1. Introduction
Audiology is a health discipline that investigates hearing, balance, and related diseases. It is dedicated to the care of impaired people of all ages and backgrounds. According to Katz, audiology is concerned with the intersection of science and art [
1]. Aside from the objective evaluation of tasks, audiology provides emotional and social support to people impacted. An audiologist is a professional that specializes in identifying, evaluating, and treating people with hearing loss. The hearing care professional is also involved in a multidisciplinary team of speech therapists, ear, nose and throat specialists, deaf instructors, engineers, pediatricians, psychologists, and occupational therapists.
A career in audiology is related to academic expectations, similar to the expansion of the audiology field. First, most audiologists hold a Bachelor’s degree before pursuing a Master’s or Ph.D. Universiti Kebangsaan Malaysia, Universiti Islam Antarabangsa Malaysia, and Universiti Sains Malaysia are the only three universities that provide undergraduate audiology programs in Malaysia [
2]. A clinical audiologist in a private hospital or clinic and a dispensing audiologist in various hearing aid centers are possible job options for audiology graduates. Despite the increase in audiology graduates, audiology services require more attention in special education than other sectors such as clinical or private hearing aid centers [
3]. Moreover, the significant number of special education students can lead to inadequate audiological care.
Since students must apply their knowledge when caring for patients, the connection between the lecturer’s room and the clinical scene is critical. It covered clinical teaching foundations, effective clinical teaching tactics, adjusting clinical teaching techniques to individual situations, and clinical evaluation for audiology students. Aside from continuous clinical assessments, audiology students must complete all clinical hours and pass the audiological clinical examination to demonstrate clinical proficiency. For example, the Malaysian Qualifications Agency stated that a Bachelor’s degree in audiology required 350 clinical hours with at least 200 direct student–patient contacts [
4]. Meanwhile, final year students are evaluated on their clinical competency in dealing with new or follow-up patients in pediatrics and adults.
Following the expansion of ICT and the global COVID-19 pandemic, clinical training in higher education has lately changed to conform to new normal and standard operating procedures (SOP). As a result, telemedicine and telehealth approaches are becoming increasingly popular in clinical teaching [
5,
6,
7]. Telehealth as a clinical teaching approach at universities has many benefits. Novak can also be used for professional collaboration, as the students learned excellent communication skills and expanded their expertise in diverse teams through this project [
8].
The word teleaudiology has been widely used in research papers and publications to describe audiological services delivered via telehealth. Teleaudiology uses ICT to provide audiological services and information to clients [
9], and it is classified into screening, diagnostic, and intervention services [
10]. American Speech-Language-Hearing Association (ASHA) identified three teleaudiology service delivery methods: synchronous, asynchronous, and hybrid [
11]. The synchronous method entails an audiologist and a client communicating through video or audio. Asynchronous refers to sending images or data to an audiologist for interpretation. A hybrid is a mix of these two approaches. These approaches are implemented directly with clients or with facilitator support.
Teleaudiology was incorporated into clinical instruction for undergraduate audiology students at the Universiti Sains Malaysia (USM) Health Campus in 2021. First, we provide online clinical knowledge and theories for lectures, clinical case studies, and problem-based learning. During the COVID-19 epidemic, clinical students did not attend clinical practice as anticipated at the start of the semester due to a rigorous movement restriction order (MCO) and decreased patient numbers at USM Audiology Clinic, notably for small children and seniors. To guarantee that clinical students could apply their knowledge, they were required to perform pure tone audiometry using the Audsim Flex audiometer simulator (audstudent.com, Hollywood, FL, USA) on the clinic’s personal computer (PC). Alternatively, the students were taught how to use Chrome Remote Desktop Version 1.5 (Google, Mountain View, CA, USA) to control the audiology clinic PC from their hostel or house.
As previously stated, clinical evaluation is critical in measuring clinical student competence. For example, we administered an online Oriented Structured Clinical Exam (OSCE) to examine their knowledge and clinical abilities. We recently conducted face-to-face clinical audiology exams for our final year clinical student, modifying Krumm’s Teleaudiology Model [
12]. As such, the purpose of this study was to determine the feasibility of an adapted teleaudiology model for pediatric clinical assessment with the following specific objectives:
To design a trial version of the adapted teleaudiology approach for observation in clinical audiology examinations.
To measure Internet connectivity and make comparisons between two distinct types of connections and geographical areas.
To assess clinical audiologists’ satisfaction with the audio-visual quality of recorded sessions.
2. Materials and Methods
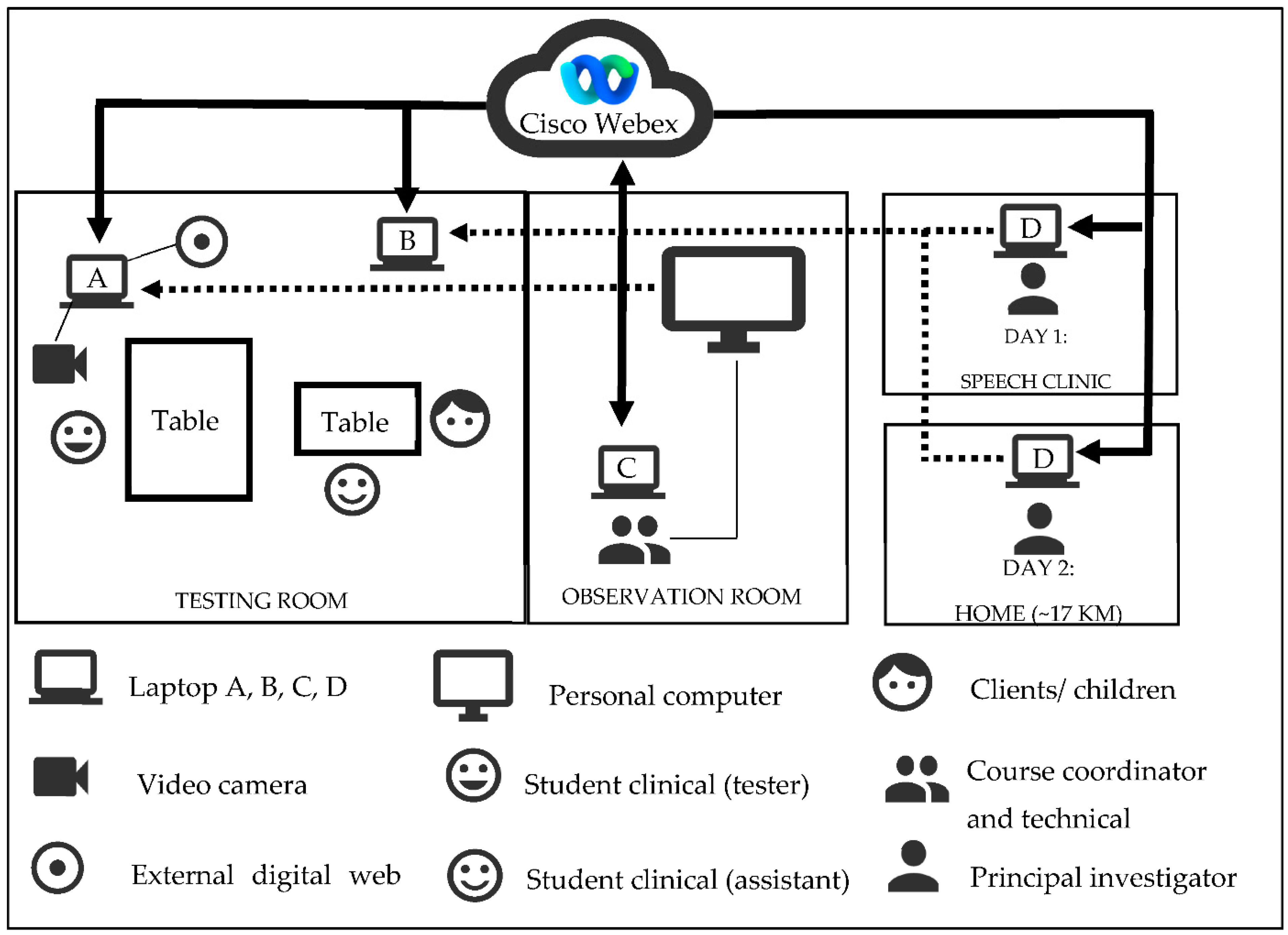
Efforts are currently being made to maximize the USM Audiological Clinic’s audiological resources, include teleaudiology in clinical education, and establish its practical feasibility. Instead, the teleaudiology model was modified to limit the testing room to one student and one patient. Moreover, each clinical step is visible to other lecturers and clinicians. We were able to link the audiological clinical examination to the principal investigator (PI), who was around 17 km away from the clinic. In total, four laptops and a personal computer running Windows 10 were employed in this study: the Acer Aspire A515-56 for Laptop A and B (Acer Inc., New Taipei City, Taiwan), the Asus ZenBook Flip UX360UAK for Laptop C (ASUSTek Computer Inc., Taipei, Taiwan), the Asus X450C Series for Laptop D (ASUSTek Computer Inc., Taipei, Taiwan), and the Lenovo c40 for PC (Lenovo Group Limited, Hong Kong, China).
2.1. Description of ICT Setup and Background of the Study
Equipment and ICT stability are crucial for long-term teleaudiology services feasibility, as this approach aims to deliver a reliable clinical service similar to face-to-face. This study optimized clinic facilities without upgrading ICT or audiology systems. The clinical coordinator’s Cisco Webex Meeting (
https://usm-cmr.webex.com (accessed on 25 July 2021), Ver. 41.7.7.9) was shared with participants of laptops A, B, and D. The student clinical (tester) has to log into Webex using laptop A using their USM email. Technical support utilized TeamViewer Version 15.19.5 (TeamViewer AG, Göppingen, Germany) to remotely control the Panasonic HC-V550 video camera (Panasonic Holdings Corporation, Osaka, Japan) and digital web camera from a PC in the observation room (free version, 64 bit). The technical support will change the camera input for Webex as asked by PI. We employed a video camera to record the candidates’ threshold searching on the audiometer (audiogram). An external digital web camera focused on the tympanometer, supporting the examiner in qualitative and quantitative tympanogram interpretation. Laptop A’s built-in camera also records candidates’ interactions with the child’s parents.
Additionally, laptop B is located in the testing room to monitor the child’s response during the audiological examinations. In general, hearing evaluations in pediatric cases may vary according to developmental age and may include distraction testing, visual reinforcement audiometry, and play audiometry. As a result, it is critical to monitor the child’s response during the audiological exams. Moreover, this laptop is connected via TeamViewer to laptop D (PI) to assist the investigator in determining the Internet connection. The clinical coordinator records all sessions and uploads them to the cloud for educational purposes and to accomplish the third objective of this project. Furthermore, as noted previously, the personal computer (observation room) was connected to laptop A (test room), allowing additional examiners or lecturers to observe all clinical procedures and outcomes as displayed on laptop A (mirror screen concept). As illustrated in
Figure A1, the PI was outside the USM Audiology Clinic, located within the USM Speech-Language Clinic (Day 1) and his home (Day 2).
2.2. Internet Connection and Measurements
As previously stated, we observed eight sessions of audiological tests using four laptops (A, B, C, and D) and a PC. Laptops A and C and the PC are essential for camera input, administrator access to the Webex application, and observation. As a result, these three laptops were connected to the Internet via a local area network (LAN) to ensure robust connectivity. Meanwhile, laptop B (testing room) and laptop D (day 1) were linked to USMSecure WiFi because of the room’s insufficient LAN port. On Day 2, the PI was at home and connected to the Internet via a mobile hotspot for this investigation. Unifi’s unlimited 2 h mobile hotspot service was subscribed to to ensure that each session’s Internet connection was uninterrupted.
Speedtest.net (Ookla, Seattle, WA, USA) and BlazeMeter (Perforce Software, Inc., Minneapolis, MN, USA) were used to measure Internet connectivity. The Internet connection speed of three laptops (A, B, and D) was measured regularly before, during, and after clinical assessment sessions. Ookla has maintained this website since 2006, reporting over 35 billion tests that meet the wide-angle contact measurement requirements [
13,
14]. It has three main features: it can upload, download, and ping. Second, Webex’s performance with four participants was rated using BlazeMeter. This open-source load testing tool for mobile apps, databases, online services, and websites [
15]. However, we did not restrict the license or scalability during the test. The test results were automatically sent to the PI after completion. Maximum users, average throughput, faults, and 50% response time were provided. The average bandwidth could not be tracked due to the testing credit restriction.
2.3. Live Observations and Satisfaction Level
During these two-day clinical tests, the principal investigator must observe all live sessions. It was also necessary to record all data acquired during the observation, including Internet speed, audio-visual quality, and comments on technical challenges. Because this is a trial version of the adapted teleaudiology approach, the PI serves as an external examiner located outside the clinic or in another state. For this study, the principal investigator did not evaluate the candidates’ performance throughout their clinical examinations. The course coordinator recorded every session and sent the URL to the PI. Because the recorded sessions contain private and confidential information, only experienced audiologists at USM were invited to evaluate the audio-visual quality. Quality and Impairment Scales of the International Telecommunication Union-R chose the grading structure (ITU, 2015). It was decided that the assessment process would be relevant to the recorded sessions. Each section covers a different aspect of the exam (
Appendix C): history taking (HT), otoscopic examination (OE), and tympanometry (tymp), as well as providing feedback (PF) and other relevant tests (OT). This process requires four experienced audiologists. During the assessments, the recorded sessions were shown on laptop B and a Panasonic television.
3. Results
All candidates for the audiological clinical examinations were familiar with the testing room’s facilities and audiological equipment, having spent nearly two years practicing in the USM Audiology Clinic. As illustrated in
Figure A1, we implemented only a few ICT facilities and incorporated comments from students, technologists, clinicians, and examiners to ensure that they do not interfere with or distract during clinical assessments. Technically, we optimized all existing infrastructure and had a few issues connecting laptop A to the exterior digital web camera due to a short cable. As a result, we were prompted to connect the camera via a three-meter USB extension wire, which resulted in signal loss. As a consequence, one of three web camera models was chosen following several trials. In general, the trial version of the adapted teleaudiology approach was successful in observing clinical examinations, and further details about the results are presented below.
3.1. Internet Connection
Ookla and BlazeMeter were used to test Internet speed for eight clinical sessions. However, in laptops B and D, the Internet speed cannot be determined during the ‘middle’ and ‘after’ sessions of Session 8 due to the PI’s laptop’s poor Internet connection. Because the data are significantly deviant from normal, all non-parametric tests were chosen to analyze ping, download, and upload Internet features. For this study, we compared the following: (i) the Internet speed properties of the same laptop, measured three times for each session; (ii) the Internet speed properties of different types of connectivity in different laptops, and (iii) the Internet speed properties of USMSecure Wireless (within USM) and unlimited Unifi Hotspot (at home) connections using laptop D.
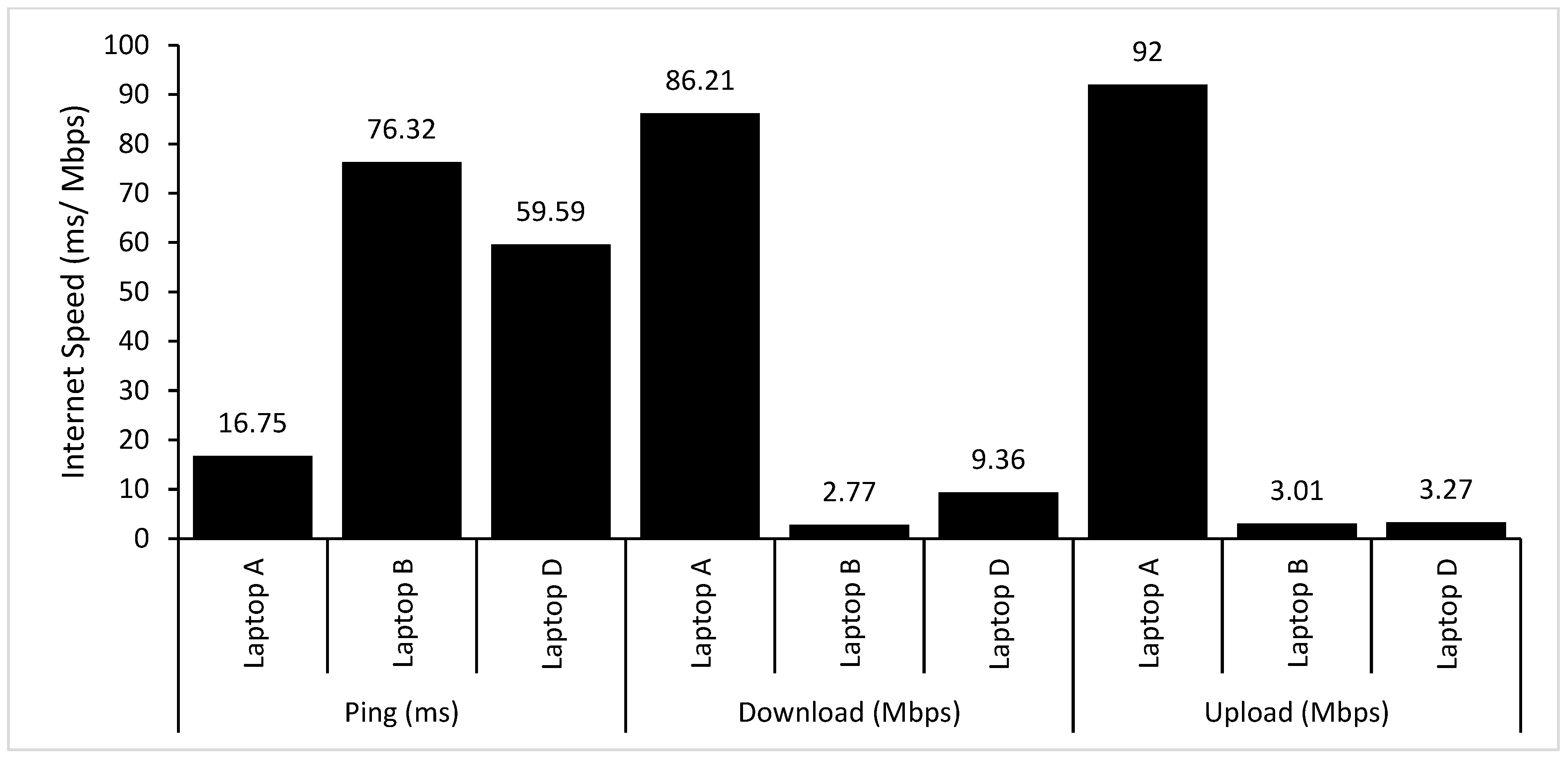
Friedman’s analysis revealed no statistically significant change in the ping (ms), download (Mbps), and upload (Mbps) values for each session, which were measured three times (before, middle, and after) (
p > 0.05). As a result, the repeated values for online properties were merged, and the mean values were calculated, as illustrated in
Figure A2. A Kruskal–Wallis H test revealed a statistically significant difference between the three laptops’ ping, download, and upload times (ms) (
Table A1). A post hoc analysis using Conover yielded a significance level of
p < 0.05. Between laptop B and laptop D, there were no significant differences in ping and upload speeds. However, statistically significant differences in download speeds were observed across laptops A, B, and C. Additionally, a Mann—Whitney test revealed no statistically significant difference between the USMSecure Wireless and the unrestricted Unifi Hotspot in all online properties.
Webex’s performance during audiology clinical examinations was evaluated using BlazeMeter. According to the test findings, the maximum number of virtual users that could be tested was 20, and the Webex load capabilities were kept to a minimum during the test period, as only four people participated. Overall, the average throughput, error rate, and response time were 16.50 hits per second, 99 percent, and 1215.88 ms, respectively. These values indicated that the Webex on the laptop D was operating at a deficient level of performance.
3.2. Live Observation Report
The live observation occurred in the USM Speech-Language Clinic on Day 1 and the PI’s home on Day 2. The PI reported on various points, and each observation criterion was divided into six segments (
Table A2). Seven clinical sessions used play audiometry to examine behavior, while one session applied visual reinforcement audiometry. These approaches were chosen following age-appropriate diagnostic audiology procedures, which required candidates to select differential diagnostic techniques that were developmentally suitable for the kid.
Due to the limits of the audiology equipment, the findings for otoscopic examination and distortion product otoacoustic emissions cannot be noticed during live observation. Overall, Session 8 had the most reported issues, at four, while Sessions 6 and 7 each had one. Additionally, the most frequently occurring recurring difficulties occurred only in two distinct sessions, and the most frequently occurring problems were noted in part for providing feedback (not related to the limitation of the equipment).
3.3. Level of Satisfaction among the Principal Investigator and Experienced Audiologists
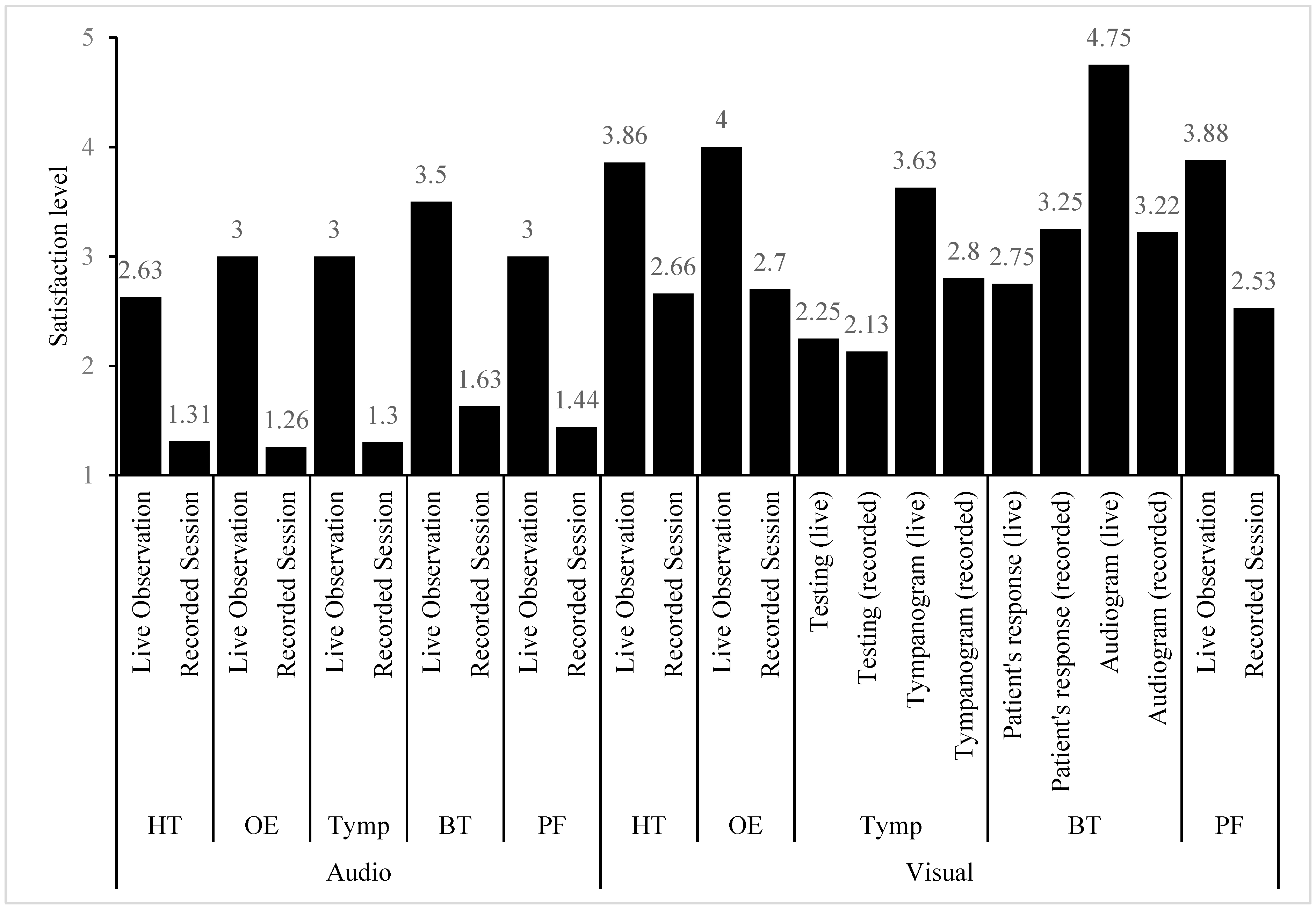
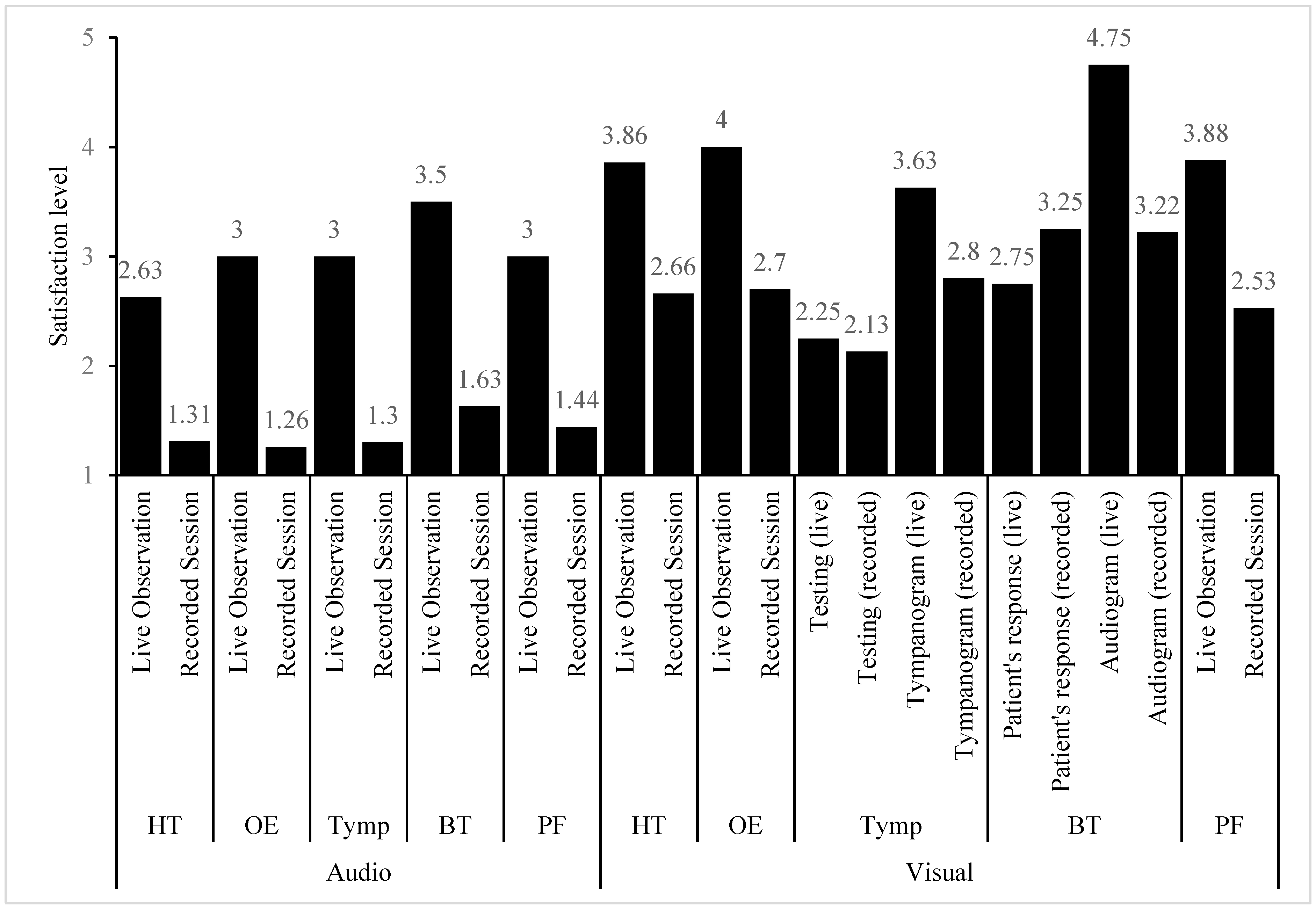
Live observation by the PI established the level of satisfaction, and four experienced audiologists analyzed the recorded Webex sessions. The assessors, two male and three female audiologists, had an average of 5.36–15.8 years of experience. Participants were required to rate the audio-visual quality in at least five segments during each session. Respondents were generally satisfied with the audio quality (M = 3.02, SD = 1.14), with behavioral testing scoring the highest (M = 3.50, SD = 0.76) and history taking scoring the lowest (M = 2.63, SD = 1.06) during the live observation. Similarly, the audio quality of behavioral testing in recorded sessions suggested the greatest degree of satisfaction (M = 1.63, SD = 0.66), but otoscopic examination indicated the lowest level of satisfaction (M = 1.26, SD = 0.44). Meanwhile, the highest degree of visual quality was reported for audiograms performed under live observation (M = 4.75, SD = 0.71), while the lowest level of satisfaction was reported for recorded tympanometry testing (M = 2.13, SD = 1.06). Additionally, we averaged all areas for each session to compare satisfaction levels across live and recorded sessions. For audio (U = 867.50,
p = 0.001) and visual (U = 4448.50,
p = 0.001), satisfaction with live observation was significantly higher than satisfaction with recorded sessions. Other testing results were removed since the task was not included in all clinical sessions.
Figure A3 summarizes the degree of satisfaction.
4. Discussion
The essential premise of a basic model of teleaudiology for adult clients was that the services should be comparable to those provided in conventional clinical settings and that they could be used in a variety of telecommunications studies utilizing synchronous, asynchronous, or hybrid technology [
14]. In this study, we adapted this model to create a trial version for use during audiology clinical evaluations. Thus, the principal investigator acted as an examiner in this study, evaluating the live audiology clinical examination via ICT applications from a distance. This approach may have a substantial impact, particularly during the COVID-19 pandemic, due to the restriction of interstate travel orders, particularly for an external examiner. As a result, it may minimize the cost of travel [
16,
17]. Additionally, live observation via Webex can be used for undergraduate or postgraduate audiology clinical practice by domestic or international students. This may be advantageous for students who remained at home or in a hostel during the epidemic COVID-19. Additionally, as demonstrated by a previous study, it can foster health professional teamwork, who successfully collaborated with nursing and audiology students to fit hearing aids using teleaudiology [
8].
In Malaysia, the first research concentrating on teleaudiology was conducted to ascertain audiologist attitudes about the field [
18] and conduct remote hearing assessments for deaf and hard-of-hearing school children [
3]. Because this approach is novel in Malaysia, we maximized the use of existing audiology equipment in the clinic, which was not PC-based. In this case, more ICT facilities are required for communication and recording of all audiological findings. For audio-visual communication, prior researchers have described the usage of Cisco Webex Meeting [
19,
20], and other studies have successfully adopted a nearly identical technique for cochlear implant users [
21,
22,
23]. However, several researchers used a variety of platforms in their investigations, including AudioProConnect (AudioProConnect Company, Bobigny, France) [
24], the Polycom System (Plantronics, Inc., 500 Series, CA, USA) [
21,
25], and Skype (Microsoft Corp., Luxembourg City, Luxembourg) [
26]. Second, this study employed TeamViewer to control the laptop in the testing room remotely, comparable to earlier teleaudiology research [
27,
28,
29]. Although this study’s general design blended prior studies, its primary objective was distinct and did not even include remote hearing assessment. As a result, it is unlikely that this design may be used in the future to accomplish a similar purpose as the prior study.
The summary of the live observation report (
Table A2) shows that most sessions encountered difficulties due to a lack of ICT resources and technical support staff. These two critical components should be highlighted in the teleaudiology approach planning checklist [
20,
30,
31,
32]. For instance, in our study, we allocated only existing staff members who are not ICT experts and must execute another duty during the clinical examination. As a result of the shortage of ICT technical support employees, specific technical issues occurred, such as camera selection input and monitoring Webex recording sessions. Additionally, because this study was conducted during a clinical assessment, all technological difficulties encountered inside the testing room were resolved remotely, as we did not intend to disrupt the sessions. In comparison, if we were to use the teleaudiology approach in daily clinical practice, any technical difficulties that arose could be resolved directly by technical support.
As a guideline to assure the proper functioning of this teleaudiology service, several researchers have established a minimum upload and download Internet connection speed of between 0.1 Mbps and 0.38 Mbps [
27,
28,
33,
34,
35]. In comparison to this study, the Internet speed was significantly faster. The download speed was recorded as being between 2.77 Mbps and 86.21 Mbps, while the upload speed was reported as being between 3.01 Mbps and 92 Mbps. Meanwhile, researchers observed ping values for Internet speed was 16.75 ms to 76.32 ms, which were found to be greater than those reported in a study conducted by Penteado, which ranged between 58.5 ms and 7.3 ms [
36]. However, no specific ping values have been established by prior studies in the teleaudiology approach.
Additionally, while the TeamViewer application utilized in this investigation was similar to those used in prior studies to operate the laptop at the testing site [
27,
28], the application’s performance is reliant on the Internet connection. According to their website, the minimal criteria for Internet speed are 6 Mbps for download and 1 Mbps for upload [
37]. Only laptop B exceeded the recommended download speed (
Figure A1). This finding is consistent with PI’s experience, during which TeamViewer regularly disconnected and one of the sessions encountered connectivity issues while using TeamViewer to test the Internet speed. Apart from that, PI observed a reduction in the audio-visual quality on laptop B after connecting to this application, which could be attributed to the volume of Internet traffic on laptop B, which was connected only via USMSecure WiFi. Additionally, we discovered that the wireless connection between USMSecure and Unifi Mobile was comparable in ping and upload speeds. This circumstance may have a beneficial influence on the use of mobile networks such as 3G cellular networks [
38] or 3G Vodafone mobile hotspots [
27] in areas with restricted Internet access, mainly rural areas.
Dharmar conducted a teleaudiology study for infant hearing assessment and discovered that audiologist satisfaction with live testing was 5.9 and 6.7, respectively, on a 7-point Likert scale [
38]. These findings indicated that satisfaction accounted for more than half of the entire score, which corresponds to this study’s findings for live observation, where the total satisfaction score for audio-visual was more significant than 2.5 on a 5-point Likert scale. However, the total score for the recorded sessions’ audio quality was less than half (M = 1.39, SD = 0.55). As we are aware, the sound quality is poor because we can only use the built-in microphone on laptop A or the video camera, which is fixed in that position. Additionally, the recorded sessions do not focus on the screen that was selected during the live observation but rather on the four primary screens of the Webex participants, which include the clinical coordinator (for recording purposes), the principal investigator (for live observation), clinical students (for testing purposes), and technical staff (patient’s response). As a result, this may affect the evaluations of the recorded sessions.
5. Conclusions and Recommendations for the Future
Students’ abilities are routinely examined in a variety of ways during pediatric clinical assessment. However, these factors can be classified into two broad categories: communication abilities and hands-on skills. The following objectives for implementing a comprehensive observation system for audiology clinical examinations are provided together with their associated challenges:
Challenges: Communication abilities are contingent upon the adequacy of ICT infrastructure and audio-visual quality. We employed an existing communication device in the clinic (
Figure A1) and fitted it to their position in this study. As a result, it may impair the audio-visual quality, mainly when working with pediatric patients who actively move throughout sessions. Meanwhile, clinical abilities are contingent on the ability to utilize audiology tools to examine the hearing status and be adaptable when dealing with patients. As previously stated, all audiology devices are not operated via a personal computer, necessitating an external camera (video camera or web camera) to watch all clinical stages while operating the machines. In general, these two concerns can be addressed by updating equipment to more portable, stable audio-visual, and PC-based devices capable of screen sharing and remote control.
Challenges: Due to the limitations of the existing Internet infrastructure, the testing room was equipped with only one LAN port for connection to laptop A (audiology device), while laptop B (patient reaction) was wirelessly connected. Thus, this may result in a significant difference in Internet speed between these two laptops with similar specifications and may affect the level of satisfaction with audio-visual quality. Additionally, using a Mobile Hotspot (Day2) may provide a more accurate forecast of the teleaudiology approach that can be used in areas with restricted Internet connectivity. However, network provider collaboration is critical to ensuring the stability of the Internet connection.
Challenges: We utilized all available employees throughout this clinical evaluation and assigned only one person to provide technological support, specifically for camera input choices. However, this staff member had a relationship with his regular employment, and as a result, the camera selection for specific clinical sessions was not as planned. Thus, the team should include skilled personnel dedicated solely to technological support, particularly during the teleaudiology session.
Overall, we were successful in implementing a trial version of an adapted teleaudiology approach that can be utilized to observe audiology clinical examinations and this strategy can also be used in the future for clinical observation, particularly during pandemic COVID-19, when the total number of students in the clinic had to be limited. Additionally, the observation can be used to expose nonclinical professionals or students who work with special needs children, such as teachers, policymakers, and parents. With specific changes and upgrades to the teleaudiology equipment, it is possible to conduct hearing tests from a distance using the same approach.


 ,
, 

{kind=link}
{kind=link}
{kind=link}