study, a randomized trial designed to compare both strategies, in addition to a 6-month regimen of ADT, has reported preliminary results indicating similar toxicity profiles, though the final results are awaited to assess differences in PFS [70]. Therefore, there remain unanswered questions regarding
- Localized treatment (SBRT) or more extensive radiotherapy (ENRT);
- The combination of these radiotherapies with ADT and/or androgen receptor pathway inhibitors (ARPIs);
- The optimal timing and duration of such treatments.
The “standard of care” for these patients who experience a recurrence in non-regional nodes is the combination of ADT and ARPIs without local therapy. However, recent data have shown definitive radiotherapy in combination with limited ADT is likely to be a more effective strategy.
10. Ongoing Trials and Future Directions
The number of metastases detected on prostate-specific antigen membrane positron-emission tomography (PSMA-PET) currently serves as the selection criterion for the indication of MDT in PCa [71]. Some patients, particularly those who have not received systemic treatment, experience rapid widespread metastatic progression. Fortunately, there is increasing interest in investigating biomarkers that could help identify and select which patients would benefit from treatment intensification [72].
Ongoing trials are exploring the efficacy of MDT combined with ADT and/or androgen receptor signaling inhibitors (ARSIs), using an intermittent approach instead of a continuous one. This approach has the advantage of providing treatment breaks from hormonal manipulation, which positively impacts patient quality of life (QoL) while potentially preventing or delaying the development of widespread metastases [73].
11. Toxicity of Radiotherapy
- Late GU toxicity: Theoretically, whole pelvic radiotherapy may increase toxicity compared with prostate-only radiotherapy [74]. There are discrepancies among studies regarding how much late GU toxicity there is, with some studies using advanced technologies reporting no significant difference in late GU toxicity with PORT versus WPRT at an intermediate dose [75,76,77,78]. In contrast, another study found a 40% increase in late GU toxicity with WPRT [16]
- Late GI toxicity: Similar inconsistencies exist with late GI toxicity. Although the GETUG-01 trial [14] did not report any excess late GI toxicity, the RTOG 9413 trial [13] found significantly worse GI toxicity with WPRT versus PORT (5.1% vs. 1.9%). Tharmalingam and colleagues confirmed this significant increase in late GI toxicity (≥grade 2) [16]. However, both studies involved patients treated before the routine use of 3D conformal EBRT.
- Hematological toxicity: Data on hematological toxicity are limited, and there were few ≥ grade 3 toxicities reported in the RTOG 9413 trial [13]. WPRT can result in lower absolute lymphocyte and white blood cell counts from baseline 1 year after treatment, particularly in smokers and in patients with low baseline lymphocyte counts. In such cases, the volume of ilium bone marrow receiving 40 Gray is a strong predictor of developing late lymphopenia [77]. WPRT increased late ≥grade 2 hematological toxicities, although absolute numbers remained low (29 [5%] of 570 patients) compared to prostate bed radiotherapy (27 [2%] of 1125 patients) [53]. Patient-reported toxicity scoring indicated more frequent bowel movements, loose stools, fecal urgency, and gas passage with WPRT [74].
12. Impact of Using Modern Radiotherapy Techniques on Toxicity
Advanced radiotherapy techniques appear to decrease both acute and late toxicity compared to traditional techniques. In general, trials using intensity-modulated radiation therapy (IMRT) or volumetric-modulated arc therapy (VMAT) report very low rates of severe toxicity, even when applying higher doses to the pelvis [16,74].
This is evident in the Prostate-Only Versus Whole-Pelvic Radiation Therapy in High-Risk and Very High-Risk Prostate Cancer (POP-RT) trial as it found a doubling of late GU toxicities, which is associated with the higher doses to the pelvis. However, no toxicities higher than grade 4 occurred, and grade 3 toxicities occurred in less than 2% of the patients (2 of 112), regardless of the treatment group [15] This low rate of ≥grade 3 toxicities has been confirmed by other studies.
Dosimetric studies showed that intensity-modulated proton therapy significantly reduces the dose to the bladder, small bowel, large bowel, and rectum compared with volumetric arc therapy [15]. However, it is still unclear whether these dosimetric advantages translate into meaningful clinical benefits in terms of reduced late toxicity. A registry study involving patients treated with pelvic proton therapy showed that intestinal and urinary toxicities were infrequent after a short follow-up of 14 months [75].
13. Additional Systemic Treatment
Combining ADT with docetaxel or second-generation hormone treatment is well established in the metastatic PCa setting [79,80]. Recently, these drugs have been studied in nonmetastatic PCa, demonstrating promising results [81].
Three trials—the STAMPEDE platform protocol, the NRG Oncology/RTOG 0512 trial, and the GETUG-12 trial—investigated the effect of adding adjuvant docetaxel to ADT. The studies found that adjuvant docetaxel combined with ADT prolonged time to relapse but not MFS or OS.
14. Conclusions
There are growing reasons for optimism about the management of node-positive prostate cancer. With advancements in therapeutic strategies, we are now better equipped to define patients at risk and balance the risks and benefits of aggressive treatment for this population of patients.
Author Contributions
Conceptualization, H.S. and M.R.3rd; methodology H.S. and M.R.3rd, software, H.S. and M.R.3rd; validation, H.S. and M.R.3rd; formal analysis, H.S. and M.R.3rd; investigation, H.S. and M.R.3rd; resources, H.S. and M.R.3rd; data curation H.S. and M.R.3rd; writing—original draft preparation, H.S. and M.R.3rd; writing—review and editing, H.S., M.R.3rd and E.E.E. visualization, H.S., M.R.3rd and E.E.E. supervision, M.R.3rd. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare that there are no conflicts of interest that could be perceived as prejudicing the impartiality of this review.
References
- Morikawa, L.K.; Roach, M., III. Pelvic nodal radiotherapy in patients with unfavorable intermediate and high-risk prostate cancer: Evidence, rationale, and future directions. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Zamboglou, C.; Peeken, J.C.; Janbain, A.; Katsahian, S.; Strouthos, I.; Ferentinos, K.; Farolfi, A.; Koerber, S.A.; Debus, J.; Vogel, M.E. Development and validation of a multi-institutional nomogram of outcomes for PSMA-PET–based salvage radiotherapy for recurrent prostate cancer. JAMA Netw. Open 2023, 6, e2314748. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; van den Bergh, R.C.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer—2020 update. Part 1: Screening, diagnosis, and local treatment with curative intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Sanda, M.G.; Cadeddu, J.A.; Kirkby, E.; Chen, R.C.; Crispino, T.; Fontanarosa, J.; Freedland, S.J.; Greene, K.; Klotz, L.H.; Makarov, D.V. Clinically localized prostate cancer: AUA/ASTRO/SUO guideline. Part I: Risk stratification, shared decision making, and care options. J. Urol. 2018, 199, 683–690. [Google Scholar] [CrossRef]
- Fossati, N.; Willemse, P.-P.M.; Van den Broeck, T.; van den Bergh, R.C.; Yuan, C.Y.; Briers, E.; Bellmunt, J.; Bolla, M.; Cornford, P.; De Santis, M. The benefits and harms of different extents of lymph node dissection during radical prostatectomy for prostate cancer: A systematic review. Eur. Urol. 2017, 72, 84–109. [Google Scholar] [CrossRef]
- Mattei, A.; Fuechsel, F.G.; Bhatta Dhar, N.; Warncke, S.H.; Thalmann, G.N.; Krause, T.; Studer, U.E. The template of the primary lymphatic landing sites of the prostate should be revisited: Results of a multimodality mapping study. Eur. Urol. 2008, 53, 118–125. [Google Scholar] [CrossRef]
- Van Eecke, H.; Devos, G.; Vansevenant, B.; Vander Stichele, A.; Devlies, W.; Berghen, C.; Everaerts, W.; De Meerleer, G.; Joniau, S. Defining the optimal template of salvage lymph node dissection for unilateral pelvic nodal recurrence of prostate cancer following radical prostatectomy. Int. J. Urol. 2023, 30, 92–99. [Google Scholar] [CrossRef]
- Quhal, F.; Bryniarski, P.; Rivas, J.G.; Gandaglia, G.; Shariat, S.F.; Rajwa, P. Salvage lymphadenectomy after primary therapy with curative intent for prostate cancer. Curr. Opin. Urol. 2023, 33, 269–273. [Google Scholar] [CrossRef]
- Ambrosini, F.; Falkenbach, F.; Budaeus, L.; Graefen, M.; Koehler, D.; Lischewski, F.; Gschwend, J.E.; Heck, M.; Eiber, M.; Knipper, S. Prevalence of bilateral loco-regional spread in unilateral pelvic PSMA PET positive recurrent prostate cancer. Minerva Urol. Nephrol. 2023, 75, 734–742. [Google Scholar] [CrossRef]
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; De Santis, M.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef]
- Lieng, H.; Kneebone, A.; Hayden, A.J.; Christie, D.R.H.; Davis, B.J.; Eade, T.N.; Emmett, L.; Holt, T.; Hruby, G.; Pryor, D.; et al. Radiotherapy for node-positive prostate cancer: 2019 Recommendations of the Australian and New Zealand Radiation Oncology Genito-Urinary group. Radiother. Oncol. 2019, 140, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; et al. NCCN Guidelines® Insights: Prostate Cancer, Version 1.2023. J. Natl. Compr. Cancer Netw. 2022, 20, 1288–1298. [Google Scholar]
- Roach, M.; Moughan, J.; Lawton, C.A.; Dicker, A.P.; Zeitzer, K.L.; Gore, E.M.; Kwok, Y.; Seider, M.J.; Hsu, I.-C.; Hartford, A.C. Sequence of hormonal therapy and radiotherapy field size in unfavourable, localised prostate cancer (NRG/RTOG 9413): Long-term results of a randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1504–1515. [Google Scholar] [CrossRef] [PubMed]
- Pommier, P.; Chabaud, S.; Lagrange, J.L.; Richaud, P.; Le Prise, E.; Wagner, J.P.; Azria, D.; Beckendorf, V.; Suchaud, J.P.; Bernier, V.; et al. Is There a Role for Pelvic Irradiation in Localized Prostate Adenocarcinoma? Update of the Long-Term Survival Results of the GETUG-01 Randomized Study. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 759–769. [Google Scholar] [CrossRef]
- Murthy, V.; Maitre, P.; Kannan, S.; Panigrahi, G.; Krishnatry, R.; Bakshi, G.; Prakash, G.; Pal, M.; Menon, S.; Phurailatpam, R.; et al. Prostate-Only Versus Whole-Pelvic Radiation Therapy in High-Risk and Very High-Risk Prostate Cancer (POP-RT): Outcomes From Phase III Randomized Controlled Trial. J. Clin. Oncol. 2021, 39, 1234–1242. [Google Scholar] [CrossRef]
- Tharmalingam, H.; Tsang, Y.; Choudhury, A.; Alonzi, R.; Wylie, J.; Ahmed, I.; Henry, A.; Heath, C.; Hoskin, P.J. External Beam Radiation Therapy (EBRT) and High-Dose-Rate (HDR) Brachytherapy for Intermediate and High-Risk Prostate Cancer: The Impact of EBRT Volume. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 525–533. [Google Scholar] [CrossRef]
- Dearnaley, D.; Griffin, C.L.; Lewis, R.; Mayles, P.; Mayles, H.; Naismith, O.F.; Harris, V.; Scrase, C.D.; Staffurth, J.; Syndikus, I.; et al. Toxicity and Patient-Reported Outcomes of a Phase 2 Randomized Trial of Prostate and Pelvic Lymph Node Versus Prostate only Radiotherapy in Advanced Localised Prostate Cancer (PIVOTAL). Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 605–617. [Google Scholar] [CrossRef]
- Roach, M., III; DeSilvio, M.; Lawton, C.; Uhl, V.; Machtay, M.; Seider, M.; Rotman, M.; Jones, C.; Asbell, S.; Valicenti, R. Phase III trial comparing whole-pelvic versus prostate-only radiotherapy and neoadjuvant versus adjuvant combined androgen suppression: Radiation Therapy Oncology Group 9413. J. Clin. Oncol. 2003, 21, 1904–1911. [Google Scholar] [CrossRef]
- Granfors, T.; Modig, H.; Damber, J.-E.; Tomic, R. Long-term followup of a randomized study of locally advanced prostate cancer treated with combined orchiectomy and external radiotherapy versus radiotherapy alone. J. Urol. 2006, 176, 544–547. [Google Scholar] [CrossRef]
- Parker, C.C.; James, N.D.; Brawley, C.D.; Clarke, N.W.; Hoyle, A.P.; Ali, A.; Ritchie, A.W.; Attard, G.; Chowdhury, S.; Cross, W. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomised controlled phase 3 trial. Lancet 2018, 392, 2353–2366. [Google Scholar] [CrossRef]
- Widmark, A.; Klepp, O.; Solberg, A.; Damber, J.-E.; Angelsen, A.; Fransson, P.; Lund, J.-Å.; Tasdemir, I.; Hoyer, M.; Wiklund, F. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7/SFUO-3): An open randomised phase III trial. Lancet 2009, 373, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Mason, M.D.; Parulekar, W.R.; Sydes, M.R.; Brundage, M.; Kirkbride, P.; Gospodarowicz, M.; Cowan, R.; Kostashuk, E.C.; Anderson, J.; Swanson, G. Final report of the intergroup randomized study of combined androgen-deprivation therapy plus radiotherapy versus androgen-deprivation therapy alone in locally advanced prostate cancer. J. Clin. Oncol. 2015, 33, 2143–2150. [Google Scholar] [CrossRef]
- Schröder, F.H.; Kurth, K.H.; Fossa, S.D.; Hoekstra, W.; Karthaus, P.P.; De Prijck, L.; Collette, L. Early versus delayed endocrine treatment of T2-T3 pN1-3 M0 prostate cancer without local treatment of the primary tumour: Final results of European Organisation for the Research and Treatment of Cancer protocol 30846 after 13 years of follow-up (a randomised controlled trial). Eur. Urol. 2009, 55, 14–22. [Google Scholar] [PubMed]
- Messing, E.M.; Manola, J.; Yao, J.; Kiernan, M.; Crawford, D.; Wilding, G.; di’SantAgnese, P.A.; Trump, D. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol. 2006, 7, 472–479. [Google Scholar] [CrossRef]
- Pilepich, M.V.; Winter, K.; Lawton, C.A.; Krisch, R.E.; Wolkov, H.B.; Movsas, B.; Hug, E.B.; Asbell, S.O.; Grignon, D. Androgen suppression adjuvant to definitive radiotherapy in prostate carcinoma--long-term results of phase III RTOG 85-31. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 1285–1290. [Google Scholar] [CrossRef]
- Tward, J.D.; Kokeny, K.E.; Shrieve, D.C. Radiation therapy for clinically node-positive prostate adenocarcinoma is correlated with improved overall and prostate cancer-specific survival. Pr. Radiat. Oncol. 2013, 3, 234–240. [Google Scholar] [CrossRef]
- Tilki, D.; Chen, M.H.; Wu, J.; Huland, H.; Graefen, M.; Wiegel, T.; Böhmer, D.; Mohamad, O.; Cowan, J.E.; Feng, F.Y.; et al. Adjuvant Versus Early Salvage Radiation Therapy for Men at High Risk for Recurrence Following Radical Prostatectomy for Prostate Cancer and the Risk of Death. J. Clin. Oncol. 2021, 39, 2284–2293. [Google Scholar] [CrossRef] [PubMed]
- Fonteyne, V.; Van Praet, C.; Ost, P.; Van Bruwaene, S.; Liefhooghe, N.; Berghen, C.; De Meerleer, G.; Vanneste, B.; Verbaeys, C.; Verbeke, S.; et al. Evaluating the Impact of Prostate Only Versus Pelvic Radiotherapy for Pathological Node-positive Prostate Cancer: First Results from the Multicenter Phase 3 PROPER Trial. Eur. Urol. Focus 2023, 9, 317–324. [Google Scholar] [CrossRef]
- Da Pozzo, L.F.; Cozzarini, C.; Briganti, A.; Suardi, N.; Salonia, A.; Bertini, R.; Gallina, A.; Bianchi, M.; Fantini, G.V.; Bolognesi, A.; et al. Long-Term Follow-up of Patients with Prostate Cancer and Nodal Metastases Treated by Pelvic Lymphadenectomy and Radical Prostatectomy: The Positive Impact of Adjuvant Radiotherapy. Eur. Urol. 2009, 55, 1003–1011. [Google Scholar] [CrossRef]
- Briganti, A.; Karnes, R.J.; Pozzo, L.F.D.; Cozzarini, C.; Capitanio, U.; Gallina, A.; Suardi, N.; Bianchi, M.; Tutolo, M.; Salonia, A.; et al. Combination of Adjuvant Hormonal and Radiation Therapy Significantly Prolongs Survival of Patients with pT2–4 pN+ Prostate Cancer: Results of a Matched Analysis. Eur. Urol. 2011, 59, 832–840. [Google Scholar] [CrossRef]
- Kaplan, J.R.; Kowalczyk, K.J.; Borza, T.; Gu, X.; Lipsitz, S.R.; Nguyen, P.L.; Friedlander, D.F.; Trinh, Q.-D.; Hu, J.C. Patterns of care and outcomes of radiotherapy for lymph node positivity after radical prostatectomy. BJU Int. 2013, 111, 1208–1214. [Google Scholar] [CrossRef] [PubMed]
- Abdollah, F.; Karnes, R.J.; Suardi, N.; Cozzarini, C.; Gandaglia, G.; Fossati, N.; Vizziello, D.; Sun, M.; Karakiewicz, P.I.; Menon, M.; et al. Impact of adjuvant radiotherapy on survival of patients with node-positive prostate cancer. J. Clin. Oncol. 2014, 32, 3939–3947. [Google Scholar] [CrossRef] [PubMed]
- Rusthoven, C.G.; Carlson, J.A.; Waxweiler, T.V.; Raben, D.; Dewitt, P.E.; Crawford, E.D.; Maroni, P.D.; Kavanagh, B.D. The Impact of Definitive Local Therapy for Lymph Node-Positive Prostate Cancer: A Population-Based Study. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 1064–1073. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.C.; Gray, P.J.; Jemal, A.; Efstathiou, J.A. Androgen deprivation with or without radiation therapy for clinically node-positive prostate cancer. J. Natl. Cancer Inst. 2015, 107, djv119. [Google Scholar] [CrossRef]
- Jegadeesh, N.; Liu, Y.; Zhang, C.; Zhong, J.; Cassidy, R.J.; Gillespie, T.; Kucuk, O.; Rossi, P.; Master, V.A.; Alemozaffar, M.; et al. The role of adjuvant radiotherapy in pathologically lymph node-positive prostate cancer. Cancer 2017, 123, 512–520. [Google Scholar] [CrossRef]
- Van Hemelryk, A.; De Meerleer, G.; Ost, P.; Poelaert, F.; De Gersem, W.; Decaestecker, K.; De Visschere, P.; Fonteyne, V. The Outcome for Patients with Pathologic Node-Positive Prostate Cancer Treated with Intensity Modulated Radiation Therapy and Androgen Deprivation Therapy: A Case-Matched Analysis of pN1 and pN0 Patients. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 323–332. [Google Scholar] [CrossRef]
- Poelaert, F.; Fonteyne, V.; Ost, P.; De Troyer, B.; Decaestecker, K.; De Meerleer, G.; De Visschere, P.; Claeys, T.; Dhondt, B.; Lumen, N. Whole pelvis radiotherapy for pathological node-positive prostate cancer: Oncological outcome and prognostic factors. Strahlenther. Onkol. 2017, 193, 444–451. [Google Scholar] [CrossRef]
- Seisen, T.; Vetterlein, M.W.; Karabon, P.; Jindal, T.; Sood, A.; Nocera, L.; Nguyen, P.L.; Choueiri, T.K.; Trinh, Q.D.; Menon, M.; et al. Efficacy of Local Treatment in Prostate Cancer Patients with Clinically Pelvic Lymph Node-positive Disease at Initial Diagnosis. Eur. Urol. 2018, 73, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Bryant, A.K.; Kader, A.K.; McKay, R.R.; Einck, J.P.; Mell, L.K.; Mundt, A.J.; Kane, C.J.; Efstathiou, J.A.; Murphy, J.D.; Rose, B.S. Definitive Radiation Therapy and Survival in Clinically Node-Positive Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1188–1193. [Google Scholar] [CrossRef]
- Touijer, K.A.; Karnes, R.J.; Passoni, N.; Sjoberg, D.D.; Assel, M.; Fossati, N.; Gandaglia, G.; Eastham, J.A.; Scardino, P.T.; Vickers, A.; et al. Survival Outcomes of Men with Lymph Node-positive Prostate Cancer After Radical Prostatectomy: A Comparative Analysis of Different Postoperative Management Strategies. Eur. Urol. 2018, 73, 890–896. [Google Scholar] [CrossRef]
- Gupta, M.; Patel, H.D.; Schwen, Z.R.; Tran, P.T.; Partin, A.W. Adjuvant radiation with androgen-deprivation therapy for men with lymph node metastases after radical prostatectomy: Identifying men who benefit. BJU Int. 2019, 123, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Vale, C.L.; Burdett, S.; Rydzewska, L.H.M.; Albiges, L.; Clarke, N.W.; Fisher, D.; Fizazi, K.; Gravis, G.; James, N.D.; Mason, M.D.; et al. Addition of docetaxel or bisphosphonates to standard of care in men with localised or metastatic, hormone-sensitive prostate cancer: A systematic review and meta-analyses of aggregate data. Lancet Oncol. 2016, 17, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Ahlgren, G.M.; Flodgren, P.; Tammela, T.L.J.; Kellokumpu-Lehtinen, P.; Borre, M.; Angelsen, A.; Iversen, J.R.; Sverrisdottir, A.; Jonsson, E.; Sengelov, L. Docetaxel Versus Surveillance After Radical Prostatectomy for High-risk Prostate Cancer: Results from the Prospective Randomised, Open-label Phase 3 Scandinavian Prostate Cancer Group 12 Trial. Eur. Urol. 2018, 73, 870–876. [Google Scholar] [CrossRef]
- Attard, G.; Murphy, L.; Clarke, N.W.; Cross, W.; Jones, R.J.; Parker, C.C.; Gillessen, S.; Cook, A.; Brawley, C.; Amos, C.L.; et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet 2022, 399, 447–460. [Google Scholar] [CrossRef] [PubMed]
- Onishi, M.; Kawamura, H.; Murata, K.; Inoue, T.; Murata, H.; Takakusagi, Y.; Okonogi, N.; Ohkubo, Y.; Okamoto, M.; Kaminuma, T. Intensity-modulated radiation therapy with simultaneous integrated boost for clinically node-positive prostate cancer: A single-institutional retrospective study. Cancers 2021, 13, 3868. [Google Scholar] [CrossRef]
- Basu, T.; Senapati, M.R.; Priyadharshni, J.M.; Karpe, A.; Gawde, S.; Gnair, R.; Saxena, U.; Maxwell, S.J.; Pawar, T. Simultaneous integrated boost (SIB) stereotactic body radiotherapy (SBRT) for prostate and pelvic nodes in high risk, node positive and oligometastatic prostate cancers: Safety, efficacy and quality of life outcome measures. J. Clin. Oncol. 2023, 41, 121. [Google Scholar] [CrossRef]
- Mizowaki, T.; Takayama, K.; Nakamura, K.; Aizawa, R.; Inoue, T.; Yamasaki, T.; Kobayashi, T.; Akamatsu, S.; Ogawa, O. Outcomes of high-dose whole pelvic simultaneous integrated boost IMRT in patients with pelvic lymph node-positive prostate cancer. J. Clin. Oncol. 2019, 37, 192. [Google Scholar] [CrossRef]
- Blanchard, P.; Faivre, L.; Lesaunier, F.; Salem, N.; Mesgouez-Nebout, N.; Deniau-Alexandre, E.; Rolland, F.; Ferrero, J.-M.; Houédé, N.; Mourey, L. Outcome according to elective pelvic radiation therapy in patients with high-risk localized prostate cancer: A secondary analysis of the GETUG 12 phase 3 randomized trial. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 85–92. [Google Scholar] [CrossRef]
- Abdollah, F.; Dalela, D.; Sood, A.; Keeley, J.; Alanee, S.; Briganti, A.; Montorsi, F.; Peabody, J.O.; Menon, M. Impact of adjuvant radiotherapy in node-positive prostate cancer patients: The importance of patient selection. Eur. Urol. 2018, 74, 253–256. [Google Scholar] [CrossRef]
- Baker, B.R.; Mohiuddin, J.J.; Chen, R.C. The role of radiotherapy in node-positive prostate cancer. Oncology 2015, 29, 108–114. [Google Scholar]
- Song, C.; Byun, S.J.; Kim, Y.S.; Ahn, H.; Byun, S.-S.; Kim, C.-S.; Lee, S.E.; Kim, J.-S. Elective pelvic irradiation in prostate cancer patients with biochemical failure following radical prostatectomy: A propensity score matching analysis. PLoS ONE 2019, 14, e0215057. [Google Scholar] [CrossRef]
- Ramey, S.J.; Agrawal, S.; Abramowitz, M.C.; Moghanaki, D.; Pisansky, T.M.; Efstathiou, J.A.; Michalski, J.M.; Spratt, D.E.; Hearn, J.W.; Koontz, B.F. Multi-institutional evaluation of elective nodal irradiation and/or androgen deprivation therapy with postprostatectomy salvage radiotherapy for prostate cancer. Eur. Urol. 2018, 74, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Pollack, A.; Karrison, T.G.; Balogh, A.G.; Gomella, L.G.; Low, D.A.; Bruner, D.W.; Wefel, J.S.; Martin, A.-G.; Michalski, J.M.; Angyalfi, S.J. The addition of androgen deprivation therapy and pelvic lymph node treatment to prostate bed salvage radiotherapy (NRG Oncology/RTOG 0534 SPPORT): An international, multicentre, randomised phase 3 trial. Lancet 2022, 399, 1886–1901. [Google Scholar] [CrossRef] [PubMed]
- Iversen, P.; Roder, M.A. The Early Prostate Cancer program: Bicalutamide in nonmetastatic prostate cancer. Expert. Rev. Anticancer. Ther. 2008, 8, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Gillessen, S.; Bossi, A.; Davis, I.D.; de Bono, J.; Fizazi, K.; James, N.D.; Mottet, N.; Shore, N.; Small, E.; Smith, M. Management of patients with advanced prostate cancer. Part I: Intermediate-/high-risk and locally advanced disease, biochemical relapse, and side effects of hormonal treatment: Report of the Advanced Prostate Cancer Consensus Conference 2022. Eur. Urol. 2023, 83, 267–293. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P. Stereotactic ablative radiotherapy for the comprehensive treatment of oligometastatic cancers: Long-term results of the SABR-COMET phase II randomized trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef]
- Phillips, R.; Shi, W.Y.; Deek, M.; Radwan, N.; Lim, S.J.; Antonarakis, E.S.; Rowe, S.P.; Ross, A.E.; Gorin, M.A.; Deville, C. Outcomes of observation vs stereotactic ablative radiation for oligometastatic prostate cancer: The ORIOLE phase 2 randomized clinical trial. JAMA Oncol. 2020, 6, 650–659. [Google Scholar] [CrossRef]
- Harrow, S.; Palma, D.A.; Olson, R.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P. Stereotactic radiation for the comprehensive treatment of oligometastases (SABR-COMET): Extended long-term outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 611–616. [Google Scholar] [CrossRef]
- Ost, P.; Reynders, D.; Decaestecker, K.; Fonteyne, V.; Lumen, N.; De Bruycker, A.; Lambert, B.; Delrue, L.; Bultijnck, R.; Claeys, T.; et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J. Clin. Oncol. 2018, 36, 446–453. [Google Scholar] [CrossRef]
- Siva, S.; Bressel, M.; Murphy, D.G.; Shaw, M.; Chander, S.; Violet, J.; Tai, K.H.; Udovicich, C.; Lim, A.; Selbie, L.; et al. Stereotactic Abative Body Radiotherapy (SABR) for Oligometastatic Prostate Cancer: A Prospective Clinical Trial. Eur. Urol. 2018, 74, 455–462. [Google Scholar] [CrossRef]
- Glicksman, R.M.; Ramotar, M.; Metser, U.; Chung, P.W.; Liu, Z.; Vines, D.; Finelli, A.; Hamilton, R.; Fleshner, N.E.; Perlis, N.; et al. Extended Results and Independent Validation of a Phase 2 Trial of Metastasis-Directed Therapy for Molecularly Defined Oligometastatic Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Hölscher, T.; Baumann, M.; Kotzerke, J.; Zöphel, K.; Paulsen, F.; Müller, A.C.; Zips, D.; Koi, L.; Thomas, C.; Löck, S.; et al. Toxicity and Efficacy of Local Ablative, Image-guided Radiotherapy in Gallium-68 Prostate-specific Membrane Antigen Targeted Positron Emission Tomography-staged, Castration-sensitive Oligometastatic Prostate Cancer: The OLI-P Phase 2 Clinical Trial. Eur. Urol. Oncol. 2022, 5, 44–51. [Google Scholar] [CrossRef]
- Conde-Moreno, A.J.; Lopez, F.; Hervas, A.; Morillo, V.; Mendez, A.; Puertas, M.D.M.; Albarrán, J.V.; De Iturriaga, A.G.; Rico, M.; Vázquez de la Torre, M.L.; et al. Phase II Trial of SBRT and Androgen Deprivation for Oligometastases in Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, S59. [Google Scholar] [CrossRef]
- Deek, M.P.; Van der Eecken, K.; Sutera, P.; Deek, R.A.; Fonteyne, V.; Mendes, A.A.; Decaestecker, K.; Kiess, A.P.; Lumen, N.; Phillips, R. Long-term outcomes and genetic predictors of response to metastasis-directed therapy versus observation in oligometastatic prostate cancer: Analysis of STOMP and ORIOLE trials. J. Clin. Oncol. 2022, 40, 3377–3382. [Google Scholar] [CrossRef]
- Gillessen, S.; Bossi, A.; Davis, I.D.; de Bono, J.; Fizazi, K.; James, N.D.; Mottet, N.; Shore, N.; Small, E.; Smith, M. Management of patients with advanced prostate cancer—Metastatic and/or castration-resistant prostate cancer: Report of the Advanced Prostate Cancer Consensus Conference (APCCC) 2022. Eur. J. Cancer 2023, 185, 178–215. [Google Scholar] [CrossRef]
- Hussain, M.; Tangen, C.; Higano, C.; Vogelzang, N.; Thompson, I. Evaluating intermittent androgen-deprivation therapy phase III clinical trials: The devil is in the details. J. Clin. Oncol. 2016, 34, 280–285. [Google Scholar] [CrossRef]
- Joseph, I.; Nelson, J.B.; Denmeade, S.R.; Isaacs, J.T. Androgens regulate vascular endothelial growth factor content in normal and malignant prostatic tissue. Clin. Cancer Res 1997, 3, 2507–2511. [Google Scholar] [PubMed]
- Roden, A.C.; Moser, M.T.; Tri, S.D.; Mercader, M.; Kuntz, S.M.; Dong, H.; Hurwitz, A.A.; McKean, D.J.; Celis, E.; Leibovich, B.C. Augmentation of T cell levels and responses induced by androgen deprivation. J. Immunol. 2004, 173, 6098–6108. [Google Scholar] [CrossRef] [PubMed]
- Philippou, Y.; Sjoberg, H.T.; Murphy, E.; Alyacoubi, S.; Jones, K.I.; Gordon-Weeks, A.N.; Phyu, S.; Parkes, E.E.; Gillies McKenna, W.; Lamb, A.D. Impacts of combining anti-PD-L1 immunotherapy and radiotherapy on the tumour immune microenvironment in a murine prostate cancer model. Br. J. Cancer 2020, 123, 1089–1100. [Google Scholar] [CrossRef]
- Zilli, T.; Dirix, P.; Heikkilä, R.; Liefhooghe, N.; Siva, S.; Gomez-Iturriaga, A.; Everaerts, W.; Otte, F.; Shelan, M.; Mercier, C. The multicenter, randomized, phase 2 PEACE V-STORM trial: Defining the best salvage treatment for oligorecurrent nodal prostate cancer metastases. Eur. Urol. Focus 2021, 7, 241–244. [Google Scholar] [CrossRef]
- Zilli, T.; Achard, V.; Dal Pra, A.; Schmidt-Hegemann, N.; Jereczek-Fossa, B.A.; Lancia, A.; Ingrosso, G.; Alongi, F.; Aluwini, S.; Arcangeli, S. Recommendations for radiation therapy in oligometastatic prostate cancer: An ESTRO-ACROP Delphi consensus. Radiother. Oncol. 2022, 176, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Swami, U.; Velho, P.I.; Nussenzveig, R.; Chipman, J.; Santos, V.S.; Erickson, S.; Dharmaraj, D.; Alva, A.S.; Vaishampayan, U.N.; Esther, J. Association of SPOP mutations with outcomes in men with de novo metastatic castration-sensitive prostate cancer. Eur. Urol. 2020, 78, 652–656. [Google Scholar] [CrossRef] [PubMed]
- Kucharczyk, M.J.; So, J.; Gravis, G.; Sweeney, C.; Saad, F.; Niazi, T. A combined biological and clinical rationale for evaluating metastasis directed therapy in the management of oligometastatic prostate cancer. Radiother. Oncol. 2020, 152, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Sini, C.; Chiorda, B.N.; Gabriele, P.; Sanguineti, G.; Morlino, S.; Badenchini, F.; Cante, D.; Carillo, V.; Gaetano, M.; Giandini, T. Patient-reported intestinal toxicity from whole pelvis intensity-modulated radiotherapy: First quantification of bowel dose–volume effects. Radiother. Oncol. 2017, 124, 296–301. [Google Scholar] [CrossRef]
- Chuong, M.D.; Hartsell, W.; Larson, G.; Tsai, H.; Laramore, G.E.; Rossi, C.J.; Wilkinson, J.B.; Kaiser, A.; Vargas, C. Minimal toxicity after proton beam therapy for prostate and pelvic nodal irradiation: Results from the proton collaborative group REG001-09 trial. Acta Oncol. 2018, 57, 368–374. [Google Scholar] [CrossRef]
- Ishii, K.; Yamanaga, T.; Ogino, R.; Hosokawa, Y.; Kishimoto, S.; Nakahara, R.; Shimada, C.; Kawamorita, R.; Tada, T.; Hayashi, Y. Bowel and urinary quality of life after whole-pelvic versus prostate-only volumetric-modulated arc therapy for localized prostate cancer. Pract. Radiat. Oncol. 2018, 8, e49–e55. [Google Scholar] [CrossRef]
- Sini, C.; Fiorino, C.; Perna, L.; Chiorda, B.N.; Deantoni, C.L.; Bianchi, M.; Sacco, V.; Briganti, A.; Montorsi, F.; Calandrino, R. Dose–volume effects for pelvic bone marrow in predicting hematological toxicity in prostate cancer radiotherapy with pelvic node irradiation. Radiother. Oncol. 2016, 118, 79–84. [Google Scholar] [CrossRef]
- Ong, A.L.; Ang, K.; Master, Z.; Wong, S.M.; Tuan, J.K. Intensity-modulated radiotherapy for whole pelvis irradiation in prostate cancer: A dosimetric and plan robustness study between photons and protons. Tech. Innov. Patient Support. Radiat. Oncol. 2018, 6, 11–19. [Google Scholar] [CrossRef]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef]
- Buonerba, C.; Ferro, M.; Dolce, P.; Crocetto, F.; Verde, A.; Lucarelli, G.; Scafuri, L.; Facchini, S.; Vaia, A.; Marinelli, A. Predictors of efficacy of androgen-receptor-axis-targeted therapies in patients with metastatic castration-sensitive prostate cancer: A systematic review and meta-analysis. Crit. Rev. Oncol./Hematol. 2020, 151, 102992. [Google Scholar] [CrossRef]
- James, N.D.; Ingleby, F.C.; Clarke, N.W.; Amos, C.L.; Attard, G.; Brawley, C.D.; Chowdhury, S.; Cross, W.; Dearnaley, D.P.; Gilbert, D.C. Docetaxel for nonmetastatic prostate cancer: Long-term survival outcomes in the STAMPEDE randomized controlled trial. JNCI Cancer Spectr. 2022, 6, pkac043. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Société Internationale d’Urologie. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).