Relationship Between Serum Testosterone and Severity of Lower Urinary Tract Symptoms among Malaysian Men


Abstract
:Introduction
Materials and Methods
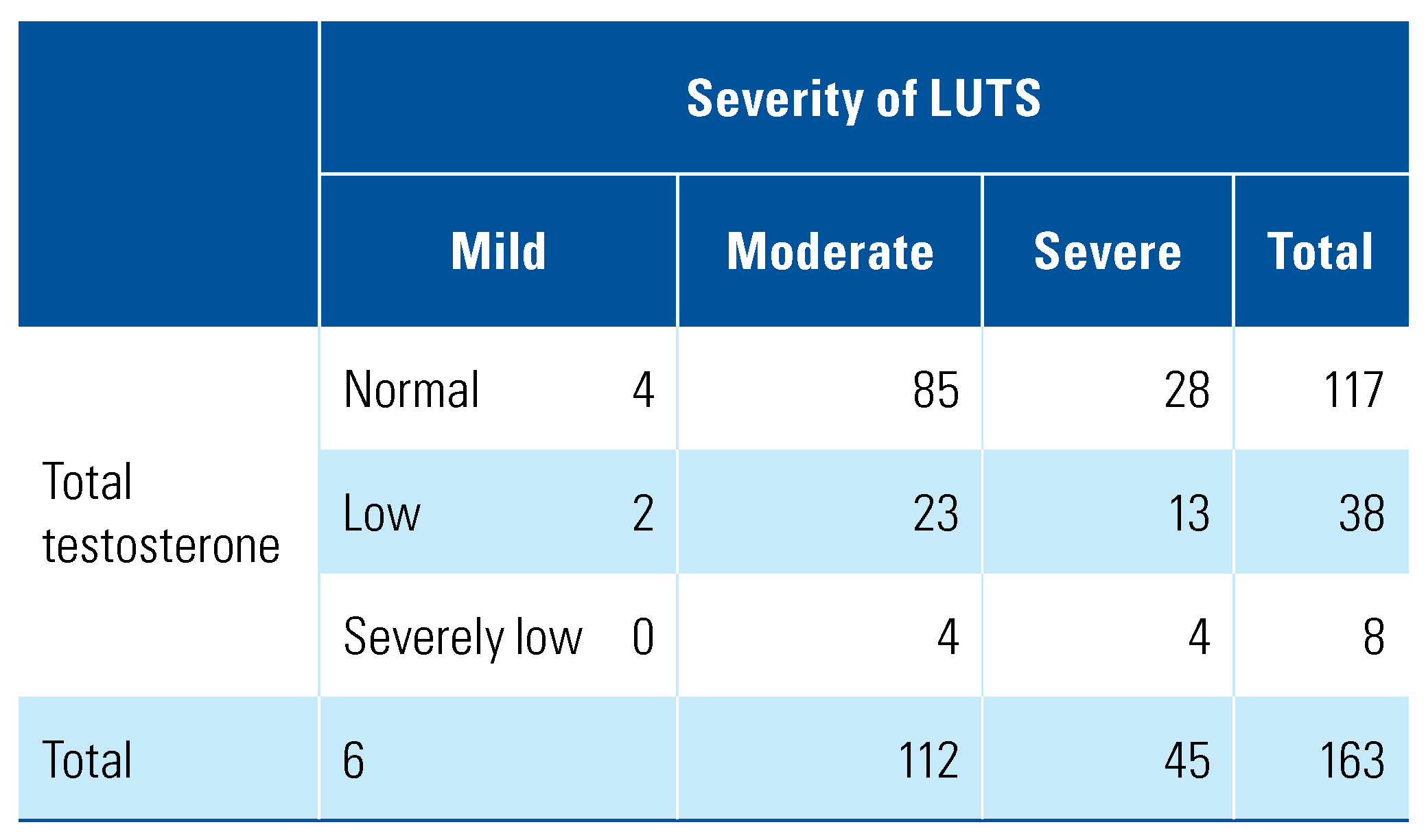
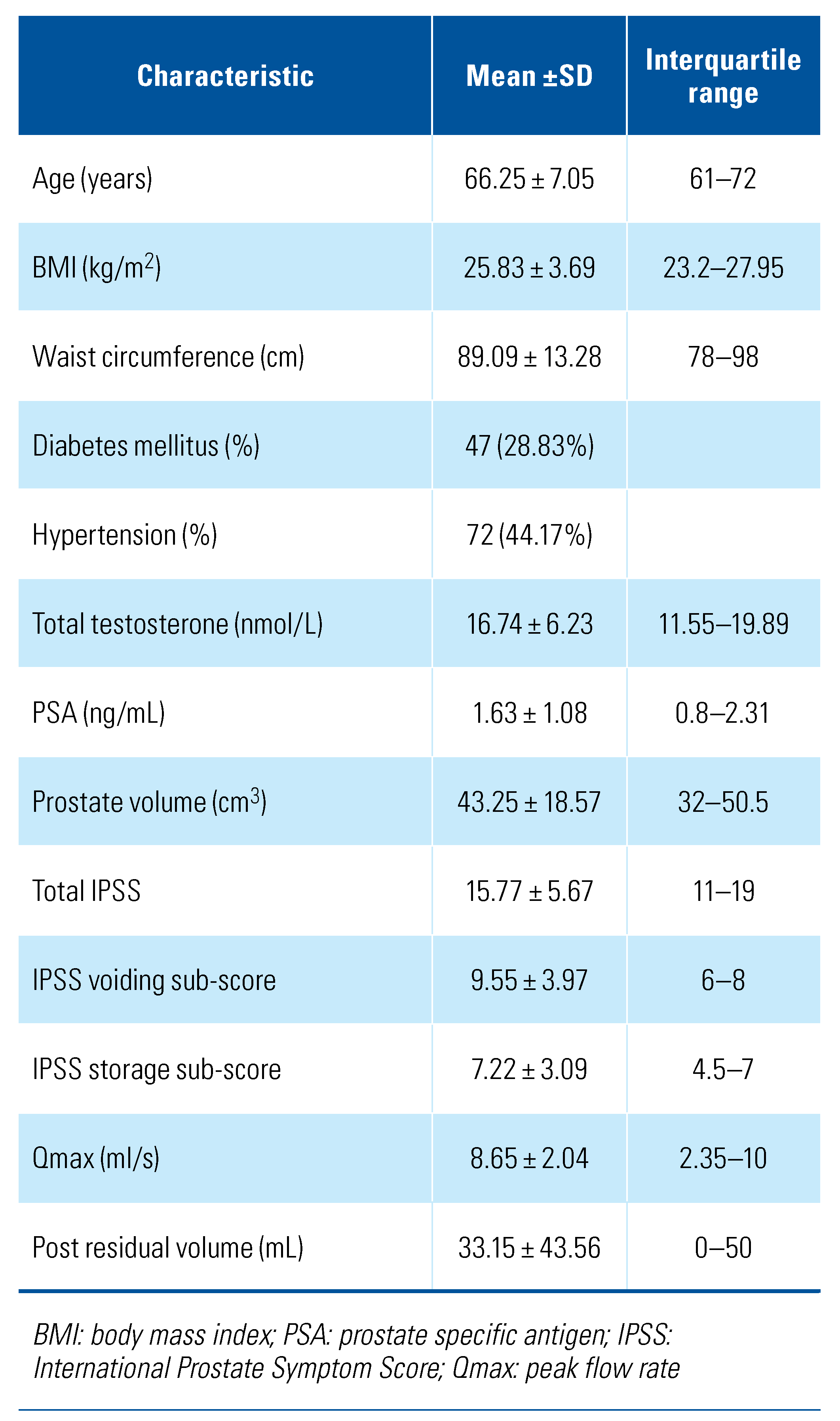
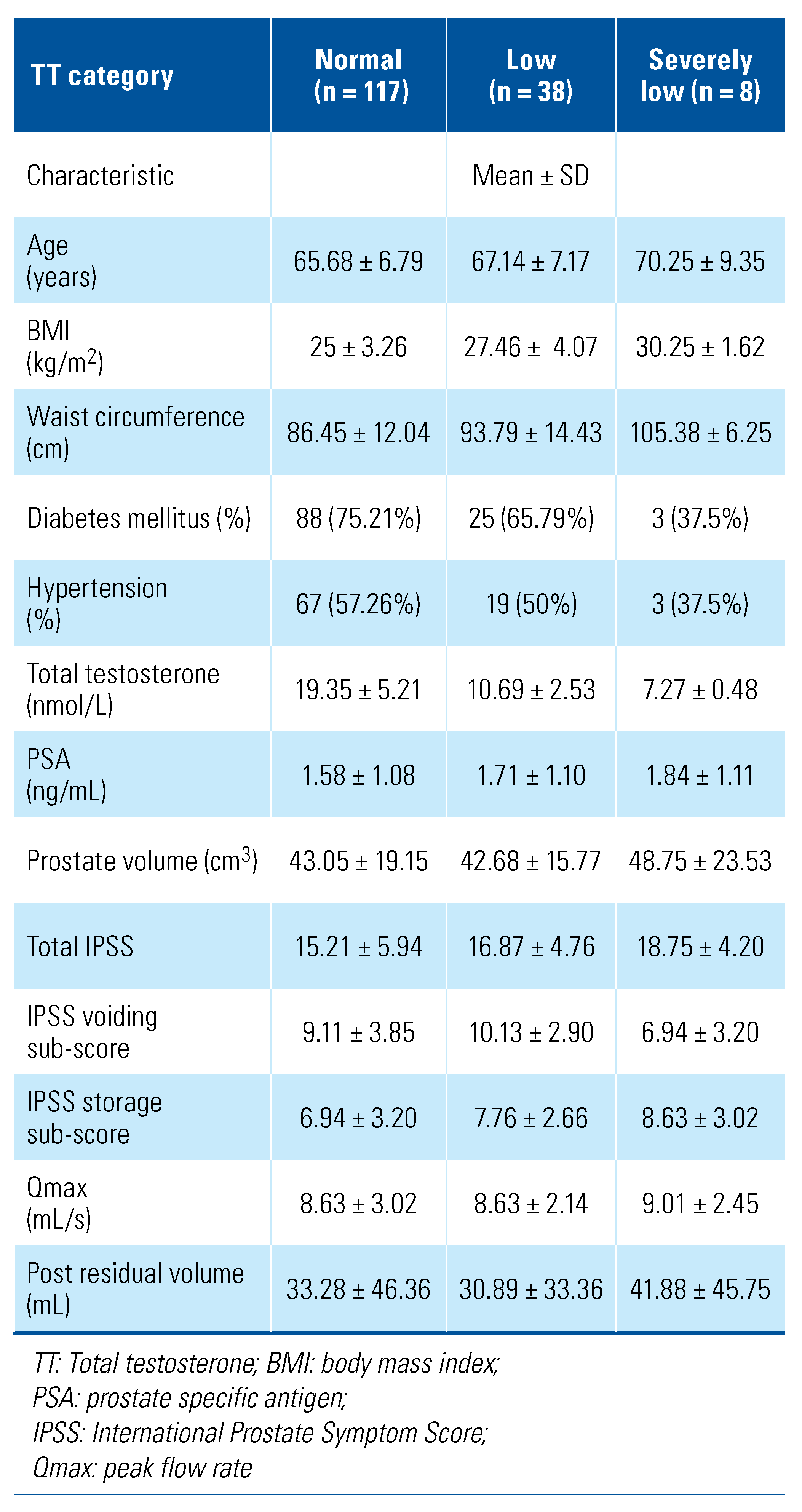
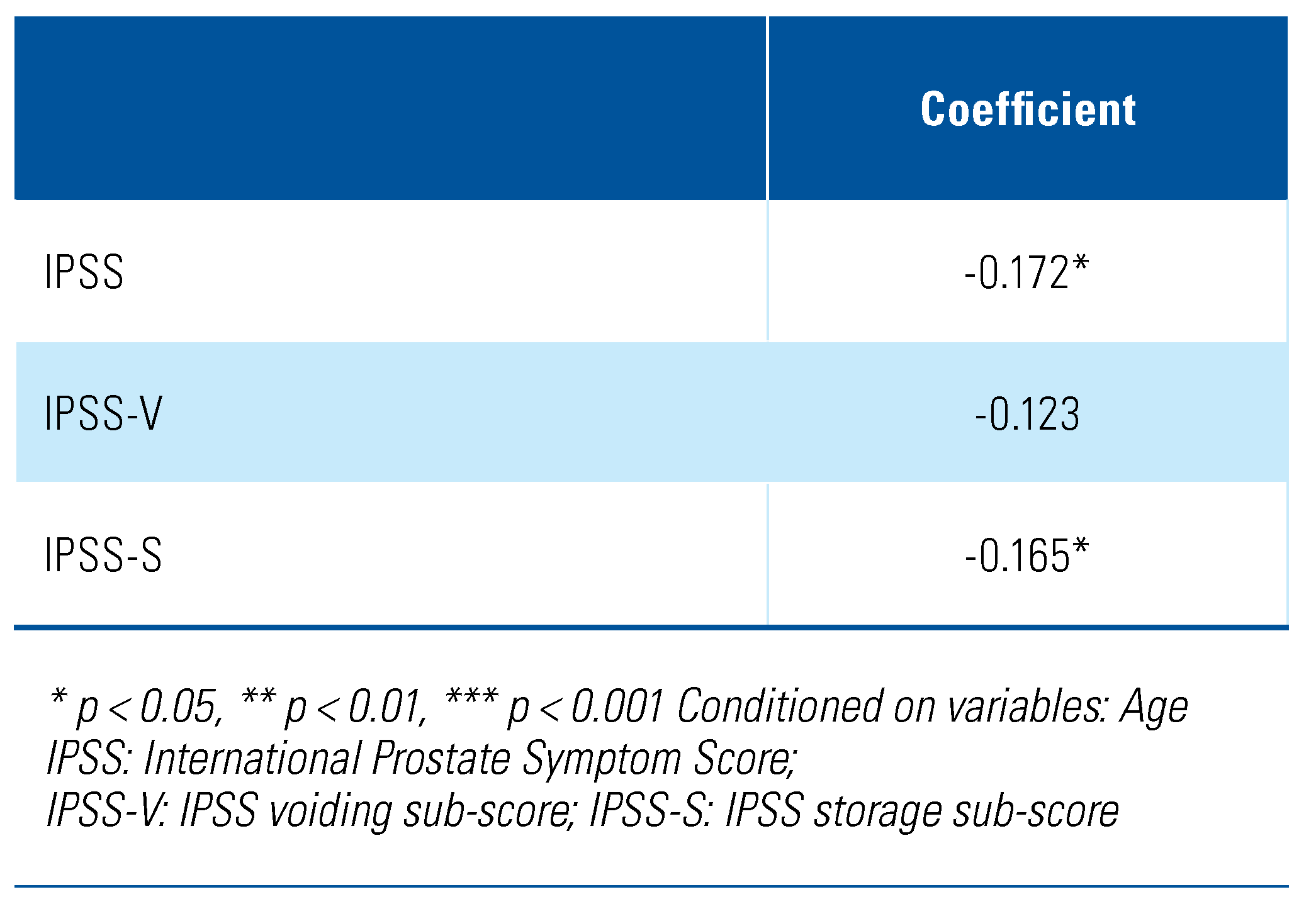
Results
Discussion
Conclusion
Acknowledgments
Competing Interests
Abbreviations
| BPH | benign prostatic hyperplasia |
| IPSS | International Prostate Symptoms Scoring |
| LUTS | lower urinary tract symptoms |
| TRT | testosterone replacement therapy |
| TT | total testosterone |
References
- Teh, G.C.; Sahabudin, R.M.; Lim, T.C.; Chong, W.L.; Woo, S.; Mohan, M.; et al. Prevalence of symptomatic BPE among Malaysian men aged 50 and above attending screening during prostate health awareness campaign. Med. J. Malaysia 2001, 56, 186–195. [Google Scholar]
- Feldman, H.A.; Longcope, C.; Derby, C.A.; Johannes, C.B.; Araujo, A.B.; Coviello, A.D.; et al. Age Trends in the level of serum testosterone and other hormones in middle-aged men: longitudinal results from the Massachusetts Male Aging Study. J. Clin. Endocrinol. Metab. 2002, 87, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.C.W.; Tajar, A.; Beynon, J.M.; Pye, S.R.; Silman, A.J.; Finn, J.D.; et al. Identification of late-onset hypogonadism in middle-aged and elderly men. N. Engl. J. Med. 2010, 363, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Crawford, E.D.; Poage, W.; Nyhuis, A.; Price, D.A.; Dowsett, S.A.; Muram, D. Effects of testosterone level on lower urinary tract symptoms. Am. J. Men’s Health 2016, 10, 440–442. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.H.; Chiang, H.S.; Yu, H.J. Serum testosterone levels significantly correlate with nocturia in men aged 40–79 years. Urology 2011, 78, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.C.; Huang, S.P.; Li, W.M.; Wang, C.J.; Chou, Y.H.; Li, C.C.; et al. Relationship between serum testosterone and measures of benign prostatic hyperplasia in aging men. Urology 2007, 70, 677–680. [Google Scholar] [CrossRef]
- Martin, S.A.; Haren, M.T.; Marshall, V.R.; Lange, K.; Wittert, G.A. Members of the Florey Adelaide Male Ageing Study. Prevalence and factors associated with uncomplicated storage and voiding lower urinary tract symptoms in community-dwelling Australian men. World J. Urol. 2011, 29, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.S.; Kim, J.H.; Yoon, Y.S.; Choi, H.; Park, J.Y.; Bae, J.H. Serum testosterone levels are negatively correlated with international prostate symptom score and transitional prostate volume. Low. Urin. Tract. Symptoms 2018, 10, 143–147. [Google Scholar] [CrossRef]
- EAU guideline. EAU Male Sexual and Reproductive health Guidelines. Edn. presented at the EAU Annual Congress Amsterdam; 2022; ISBN 978-94-92671-16-5. [Google Scholar]
- Berry, S.J.; Coffey, D.S.; Walsh, P.C.; Ewing, L.L. The development of human benign prostatic hyperplasia with age. J. Urol. 1984, 132, 474–479. [Google Scholar] [CrossRef]
- Partin, A.W.; Oesterling, J.E.; Epstein, J.I.; Horton, R.; Walsh, P.C. Influence of age and endocrine factors on the volume of benign prostatic hyperplasia. J. Urol. 1991, 145, 405–409. [Google Scholar] [CrossRef]
- Xia, B.W.; Zhao, S.C.; Chen, Z.P.; Chen, C.; Liu, T.S.; Yang, F.; et al. Relationship between serum total testosterone and prostate volume in aging men. Sci. Rep. 2021, 11, 14122. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, C.S.; Chalise, P.R.; Bhandari, B.B. Correlation of prostate volume with international prostate symptom score and quality of life in men with benign prostatic hyperplasia. Nepal. Med. Coll. J. 2008, 10, 104–107. [Google Scholar]
- Bosch, J.L.; Hop, W.C.; Kirkels, W.J.; Schröder, F.H. The International Prostate Symptom Score in a community-based sample of men between 55 and 74 years of age: prevalence and correlation of symptoms with age, prostate volume, flow rate and residual urine volume. Br. J. Urol. 1995, 75, 622–630. [Google Scholar] [CrossRef]
- Schatzl, G.; Brössner, C.; Schmid, S.; Kugler, W.; Roehrich, M.; Treu, T.; et al. Endocrine status in elderly men with lower urinary tract symptoms: correlation of age, hormonal status, and lower urinary tract function. The Prostate Study Group of the Austrian Society of Urology. Urology 2000, 55, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Khera, M.; Crawford, D.; Morales, A.; Salonia, A.; Morgentaler, A. A new era of testosterone and prostate cancer: from physiology to clinical implications. Eur. Urol. 2014, 65, 115–123. [Google Scholar] [CrossRef]
- Yassin, A.A.; El-Sakka, A.I.; Saad, F.; Gooren, L.J.G. Lower urinary-tract symptoms and testosterone in elderly men. World J. Urol. 2008, 26, 359–364. [Google Scholar] [CrossRef]
- Smet, P.J.; Jonavicius, J.; Marshall, V.R.; de Vente, J. Distribution of nitric oxide synthase-immunoreactive nerves and identification of the cellular targets of nitric oxide in guinea-pig and human urinary bladder by cGMP immunohistochemistry. Neuroscience 1996, 71, 337–348. [Google Scholar] [CrossRef]
- Shigehara, K.; Sugimoto, K.; Konaka, H.; Iijima, M.; Fukushima, M.; Maeda, Y.; et al. Androgen replacement therapy contributes to improving lower urinary tract symptoms in patients with hypogonadism and benign prostate hypertrophy: a randomised controlled study. Aging Male 2011, 14, 53–58. [Google Scholar] [CrossRef]
- Rastrelli, G.; Vignozzi, L.; Corona, G.; Maggi, M. Testosterone and benign prostatic hyperplasia. Sex. Med. Rev. 2019, 7, 259–271. [Google Scholar] [CrossRef]
- Tsujimura, A.; Miyagawa, Y.; Takezawa, K.; Okuda, H.; Fukuhara, S.; Kiuchi, H.; et al. Is low testosterone concentration a risk factor for metabolic syndrome in healthy middle-aged men? Urology 2013, 82, 814–819. [Google Scholar] [CrossRef]
- Kang, W.H.; Siruhan, M.; Shree, V.N.; Karupiah, M.; Sukor, N.; Kamaruddin, N.A. Prevalence of hypogonadism among male Type 2 diabetes mellitus patients in Pusat Perubatan Universiti Kebangsaan Malaysia. J. ASEAN Fed. Endocr. Soc. 2021, 36, 12. [Google Scholar] [CrossRef]
- Ho, C.C.; Singam, P.; Hong, G.E.; Zainuddin, Z.M. Male sexual dysfunction in Asia. Asian J. Androl. 2011, 13, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Tsuru, T.; Tsujimura, A.; Mizushima, K.; Kurosawa, M.; Kure, A.; Uesaka, Y.; et al. International Prostate Symptom Score and quality of life index for lower urinary tract symptoms are associated with aging males symptoms rating scale for late-onset hypogonadism symptoms. World J. Mens. Health 2022, 41, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Raynaud, J.P.; Gardette, J.; Rollet, J.; Legros, J.J. Prostate-specific antigen (PSA) concentrations in hypogonadal men during 6 years of transdermal testosterone treatment. BJU Int. 2013, 111, 880–890. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Zhang, Y. The effect of androgen-replacement therapy on prostate growth: a systematic review and meta-analysis. Eur. Urol. 2013, 64, 811–822. [Google Scholar] [CrossRef] [PubMed]
- Yassin, D.J.; El Douaihy, Y.; Yassin, A.A.; Kashanian, J.; Shabsigh, R.; Hammerer, P.G. Lower urinary tract symptoms improve with testosterone replacement therapy in men with late-onset hypogonadism: 5-year prospective, observational and longitudinal registry study. World J. Urol. 2014, 32, 1049–1054. [Google Scholar] [CrossRef] [PubMed]
- Kohn, T.P.; Mata, D.A.; Ramasamy, R.; Lipshultz, L.I. Effects of testosterone replacement therapy on lower urinary tract symptoms: A systematic review and meta-analysis. Eur. Urol. 2016, 69, 1083–1090. [Google Scholar] [CrossRef]
- Lee, M.H.; Shin, Y.S.; Kam, S.C. Correlation between testosterone replacement treatment and lower urinary tract symptoms. Int. Neurourol. J. 2021, 25, 12–22. [Google Scholar] [CrossRef]


This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2022 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.
Share and Cite
Shukor, S.; Inn, F.X.; Zainuddin, Z.M. Relationship Between Serum Testosterone and Severity of Lower Urinary Tract Symptoms among Malaysian Men. Soc. Int. Urol. J. 2022, 3, 296-302. https://doi.org/10.48083/POJQ7964
Shukor S, Inn FX, Zainuddin ZM. Relationship Between Serum Testosterone and Severity of Lower Urinary Tract Symptoms among Malaysian Men. Société Internationale d’Urologie Journal. 2022; 3(5):296-302. https://doi.org/10.48083/POJQ7964
Chicago/Turabian StyleShukor, Suzliza, Fam Xeng Inn, and Zulkifli Md Zainuddin. 2022. "Relationship Between Serum Testosterone and Severity of Lower Urinary Tract Symptoms among Malaysian Men" Société Internationale d’Urologie Journal 3, no. 5: 296-302. https://doi.org/10.48083/POJQ7964
APA StyleShukor, S., Inn, F. X., & Zainuddin, Z. M. (2022). Relationship Between Serum Testosterone and Severity of Lower Urinary Tract Symptoms among Malaysian Men. Société Internationale d’Urologie Journal, 3(5), 296-302. https://doi.org/10.48083/POJQ7964