
The Impact of Socioeconomic Factors on Kidney Transplantation: A Systematic Review of Low- and Middle-Income Countries

 , ,
, ,  , , , , , , , and
, , , , , , , and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Low- and Middle-Income Countries
2.2. Literature Search
2.3. Selection Criteria and Abstract Screening
2.4. Full-Text Screening and Data Extraction
3. Results
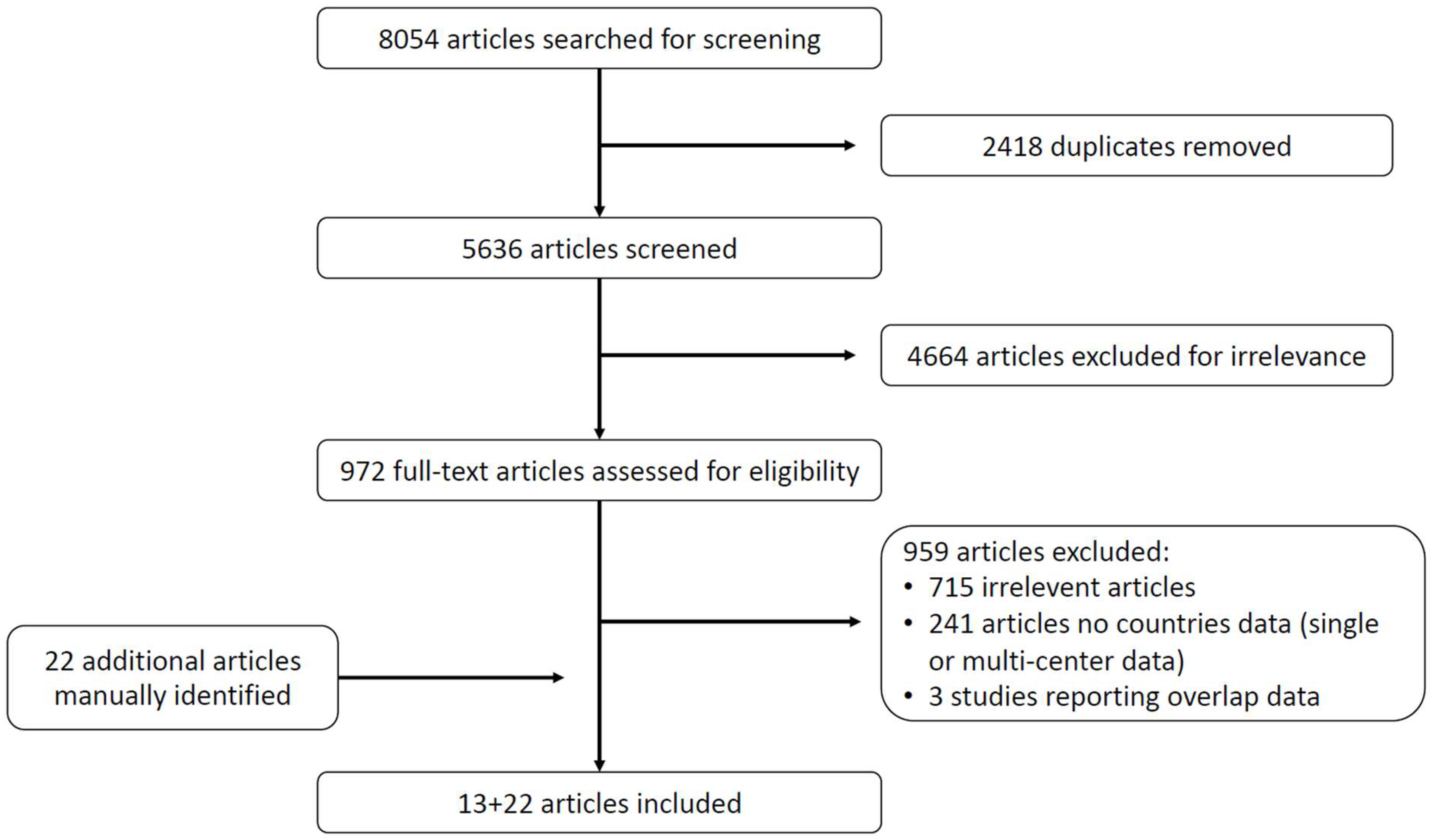
3.1. Search Results
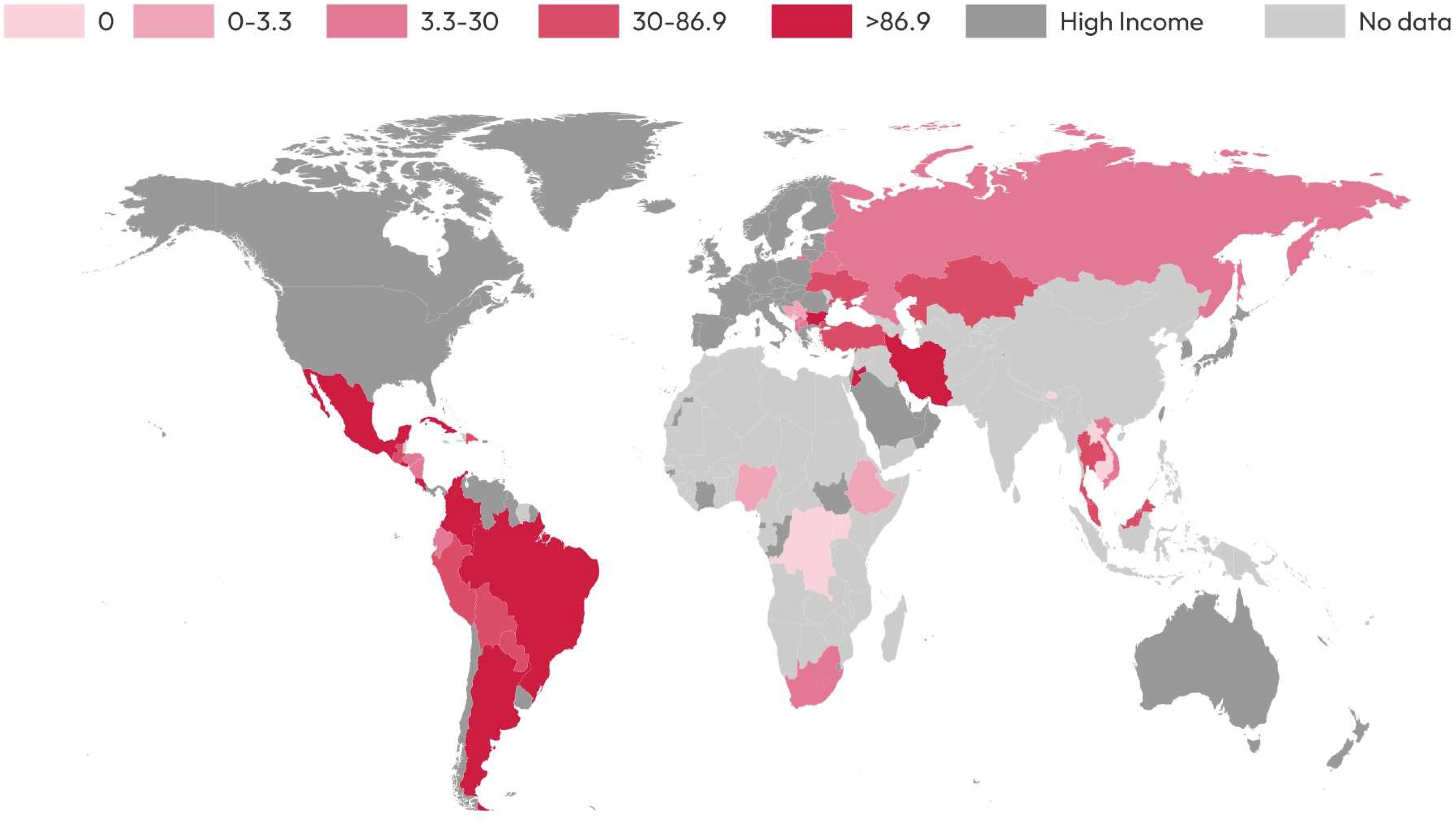
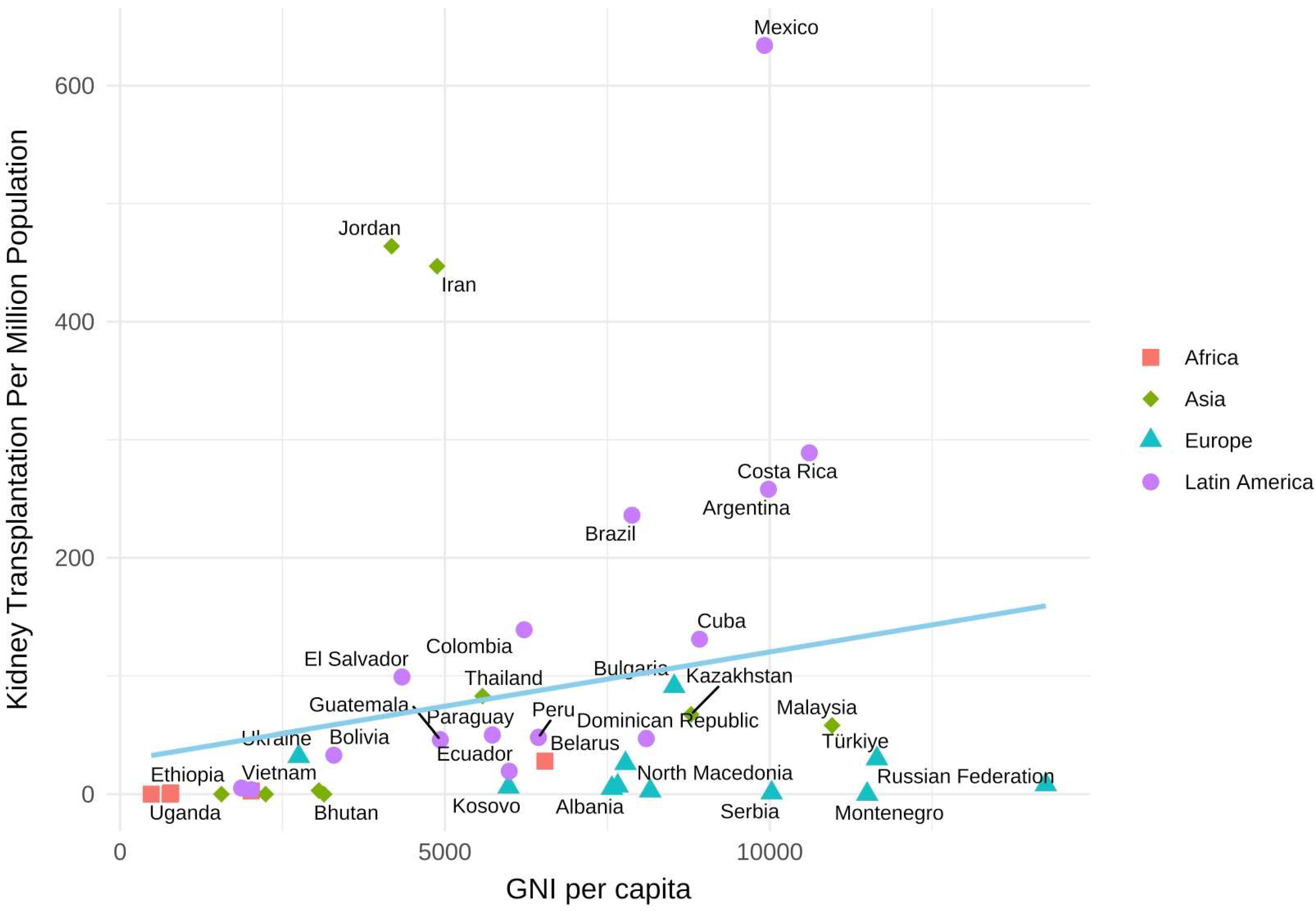
3.2. The Relationship between Country’s Income and KT Prevalence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yoo, K.D.; Kim, C.T.; Kim, M.H.; Noh, J.; Kim, G.; Kim, H.; An, J.N.; Park, J.Y.; Cho, H.; Kim, K.H.; et al. Superior outcomes of kidney transplantation compared with dialysis: An optimal matched analysis of a national population-based cohort study between 2005 and 2008 in Korea. Medicine 2016, 95, e4352. [Google Scholar] [CrossRef] [PubMed]
- Boenink, R.; Kramer, A.; Vanholder, R.C.; Mahillo, B.; Massy, Z.A.; Bušić, M.; Ortiz, A.; Stel, V.S.; Jager, K.J. Factors influencing kidney transplantation rates: A study from the ERA Registry. Nephrol. Dial. Transplant. 2023, 38, 1540–1551. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, A.; McCulloch, M.I. Paediatric kidney transplantation in under-resourced regions—A panoramic view. Pediatr. Nephrol. 2022, 37, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Wainstein, M.; Bello, A.K.; Jha, V.; Harris, D.C.; Levin, A.; Gonzalez-Bedat, M.C.; Rosa-Diez, G.J.; Fuentes, A.F.; Sola, L.; Pecoits-Filho, R.; et al. International Society of Nephrology Global Kidney Health Atlas: Structures, organization, and services for the management of kidney failure in Latin America. Kidney Int. Suppl. 2021, 11, e35–e46. [Google Scholar] [CrossRef] [PubMed]
- Muralidharan, A.; White, S. The need for kidney transplantation in low- and middle-income countries in 2012: An epidemiological perspective. Transplantation 2015, 99, 476–481. [Google Scholar] [CrossRef]
- Chan-on, C.; Sarwal, M.M. A Comprehensive Analysis of the Current Status and Unmet Needs in Kidney Transplantation in Southeast Asia [Review]. Front. Med. 2017, 4, 84. [Google Scholar] [CrossRef]
- World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 25 April 2024).
- Abdugafarov, S.; Assykbayev, M. Kidney transplantation in Kazakhstan: The burden of organ shortage. Russ. J. Transplantol. Artif. Organs 2021, 23, 36–40. [Google Scholar] [CrossRef]
- Abraham, G.; Vijayan, M.; Gopalakrishnan, N.; Shroff, S.; Amalorpavanathan, J.; Yuvaraj, A.; Nair, S.; Sundarrajan, S. State of deceased donor transplantation in India: A model for developing countries around the world. World J. Transplant. 2016, 6, 331–335. [Google Scholar] [CrossRef]
- Ahmed, M.M.; Tedla, F.M.; Leichtman, A.B.; Punch, J.D. Organ Transplantation in Ethiopia. Transplantation 2019, 103, 449–451. [Google Scholar] [CrossRef]
- Arogundade, F.A.; Esezobor, C.I.; Okafor, H.U.; Abdu, A.; Balogun, R.A.; Effa, E.E.; Popoola, J.; Bamgboye, E.L. Nephrology in Nigeria. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 41–54. [Google Scholar]
- Astley, M.E.; Boenink, R.; Abd ElHafeez, S.; Trujillo-Alemán, S.; Arribas, F.; Åsberg, A.; Beckerman, P.; Bell, S.; Bouzas-Caamaño, M.E.; Farnés, J.C.; et al. The ERA Registry Annual Report 2020: A summary. Clin. Kidney J. 2023, 16, 1330–1354. [Google Scholar] [CrossRef]
- Babloyan, S.; Voskanyan, M.; Shekherdimian, S.; Nazaryan, H.; Arakelyan, S.; Kurkchyan, K.; Geyikyan, P.; Babloyan, A.; Sarkissian, A. Kidney Transplantation in Low- to Middle-Income Countries: Outcomes and Lessons Learned from Armenia. Ann. Transplant. 2021, 26, e930943. [Google Scholar] [CrossRef] [PubMed]
- Bayramov, N.Y.; Gahramanova, F.A. A Brief History of Organ and Tissue Transplantation in Azerbaijan. Exp. Clin. Transplant. 2022, 20, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Bharati, J.; Jha, V. Nephrology in India. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 291–298. [Google Scholar]
- Broumand, B. Nephrology in Iran. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 313–327. [Google Scholar]
- Davids, M.R.; Chothia, M.-Y.; Wearne, N.; Davidson, B.; McCulloch, M. Nephrology in South Africa. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 55–73. [Google Scholar]
- Davids, M.R.; Marais, N.; Sebastian, S.; Jardine, T.; Jacobs, J.C. South African Renal Registry Annual Report 2021. Afr. J. Nephrol. 2023, 26, 83–94. [Google Scholar]
- Ejigu, A.M.; Ahmed, M.M.; Mengistu, Y.T. Nephrology in Ethiopia. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 35–40. [Google Scholar]
- Gonzalez-Bedat, M.; Rosa-Diez, G.; Pecoits-Filho, R.; Ferreiro, A.; García-García, G.; Cusumano, A.; Fernandez-Cean, J.; Noboa, O.; Douthat, W. Burden of disease: Prevalence and incidence of ESRD in Latin America. Clin. Nephrol. 2015, 83 (Suppl. S1), 3–6. [Google Scholar] [CrossRef]
- Jha, V.; Ur-Rashid, H.; Agarwal, S.K.; Akhtar, S.F.; Kafle, R.K.; Sheriff, R. The state of nephrology in South Asia. Kidney Int. 2019, 95, 31–37. [Google Scholar] [CrossRef]
- Kalyesubula, R.; Makanga, G.; Gyagenda, J.O.; Atuhe, D.; Kansiime, G.; Kiggundu, D.; Eyoku, S.P.; Batte, A.; Bagasha, P.; Ssekasanvu, E. Nephrology in Uganda. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 75–83. [Google Scholar]
- Kalyesubula, R.; Nankabirwa, J.I.; Ssinabulya, I.; Siddharthan, T.; Kayima, J.; Nakibuuka, J.; Salata, R.A.; Mondo, C.; Kamya, M.R.; Hricik, D. Kidney disease in Uganda: A community based study. BMC Nephrol. 2017, 18, 116. [Google Scholar] [CrossRef]
- Kolesnyk, M.; Kozliuk, N.; Razvazhaeva, O. National Registry of Patients with Chronic Kidney Disease and Patients with Acute Kidney Injury 20 years: Acquisitions and perspectives. Ukr. J. Nephrol. Dial. 2022, 4, 3–9. [Google Scholar] [CrossRef]
- Kolesnyk, M.; Stepanova, N.; Dudar, I.; Bagdasarova, I.; Fomina, S. Nephrology in Ukraine. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 675–685. [Google Scholar]
- Kramer, A.; Boenink, R.; Noordzij, M.; Bosdriesz, J.R.; Stel, V.S.; Beltrán, P.; Ruiz, J.C.; Seyahi, N.; Comas Farnés, J.; Stendahl, M.; et al. The ERA-EDTA Registry Annual Report 2017: A summary. Clin. Kidney J. 2020, 13, 693–709. [Google Scholar] [CrossRef]
- Kramer, A.; Pippias, M.; Noordzij, M.; Stel, V.S.; Andrusev, A.M.; Aparicio-Madre, M.I.; Arribas Monzón, F.E.; Åsberg, A.; Barbullushi, M.; Beltran, P.; et al. The European Renal Association—European Dialysis and Transplant Association (ERA-EDTA) Registry Annual Report 2016: A summary. Clin. Kidney J. 2019, 12, 702–720. [Google Scholar] [CrossRef]
- Lydia, A.; Widiana, I.G.R.; Bandiara, R.; Afiatin; Ali, Z.; Nugroho, P.; Hidayati, E.L. Nephrology in Indonesia. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 299–312. [Google Scholar]
- Moosa, M.R. The state of kidney transplantation in South Africa. S. Afr. Med. J. 2019, 109, 235–240. [Google Scholar] [CrossRef]
- Moradpour, A.; Hadian, M.; Tavakkoli, M. Economic evaluation of End Stage Renal Disease treatments in Iran. Clin. Epidemiol. Glob. Health 2020, 8, 199–204. [Google Scholar] [CrossRef]
- Morovatdar, N.; Tayebi Nasrabad, G.; Tsarouhas, K.; Rezaee, R. Etiology of Renal Replacement Therapy in Iran. Int. J. Nephrol. 2019, 2019, 5010293. [Google Scholar] [CrossRef] [PubMed]
- Nephrology ISo. 13th Report of Indonesian Renal Registry; Indonesian Renal Registry: Jakarta, Indonesia, 2023. [Google Scholar]
- Noppakun, K.; Ingsathit, A.; Pongskul, C.; Premasthian, N.; Avihingsanon, Y.; Lumpaopong, A.; Vareesangthip, K.; Sumethkul, V.; Subcommittee for Kidney Transplant Registry and Thai Transplantation Society. A 25-year experience of kidney transplantation in Thailand: Report from the Thai Transplant Registry. Nephrology 2015, 20, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Sumaili, E.K.; Ekulu, P.M.; Pakasa, N.M.; Tshala-Katumbay, D.; Nseka, N.M. Nephrology in the Democratic Republic of the Congo. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 25–34. [Google Scholar]
- Tang, S.C.W.; Yu, X.; Chen, H.C.; Kashihara, N.; Park, H.C.; Liew, A.; Goh, B.L.; Nazareth, M.G.C.; Bunnag, S.; Tan, J.; et al. Dialysis Care and Dialysis Funding in Asia. Am. J. Kidney Dis. 2020, 75, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Ulasi, I.I.; Ijoma, C.K. Organ Transplantation in Nigeria. Transplantation 2016, 100, 695–697. [Google Scholar] [CrossRef] [PubMed]
- Vazelov, E.S.; Bogov, B.I.; Gaydarova, M.S.; Georgiev, M.I.; Roussinov, D.L. Nephrology in Bulgaria. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 477–486. [Google Scholar]
- Wang, A.Y.-M.; An, Y.; Cai, G.-Y.; Chen, J.H.; Chen, W.; Chen, X.M.; Cui, Z.; Hao, C.M.; Hou, F.F.; Liu, B.C.; et al. Nephrology in China. In Nephrology Worldwide; Moura-Neto, J.A., Divino-Filho, J.C., Ronco, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 251–290. [Google Scholar]
- Wang, F.; Yang, C.; Long, J.; Zhao, X.; Tang, W.; Zhang, D.; Bai, K.; Su, Z.; Gao, B.; Chu, H.; et al. Executive summary for the 2015 Annual Data Report of the China Kidney Disease Network (CK-NET). Kidney Int. 2019, 95, 501–505. [Google Scholar] [CrossRef]
- Tran, S.N.; Du, T.T.N.; Thai, S.M.; Nguyen, H.T.; Bui, T.V.; Lo-Cao, E.A.; Pleass, H.; Allen, R.; Robertson, P.; Nguyen, S.T.; et al. Current Status of Organ Donation for Transplantation in Vietnam. Transplantation 2018, 102, S382. [Google Scholar] [CrossRef]
- García-García, G.; Harden, P.; Chapman, J. The global role of kidney transplantation. Nefrología 2012, 32, 1–6. [Google Scholar] [CrossRef]
- World Health Organization. Human Organ and Tissue Transplantation: Report by the Director-General; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Region | Number of Countries Reported | GNI per Capita (Median, Q25–Q75) (in $) | KRT Prevalence (Median, Q25–Q75) (pmp) | KT Prevalence (Median, Q25–Q75) (pmp) |
|---|---|---|---|---|
| Africa | 5 | 780 (770–2020) | 15 (7.1–51.8) | 1.05 (0–2.7) |
| Asia | 24 | 3805 (2010–5055) | 499 (175–958.7) | 58 (0–82.8) |
| Europe | 11 | 8160 (7615–10,765) | 591 (420.5–786.5) | 7 (3.9–28) |
| Latin America | 16 | 6105 (4077.5–8305) | 469 (332.95–753.5) | 50 (39.5–187.5) |
| Region | Country | Year of Report | Population (in Thousands) | GNI per Capita | Number of Renal Centers | Number of KRTs (n) | Prevalence of KRT (pmp) | Prevalence of HD (pmp) | Prevalence of PD (pmp) | Prevalence of KT (pmp) |
|---|---|---|---|---|---|---|---|---|---|---|
| Europe | Albania [12] | 2023 | 2818 | 7570 | 14 | 1664 | 591 | 5 | ||
| Europe | Belarus [12] | 2023 | 9380 | 7780 | 54 | 3881 | 414 | 26 | ||
| Europe | Bosnia and Herzegovina [12] | 2023 | 3531 | 8160 | 29 | 2547 | 721 | 2.8 | ||
| Europe | Bulgaria [27,37] | 2018 | 7000 | 8530 | 3893 | 610 | 522 | 19 | 91 | |
| Europe | Kosovo [12] | 2023 | 1688 | 5980 | 9 | 784 | 465 | 6 | ||
| Europe | Montenegro [12] | 2023 | 621 | 11,500 | 12 | 241 | 387.9 | 381.5 | 0 | 0 |
| Europe | North Macedonia [12] | 2023 | 2069 | 7660 | 23 | 1762 | 852 | 7 | ||
| Europe | Russian Federation [12] | 2023 | 143,248 | 14,250 | 740 | 61,164 | 427 | 8 | ||
| Europe | Serbia [12] | 2023 | 6209 | 10,030 | 64 | 5516 | 888.4 | 679.8 | 73.6 | 1.1 |
| Europe | Türkiye [12] | 2023 | 83,614 | 11,650 | 1111 | 83,350 | 997 | 30 | ||
| Europe | Ukraine [24,25] | 2021 | 42,216 | 2750 | 8290 | 267.9 | 208.9 | 22.3 | 35.7 | |
| Asia | Afghanistan [21] | 2018 | 34,700 | 520 | 5000 | 144 | ||||
| Asia | Armenia [13] | 2021 | 2780.469 | 4850 | ||||||
| Asia | Azerbaijan [14] | 2022 | 5670 | |||||||
| Asia | Bangladesh [35] | 2022 | 167,000 | 2820 | 101 | |||||
| Asia | Bhutan [35] | 2018 | 800 | 3140 | 3 | 140 | 175 | 0 | ||
| Asia | Cambodia [35] | 2019 | 15,000 | 1560 | 40 | 40 | 0 | 0 | ||
| Asia | China (Mainland) [38,39] | 2019 | 1,428,000 | 10,310 | 610,811 | 402.18 | 39.95 | |||
| Asia | India [9,15,21] | 2019 | 1,340,000 | 2080 | 134 | |||||
| Asia | Indonesia [21,28,32,35] | 2019 | 267,663 | 4070 | 797 | 77,892 | 499 | 494 | 5 | |
| Asia | Iran [16,30,31] | 2018 | 81,672 | 4880 | 892 | 408 | 37 | 447 | ||
| Asia | Jordan [35] | 2019 | 9700 | 4180 | 9300 | 958.7 | 546.5 | 95.9 | 463.9 | |
| Asia | Kazakhstan [8] | 2021 | 19,196.465 | 8790 | 67.3 | |||||
| Asia | Laos [6] | 2017 | 2240 | 0 | ||||||
| Asia | Malaysia [6,35] | 2019 | 32,000 | 10,960 | 41,525 | 1345 | 1160 | 128 | 58 | |
| Asia | Maldives [35] | 2018 | 400 | 9880 | ||||||
| Asia | Mongolia [35] | 2019 | 3200 | 3840 | 390 | |||||
| Asia | Myanmar [35] | 2019 | 1370 | |||||||
| Asia | Nepal [35] | 2019 | 26,000 | 1220 | 1500 | |||||
| Asia | Pakistan [35] | 2018 | 193,200 | 1610 | ||||||
| Asia | Philippines [6,35] | 2019 | 105,000 | 3770 | 32,077 | 607 | ||||
| Asia | Sri Lanka [35] | 2018 | 21,200 | 4360 | 5482 | 258 | ||||
| Asia | Thailand [6,33,35] | 2015 | 69,157.023 | 5580 | 1307 | 82.8 | ||||
| Asia | Timor-Leste [6] | 2017 | 1800 | |||||||
| Asia | Vietnam [37,40] | 2018 | 94,914.33 | 3060 | 3.04 | |||||
| Africa | Democratic Republic of the Congo [34] | 2018 | 82,366,288 | 480 | 15 | 242 | 3 | 2.9 | 0 | |
| Africa | Ethiopia [10,19] | 2018 | 112,000 | 780 | 30 | 800 | 7.1 | 7.1 | 0 | 1.05 |
| Africa | Nigeria [11,36] | 2018 | 203,000 | 2020 | 10 | 15 | 14.7 | 0.05 | 2.7 | |
| Africa | Uganda [22,23] | 2018 | 44,700 | 770 | 10 | 51.8 | 0 | |||
| Africa | South Africa [17,18,29] | 2021 | 60.14 | 6540 | 281 | 8866 | 147 | 105 | 14 | 28 |
| Latin America | Argentina [4] | 2021 | 44,694.198 | 9980 | 976 | 673 | 45 | 258 | ||
| Latin America | Bolivia [4] | 2021 | 11,306.341 | 3290 | 451 | 33 | ||||
| Latin America | Brazil [4] | 2021 | 208,846.892 | 7880 | 876 | 591 | 49 | 236 | ||
| Latin America | Colombia [4] | 2021 | 48,168.996 | 6220 | 686 | 400 | 148 | 139 | ||
| Latin America | Costa Rica [20] | 2015 | 4669.000 | 10,610 | 338.8 | 29.1 | 20.8 | 288.9 | ||
| Latin America | Cuba [4] | 2021 | 11,116.396 | 8920 | 430 | 293 | 6 | 131 | ||
| Latin America | Dominican Republic [4] | 2021 | 10,298.756 | 8100 | 305 | 183 | 75 | 47 | ||
| Latin America | Ecuador [20] | 2015 | 14,490.000 | 5990 | 405.9 | 352 | 34.5 | 19.5 | ||
| Latin America | Guatemala [4] | 2021 | 16,581.273 | 4930 | 508 | 257 | 204 | 46 | ||
| Latin America | Honduras [20] | 2015 | 7619.000 | 2020 | 187.2 | 167.1 | 16.3 | 3.8 | ||
| Latin America | Haiti [4] | 2021 | 10,788.440 | 1440 | ||||||
| Latin America | Mexico [4] | 2021 | 125,959.205 | 9920 | 1405 | 272 | 499 | 634 | ||
| Latin America | Nicaragua [20] | 2015 | 5813.000 | 1870 | 37 | 29.2 | 2.6 | 5.2 | ||
| Latin America | Peru [4] | 2021 | 31,331.228 | 6440 | 590 | 486 | 56 | 48 | ||
| Latin America | Paraguay [4] | 2021 | 7025.763 | 5730 | 331 | 271 | 10 | 50 | ||
| Latin America | El Salvador [4] | 2021 | 6187.271 | 4340 | 776 | 297 | 380 | 99 |
| Country | Prevalence of KTs (pmp) | First Year of KTs | Number of KT Centers | Total Number of KTs | Number of KTs per Year | Deceased Donor (%) | Living Donor (%) |
|---|---|---|---|---|---|---|---|
| Albania [12] | 5 | 14 | 0 | 100 | |||
| Belarus [12] | 26 | 242 | 100 | 0 | |||
| Bosnia and Herzegovina [12] | 2.8 | 10 | 18 | 82 | |||
| Bulgaria [27,37] | 91 | 1968 | 3 | 638 | 25 | ||
| Kosovo [12] | 6 | 10 | 0 | 100 | |||
| Montenegro [12] | 0 | 0 | 0 | 0 | |||
| North Macedonia [12] | 7 | 14 | 29 | 71 | |||
| Russian Federation [12] | 8 | 1124 | 87.5 | 12.5 | |||
| Serbia [12] | 1.1 | 7 | 72.7 | 27.3 | |||
| Türkiye [12] | 30 | 197 | 10 | 90 | |||
| Ukraine [24,25] | 35.7 | 1933 | 7 | 1533 | 135 | 0 * | 100 |
| Afghanistan [21] | 1 | ||||||
| Armenia [13] | 1 | 196 | 20 | ||||
| Azerbaijan [14] | 1971 | 7 | 898 | 100 | |||
| Bangladesh [35] | 10 | 1500 | 350 | 0 | 100 | ||
| Bhutan [35] | 0 | NA | 0 | 0 | 0 | ||
| Cambodia [35] | 0 | NA | 0 | 0 | 0 | ||
| China (Mainland) [38,39] | 1972 | 10,000 | 86.8 | 13.2 | |||
| India [9,15,21] | 1971 | 233 | 8000 | 0.34 | |||
| Indonesia [21,28,32,35] | 1977 | 16 | 142 | 0 | 100 | ||
| Iran [16,30,31] | 447 | 1967 | 2281 | 10 | 90 | ||
| Jordan [35] | 463.9 | 4500 | 230–250 | ||||
| Kazakhstan [8] | 67.3 | 1278 | 12.5 | 87.5 | |||
| Laos [6] | 0 | 0 | 0 | 0 | |||
| Malaysia [6,35] | 58 | ||||||
| Maldives [35] | |||||||
| Mongolia [35] | |||||||
| Myanmar [35] | 1995 | 220 | |||||
| Nepal [35] | 4 | 312 | |||||
| Pakistan [35] | 16 | 476 | |||||
| Philippines [6,35] | |||||||
| Sri Lanka [35] | 7 | 267 | |||||
| Thailand [6,33,35] | 82.8 | 1972 | 26 | 5729 | 50.4 | 49.6 | |
| Timor-Leste [6] | |||||||
| Vietnam [37,40] | 3.04 | 1992 | 17 | 2426 | 7.3 | 92.7 | |
| Democratic Republic of the Congo [34] | 0 | 0 | 0 | ||||
| Ethiopia [10,19] | 1.05 | 2015 | 118 | 35–40 | 0 | 100 | |
| Nigeria [11,36] | 2.7 | 2000 | 14 | 550 | 142 | 0 | 100 |
| Uganda [22,23] | 0 | 0 | 100 (outside Uganda) | 0 | 0 | 100 | |
| South Africa [17,18,29] | 28 | 1966 | 7 | 1697 | 260 | 58.3 | 41.7 |
| Argentina [4] | 258 | ||||||
| Bolivia [4] | 33 | ||||||
| Brazil [4] | 236 | ||||||
| Colombia [4] | 139 | ||||||
| Costa Rica [20] | 288.9 | ||||||
| Cuba [4] | 131 | ||||||
| Dominican Republic [4] | 47 | ||||||
| Ecuador [20] | 19.5 | ||||||
| Guatemala [4] | 46 | ||||||
| Honduras [20] | 3.8 | ||||||
| Haiti [4] | |||||||
| Mexico [4] | 634 | ||||||
| Nicaragua [20] | 5.2 | ||||||
| Peru [4] | 48 | ||||||
| Paraguay [4] | 50 | ||||||
| El Salvador [4] | 99 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Published by MDPI on behalf of the Société Internationale d’Urologie. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duong, N.X.; Thai, M.S.; Tran, N.S.; Hoang, K.C.; Chau, Q.T.; Ngo, X.T.; Duong, T.T.; Truong, T.H.T.; Ngo, H.T.T.; Nguyen, D.T.; et al. The Impact of Socioeconomic Factors on Kidney Transplantation: A Systematic Review of Low- and Middle-Income Countries. Soc. Int. Urol. J. 2024, 5, 349-360. https://doi.org/10.3390/siuj5050054
Duong NX, Thai MS, Tran NS, Hoang KC, Chau QT, Ngo XT, Duong TT, Truong THT, Ngo HTT, Nguyen DT, et al. The Impact of Socioeconomic Factors on Kidney Transplantation: A Systematic Review of Low- and Middle-Income Countries. Société Internationale d’Urologie Journal. 2024; 5(5):349-360. https://doi.org/10.3390/siuj5050054
Chicago/Turabian StyleDuong, Nguyen Xuong, Minh Sam Thai, Ngoc Sinh Tran, Khac Chuan Hoang, Quy Thuan Chau, Xuan Thai Ngo, Trung Toan Duong, Tan Ho Trong Truong, Hanh Thi Tuyet Ngo, Dat Tien Nguyen, and et al. 2024. "The Impact of Socioeconomic Factors on Kidney Transplantation: A Systematic Review of Low- and Middle-Income Countries" Société Internationale d’Urologie Journal 5, no. 5: 349-360. https://doi.org/10.3390/siuj5050054
APA StyleDuong, N. X., Thai, M. S., Tran, N. S., Hoang, K. C., Chau, Q. T., Ngo, X. T., Duong, T. T., Truong, T. H. T., Ngo, H. T. T., Nguyen, D. T., Quy, K., Hoang, T. D., Nguyen, D.-D., Onder, N. K., Mendiola, D. F., Mai, A. T., Hammad, M. A. M., Vuong, H. G., Tiong, H. Y., ... Nguyen, T. T. (2024). The Impact of Socioeconomic Factors on Kidney Transplantation: A Systematic Review of Low- and Middle-Income Countries. Société Internationale d’Urologie Journal, 5(5), 349-360. https://doi.org/10.3390/siuj5050054