
Challenges and Impacts of COVID-19 Pandemic on Global Waste Management Systems: A Review




Abstract
:1. Introduction
1.1. Off-Putting Impacts of COVID-19 Scenario on Environments
1.1.1. Escalation in Wastes
1.1.2. Diminution of Waste Recycling
1.2. Research Methodology
1.3. Types of Waste Generated in COVID-19
1.3.1. Use of PPE
1.3.2. Use of Masks
1.3.3. Use of Gloves
1.3.4. Use of Goggles and Protective Face Shields/Face Screens
1.3.5. Use of Gowns and Protective Clothing
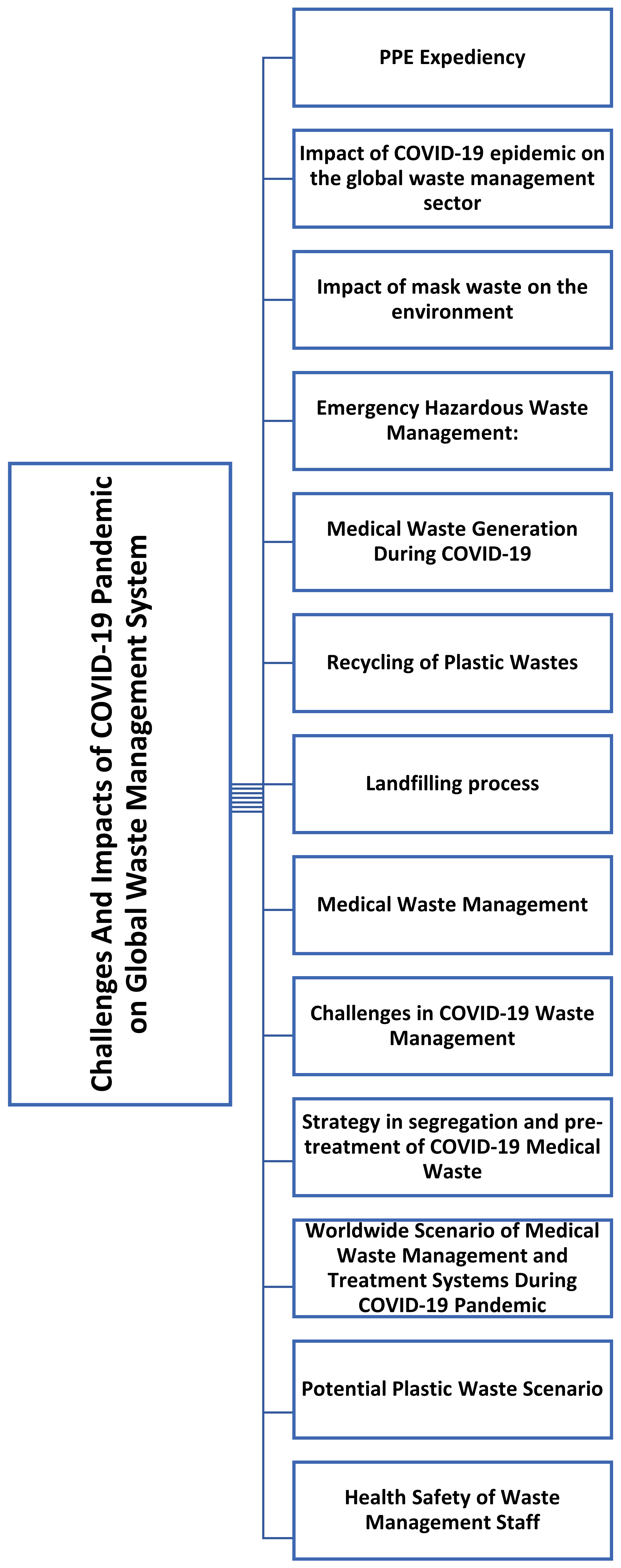
2. Impact of the COVID-19 Pandemic on the Global Waste Management Sector
2.1. Impact of Mask Waste on the Environment
2.2. Emergency Hazardous Waste Management
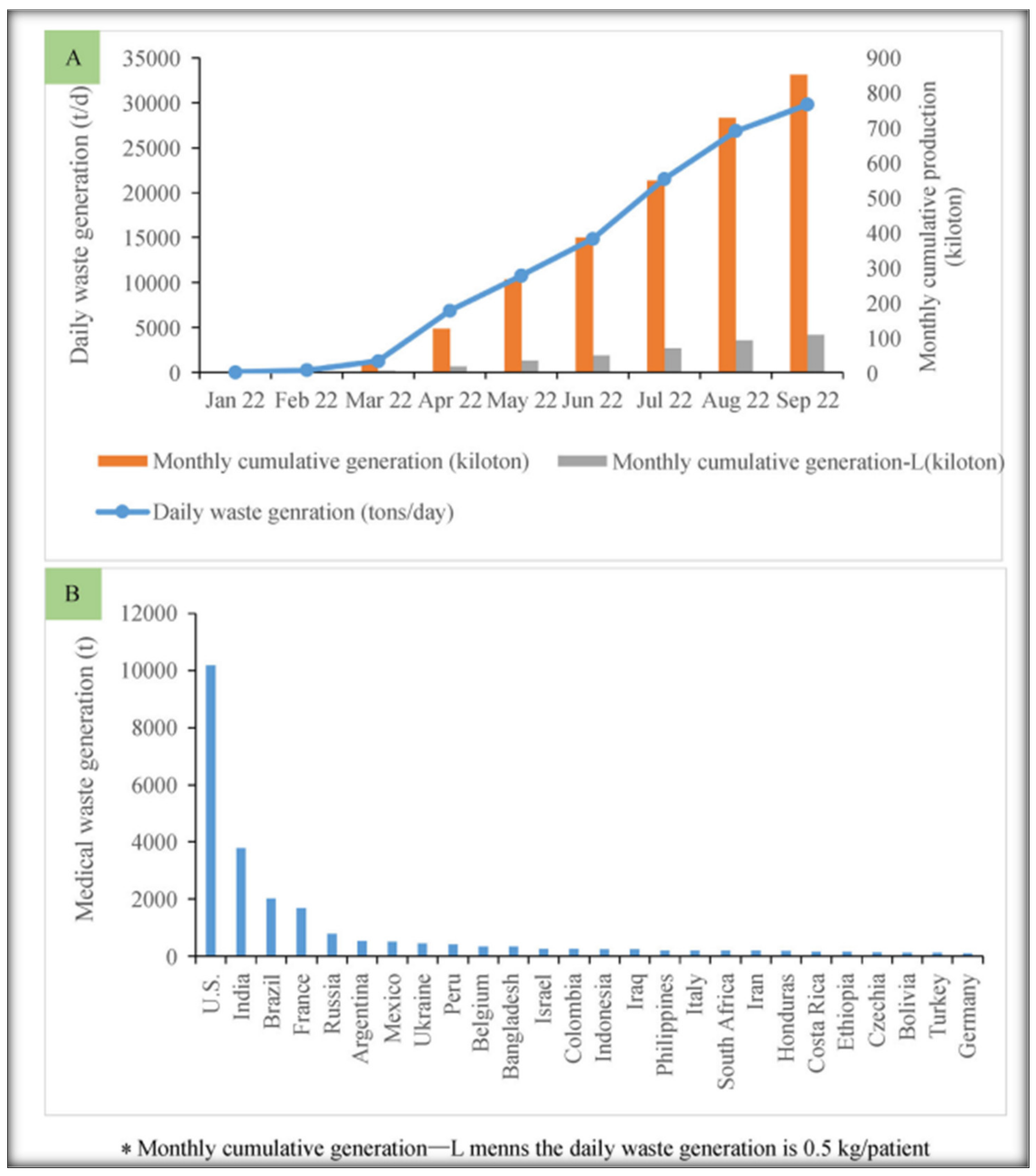
2.3. Medical Waste Generation during COVID-19
2.4. Recycling of Plastic Wastes
2.5. Landfilling Process
2.6. Medical Waste Management
3. Challenges in COVID-19 Waste Management
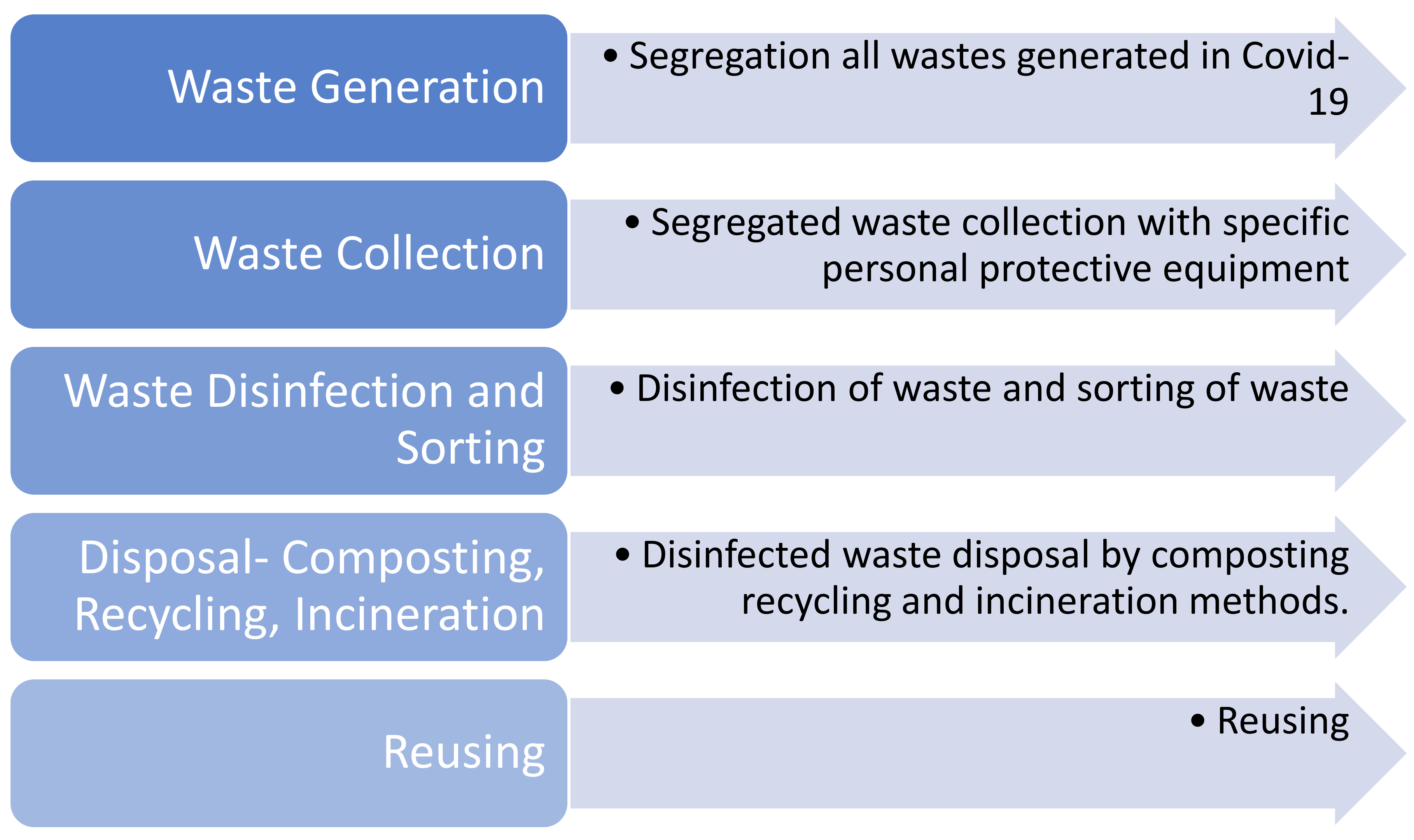
4. Methods for Segregation and Pre-Treatment of COVID-19 Medical Waste
5. Worldwide Scenario of Medical Waste Management and Treatment Systems during COVID-19 Pandemic
5.1. International Guidelines
5.2. Policies and Practices for Medical Waste Management
5.2.1. Republic of China
5.2.2. South Korea
5.2.3. India
5.2.4. Iran
5.2.5. Romania
Municipal Solid Wastes Management Modifications
Management of PPE Wastes
Collection and Recycling of MSW
6. Potential Plastic Waste Scenario
7. Health Safety of Waste Management Staff
- The provision of PPE and disinfectants to workers and associated staff;
- The fulfilment of hygiene protocols for waste management workers such as regular changing and washing of PPE, the provision of clothing during exposure, hand gloves, and the repeated sanitization of vehicle cabins, clothes, storage and collection facilities;
- Shield workers from potential exposure and provide training for adherence to the essential protocols to avoid the transmission of COVID-19 among workers and related staff;
- The required physical distancing among staff members, implement a reduction in the number of workers at a particular work point and special care should be taken of senior staff and workers with chronic illness.
8. Discussion and Potential Suggestions
- ▪
- A larger quantity of hazardous medical and other waste generation and its systematic management alongside the health and safety crises associated with the handling, collection, transportation, and final methodical disposal of such wastes from society to the individual;
- ▪
- The possible health hazards associated with frontline workers, health care workers, informal waste collectors, and the general public living in the vicinity of the waste disposal yards alongside the financial issues;
- ▪
- The unexpected surge in perilous waste and plastic safety gear and packaging will adversely influence the common recycling competence and other waste clearance processes which presents a key long-standing negative impact on the terrestrial and marine environment;
- ▪
- The new PPE contamination on land and in coastal areas has led to a novel situation for handling and dumping as well as probable issues for the health of the general public living in contact with such haphazardly disposed of items.
Author Contributions
Funding
Conflicts of Interest
References
- MacLean, O.A.; Orton, R.; Singer, J.B.; Robertson, D.L. Response to “On the origin and continuing evolution of SARS-CoV-2”. Natl. Sci. Rev. 2020, 7, 1012–1023. [Google Scholar] [CrossRef]
- Worldometers. Current World Population. Available online: www.worldometers.info (accessed on 1 September 2022).
- World Health Organization (WHO). Coronavirus (COVID-19). 2020. Available online: https://www.who.int/health-topics/coronavirus/coronavirus#tab=tab_1 (accessed on 1 September 2022).
- World Health Organization (WHO). Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19); WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Muhammad, S.; Long, X.; Salman, M. COVID-19 pandemic and environmental pollution: A blessing in disguise? Sci. Total Environ. 2020, 728, 138820. [Google Scholar] [CrossRef] [PubMed]
- AWWA. The Financial Impact of the COVID-19 Crisis, U.S.; HORIBA Ltd.: Kyoto, Japan, 2020. [Google Scholar]
- Fine, P.; Reichle, S.; Lord, K.M. Youth or Consequences: Put Youth at the Centre of COVID-19 Recovery. 2020. Available online: https://www.unhabitatyouth.org/2020/06/15/youth-covid19-response/ (accessed on 1 September 2022).
- Wuyts, W.; Maria, J.; Brusselaers, J.; Vrancken, K. Circular economy as a COVID-19 cure? Resour. Conserv. Recycl. 2020, 162, 105016. [Google Scholar] [CrossRef]
- Nzediegwu, C.; Chang, S.X. Improper solid waste management increases potential for COVID-19 spread in developing countries. Resour. Conserv. Recycl. 2020, 161, 104947. [Google Scholar] [CrossRef] [PubMed]
- Klemeš, J.J.; Fan, Y.V.; Tan, R.R.; Jiang, P. Minimising the present and future plastic waste, energy and environmental footprints related to COVID-19. Renew. Sustain. Energy Rev. 2020, 127, 109883. [Google Scholar] [CrossRef] [PubMed]
- Czig’any, T.; Ronkay, F. The coronavirus and plastics. eXPRESS Polym. Lett. 2020, 14, 510–511. [Google Scholar] [CrossRef]
- ADB. Managing Infectious Medical Waste during the COVID-19 Pandemic; Asian Development Bank (ADB): Manila, Philippines, 2020. [Google Scholar]
- Boucher, J.; Billard, G. Review of Plastic Footprint Methodologies, Portals. In The Challenges of Measuring Plastic Pollution—Field Actions Science Reports; IUCN: Gland, Switzerland, 2019; pp. 68–75. [Google Scholar]
- Rajmohan, K.V.S.; Ramya, C.; Viswanathan, M.R.; Varjani, S. Plastic pollutants: Effective waste management for pollution control and abatement. Curr. Opin. Environ. Sci. Health 2019, 12, 72–84. [Google Scholar] [CrossRef]
- Nghiem, L.D.; Morgon, B.; Donner, E.; Short, M.D. The COVID-19 pandemic: Considerations for the waste and wastewater services sector. Case Stud. Chem. Environ. Eng. 2020, 1, 100006. [Google Scholar] [CrossRef]
- Dente, S.M.R.; Hashimoto, S. COVID-19: A pandemic with positive and negative outcomes on resource and waste flows and stocks. Resour. Conserv. Recycl. 2020, 161, 104979. [Google Scholar] [CrossRef]
- Zahur, M. Solid Waste Management of Dhaka City: Public Private Community Partnership; BRAC University: Dhaka, Bangladesh, 2007; Volume 4, pp. 93–97. [Google Scholar]
- Mallapaty, S. How sewage could reveal the true scale of coronavirus outbreak. Nature 2020, 580, 176–177. [Google Scholar] [CrossRef]
- Lodder, W.; de Roda Husman, A.M. SARS-CoV-2 in wastewater: Potential health risk, but also data source. Lancet Gastroenterol. Hepatol. 2020, 5, 533–534. [Google Scholar] [CrossRef]
- MacKenzie, D. Covid-19 goes global. New Sci. 2020, 245, 7. [Google Scholar] [CrossRef]
- Butot, S.; Putallaz, T.; Croquet, C.; Lamothe, G.; Meyer, R.; Joosten, H.; Sánchez, G. Attachment of Enteric Viruses to Bottles. Appl. Environ. Microbiol. 2007, 73, 5104–5110. [Google Scholar] [CrossRef] [PubMed]
- Chin, A.W.H.; Chu, J.T.S.; Perera, M.R.A.; Hui, K.P.Y.; Yen, H.-L.; Chan, M.C.W.; Poon, L.L.M. Stability of SARS-CoV-2 in different environmental conditions. Lancet Microbe 2020, 1, e10. [Google Scholar] [CrossRef]
- Qu, G.; Li, X.; Hu, L.; Jiang, G. An imperative need for research on the role of environmental factors in the transmission of novel coronavirus (COVID-19). Environ. Sci. Technol. 2020, 54, 3730–3732. [Google Scholar] [CrossRef]
- Rafigh, P.; Akbari, A.A.; Bidhandi, H.M.; Kashan, A.H. Sustainable closed-loop supply chain network under uncertainty: A response to the COVID-19 pandemic. Environ. Sci. Pollut. Res. 2021, 1–17. [Google Scholar] [CrossRef]
- Fathollahi-Fard, A.M.; Ahmadi, A.; Karimi, B. Sustainable and Robust Home Healthcare Logistics: A Response to the COVID-19 Pandemic. Symmetry 2022, 14, 193. [Google Scholar] [CrossRef]
- Mojtahedi, M.; Fathollahi-Fard, A.M.; Tavakkoli-Moghaddam, R.; Newton, S. Sustainable Vehicle Routing Problem for Coordinated Solid Waste Management. J. Ind. Inf. Integr. 2021, 23, 100220. [Google Scholar] [CrossRef]
- Shahsavar, M.M.; Akrami, M.; Kian, Z.; Gheibi Behzadian Moghadam, K. Bio-recovery of municipal plastic waste management based on an integrated decision-making framework. J. Ind. Eng. Chem. 2022, 108, 215–234. [Google Scholar] [CrossRef]
- Van-Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and surface stability of SARSCoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Islam, S.M.D.; Bhuiyan, M.A.H. Impact scenarios of shrimp farming in coastal region of Bangladesh: An approach of an ecological model for sustainable management. Aquac. Int. 2016, 24, 1163–1190. [Google Scholar] [CrossRef]
- Singh, N.; Tang, Y.; Ogunseitan, O.A. Environmentally sustainable management of used personal protective equipment. Environ. Sci. Technol. 2020, 54, 8500–8502. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.; Angel, N.; Edson, J.; Bibby, K.; Bivins, A.; O’Brier, J.W.; Choi, P.M.; Kitajima, M.; Simpson, S.L.; Li, J.; et al. First confirmed detection of SARS-CoV-2 in untreated wastewater in Australia: A proof of concept for the wastewater surveillance of COVID-19 in the community. Sci. Total Environ. 2020, 728, 13876. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.H.; Islam, S.M.D. Degrading riverine ecology of Bangladesh and options for management. SUB J. Sustain. Environ. Develop. 2016, 1, 11–27. [Google Scholar]
- Zambrano-Monserrate, M.A.; Ruanob, M.A.; Sanchez-Alcalde, L. Indirect effects of COVID-19 on the environment. Sci. Total Environ. 2020, 728, 138813. [Google Scholar] [CrossRef]
- Fadare, O.O.; Okoffo, E.D. Covid-19 face masks: A potential source of microplastic fibers in the environment. Sci. Total Environ. 2020, 737, 140279. [Google Scholar] [CrossRef]
- Ma, Y.; Lin, X.; Wu, A.; Huang, Q.; Li, X.; Yan, J. Suggested guidelines for emergency treatment of medical waste during COVID-19: Chinese experience. Waste Dispos. Sustain. Energy 2020, 2, 81–84. [Google Scholar] [CrossRef]
- Saadat, S.; Rawtani, D.; Hussain, C.M. Environmental perspective of COVID-19. Sci. Total Environ. 2020, 728, 138870. [Google Scholar] [CrossRef]
- Somani, M.; Srivastava, A.N.; Gummadivalli, S.K.; Sharma, A. Indirect implications of COVID-19 towards sustainable environment: An investigation in Indian context. Bioresour. Technol. Rep. 2020, 11, 100491. [Google Scholar] [CrossRef]
- Rahman, M.M.; Bodrud-Doza, M.; Griffiths, M.D.; Mamun, M.A. Biomedical Waste amid COVID-19: Perspectives from Bangladesh. Lancet Glob. Health 2020, 8, e1262. [Google Scholar] [CrossRef]
- Mehta. The War on Plastics Runs into a Perfect Storm with Covid-19; Ethical Corporation: London, UK, 2020. [Google Scholar]
- Morawski, L.C. Reusable Packaging and COVID-19; Zero Waste Europe, Reloop Platform: Brussels, Belgium, 2020. [Google Scholar]
- Grodzinska-Jurczak, M.; Krawczyk, A.; Jurczak, A.; Strzelecka, M.; Bockowski, M.; Rechcinski, M. Environmental choices vs. COVID-19 pandemic fear—plastic governance re-assessment. Soc. Regist. 2020, 4, 49–66. [Google Scholar] [CrossRef]
- Ramteke, S.; Sahu, B.L. Novel coronavirus disease 2019 (COVID-19) pandemic: Considerations for the biomedical waste sector in India. Case Studies Chem. Environ. Eng. 2020, 2, 100029. [Google Scholar] [CrossRef]
- Kitchener, J. A New Type of Ocean Pollution: PPE; Reuters: London, UK, 2020. [Google Scholar]
- Hale, R.C.; Song, B. Single-use plastics and COVID-19: Scientific evidence and environmental regulations. Environ. Sci. Technol. 2020, 54, 7034–7036. [Google Scholar] [CrossRef] [PubMed]
- Godbole, T. Coronavirus Worsens Thailand’s Plastic Waste Crisis; Thailand Environment Institute Foundation: Nonthaburi, Thailand, 2020. [Google Scholar]
- Siwal, S.S.; Chaudhary, G.; Saini, A.K.; Kaur, H.; Saini, V.; Mokhta, S.K.; Thakur, V.K. Key ingredients and recycling strategy of personal protective equipment (PPE): Towards sustainable solution for the COVID-19 like pandemics. J. Environ. Chem. Eng. 2021, 9, 106284. [Google Scholar] [CrossRef]
- World Bank. Trends in Solid Waste Management. Available online: https://datatopics.worldbank.org/what-a-waste/trends_in_solid_waste_management.html (accessed on 1 September 2022).
- Sangkham, S. Face mask and medical waste disposal during the novel COVID-19 pandemic in Asia. Case Stud. Chem. Environ. Eng. 2020, 2, 100052. [Google Scholar] [CrossRef]
- De Sousa, F.D.B. Pros and Cons of Plastic during the COVID-19 Pandemic. Recycling 2020, 5, 27. [Google Scholar] [CrossRef]
- Parashar, N.; Hait, S. Plastics in the time of COVID-19 pandemic: Protector or polluter? Sci. Total Environ. 2021, 759, 144274. [Google Scholar] [CrossRef]
- Ayse, L.A.; Esther, A.-D.; Teresa, D.A.; Maria, B.; Miguel, C.A.; Charnett, C.; Kimberley, C.; Dragana, D.; Helen, H.; Paola, L.; et al. The Environmental Dangers of Employing Single-Use Face Masks as Part of a COVID-19 Exit Strategy; UCL Press: London, UK, 2020. [Google Scholar]
- Kumar, H.; Azad, A.; Gupta, A.; Sharma, J.; Bherwani, H.; Labhsetwar, N.K.; Kumar, R. COVID-19 Creating Another Problem? Sustainable Solution for PPE Disposal Through LCA Approach. Environ. Dev. Sustain. 2020, 23, 9418–9432. [Google Scholar] [CrossRef]
- Boyle, L. Bird Dies After Getting Tangled in Coronavirus Face Mask. Indep. New York. 2020. Available online: https://www.independent.co.uk/climate-change/news/coronavirus-face-mask-bird-death-recycle-environment-conservation-a9475341.html (accessed on 1 September 2022).
- Yang, Y.; Liu, W.; Zhang, Z.; Grossart, H.-P.; Gadd, G.M. Microplastics provide new microbial niches in aquatic environments. Appl. Microbiol. Biotechnol. 2020, 104, 6501–6511. [Google Scholar] [CrossRef]
- Rowan, N.J.; Laffey, J.G. Unlocking the surge in demand for personal and protective equipment (PPE) and improvised face coverings arising from coronavirus disease (COVID-19) pandemic—implications for efficacy, re-use and sustainable waste management. Sci. Total Environ. 2021, 752, 142259. [Google Scholar] [CrossRef]
- Sharma, H.B.; Vanapalli, K.R.; Cheelaa, V.R.; Ranjan, V.P.; Jaglan, A.K.; Dubey, B.; Goel, S.; Bhattacharya, J. Challenges, opportunities, and innovations for effective solid waste management during and post COVID-19 pandemic. Resour. Conserv. Recycl. 2020, 162, 105052. [Google Scholar] [CrossRef] [PubMed]
- Ilyas, S.; Srivastava, R.R.; Kim, H. Disinfection technology and strategies for COVID-19 hospital and bio-medical waste management. Sci. Total Environ. 2020, 749, 141652. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; AhujA, S.; MAdAn, M.; ASthAnA, A.K. Bio-medical waste management in a tertiary care hospital: An overview. J. Clin. Diagn. Res. 2016, 10, DC01. [Google Scholar] [PubMed]
- Anthru, S. Medical waste management in Covid 19 era. Int. Res. J. Eng. Tech. 2020, 7, 4597–4600. [Google Scholar]
- Hopman, J.; Allegranzi, B.; Mehtar, S. Managing COVID-19 in low- and middle-income countries. J. Am. Med. Assoc. 2020, 323, 1549–1550. [Google Scholar] [CrossRef] [PubMed]
- Jribi, S.; Ben, H.; Doggui, D.; Debbabi, H. COVID-19 virus outbreak lockdown: What impacts on household food wastage? Environ. Dev. Sustain. 2020, 22, 3939–3955. [Google Scholar] [CrossRef]
- Francis, R. Recycling of Polymers: Methods, Characterization and Applications; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Wang, J.; Shen, J.; Ye, D.; Yan, X.; Zhang, Y.; Yang, W.; Li, X.; Wang, J.; Zhang, L.; Pan, L. Disinfection technology of hospital wastes and wastewater: Suggestions for disinfection strategy during coronavirus disease 2019 (COVID-19) pandemic in China. Environ. Pollut. 2020, 262, 114665. [Google Scholar] [CrossRef]
- Vanapalli, K.R.; Sharma, H.B.; Ranjan, V.P.; Samal, B.; Bhattacharya, J.; Dubey, B.K.; Goel, S. Challenges and strategies for effective plastic waste management during and post COVID-19 pandemic. Sci. Total Environ. 2021, 750, 141514. [Google Scholar] [CrossRef]
- UNEP. Waste Management an Essential Public Service in the Fight to Beat COVID-19. In The United Nations Environment Programme (UNEP) and the Basel Convention; UNEP: Athens, Greece, 2020. [Google Scholar]
- Barcelo, D. An environmental and health perspective for COVID-19 outbreak: Meteorology and air quality influence, sewage epidemiology indicator, hospitals disinfection, drug therapies and recommendations. J. Environ. Chem. Eng. 2020, 8, 104006. [Google Scholar] [CrossRef]
- Bourouiba, L. Turbulent gas clouds and respiratory pathogen emissions potential implications for reducing transmission of COVID-19. J. Am. Med. Assoc. 2020, 323, 1837–1838. [Google Scholar]
- Singh, N.; Tang, Y.; Zhang, Z.; Zheng, C. COVID-19 waste management: Effective and successful measures in Wuhan, China. Resour. Conserv. Recycl. 2020, 163, 105071. [Google Scholar] [CrossRef] [PubMed]
- Ragazzi, M.; Rada, E.C.; Schiavon, M. Municipal solid waste management during the SARS-COV-2 outbreak and lockdownease: Lessons from Italy. Sci. Total Environ. 2020, 745, 141159. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Ecology and Environment of China (MEE). The Ministry of Ecology and Environment Issued Guide on Management and Technical on Emergency Treatment and Disposal of Medical Waste Caused by COVID-19; MEE: Beijing, China, 2020.
- National Health Commission of China (NHC). Notice on Environmental Management of Medical Waste Caused by COVID19; NHC: Beijing, China, 2020.
- Peng, J.; Wu, X.; Wang, R.; Li, C.; Zhang, Q.; Wei, D. Medical waste management practice during the 2019–2020 novel coronavirus pandemic: Experience in a general hospital. Am. J. Infect. Control 2020, 48, 918–921. [Google Scholar] [CrossRef] [PubMed]
- ESCAP. The Safe Waste Treatment for COVID-19, Lessons from the Republic of Korea: ESCAP-United Nation Economic and Social Commission for Asia and the Pacific; ESCAP: Bangkok, Thailand, 2020. [Google Scholar]
- Zand, A.D.; Heir, A.V. Emerging challenges in urban waste management in Tehran, Iran during the COVID-19 pandemic. Resour. Conserv. Recycl. 2020, 162, 105051. [Google Scholar] [CrossRef]
- Mihai, F.C. Assessment of COVID-19 waste flows during the emergency state in Romania and related public health and environmental concerns. Int. J. Environ. Res. Public Health 2020, 17, 5439. [Google Scholar] [CrossRef]
- Texas Commission on Environmental Quality (TCEQ). COVID19: Waste Disposal Guidance; TCEQ: Austin, TX, USA, 2020.
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef]
- Rhee, S.W. Management of used personal protective equipment and wastes related to COVID-19 in South Korea. Waste Manag. Res. 2020, 38, 820–824. [Google Scholar] [CrossRef]
- Patrício Silva, A.L.; Prata, J.C.; Walker, T.R.; Duarte, A.C.; Ouyang, W.; Barcelo, D.; Rocha-Santos, T. Increased plastic pollution due to COVID-19 pandemic: Challenges and recommendations. Chem. Eng. J. 2021, 405, 126683. [Google Scholar] [CrossRef]
- ISS. How to Dispose of Household Waste; ISS: Copenhagen, Denmark, 2020. [Google Scholar]
- Ikiz, E.; Maclaren, V.W.; Alfred, E.; Sivanesan, S. Impact of COVID19 on household waste flows, diversion and reuse: The case of multiresidential buildings in Toronto, Canada. Resour. Conserv. Recycl. 2021, 164, 105111. [Google Scholar] [CrossRef]
- Cook, T.M. Personal protective equipment during the coronavirus disease (COVID) 2019 pandemic—A narrative review. Anaesthesia 2020, 75, 920–927. [Google Scholar] [CrossRef]
- Huang, H.; Fan, C.; Li, M.; Nie, H.L.; Wang, F.B.; Wang, H.; Wang, R.; Xia, J.; Zheng, X.; Zuo, X.; et al. COVID-19: A call for physical scientists and engineers. ACS Nano 2020, 14, 3747–3754. [Google Scholar] [CrossRef] [PubMed]
- Kalina, M.; Tilley, E. ‘This is our next problem’: Cleaning up from the COVID-19 response. Waste Manag. 2020, 108, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Kojima, M.; Iwasaki, F.; Johannes, H.P.; Edita, E.P. Strengthening Waste Management Policies to Mitigate the COVID-19 Pandemic; No. 2020-05; Economic Research Institute for ASEAN and East Asia: Jakarta, Indonesia, 2020. [Google Scholar]
- Cesaro, A.; Pirozzi, F. About the effects of Covid-19 on solid waste management. TeMA-J. Land Use Mobil. Environ. 2020, 59–66. [Google Scholar] [CrossRef]
- Prata, J.C.; Silva, A.L.; Walker, T.R.; Duarte, A.C.; Rocha-Santos, T. COVID-19 pandemic repercussions on the use and management of plastics. Environ. Sci. Technol. 2020, 54, 7760–7765. [Google Scholar] [CrossRef]
- Silva, A.L.P.; Prata, J.C.; Walker, T.R.; Campos, D.; Duarte, A.C.; Soares, A.M.; Barcelò, D.; Rocha-Santos, T. Rethinking and optimising plastic waste management under COVID-19 pandemic: Policy solutions based on redesign and reduction of single-use plastics and personal protective equipment. Sci. Total Environ. 2020, 742, 140565. [Google Scholar] [CrossRef]
- Chaturvedi, I. COVID-19 and India: The Challenges of Marine Debris; National Maritime Foundation: New Delhi, India, 2020. [Google Scholar]
- European Commission. Waste Management in the Context of the Coronavirus Crisis; The European Commission: Brussels, Belgium, 2020. [Google Scholar]
- Masaki, E. Appraisal Environmental and Social Review Summary (ESRS)—Lao PDR COVID-19 Response Project—P173817; The World Bank Group: Washington, DC, USA, 2020. [Google Scholar]
- Benson, N.U.; Bassey, D.E.; Palanisami, T. COVID pollution: Impact of COVID-19 pandemic on global plastic waste footprint. Heliyon 2021, 7, e06343. [Google Scholar] [CrossRef]
- Mondal, S. Environmental Catastrophe amidst COVID-19 Pandemic: Disposal and Management of PPE Kits for the Production of Biofuel with the Sustainable Approach in Solar Thermal Energy. Mater. Today Proc. 2022, 64, 1266–1271. [Google Scholar] [CrossRef]
- Almulhim, A.I.; Ahmad, I.; Sarkar, S.; Chavali, M. Consequences of COVID-19 pandemic on solid waste management: Scenarios pertaining to developing countries. Remediat. J. 2021, 31, 111–121. [Google Scholar] [CrossRef]
- Das, A.K.; Islam, M.N.; Billah, M.M.; Sarker, A. COVID-19 pandemic and healthcare solid waste management strategy—A mini-review. Sci. Total Environ. 2021, 778, 146220. [Google Scholar] [CrossRef]
- Yousefi, M.; Oskoei, V.; Jonidi Jafari, A.; Farzadkia, M.; Hasham Firooz, M.; Abdollahinejad, B.; Torkashvand, J. Municipal solid waste management during COVID-19 pandemic: Effects and repercussions. Environ. Sci. Pollut. Res. 2021, 28, 32200–32209. [Google Scholar] [CrossRef]
- Singh, E.; Kumar, A.; Mishra, R.; Kumar, S. Solid waste management during COVID-19 pandemic: Recovery techniques and responses. Chemosphere 2022, 288, 132451. [Google Scholar] [CrossRef] [PubMed]
- Capoor, M.R.; Parida, A. Current perspectives of biomedical waste management in context of COVID-19. Indian J. Med. Microbiol. 2021, 39, 171–178. [Google Scholar] [CrossRef]
- Liang, Y.; Song, Q.; Wu, N.; Li, J.; Zhong, Y.; Zeng, W. Repercussions of COVID-19 pandemic on solid waste generation and management strategies. Front. Environ. Sci. Eng. 2021, 15, 115. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus Disease (COVID-19): Situation Report—177; World Health Organization (WHO): Geneva, Switzerland, 2020. [Google Scholar]
- Hughes, K. Protector or Polluter? The Impact of COVID-19 on the Movement to End Plastic Waste; World Economic Forum: Geneva, Switzerland, 2020. [Google Scholar]
- Tillett, R.L.; Sevinsky, J.R.; Hartley, P.D.; Kerwin, H.; Crawford, N.; Gorzalski, A.; Laverdure, C.; Verma, S.C.; Rossetto, C.C.; Jackson, D.; et al. Genomic evidence for reinfection with SARS-CoV-2: A case study. Lancet Infect. Dis. 2020, 21, 52–58. [Google Scholar] [CrossRef]
- Geyer, R.; Jambeck, J.R.; Law, K.L. Production, use, and fate of all plastics ever made. Sci. Adv. 2017, 3, e1700782. [Google Scholar] [CrossRef] [PubMed]
- Moosavi, J.; Fathollahi-Fard, A.M.; Dulebenets, M.A. Supply chain disruption during the COVID-19 pandemic: Recognizing potential disruption management strategies. Int. J. Disaster Risk Reduct. 2022, 1, 102983. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Projected Waste Generation (Millions of Tons/Year) | ||
|---|---|---|---|
| 2016 | 2030 | 2050 | |
| East Asia and Pacific | 468 | 602 | 714 |
| Europe and Central Asia | 392 | 440 | 490 |
| Latin America and Caribbean | 231 | 290 | 369 |
| Middle East and North Africa | 129 | 177 | 255 |
| North America | 289 | 342 | 396 |
| South Asia | 334 | 466 | 661 |
| Sub-Saharan Africa | 174 | 269 | 516 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luhar, I.; Luhar, S.; Abdullah, M.M.A.B. Challenges and Impacts of COVID-19 Pandemic on Global Waste Management Systems: A Review. J. Compos. Sci. 2022, 6, 271. https://doi.org/10.3390/jcs6090271
Luhar I, Luhar S, Abdullah MMAB. Challenges and Impacts of COVID-19 Pandemic on Global Waste Management Systems: A Review. Journal of Composites Science. 2022; 6(9):271. https://doi.org/10.3390/jcs6090271
Chicago/Turabian StyleLuhar, Ismail, Salmabanu Luhar, and Mohd Mustafa Al Bakri Abdullah. 2022. "Challenges and Impacts of COVID-19 Pandemic on Global Waste Management Systems: A Review" Journal of Composites Science 6, no. 9: 271. https://doi.org/10.3390/jcs6090271
APA StyleLuhar, I., Luhar, S., & Abdullah, M. M. A. B. (2022). Challenges and Impacts of COVID-19 Pandemic on Global Waste Management Systems: A Review. Journal of Composites Science, 6(9), 271. https://doi.org/10.3390/jcs6090271