
Nasal Septal Deviation Classifications Associated with Revision Septoplasty

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographics
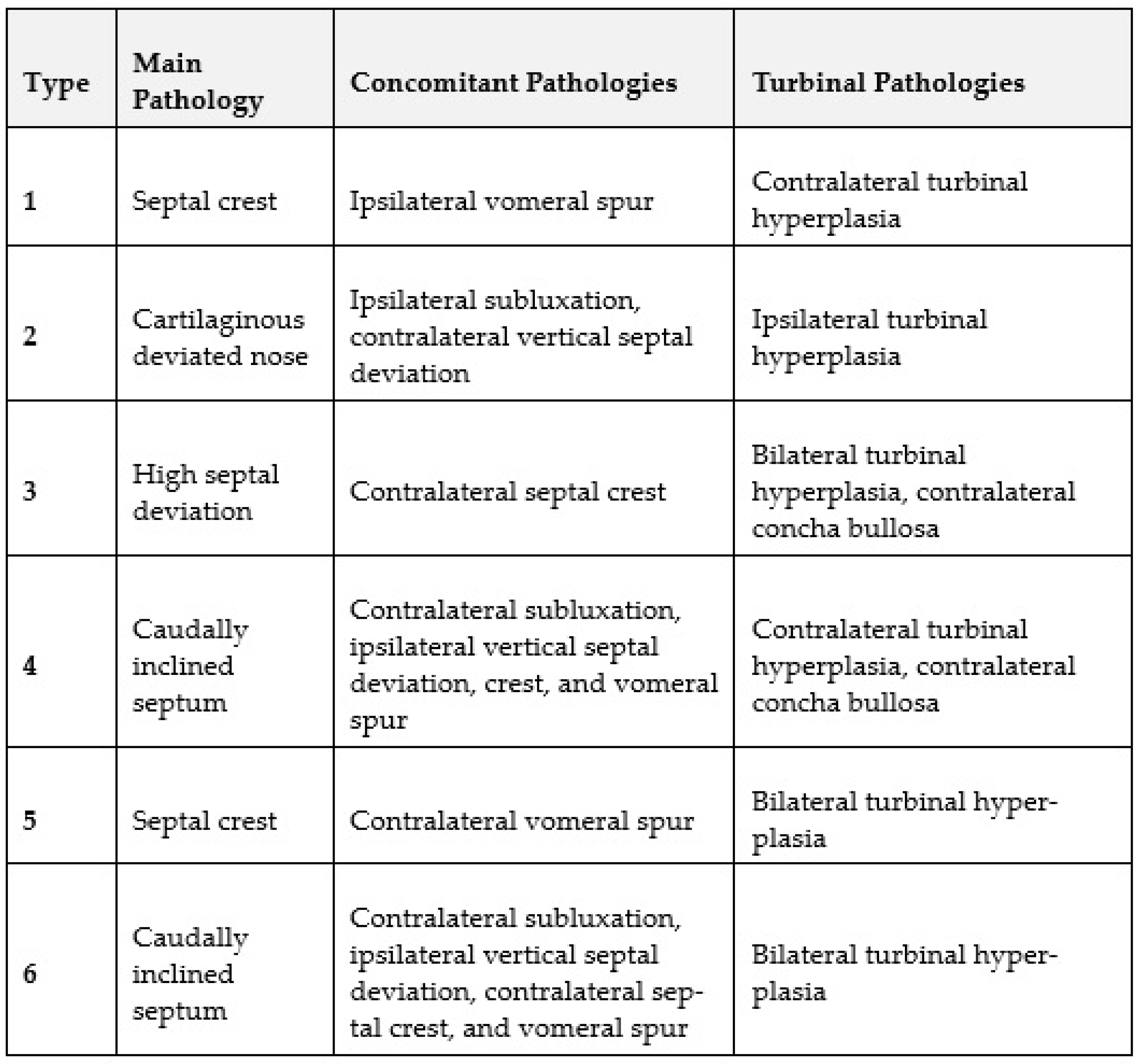
3.2. Rates of Baumann Types of Septal Deviations
3.3. Rates of Individual Septal Pathologies
3.4. Differences between Primary and Revision Surgery
3.5. Similarities between Primary and Revision Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- van Egmond, M.M.H.T.; Rovers, M.M.; Tillema, A.H.J.; van Neerbeek, N. Septoplasty for nasal obstruction due to a deviated nasal septum in adults: A systematic review. Rhinology 2018, 56, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Manoukian, P.D.; Wyatt, J.R.; Leopold, D.A.; Bass, E.B. Recent Trends in Utilization of Procedures in Otolaryngology-Head and Neck Surgery. Laryngoscope 1997, 107, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Youn, G.M.; Shah, J.P.; Wei, E.X.; Kandathil, C.; Most, S.P. Revision Rates of Septoplasty in the United States. Facial Plast. Surg. Aesthetic Med. 2023, 25, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, T.R.; Shakeel, M.; Al-Adhami, A.; Suhailee, S.; Ram, B.; Ah-See, K.W. Revision nasal surgery after septoplasty: Trainees versus trainers. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 3063–3067. [Google Scholar] [CrossRef] [PubMed]
- Gillman, G.S.; Egloff, A.M.; Rivera-Serrano, C.M. Revision septoplasty: A prospective disease-specific outcome study. Laryngoscope 2014, 124, 1290–1295. [Google Scholar] [CrossRef] [PubMed]
- van Egmond, M.M.H.T.; Rovers, M.M.; Hannink, G.; Hendriks, C.T.M.; van Heerbeek, N. Septoplasty with or without concurrent turbinate surgery versus non-surgical management for nasal obstruction in adults with a deviated septum: A pragmatic, randomised controlled trial. Lancet 2019, 394, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Erdivanli, O.C.; Coskun, Z.O.; Ozgur, A.; Ogurlu, M.; Demirci, M.; Dursun, E. Comparison of Quality of Life Before and After Septoplasty With Short Form-36. J. Craniofac. Surg. 2020, 31, 832–835. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, J.; Certal, V.; Chang, E.T.; Camacho, M. Nasal Septal Deviations: A Systematic Review of Classification Systems. Plast. Surg. Int. 2016, 2016, 7089123. [Google Scholar] [CrossRef] [PubMed]
- Lawson, V.G. Management of the twisted nose. J. Otolaryngol. 1978, 7, 56–66. [Google Scholar] [PubMed]
- Mladina, R.; Cujić, E.; Subarić, M.; Vuković, K. Nasal septal deformities in ear, nose, and throat patients: An international study. Am. J. Otolaryngol. 2008, 29, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Baumann, I.; Baumann, H. A new classification of septal deviations. Rhinology 2007, 45, 220–223 PMID: 17956023. [Google Scholar] [PubMed]
- Jin, H.R.; Kim, D.W.; Jung, H.J. Common Sites, Etiology, and Solutions of Persistent Septal Deviation in Revision Septoplasty. Clin. Exp. Otorhinolaryngol. 2018, 11, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Most, S.P.; Rudy, S.F. Septoplasty: Basic and Advanced Techniques. Facial Plast. Surg. Clin. N. Am. 2017, 25, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Haack, J.; Papel, I.D. Caudal Septal Deviation. Otolaryngol. Clin. N. Am. 2009, 42, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.S.; Dobratz, E.J.; Stowell, N.; Barker, D.; Park, S.S. Revision septoplasty: Review of sources of persistent nasal obstruction. Am. J. Rhinol. 2008, 22, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Schultz-Coulon, H.-J. Comments on septoplasty. HNO 2006, 54, 59–69, quiz 70. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowska-Bień, J.; Skarżyński, P.H.; Gwizdalska, I.; Łazęcka, K.; Skarżyński, H. Complications in septoplasty based on a large group of 5639 patients. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 1789–1794. [Google Scholar] [CrossRef] [PubMed]
- Ketcham, A.S.; Han, J.K. Complications and management of septoplasty. Otolaryngol. Clin. N. Am. 2010, 43, 897–904. [Google Scholar] [CrossRef] [PubMed]
- Şevik Eliçora, S.; Erdem, D.; Işık, H.; Damar, M.; Dinç, A.E. Difficult septal deviation cases: Open or closed technique? Braz. J. Otorhinolaryngol. 2017, 83, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Costache, A.; Berghi, O.N.; Cergan, R.; Dumitru, M.; Neagos, A.; Popa, L.G.; Giurcaneanu, C.; Vrinceanu, D. Respiratory allergies: Salicaceae sensitization (Review). Exp. Ther. Med. 2021, 21, 609. [Google Scholar] [CrossRef]

{kind=link}
| Demographics | All Cases (N = 652) | Primary Surgeries (N = 600) | Revisions (N = 52) | p-Value * |
|---|---|---|---|---|
| Age (years) | 34.6 ± 12.7 | 34.4 ± 12.7 | 36.5 ± 11.8 | 0.263 1 |
| Gender, female | 182 (27.9%) | 168 (28.0%) | 14 (26.9%) | 0.868 2 |
| Smoking, yes | 138 (21.2%) | 124 (20.7%) | 14 (26.9%) | 0.289 2 |
| Diabetes mellitus, yes | 4 (0.6%) | 4 (0.7%) | 0 (0.0%) | 1.000 3 |
| OSAS | 25 (3.8%) | 23 (3.8%) | 2 (3.8%) | 1.000 3 |
| Nose/face trauma, yes | 127 (19.5%) | 115 (19.2%) | 12 (23.1%) | 0.495 2 |
| Number of previous septoplasties | - | - | 1.1 ± 0.4 | - |
| Septal Pathologies. | All Cases (N = 652) | Primary Surgeries (N = 600) | Revisions (N = 52) | p-Value * |
|---|---|---|---|---|
| Baumann classification | ||||
| Type 1 | 381 (58.4%) | 362 (60.3%) | 19 (36.5%) | 0.001 1 |
| Type 2 | 54 (8.3%) | 45 (7.5%) | 9 (17.3%) | 0.030 2 |
| Type 3 | 73 (11.2%) | 60 (10.0%) | 13 (25.0%) | 0.001 1 |
| Type 4 | 58 (8.9%) | 50 (8.3%) | 8 (15.4%) | 0.121 2 |
| Type 5 | 66 (10.1%) | 63 (10.5%) | 3 (5.8%) | 0.278 1 |
| Type 6 | 20 (3.1%) | 20 (3.3%) | 0 (0.0%) | 0.394 2 |
| Subluxation | 88 (13.5%) | 77 (12.8%) | 11 (21.2%) | 0.092 1 |
| Oblique septum | 639 (98.0%) | 588 (98.0%) | 51 (98.1%) | 1.000 2 |
| Septal spur | 145 (22.2%) | 139 (23.2) | 6 (11.5%) | 0.053 2 |
| High septal deviation | 98 (15.0%) | 83 (13.8%) | 15 (28.8%) | 0.004 1 |
| Ipsilateral septal crest | 498 (76.4%) | 471 (78.5%) | 27 (51.9%) | <0.001 1 |
| Contralateral septal crest | 96 (14.7%) | 93 (15.5%) | 3 (5.8%) | 0.057 1 |
| Ipsilateral concha bullosa | 37 (5.7%) | 33 (5.5%) | 4 (7.7%) | 0.526 2 |
| Contralateral concha bullosa | 57 (8.7%) | 51 (8.5%) | 6 (11.5%) | 0.442 2 |
| Vomeral spur | 260 (39.9%) | 247 (41.2%) | 13 (25.0%) | 0.022 1 |
| Septal perforation | 15 (2.3%) | 10 (1.7%) | 5 (9.6%) | 0.004 2 |
| Ipsilateral turbinal hyperplasia | 238 (36.5%) | 221 (36.8%) | 17 (32.7%) | 0.552 1 |
| Contralateral turbinal hyperplasia | 277 (42.5%) | 258 (43.1%) | 19 (36.5%) | 0.361 1 |
| Bilateral turbinal hyperplasia | 196 (30.1%) | 183 (30.5%) | 13 (25.0%) | 0.407 1 |
| Absent turbinal hyperplasia | 319 (48.9%) | 292 (48.7%) | 27 (51.9%) | 0.652 1 |
| Nasal alar collapse | 10 (1.5%) | 8 (1.3%) | 2 (0.3%) | 0.186 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayer, K.; Brady-Praun, J.; Besser, G.; Brkic, F.F.; Haas, M.; Mueller, C.A.; Liu, D.T. Nasal Septal Deviation Classifications Associated with Revision Septoplasty. J. Otorhinolaryngol. Hear. Balance Med. 2024, 5, 14. https://doi.org/10.3390/ohbm5020014
Bayer K, Brady-Praun J, Besser G, Brkic FF, Haas M, Mueller CA, Liu DT. Nasal Septal Deviation Classifications Associated with Revision Septoplasty. Journal of Otorhinolaryngology, Hearing and Balance Medicine. 2024; 5(2):14. https://doi.org/10.3390/ohbm5020014
Chicago/Turabian StyleBayer, Karina, Johannes Brady-Praun, Gerold Besser, Faris F. Brkic, Markus Haas, Christian A. Mueller, and David T. Liu. 2024. "Nasal Septal Deviation Classifications Associated with Revision Septoplasty" Journal of Otorhinolaryngology, Hearing and Balance Medicine 5, no. 2: 14. https://doi.org/10.3390/ohbm5020014
APA StyleBayer, K., Brady-Praun, J., Besser, G., Brkic, F. F., Haas, M., Mueller, C. A., & Liu, D. T. (2024). Nasal Septal Deviation Classifications Associated with Revision Septoplasty. Journal of Otorhinolaryngology, Hearing and Balance Medicine, 5(2), 14. https://doi.org/10.3390/ohbm5020014