Abstract
Purpose: Substantial evidence indicates that men with prostate cancer are at an increased risk for cardiovascular disease, and medical and surgical androgen deprivation therapy is associated with further increased cardiovascular risk. There are conflicting reports of differences in cardiovascular safety between gonadotropin-releasing hormone (GnRH) agonists and antagonists. The purpose of this narrative review is to compare data on the cardiovascular risks and safety outcomes associated with different hormonal treatment options in prostate cancer patients and to provide guidance on how to manage the increased risk associated with the condition. Methods: A PubMed search was conducted for papers published in the last 15 years using the following MeSH terms: “prostate neoplasms,” “gonadotropin-releasing hormone,” “androgen agonist,” “androgen antagonists,” “cardiovascular disease,” “epidemiology.” Results: Evidence regarding the risk of cardiovascular events during treatment with GnRH agonists and antagonists is conflicting. Some retrospective studies have shown that agonists are associated with a greater risk of cardiovascular disease and cardiovascular mortality and morbidity, and a similar risk with agonists and combined androgen blockade. Some studies have reported that antagonists are associated with a decreased risk of cardiovascular mortality and morbidity compared with agonists. With respect to coronary heart disease, ischemic heart disease, myocardial infarction, stroke, or sudden cardiac death, current evidence has failed to demonstrate a significant difference between antagonists and agonists. Cardiovascular risks in patients should be mitigated by regular monitoring of blood pressure, blood glucose, and lipids, as well as counseling patients to abstain from alcohol and improve their diet and exercise. Statins, metformin, and aspirin should also be considered. Conclusions: The evidence for the increased cardiovascular risk of GnRH agonists over antagonists for androgen deprivation therapy is unclear. Differences in methodology, population sizes, risk stratification, and outcomes between studies make direct comparisons problematic. The single prospective, randomized prostate cancer trial with a primary cardiovascular end point in men with pre-existing cardiovascular disease comparing GnRH agonist to antagonist was stopped early due to an interim futility analysis. The results are inconclusive.
Introduction
The burden of prostate cancer (PCa) is expected to increase owing to natural growth and aging of the global population [1]. Because of the high incidence-to-mortality ratio of PCa, cardiovascular (CV) disease (CVD) is the leading cause of death in these men [2,3]. Aside from the high prevalence of slow-growing malignancy, there is substantial evidence that men with PCa are at an increased risk for CVD because of comorbid risk factors [4,5]. An analysis of the Surveillance, Epidemiology and End Results (SEER) program of the US National Cancer Institute, a network of population-based incident tumor registries, showed that men with PCa had a higher risk of CVD and CVD than the average US resident, after adjusting for age, race, and sex over the same period [4].
Van Hemelrijck et al. found that patients with PCa on surveillance (n = 19 526) had an elevated standardized incidence ratio (SIR) for all CVD subtypes (myocardial infarction [MI], arrhythmia, ischemic heart disease, heart failure, and stroke) compared with the general population [6]. The SIR was greater in patients with no circulatory disease detected at baseline (range 1.15 to 1.49) for all subtypes except ischemic heart disease, which was more common in patients with circulatory disease at baseline.
PCa patients who have undergone surgical castration, or who are receiving medical androgen deprivation therapy (ADT), are at particularly high risk for CVD [6]. A cross-sectional analysis of the United States Veterans Health Administration population examined the association between CV risk factors in men with PCa receiving ADT versus those not receiving ADT [7]. Among the two-thirds of men who received CV risk factor assessments (blood pressure measurements, serum cholesterol levels, blood glucose levels), about half had ≥ 1 uncontrolled CV risk factor, and 30% of those were not receiving treatment for it. Patients with PCa who had a history of atherosclerotic CVD, whether taking ADT or not, had about a 20% lower risk of having an untreated CV risk factor compared with those without a history of CVD or those who had no history of ADT. Patients on ADT with no history of CVD had a 5% lower risk for an untreated CV risk factor compared with patients with a CVD history who were ADT-naïve [7]. This reflects the tendency for patients who have had a history of CVD to have more intensive management of their CV risk factors than those with no prior history. These data suggest that patients receiving ADT are at risk for the unrecognized development of CVD or CV-related mortality. Whether the association between ADT and CVD is because of differential patient monitoring or because of adverse effects of ADT (or both) remains an unanswered question. CV risks in men with PCa are driven by a number of factors, including age (which might itself predict underlying health conditions), high-fat diet, visceral adiposity and low levels of high-density lipoprotein (HDL), pre-existing CV risk factors, and metabolic syndrome [2,8,9,10].
Recently, there have been studies reporting differences in CV safety between gonadotropin-releasing hormone (GnRH) agonists and antagonists, with mixed results [11,12,13,14]. Some studies report differences in CV safety between GnRH agonists and antagonists in patients with pre-existing CVD, whereas others show no differences. Several mechanisms have been proposed to explain CV safety differences between GnRH agonists and antagonists, such as differences in follicle-stimulating hormone levels, and the interaction between the agonists and GnRH receptors in endothelial plaque macrophages. These hypothesis-generating explanations remain speculative. The only randomized prospective study with CV event endpoints was closed early after an interim analysis because of a very low probability that a difference would be observed between agonists and antagonists (futility analysis) [12]. The purpose of this review is to elucidate the data on the CV risks and safety outcomes associated with different ADT options in patients with PCa and to consider strategies for mitigation of their CV risk.
Search Method
A search was conducted using PubMed, and articles published after 2006 were included in the initial search. This allowed for research published in the past 15 years to be eligible for inclusion in the literature review. The search method is shown in Figure 1. After selection, 71 papers were included in this review.
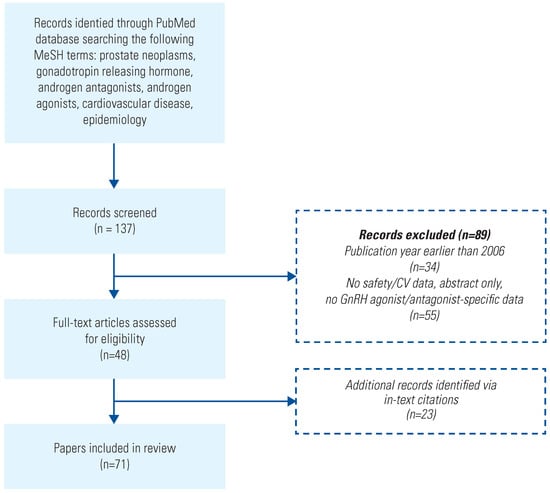
Figure 1.
Literature search.
CV Risks Reported With ADT
A landmark population-based study by Keating et al. (n = 73 196) using retrospective data obtained from the SEER database demonstrated that GnRH agonists were associated with a significantly increased risk of coronary heart disease (CHD), MI, and sudden cardiac death compared with ADT-naïve adult men ≥ 66 years of age with local or regional PCa. CHD was defined as an inpatient admission with a primary or secondary diagnosis code of ischemic heart disease or MI. Sudden cardiac death was defined as a primary or secondary diagnosis code of sudden death or life-threatening ventricular arrhythmia. Using Cox proportional hazard models and accounting for patient and tumor characteristics, the adjusted hazard ratios (aHRs) were 1.16 (P < 0.001), 1.11 (P = 0.03), and 1.16 (P = 0.004) for CHD, MI, and sudden cardiac mortality, respectively, when using a GnRH agonist. Furthermore, patients given GnRH agonists showed a significantly increased risk of CHD after only 1 to 4 months of treatment (aHR, 1.14; P = 0.007) compared with patients not receiving ADT. This risk stayed elevated as treatment duration continued for 5 to 12 months (aHR, 1.19; P < 0.001), 13 to 14 months (aHR, 1.11; P = 0.04), and ≥ 25 months (aHR, 1.18; P = 0.001) [15]. These results led to a 2010 joint statement from the American Urological Association, the American Society for Radiation Oncology, and the American Heart Association alerting clinicians to a potential relationship between ADT and CVD risk [16]. The US labels for GnRH agonists were revised to add a safety statement stating that an increased risk of MI, sudden cardiac death, and stroke has been reported in association with use of GnRH analogs in men. The safety statements emphasize the importance of monitoring for the development of CVD and managing patients appropriately [17,18,19,20].
Quantifying the CV Risk of ADT and the Importance of Pre-Existing CVD
Several studies suggest that patients with pre-existing CVD are particularly at risk from the CV effects of ADT. Gandaglia et al. found a 5-year cumulative CV mortality estimate of 14.8% in patients with metastatic PCa receiving ADT (ie, GnRH agonist and/or bilateral orchiectomy) with underlying CV risk factors versus 9.8% in those without baseline CV morbidities. Of the 9596 men on ADT, 31.8% had CV comorbidities (n = 3049) at baseline, and 1083 CV mortality events (11.3%) were recorded. Pre-existing CVD is the strongest predictor of CV mortality risk and warrants maximizing CV risk factor control before initiating ADT [21].
A similar observational study, also by Gandaglia et al. [22] assessed the 10-year cumulative incidence rates of CHD, MI, and CV mortality in patients with non-metastatic PCa. After propensity score matching and stratifying patients according to treatment type, the study found that patients using GnRH agonists (n = 28 988) had significantly greater incidence (P < 0.001) of CHD, MI, and CV mortality events of 26.9%, 16.6%, and 17.7%, respectively, compared with 25.1%, 14.8%, and 14.2%, respectively, for those not on ADT (n = 29984). A multivariable, competing-risks regression analysis of the score-matched GnRH agonist cohort identified a statistically significant (P < 0.001) rate increase in CHD (aHR, 1.11), MI (aHR, 1.09), and CV mortality (aHR, 1.18) [22]. These rates parallel those seen in Keating et al. (aHR, 1.16, 1.11, and 1.16, respectively) and reinforce the significance of ADT-associated CV risks [15].
In contrast, a meta-analysis by Zhao et al. in 2014 consisting of patients receiving ADT (GnRH agonist, antiandrogens, orchiectomy, or a combination of 2 or more treatments) (n = 129 802) and non-ADT users (n = 165 605) failed to find a significant relationship between ADT and CVD development (17.8% and 16.0%, P = 0.06, respectively) [23]. They did, however, find a significant relationship between CVD and GnRH agonists taken alone (aHR, 1.19; P = 0.01) and GnRH agonists plus antiandrogens (aHR, 1.46; P = 0.04), but not with ADT using antiandrogens alone (aHR, 0.95; P = 0.16). ADT use was significantly associated with a rise in CV mortality (aHR, 1.17; P = 0.01) compared with non-ADT use when the prevalence of CV mortality events was assessed (11.7% and 9.0%, respectively). GnRH agonists had a significantly higher risk of CV mortality compared with non-ADT (aHR, 1.36; P = 0.004), although men on GnRH agonists plus antiandrogen or those who had undergone orchiectomy had an even higher risk (aHR, 1.44; P < 0.001 and aHR, 1.69; P = 0.03, respectively). Although ADT did not have a significant association with MI incidence (P = 0.14), it did show a positive relationship with the GnRH agonist subgroup (aHR, 1.20; P = 0.008). Treatment with antiandrogens alone reduced the MI aHR to 0.88 (P = 0.002) [23].
Nguyen et al. performed another meta-analysis (n = 2200) that compared patients with non-metastatic PCa on GnRH agonists with those not on ADT (n = 1941) [24]. In this meta-analysis, GnRH agonist was not associated with a significant increase in risk for CV mortality (n = 255 events; relative risk [RR], 0.93; P = 0.41). Additional subgroup analyses of shortand long-term therapy, of supplemental therapy (ie, radiation), and of older age cohorts also failed to find an association between GnRH agonist use and a significant increase in CV mortality.
The evidence regarding the CV risks of ADT is thus inconclusive (Table 1) [25,26]. Various confounding factors have been proposed to explain the variability in these studies. These include (1) that ADT is often used for patients who are not considered for curative treatment. Men selected for ADT are typically older or in worse overall health and thereby may have an increased risk of CV mortality, although an important exception is the use of adjuvant ADT with radiation therapy; (2) the presence of unknown CVD risk factors in populations being studied is a potential confounder; and (3) patients with ADT in clinical trials are more likely to be closely monitored (so more likely that CV issues are detected) and treated than those in the general population [27].

Table 1.
Summary of CV risk factors for patients receiving androgen deprivation therapy.
The aim of ADT is to reduce serum testosterone levels to castrate levels (20 to 50 ng/dL); this promotes regression of the disease [28]. Patients with testosterone levels of >20 ng/dL (> 0.7 nmol/L) over the first year of ADT have a higher risk of dying, with an HR of 2.08 compared with those who have testosterone levels of < 20 ng/dL (< 0.7 nmol/L). For those whose level was > 50 ng/dL (> 1.7 nmol/L), the HR was higher still at 2.93 [29].
CV Risk with Orchiectomy
Most studies of the effect of ADT on CV health have grouped all patients receiving ADT together, whether castration is surgical or medical. Since all of these techniques achieve castrate levels of testosterone in most patients, the metabolic syndrome associated with ADT occurs regardless of method. However, some pre-clinical and clinical data suggest that the cardiovascular effects of surgical castration are greater than with medical castration. In the hyperglycemic male ApoE -/-:Ins2 +/Akita mouse model, orchiectomy induced greater weight gain, higher BMI, and necrotic plaque at the aortic root compared with LHRH agonist and antagonist [30]. The clinical data are more equivocal. Some studies that have addressed this question, but not all, have reported that men treated with surgical castration have a higher rate of CV disease than those treated with LHRH agonists [31,32,33].
CV Risk with GnRH Antagonists and Agonists
In addition to the general lack of clarity about the CVD risks of ADT, there is an uncertainty as to whether the link between ADT and CV events is primarily a function of the reduction in testosterone, or whether it is a specific effect related to the type of ADT drug, specifically GnRH agonists versus antagonists [16,23]. The difference in CV risk associated with use of GnRH agonists and antagonists has been summarized in Table 2.
Table 2.
Study compilation of CV risk assessment with GnRH agonists and antagonists in men with prostate cancer.
GnRH antagonists have been in clinical use since 2008 and have had a lower rate of use than their agonist counterparts. Therefore, there are fewer data on their correlation with CVD. Scailteux et al. performed a retrospective analysis of 2010 to 2013 French Health Reimbursement Agency and French hospital discharge database data for adult men (≥ 18 years) with PCa who were newly prescribed ADT using a composite endpoint of “ischemic events” (MI or ischemic stroke, whichever came first after ADT initiation). Of the total studied population (n = 35118), 71% of the patients received GnRH agonists versus 3.6% who received a GnRH antagonist. Relative to GnRH antagonists, agonist use did not have a significantly higher MI risk profile (aHR, 1.17; 95% CI 0.48 to 2.86 antagonist versus agonist using Cox proportional hazard model), nor an increased risk for ischemic stroke (aHR, 1.28; 95% CI 0.60 to 2.72 antagonist versus agonist). The overall mortality rate was the same for both agonists and antagonists (0.03 per 100 person-years), and incidence of ischemic events was lower for agonists (0.74 per 100 person-years) than for antagonists (0.87 per 100 person-years) [34]. Albertsen et al. [14] measured CV mortality and CVD among patients using GnRH agonists (leuprolide or goserelin n = 837) and the antagonist degarelix (n = 1491) by pooling data from 6 phase 3 prospective randomized trials (n = 2328). In men without pre-existing CVD, no differences in either the incidence of cardiac events or death form any cause was noted. In men with pre-existing CVD (n = 619), Cox regression modeling revealed an RR reduction of 56% of CV event or death with use of degarelix compared with GnRH agonists within 1 year of therapy initiation (aHR, 0.44; P = 0.002). In contrast, in this post hoc analysis, there were no significant differences in the incidence of a non-fatal cardiac event or death identified in patients without pre-existing CV morbidities. Follow-up was 1 year in 3 of the studies, and 3 months in the other 3. All of the recorded CV events occurred in the 3 longer studies of 12 months’ duration. Importantly, these trials were not designed to evaluate CV risk, nor were the events adjudicated by clinical CV event reviewers for their veracity. The authors also stated that the quality of the study data was “subject to bias” (according to The Cochrane Collaboration’s tool) because both patients and study personnel were not blinded regarding which form of ADT was administered.
A retrospective database analysis by Cardwell et al. compared the CVD risk rate of degarelix (n = 387) and GnRH agonists (including goserelin, leuprolide, triptorelin, and histrelin) use in men (n = 10 480) with newly diagnosed PCa versus untreated patients receiving active surveillance or watchful waiting (n = 4903) [35]. Using Cox regression modeling, Cardwell et al. determined that degarelix use had a 50% increased risk of CV events (71 events; aHR, 1.5; 95% CI, 1.2–1.9) compared with a 30% increased risk for GnRH agonists (2075 events; aHR, 1.3; 95% CI 1.2 to 1.4). GnRH agonists and degarelix continued to have an elevated CV event risk (20% to 50%) for both short-term (< 365 daily defined doses) and long-term use (≥ 365 daily defined doses). Further analysis revealed that GnRH agonist only use had a statistically significant risk increase of 20% for developing an MI (aHR, 1.2; 95% CI 1.0 to 1.5) relative to untreated patients. They also found that GnRH agonist use in patients with baseline CV morbidities had a 20% increased risk for a CV event (aHR, 1.2; 95% CI 1.0 to 1.3). Both GnRH agonists (aHR, 1.3; 95% CI 1.2 to 1.5) and degarelix (aHR, 1.8; 95% CI 1.3 to 2.6), however, had an elevated risk for CV events in patients without baseline CV morbidities relative to untreated patients. A recent meta-analysis by Ma et al. of 6 controlled studies (4 RCTs and 2 controlled clinical trials) concluded that the risk of CVD was the same for GnRH agonists as for GnRH antagonists for patients with PCa [36].
The prospective phase 3 HERO trial (n = 930) by Shore et al. compared the GnRH antagonist relugolix with the GnRH agonist leuprolide and identified a lower incidence of major adverse CV events (MACE) in the relugolix cohort [37]. However, the study was not powered to make distinctions in CV events. The reporting of CV events was based on a descriptive analysis of the non-adjudicated adverse events. The incidence of ischemic heart disease was reported as 2.4% for relugolix compared with 1.6% for leuprolide. The reported any-grade MACE incidence was 2.9% for relugolix versus 6.2% for leuprolide. Importantly, the incidences of grade 3 or 4 MACEs were identical (1.3%) [37]. Because the incidence of MACE grades 3 and 4 were identical between the 2 treatments and there was no adjudication by blinded clinical event reviewers, the clinical relevance of the difference in the incidence of all MACE events with relugolix compared with leuprolide should be treated with caution. The reported difference in MACE did not lead to a difference in castration resistance-free survival in the subgroup of men with metastatic disease treated with relugolix versus those treated with leuprolide (74% versus 75% of men, respectively; HR, 1.03, P = 0.84). MACEs were defined as non-fatal MI, non-fatal stroke, and all-cause mortality [37]. The US Food and Drug Administration have historically defined MACEs differently, as non-fatal MI, non-fatal stroke, and mortality due to CV causes when labeling traditional ADT drugs and testosterone replacement therapies [38]. The HERO study [37], however, defined MACEs differently from the Keating et al. [15] study and other phase 3 hormonal drug trials, making direct comparisons challenging [39,40].
A limitation of most ADT studies is that they were not designed, or statistically powered, to evaluate cardiac events. Rather they were reported as adverse events and may not have been comprehensive [14]. Directly comparing studies is also hindered by differences in methodology, risk stratification, and assessed outcomes.
The Cardwell et al. analysis comparing 6 studies acknowledged incomplete patient data sets (stage, Gleason score, lifestyle) that may have confounded the results. Medication adherence was determined via dispensing record, so actual adherence cannot be confirmed. Additionally, patients receiving ADT would have had increased monitoring and therefore there would have been an increased likelihood of CVD being identified [35]. In Scailteux et al., the composite outcome of “ischemic events” (MI or ischemic stroke, whichever came first) does not account for clinical differences among subgroup analyses (eg, MI and stroke are considered equal), and no significant heterogeneity was observed across these subgroups [34] This approach may have its limitations because a direct study comparison cannot be performed [36].
The Lopes et al. PRONOUNCE study was designed to determine whether there was a significant difference favoring GnRH antagonists versus agonists in patients with pre-existing CVD, as hypothesized from the retrospective Albertsen et al. meta-analysis described previously [12]. It was the first prospective, randomized CV outcomes study of men with advanced PCa receiving ADT. Unlike most other trials to date, including the HERO trial, there was a clinical event classification committee, composed of a cardiologist, a neurologist, and an oncologist, whose purpose was to provide independent, blinded adjudication of MACEs throughout the trial, as is the common standard for CV outcomes trials. In addition, the investigators were required to ensure that a cardiologist was treating the enrolled participant so that their CVD treatment was optimized. The primary outcome was the time from randomization to first occurrence of centrally adjudicated MACE. Key secondary outcomes were the time to first occurrence of CV-related death, non-fatal MI, or non-fatal stroke; time to first occurrence of CV-related death; and time to first occurrence of MI. The study had markedly fewer than expected MACE events. Sixty-six MACE events were required to reject the null hypothesis of equal hazard for degarelix and leuprolide. Hence, the study was terminated early after the enrollment of 545 participants (61% of the planned 900) owing to futility. The total number of MACE events recorded over 12 months was 26: 15 (5.5%) for degarelix, and 11 (4.1%) for leuprolide (P = 0.53). Thus, even if completed with full accrual, the study likely would have had insufficient statistical power to compare the relative CV safety of the 2 treatments with precision. The number of events for the secondary outcomes was also very low, and there were no significant differences between treatments for any of these outcomes.
A similar study by Wallach et al. was designed to replicate the PRONOUNCE trial, but using retrospective data from health care insurance claims [13]. This study could not replicate many features of the original prospective trial, including the assurance of having cardiologist involvement and adjudicated events, but used proxy selection criteria and outcomes to try to replicate it as closely as possible. The results from this realworld study are supportive of those in PRONOUNCE. Among propensity-matched patients (n = 2226), no significant difference was observed in the risk of MACEs (defined as a composite endpoint of death from any cause, MI, or stroke) between degarelix and leuprolide (10.18 versus 8.60 events per 100 person-years; HR, 1.18; P = 0.30). Degarelix was associated with a higher risk of death from any cause (HR, 1.48; P = 0.046) but not of MI (HR, 1.16; P = 0.66), stroke (HR, 0.92.; P = 0.81), or angina (HR, 1.36; P = 0.60).
In summary, the sole randomized, prospective CV outcome study did not demonstrate a difference in CV risk between GnRH agonists and antagonists. The event rate in this study was too low to provide sufficient power to identify a difference, and the evidence remains inconclusive. It is possible that the low event rate reflected the optimization of CV care provided to the patients in the trial.
Management of CV Risks in Men With PCa Who Are Receiving ADT
Patients with PCa who have undergone surgical castration, or are receiving medical ADT, are at particularly high risk for CVD [6]. Because of comorbid risk factors, men with PCa have a higher risk of CVD even if they are not receiving ADT [5,7], and those who have undergone surgical or medical castration with ADT are at an even higher risk for CVD and CV mortality [6]. Although many of the CV risks in men with PCa can be mitigated by controlling the underlying comorbid risk factors, recent data indicate that many are not being controlled [7]. In the recent Veterans Health Administration study, about half the population of men with PCa who were receiving ADT and who had been assessed had ≥ 1 uncontrolled CV risk factor, and almost one-third of those with important CV risk factors were not receiving treatment to control their CV risk factors, suggesting that PCa patients receiving ADT are not being adequately assessed or their underlying risk factors treated for CVD in accordance with the various consensus recommendations [7].
In addition to potentially undesirable side effects, such as decreased libido, impotence, decreased muscle mass, increased fat mass, anemia, fatigue, and osteoporosis, changes in patient body composition as a result of medical castration create the potential for more severe metabolic complications and CV morbidities. For instance, the increase of adipose tissue and body weight in patients receiving ADT could be associated with rising insulin levels; insulin resistance; and an elevation in HDL, low-density lipoprotein (LDL), and triglycerides. These conditions predispose individuals to diabetes and CV events (Figure 2) [41]. ADT, by reducing androgen levels, is thought to reduce the androgen-mediated inhibition of stem cell differentiation into adipocytes, thereby increasing visceral and subcutaneous fat and decreasing lean body mass [42]. This is a factor that may increase obesity and fat mass, which also contribute to insulin resistance and metabolic syndrome [10]. ADT may be associated with an increase in arterial wall thickness and endothelial dysfunction as a result of low testosterone levels; this change in vascular structure could promote atherosclerosis and could, eventually, lead to plaque rupture (Figure 3) [41].
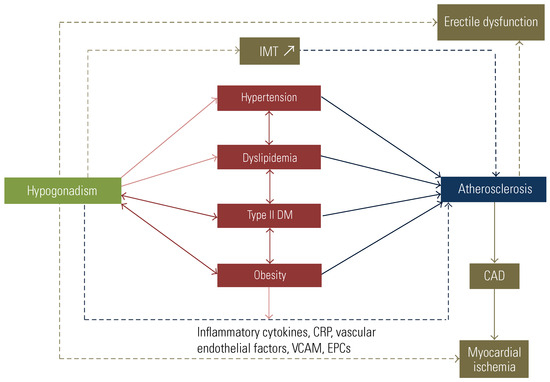
Figure 2.
Interconnections between hypogonadism and cardiovascular risk factors on atherosclerosis development.
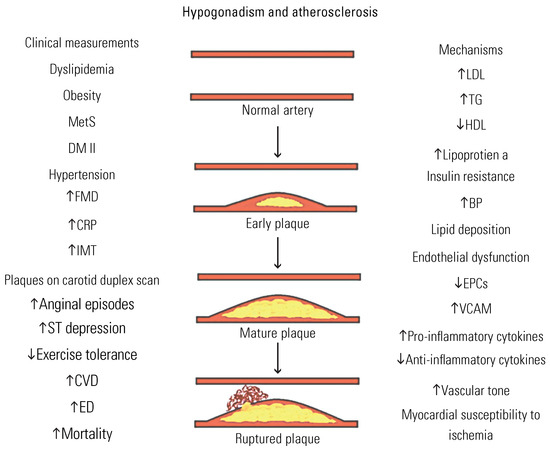
Figure 3.
Clinical measurements and resultant mechanistic processes in the relation between hypogonadism and specific stages of atherosclerosis.
Many associations have developed recommendations regarding assessment of baseline CVD in men initiating ADT [43,44,45,46,47]. Most guidelines offer generic advice. Men with CV comorbidities are encouraged to discuss treatment options with their care providers [41]. Risk mitigation strategies include an assessment of the patient’s CV health before the initiation of ADT and during treatment; frequent monitoring of blood pressure, blood glucose levels, and lipid profile; diet and regular exercise; cessation of smoking; and reduction in alcohol consumption (Figure 4). The American Heart Association (AHA) recommends that ADT users be treated with antihypertensive therapy to lower blood pressure to < 130/80 mmHg, as dictated by specific comorbidities, and with glucose-lowering therapies in prediabetic and diabetic individuals. The AHA also recommends low-dose aspirin therapy and statin therapy to reduce serum LDL levels to < 100 mg/dL [16]. The National Comprehensive Cancer Network also recommends that patients receiving ADT should be treated with statins and undergo frequent screening and monitoring for metabolic and CV disorders [48]. In a large observational study (n = 87 346) of men with advanced PCa being treated with ADT, Anderson-Carter et al. showed that those taking statins had longer overall survival (median, 6.5 years versus 4.0 years; P < 0.001) and decreased death from cancer (5-year Pca-specific survival [94.0% versus 87.3%; P < 0.001]) than those who were not statin users [49]. Another study of patients starting ADT showed that statin use was associated with reduced HRs for overall mortality and Pca-specific mortality [50]. Statins may exert their effect by competitively binding to the organic anionic transporter SLCO2B1, which decreases the level of dehydroepiandrosterone sulfate (a precursor of androgens such as dihydrotestosterone), thereby depriving the tumor of endogenous androgens [51]. Interventional studies have also found potential benefits in the use of metformin combined with lifestyle changes in men receiving ADT. The rationale for its use is based on its ability to reduce hyperinsulinemia and improve metabolic syndrome. A systematic review and meta-analysis of 30 cohort studies in patients with PCa (n = 1 660 795) concluded that metformin treatment improves overall survival (HR, 0.72; P = 0.001), Pca-specific survival (HR, 0.78; P = 0.001), and recurrence-free survival (HR, 0.60; P = 0.001) compared with non-metformin treatment [52]. The risk reduction was also seen in those patients receiving ADT who had an overall survival HR of 0.77 and a Pca-specific survival of 0.72 (P < 0.00001 for both) [52,53]. Metformin use has also led to improvements in abdominal girth in men with PCa after 6 months of ADT treatment compared with the control population (mean 0.58% reduction for metformin group versus 2.15% increase for the control), as well as in weight (3.19% decrease versus 2.18% increase), body mass index (3.15% decrease versus 2.10% increase), and systolic blood pressure (5.96% decrease versus 1.77% increase) [54].
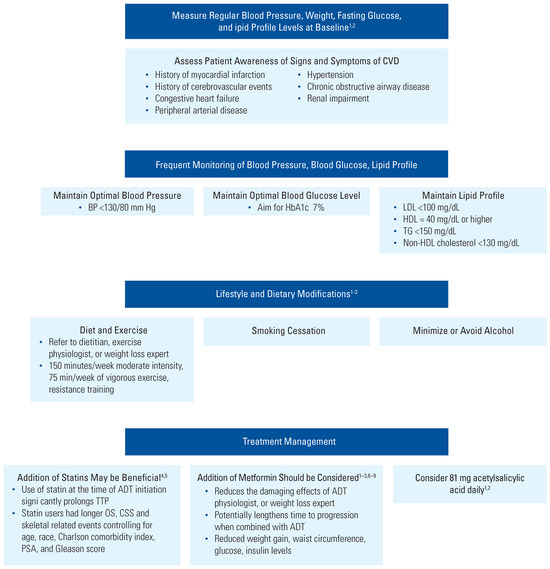
Figure 4.
CVD risk mitigation and recommended management for men receiving ADT.
Conclusions
Men with PCa have a higher risk for CVD than those without PCa, and there is substantial evidence that ADT increases this risk, although the evidence is not conclusive. In these men, CV history and the CV risk factors that may trigger a MACE should be evaluated and steps taken to mitigate them. The published CV risk data for GnRH agonists and antagonists are inconsistent and reflect different populations, sizes, and study designs. The only rigorous, prospective, randomized trial comparing CV events for men with pre-existing CVD receiving a GnRH agonist or antagonist was inconclusive over the time period studied, and the study was discontinued owing to there being insufficient events to achieve adequate power. There is currently no prospective study that will resolve this issue. Although the data are conflicting, both GnRH agonists and antagonists are associated with increased CVD and CV mortality, but no randomized controlled trial (versus pooled approaches) supports the hypothesis of a CV risk difference between GnRH agonists and antagonists. An important factor to mitigate potential adverse events associated with receiving ADT is to promote patient awareness of the increased risk of CVD and to provide education on how to improve CV health. This includes careful monitoring and lowering of blood pressure, glucose levels, and total and LDL cholesterol levels by making appropriate lifestyle changes and by using statins for hyperlipidemia. However, the focus of CV risk in people with PCa should be mitigation strategies with individualized treatment options addressed by experienced cardiologists or cardio-oncologists working with urologists and oncologists.
Funding
AbbVie (North Chicago, IL) sponsored the editorial assistance for this review and approved the final version. No honoraria and payments were made for authorship.
Acknowledgments
Editorial support was provided by Connor Hunter, PharmD, and Robin Smith, PhD, of The Curry Rockefeller Group, LLC (Tarrytown, NY), and was funded by AbbVie (North Chicago, IL). Additional thanks go to Gabriel Krigsfeld, PhD, of AbbVie (Mettawa, IL), for providing support in the writing of the paper.
Conflicts of Interest
Laurence Klotz has no competing interests to declare. Stephen Van Komen and Sanja Dragnic are employees of and own stock in AbbVie. William B. White has received personal fees for cardiovascular drug safety consulting (including data safety monitoring boards, cardiovascular endpoint committees, and data analysis) to AbbVie, Alnylam, AstraZeneca, Bristol-Myers Squibb, Jazz, Marius, Mylan, Takeda-Millennium, and TerSera. He also receives royalties from Wolters Kluwer as an editor of UptoDate.
Abbreviations
| ADT | androgen deprivation therapy CVD cardiovascular disease |
| GnRH | gonadotropin-releasing hormone MI myocardial infarction |
| PCa | prostate cancer |
| SIR | standardized incidence ratio |
References
- Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Cancer Stat Facts: Prostate Cancer. Available online: https://seer.cancer.gov/statfacts/html/prost.html (accessed on 11 November 2021).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Sturgeon, K.M.; Deng, L.; Bluethmann, S.M.; Zhou, S.; Trifiletti, D.M.; Jiang, C.; et al. A population-based study of cardiovascular disease mortality risk in US cancer patients. Eur. Heart J. 2019, 40, 3889–3897. [Google Scholar] [CrossRef] [PubMed]
- Koene, R.J.; Prizment, A.E.; Blaes, A.; Konety, S.H. Shared risk factors in cardiovascular disease and cancer. Circulation 2016, 133, 1104–1114. [Google Scholar] [CrossRef] [PubMed]
- Van Hemelrijck, M.; Garmo, H.; Holmberg, L.; Ingelsson, E.; Bratt, O.; Bill-Axelson, A.; et al. Absolute and relative risk of cardiovascular disease in men with prostate cancer: Results from the Population-Based PCBaSe Sweden. J. Clin. Oncol. 2010, 28, 3448–3456. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Parikh, R.B.; Hubbard, R.A.; Cashy, J.; Takvorian, S.U.; Vaughn, D.J.; et al. Assessment and management of cardiovascular risk factors among US veterans with prostate cancer. JAMA Netw. Open. 2021, 4, e210070. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, N.; Santos, M.; Jones, L.W.; Beckman, J.A.; Penson, D.F.; Morgans, A.; et al. Cardiovascular effects of androgen deprivation therapy for the treatment of prostate cancer: ABCDE steps to reduce cardiovascular disease in patients with prostate cancer. Circulation 2016, 133, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Punnen, S.; Cooperberg, M.R.; Sadetsky, N.; Carroll, P.R. Androgen deprivation therapy and cardiovascular risk. J. Clin. Oncol. 2011, 29, 3510–3516. [Google Scholar] [CrossRef] [PubMed]
- Zareba, P.; Duivenvoorden, W.; Leong, D.P.; Pinthus, J.H. Androgen deprivation therapy and cardiovascular disease: What is the linking mechanism? Ther. Adv. Urol. 2016, 8, 118–129. [Google Scholar] [CrossRef]
- Ahmadi, H.; Daneshmand, S. Androgen deprivation therapy for prostate cancer: Long-term safety and patient outcomes. Patient Relat. Outcome Meas. 2014, 5, 63–70. [Google Scholar] [CrossRef]
- Lopes, R.D.; Higano, C.S.; Slovin, S.F.; Nelson, A.J.; Bigelow, R.; Sørensen, P.S.; et al. Cardiovascular safety of degarelix versus leuprolide in patients with prostate cancer: The primary results of the PRONOUNCE Randomized Trial. Circulation 2021, 144, 1295–1307. [Google Scholar] [CrossRef] [PubMed]
- Wallach, J.D.; Deng, Y.; McCoy, R.G.; Dhruva, S.S.; Herrin, J.; Berkowitz, A.; et al. Real-world cardiovascular outcomes associated with degarelix vs. leuprolide for prostate cancer treatment. JAMA Netw. Open. 2021, 4, e2130587. [Google Scholar] [CrossRef] [PubMed]
- Albertsen, P.C.; Klotz, L.; Tombal, B.; Grady, J.; Olesen, T.K.; Nilsson, J. Cardiovascular morbidity associated with gonadotropin releasing hormone agonists and an antagonist. Eur. Urol. 2014, 65, 565–573. [Google Scholar] [CrossRef]
- Keating, N.L.; O’Malley, A.J.; Smith, M.R. Diabetes and cardiovascular disease during androgen deprivation therapy for prostate cancer. J. Clin. Oncol. 2006, 24, 4448–4456. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; D’Amico, A.V.; Berger, P.; Clark, P.E.; Eckel, R.H.; Keating, N.L.; et al. Androgen-deprivation therapy in prostate cancer and cardiovascular risk: A science advisory from the American Heart Association, American Cancer Society, and American Urological Association: Endorsed by the American Society for Radiation Oncology. CA Cancer J. Clin. 2010, 60, 194–201. [Google Scholar] [CrossRef] [PubMed]
- AbbVie Inc. Lupron-Depot (Leuprolide Acetate for Depot Suspension): Prescribing Information Full Prescribing Information; AbbVie, Inc.: North Chicago, IL, USA, 2019. [Google Scholar]
- Foresee Pharmaceuticals. CAMCEVI (Leuprolide) Injectable Emulsion, for Subcutaneous Use (Prescribing Information). Available online: https://www. accessdata.fda.gov/drugsatfda_docs/label/2021/211488s000lbl.pdf (accessed on 10 October 2021).
- Shore, N.; Mincik, I.; DeGuenther, M.; Student VJr Jievaltas, M.; Patockova, J.; et al. A phase 3, open-label, multicenter study of a 6-month pre-mixed depot formulation of leuprolide mesylate in advanced prostate cancer patients. World J. Urol. 2020, 38, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Tolmar Pharmaceuticals Inc. Eligard (Leuprolide Acetate) for Injectable Suspension, for Subcutaneous Use (Prescribing Information). Available online: https://eligardhcp.com/sites/default/files/pdfs/ELI_Full_PI.pdf (accessed on 13 July 2021).
- Gandaglia, G.; Sun, M.; Popa, I.; Schiffmann, J.; Trudeau, V.; Shariat, S.F.; et al. Cardiovascular mortality in patients with metastatic prostate cancer exposed to androgen deprivation therapy: A population-based study. Clin. Genitourin Cancer. 2015, 13, e123–e130. [Google Scholar] [CrossRef] [PubMed]
- Gandaglia, G.; Sun, M.; Popa, I.; Schiffmann, J.; Abdollah, F.; Trinh, Q.-D.; et al. The impact of androgen-deprivation therapy (ADT) on the risk of cardiovascular (CV) events in patients with non-metastatic prostate cancer: A population-based study. BJU Int. 2014, 114, E82–E89. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhu, S.; Sun, L.; Meng, F.; Zhao, L.; Zhao, Y.; et al. Androgen deprivation therapy for prostate cancer is associated with cardiovascular morbidity and mortality: A meta-analysis of population-based observational studies. PLoS ONE 2014, 9, e107516. [Google Scholar] [CrossRef]
- Nguyen, P.L.; Je, Y.; Schutz, F.A.; Hoffman, K.E.; Hu, J.C.; Parekh, A.; et al. Association of androgen deprivation therapy with cardiovascular death in patients with prostate cancer: A meta-analysis of randomized trials. JAMA 2011, 306, 2359–2366. [Google Scholar] [CrossRef]
- Melloni, C.; Slovin, S.F.; Blemings, A.; Goodman, S.G.; Evans, C.P.; Nilsson, J.; et al. Cardiovascular safety of degarelix versus leuprolide for advanced prostate cancer. JACC CardioOncology 2020, 2, 70–81. [Google Scholar] [CrossRef]
- A Trial Comparing Cardiovascular Safety of Degarelix Versus Leuprolide in Patients With Advanced Prostate Cancer and Cardiovascular Disease (PRONOUNCE) (NCT02663908). Available online: https://clinicaltrials.gov/ct2/show/NCT02663908?term=degarelix+leuprolide+acetate&cond=Prostate+Cancer&draw=2 (accessed on 13 July 2021).
- Rhee, H.; Gunter, J.H.; Heathcote, P.; Ho, K.; Stricker, P.; Corcoran, N.M.; et al. Adverse effects of androgen-deprivation therapy in prostate cancer and their management. BJU Int. 2015, 115 (Suppl. 5), 3–13. [Google Scholar] [CrossRef]
- Huggins, C.; Hodges, C.V. Studies on prostatic cancer: II. The effects of castration on advanced carcinoma of the prostate gland. Arch. Surg. 1941, 43, 209–223. [Google Scholar] [CrossRef]
- Klotz, L.; O’Callaghan, C.; Ding, K.; Toren, P.; Dearnaley, D.; Higano, C.S.; et al. Nadir testosterone within first year of androgen-deprivation therapy (ADT) predicts for time to castration-resistant progression: A secondary analysis of the PR-7 trial of intermittent versus continuous ADT. J. Clin. Oncol. 2015, 33, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Duivenvoorden, W.C.M.; Naeim, M.; Hopmans, S.N.; Yousef, S.; Werstuck, G.H.; Dason, S.; et al. Protective effect of pharmacological castration on metabolic perturbations and cardiovascular disease in the hyperglycemic male ApoE(-/-):Ins2(+/Akita) mouse model. Prostate Cancer Prostatic Dis. 2021, 24, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.Y.; See, L.C.; Liu, J.R.; Chuang, C.K.; Pang, S.T.; Hsieh, I.C.; et al. Risk of cardiovascular ischemic events after surgical castration and gonadotropin-releasing hormone agonist therapy for prostate cancer: A nationwide cohort study. J. Clin. Oncol. 2017, 35, 3697–3705. [Google Scholar] [CrossRef] [PubMed]
- Kan, W.C.; Hsieh, K.L.; Chen, Y.C.; Ho, C.H.; Hong, C.S.; Chiang, C.Y.; et al. Comparison of surgical or medical castration-related cardiotoxicity in patients with prostate cancer. J. Urol. 2022, 207, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, F.B.; Sandin, F.; Garmo, H.; Lissbrant, I.F.; Ahlgren, G.; Van Hemelrijck, M.; et al. Gonadotropin-releasing hormone agonists, orchiectomy, and risk of cardiovascular disease: Semi-ecologic, nationwide, population-based study. Eur. Urol. 2017, 72, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Scailteux, L.M.; Vincendeau, S.; Balusson, F.; Leclercq, C.; Happe, A.; Le Nautout, B.; et al. Androgen deprivation therapy and cardiovascular risk: No meaningful difference between GnRH antagonist and agonists-a nationwide population-based cohort study based on 2010-2013 French health insurance data. Eur. J. Cancer. 2017, 77, 99–108. [Google Scholar] [CrossRef]
- Cardwell, C.R.; O’Sullivan, J.M.; Jain, S.; Harbinson, M.T.; Cook, M.B.; Hicks, B.M.; et al. The risk of cardiovascular disease in prostate cancer patients receiving androgen deprivation therapies. Epidemiology 2020, 31, 432–440. [Google Scholar] [CrossRef]
- Ma, C.; Abeysekera, I.R.; Xu, W.; Wang, Y.; Peng, J.; Li, H. Comparing the risk of cardiovascular disease following GnRH agonist and GnRH antagonist therapy for patient with prostate cancer: A systematic review and meta-analysis. Minerva Urol. Nephrol. 2021, 73, 276–282. [Google Scholar] [CrossRef]
- Shore, N.D.; Saad, F.; Cookson, M.S.; George, D.J.; Saltzstein, D.R.; Tutrone, R.; et al. Oral relugolix for androgen-deprivation therapy in advanced prostate cancer. N. Engl. J. Med. 2020, 382, 2187–2196. [Google Scholar] [CrossRef]
- Chong, W.H. Endocrinologic and Metabolic Drugs Advisory Committee meeting. In Proceedings of the FDA Advisory Committee Meeting, Silver Spring, MD, USA, 24–25 October 2018. [Google Scholar]
- AbbVie Inc. AndroGel (testosterone gel 1% ). In Full Prescribing Information; AbbVie Inc.: North Chicago, IL, USA, 2019. [Google Scholar]
- AbbVie Inc. Lupron-Depot (leuprolide acetate for depot suspension). In Full Prescribing Information; AbbVie Inc.: North Chicago, IL, USA, 2019. [Google Scholar]
- Conteduca, V.; Di Lorenzo, G.; Tartarone, A.; Aieta, M. The cardiovascular risk of gonadotropin releasing hormone agonists in men with prostate cancer: An unresolved controversy. Crit. Rev. Oncol. Hematol. 2013, 86, 42–51. [Google Scholar] [CrossRef]
- Chazenbalk, G.; Singh, P.; Irge, D.; Shah, A.; Abbott, D.H.; Dumesic, D.A. Androgens inhibit adipogenesis during human adipose stem cell commitment to preadipocyte formation. Steroids 2013, 78, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Cassinello, J.; Arranz, J.A.; Piulats, J.M.; Sánchez, A.; Pérez-Valderrama, B.; Mellado, B.; et al. SEOM clinical guidelines for the treatment of metastatic prostate cancer (2017). Clin. Transl. Oncol. 2018, 20, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, A.; Bastian, P.J.; Bellmunt, J.; et al. EAU guidelines on prostate cancer. Part 1: Screening, diagnosis, and local treatment with curative intent-update 2013. Eur. Urol. 2014, 65, 124–137. [Google Scholar] [CrossRef]
- Heidenreich, A.; Bastian, P.J.; Bellmunt, J.; Bolla, M.; Joniau, S.; van der Kwast, T.; et al. EAU guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur. Urol. 2014, 65, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Mohler, J.L.; Antonarakis, E.S.; Armstrong, A.J.; D’Amico, A.V.; Davis, B.J.; Dorff, T.; et al. Prostate Cancer, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2019, 17, 479–505. [Google Scholar] [CrossRef]
- Morris, M.J.; Rumble, R.B.; Basch, E.; Hotte, S.J.; Loblaw, A.; Rathkopf, D.; et al. Optimizing anticancer therapy in metastatic non-castrate prostate cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1521–1539. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines Version 2. 2021 Prostate Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 3 March 2021).
- Anderson-Carter, I.; Posielski, N.; Liou, J.I.; Khemees, T.A.; Downs, T.M.; Abel, E.J.; et al. The impact of statins in combination with androgen deprivation therapy in patients with advanced prostate cancer: A large observational study. Urol. Oncol. 2019, 37, 130–137. [Google Scholar] [CrossRef]
- Hamilton, R.J.; Ding, K.; Crook, J.M.; O’Callaghan, C.J.; Higano, C.S.; Dearnaley, D.P.; et al. The association between statin use and outcomes in patients initiating androgen deprivation therapy. Eur. Urol. 2021, 79, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Harshman, L.C.; Wang, X.; Nakabayashi, M.; Xie, W.; Valenca, L.; Werner, L.; et al. Statin use at the time of initiation of androgen deprivation therapy and time to progression in patients with hormone-sensitive prostate cancer. JAMA Oncol. 2015, 1, 495–504. [Google Scholar] [CrossRef]
- He, K.; Hu, H.; Ye, S.; Wang, H.; Cui, R.; Yi, L. The effect of metformin therapy on incidence and prognosis in prostate cancer: A systematic review and meta-analysis. Sci. Rep. 2019, 9, 2218. [Google Scholar] [CrossRef] [PubMed]
- Richards, K.A.; Liou, J.I.; Cryns, V.L.; Downs, T.M.; Abel, E.J.; Jarrard, D.F. Metformin use is associated with improved survival for patients with advanced prostate cancer on androgen deprivation therapy. J. Urol. 2018, 200, 1256–1263. [Google Scholar] [CrossRef] [PubMed]
- Nobes, J.P.; Langley, S.E.; Klopper, T.; Russell-Jones, D.; Laing, R.W. A prospective, randomized pilot study evaluating the effects of metformin and lifestyle intervention on patients with prostate cancer receiving androgen deprivation therapy. BJU Int. 2012, 109, 1495–1502. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, A.V.; Chen, M.H.; Renshaw, A.A.; Loffredo, M.; Kantoff, P.W. Androgen suppression and radiation vs. radiation alone for prostate cancer: A randomized trial. JAMA 2008, 299, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Faris, J.E.; Smith, M.R. Metabolic sequelae associated with androgen deprivation therapy for prostate cancer. Curr. Opin. Endocrinol. Diabetes Obes. 2010, 17, 240–246. [Google Scholar] [CrossRef] [PubMed]
- O’Farrell, S.; Garmo, H.; Holmberg, L.; Adolfsson, J.; Stattin, P.; Van Hemelrijck, M. Risk and timing of cardiovascular disease after androgen-deprivation therapy in men with prostate cancer. J. Clin. Oncol. 2015, 33, 1243–1251. [Google Scholar] [CrossRef] [PubMed]
- Bosco, C.; Bosnyak, Z.; Malmberg, A.; Adolfsson, J.; Keating, N.L.; Van Hemelrijck, M. Quantifying observational evidence for risk of fatal and nonfatal cardiovascular disease following androgen deprivation therapy for prostate cancer: A meta-analysis. Eur. Urol. 2015, 68, 386–396. [Google Scholar] [CrossRef]
- Lester, J.F.; Mason, M.D. Cardiovascular effects of hormone therapy for prostate cancer. Drug Healthc. Patient Saf. 2015, 7, 129–138. [Google Scholar] [CrossRef]
- Meng, F.; Zhu, S.; Zhao, J.; Vados, L.; Wang, L.; Zhao, Y.; et al. Stroke related to androgen deprivation therapy for prostate cancer: A meta-analysis and systematic review. BMC Cancer 2016, 16, 180. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Lee Chuy, K.; Yang, J.C.; Bates, M.; Lombardo, M.; Steingart, R.M. Cardiovascular and metabolic effects of androgen-deprivation therapy for prostate cancer. J. Oncol. Pract. 2018, 14, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Nanda, A.; Chen, M.H.; Braccioforte, M.H.; Moran, B.J.; D’Amico, A.V. Hormonal therapy use for prostate cancer and mortality in men with coronary artery disease-induced congestive heart failure or myocardial infarction. JAMA 2009, 302, 866–873. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Klotz, L.; Persson, B.E.; Olesen, T.K.; Wilde, A.A. Cardiovascular safety of degarelix: Results from a 12-month, comparative, randomized, open label, parallel group phase III trial in patients with prostate cancer. J. Urol. 2010, 184, 2313–2319. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Klotz, L.; van der Meulen, E.; Colli, E.; Tanko, L.B. Gonadotropin-releasing hormone blockers and cardiovascular disease risk: Analysis of prospective clinical trials of degarelix. J. Urol. 2011, 186, 1835–1842. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Klotz, L.; Miller, K.; Crawford, E.D.; Shore, N.; Tombal, B.; Karup, C.; et al. Disease control outcomes from analysis of pooled individual patient data from five comparative randomized clinical trials of degarelix versus luteinizing hormone-releasing hormone agonists. Eur. Urol. 2014, 66, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Haque, R.; UlcickasYood, M.; Xu, X.; Cassidy-Bushrow, A.E.; Tsai, H.-T.; Keating, N.L.; et al. Cardiovascular disease risk and androgen deprivation therapy in patients with localized prostate cancer: A prospective cohort study. Br. J. Cancer 2017, 117, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Fahed, A.C.; Gholmieh, J.M.; Azar, S.T. Connecting the lines between hypogonadism and atherosclerosis. Int. J. Endocrinol. 2012, 2012, 793953. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; et al. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Galvão, D.A.; Taaffe, D.R.; Spry, N.; Gardiner, R.A.; Taylor, R.; Risbridger, G.P.; et al. Enhancing active surveillance of prostate cancer: The potential of exercise medicine. Nat. Rev. Urol. 2016, 13, 258–265. [Google Scholar] [CrossRef]
- Saraei, P.; Asadi, I.; Kakar, M.A.; Moradi-Kor, N. The beneficial effects of metformin on cancer prevention and therapy: A comprehensive review of recent advances. Cancer Manag. Res. 2019, 11, 3295–3313. [Google Scholar] [CrossRef] [PubMed]
- Alghandour, R.; Ebrahim, M.A.; Elshal, A.M.; Ghobrial, F.; Elzaafarany, M.; Elbaiomy, M. 617MO Repurposing metformin as an anticancer drug: Preliminary results of randomized controlled trial in advanced prostate cancer (MANSMED). Ann. Oncol. 2020, 31, S511. [Google Scholar] [CrossRef]





This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2022 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.