Chronic Ankle Instability Does Not Influence Tibiofemoral Contact Forces during Drop Landings †


Abstract
:1. Introduction
2. Method
2.1. Participants
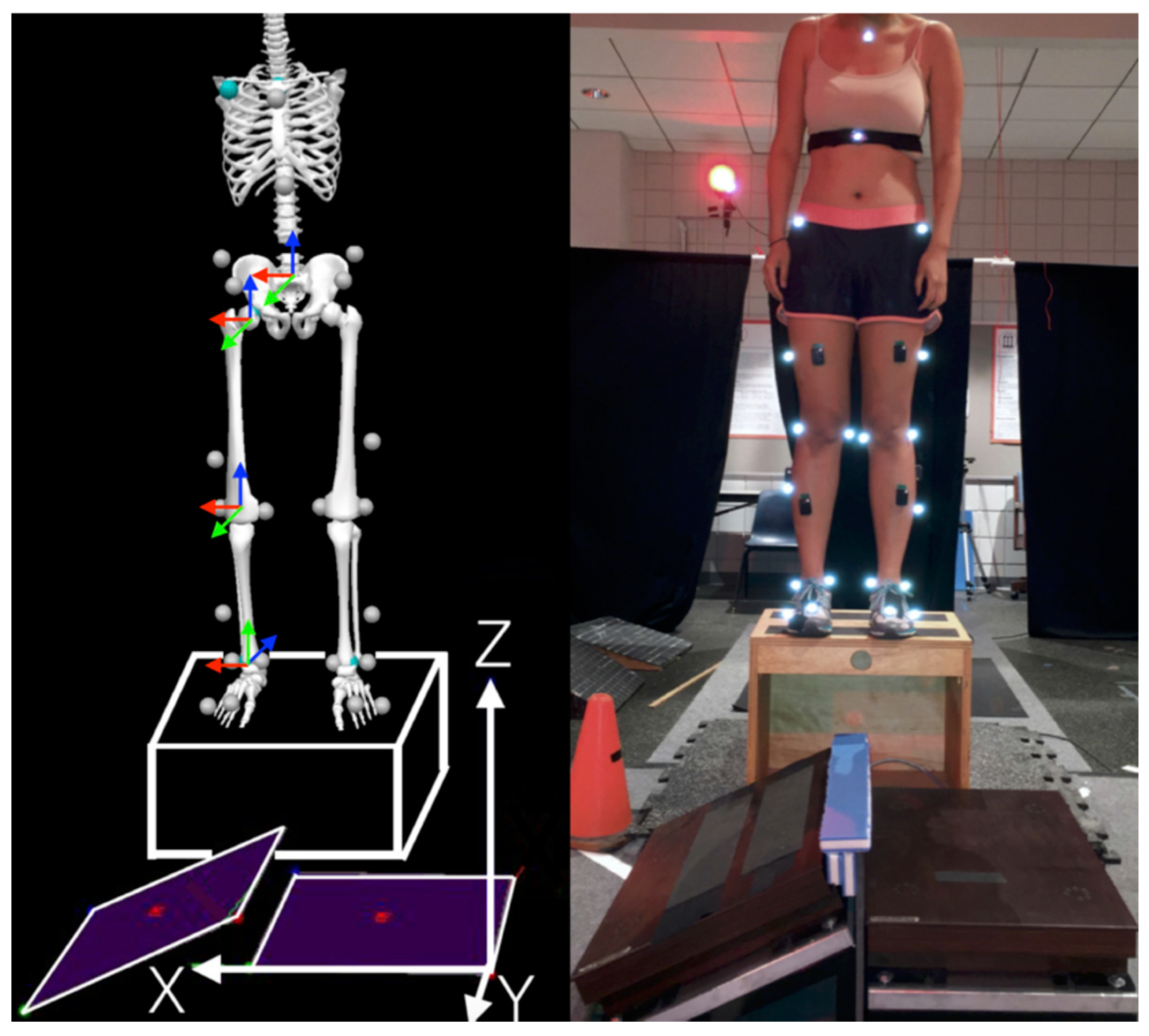
2.2. Test Protocol
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Kobayashi, T.; Gamada, K. Lateral ankle sprain and chronic ankle instability: A critical review. Foot Ankle Spec. 2014, 7, 298–326. [Google Scholar] [CrossRef] [PubMed]
- Söderman, K.; Alfredson, H.; Pietilä, T.; Werner, S. Risk factors for leg injuries in female soccer players: A prospective investigation during one out-door season. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Kramer, L.C.; Denegar, C.R.; Buckley, W.E.; Hertel, J. Factors associated with anterior cruciate ligament injury: History in female athletes. J. Sports Med. Phys. Fit. 2007, 47, 446–454. [Google Scholar]
- Terada, M.; Pietrosimone, B.; Gribble, P.A. Individuals with chronic ankle instability exhibit altered landing knee kinematics: Potential link with the mechanism of loading for the anterior cruciate ligament. Clin. Biomech. 2014, 29, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ko, J.; Walker, M.; Brown, C.; Schmidt, J.; Kim, S.H.; Simpson, K. Does chronic ankle instability influence knee biomechanics of females during inverted surface landings? Int. J. Sports Med. 2018, 39, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ko, J.; Walker, M.A.; Brown, C.N.; Schmidt, J.D.; Kim, S.H.; Simpson, K.J. Does chronic ankle instability influence lower extremity muscle activation of females during landing? J. Electromyogr. Kinesiol. 2018, 38, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.; Caulfield, B.; Docherty, C.L.; Fourchet, F.; Fong, D.; Hertel, J.; Hiller, C.; Kaminski, T.W.; et al. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the international ankle consortium. J. Orthop. Sports Phys. Ther. 2013, 43, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.S.; Chaudhari, A.M.; Andriacchi, T.P. The influence of deceleration forces on ACL strain during single-leg landing: A simulation study. J. Biomech. 2007, 40, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Garrett, W.E. Mechanisms of non-contact ACL injuries. Br. J. Sports Med. 2007, 41 (Suppl. 1), i47–i51. [Google Scholar] [CrossRef] [PubMed]
- Nunley, R.; Wright, D.; Renner, J.; Yu, B.; Garrett, W.E. Gender comparison of patellar tendon tibial shaft angle with weight bearing. Res. Sports Med. 2003, 11, 173–185. [Google Scholar] [CrossRef]
- Laughlin, W.A.; Weinhandl, J.T.; Kernozek, T.W.; Cobb, S.C.; Keenan, K.G.; O’Connor, K.M. The effects of single-leg landing technique on ACL loading. J. Biomech. 2011, 44, 1845–1851. [Google Scholar] [CrossRef] [PubMed]
- Kernozek, T.W.; Ragan, R.J. Estimation of anterior cruciate ligament tension from inverse dynamics data and electromyography in females during drop landing. Clin. Biomech. 2008, 23, 1279–1286. [Google Scholar] [CrossRef]
- Chen, Q.; Wortley, M.; Bhaskaran, D.; Milner, C.E.; Zhang, S. Is the inverted surface landing more suitable in evaluating ankle braces and ankle inversion perturbation? Clin. J. Sports Med. 2012, 22, 214–220. [Google Scholar] [CrossRef] [PubMed]
- D’Lima, D.D.; Fregly, B.J.; Patil, S.; Steklov, N.; Colwell, C.W., Jr. Knee joint forces: Prediction, measurement, and significance. Proc. Inst. Mech. Eng. Part H 2012, 226, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Boden, B.P.; Torg, J.S.; Knowles, S.B.; Hewett, T.E. Video analysis of anterior cruciate ligament injury: Abnormalities in hip and ankle kinematics. Am. J. Sports Med. 2009, 37, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Wall, S.J.; Rose, D.M.; Sutter, E.G.; Belkoff, S.M.; Boden, B.P. The role of axial compressive and quadriceps forces in noncontact anterior cruciate ligament injury: A cadaveric study. Am. J. Sports Med. 2012, 40, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Meyer, E.G.; Haut, R.C. Anterior cruciate ligament injury induced by internal tibial torsion or tibiofemoral compression. J. Biomech. 2008, 41, 3377–3383. [Google Scholar] [CrossRef] [PubMed]
- Weinhandl, J.T.; Earl-Boehm, J.E.; Ebersole, K.T.; Huddleston, W.E.; Armstrong, B.S.R.; O’Connor, K.M. Reduced hamstring strength increases anterior cruciate ligament loading during anticipated sidestep cutting. Clin. Biomech. 2014, 29, 752–759. [Google Scholar] [CrossRef]
- Cleather, D.J.; Goodwin, J.E.; Bull, A.M.J. Hip and knee joint loading during vertical jumping and push jerking. Clin. Biomech. 2013, 28, 98–103. [Google Scholar] [CrossRef]
- D’Lima, D.D.; Steklov, N.; Patil, S.; Colwell, C.W. The mark coventry award: In vivo knee forces during recreation and exercise after knee arthroplasty. Clin. Orthop. Relat. Res. 2008, 466, 2605–2611. [Google Scholar] [CrossRef]

{kind=link}
| Variable | CAI | Controls |
|---|---|---|
| Sample Size | 21 | 21 |
| Body mass (kg) | 64.4 ± 12.4 | 64.4 ± 11.9 |
| Height (cm) | 164 ± 6 | 165 ± 6 |
| Age (years) | 21 ± 2 | 21 ± 2 |
| CAIT score | 19.3 ± 6.0 | 29.5 ± 0.9 |
| IdFAI score | 22.2 ± 9.2 | 1.3 ± 2.1 |
| Variables (×BW) | CAI | CON | p Values | Cohen’s d |
|---|---|---|---|---|
| Posterior Force | 1.23 ± 0.51 | 1.04 ± 0.40 | 0.14 | 0.41 |
| Medial Force | 0.88 ± 0.19 | 0.93 ± 0.34 | 0.48 | 0.18 |
| Compressive Force | 10.23 ± 2.09 | 9.65 ± 1.39 | 0.28 | 0.33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Wang, H.; Simpson, K.J. Chronic Ankle Instability Does Not Influence Tibiofemoral Contact Forces during Drop Landings. Proceedings 2020, 49, 5. https://doi.org/10.3390/proceedings2020049005
Li Y, Wang H, Simpson KJ. Chronic Ankle Instability Does Not Influence Tibiofemoral Contact Forces during Drop Landings. Proceedings. 2020; 49(1):5. https://doi.org/10.3390/proceedings2020049005
Chicago/Turabian StyleLi, Yumeng, He Wang, and Kathy J. Simpson. 2020. "Chronic Ankle Instability Does Not Influence Tibiofemoral Contact Forces during Drop Landings" Proceedings 49, no. 1: 5. https://doi.org/10.3390/proceedings2020049005
APA StyleLi, Y., Wang, H., & Simpson, K. J. (2020). Chronic Ankle Instability Does Not Influence Tibiofemoral Contact Forces during Drop Landings. Proceedings, 49(1), 5. https://doi.org/10.3390/proceedings2020049005