Infrared Thermography for DIEP Flap Breast Reconstruction Part I: Measurements †


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methodology and Measurement Setup
3. Results & Discussion
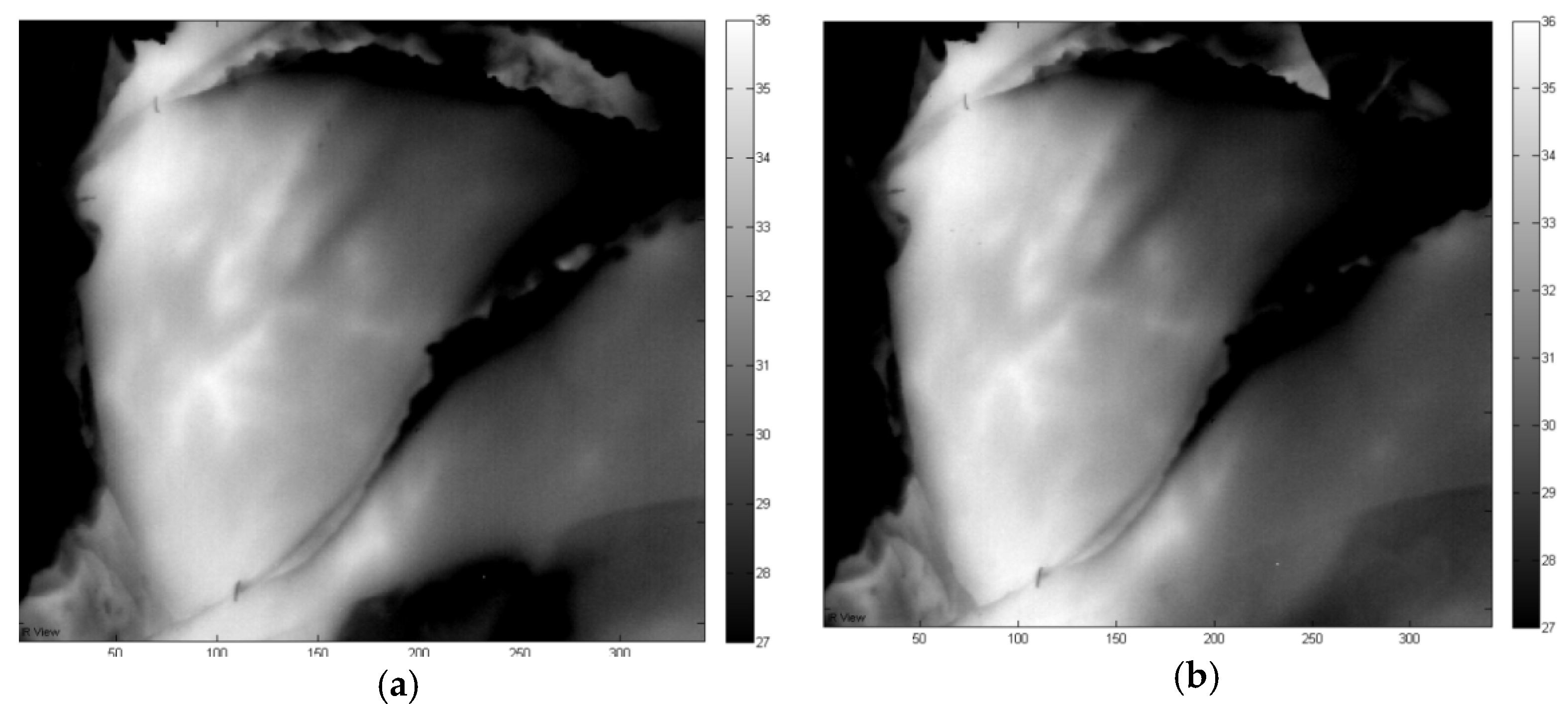
3.1. Left Flap in Rest 2 Perforators (A+B) Open
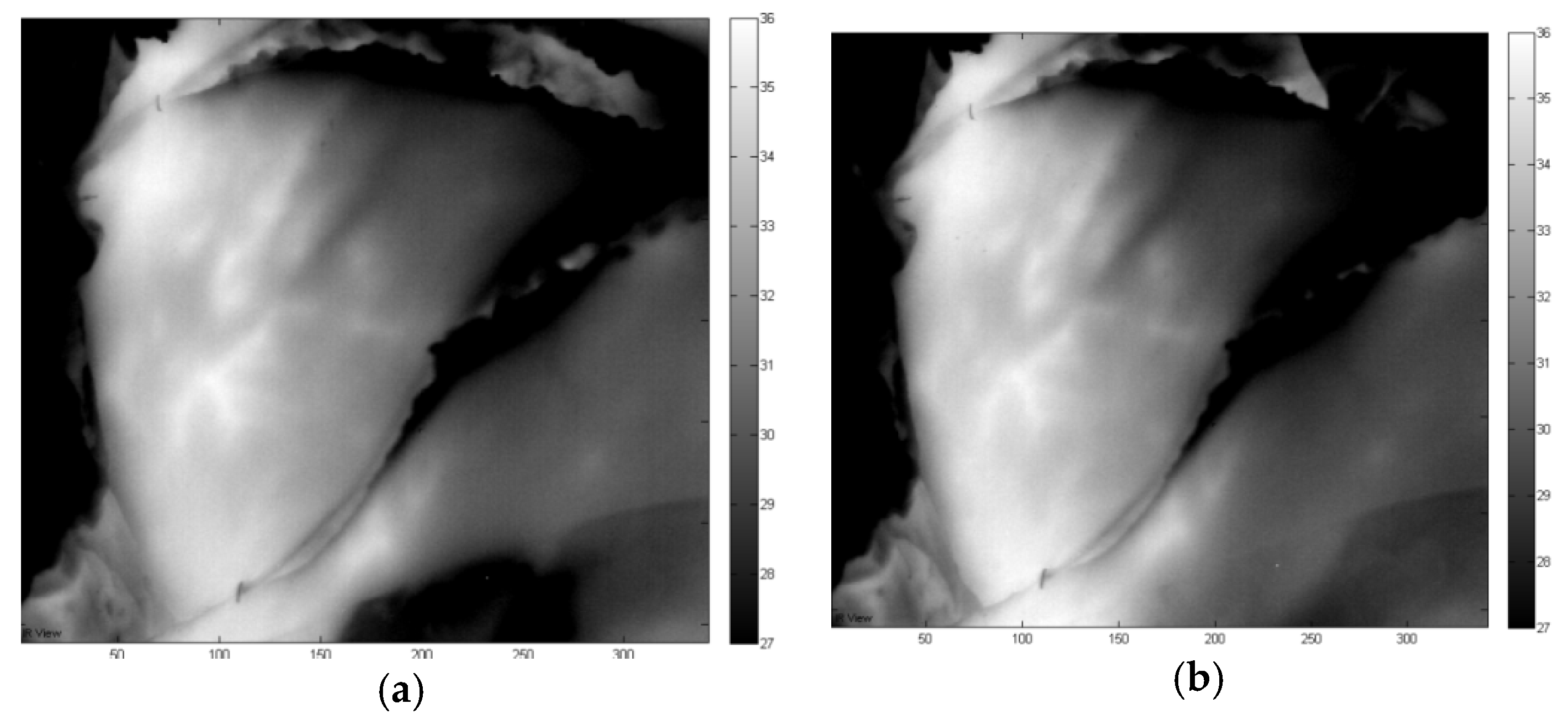
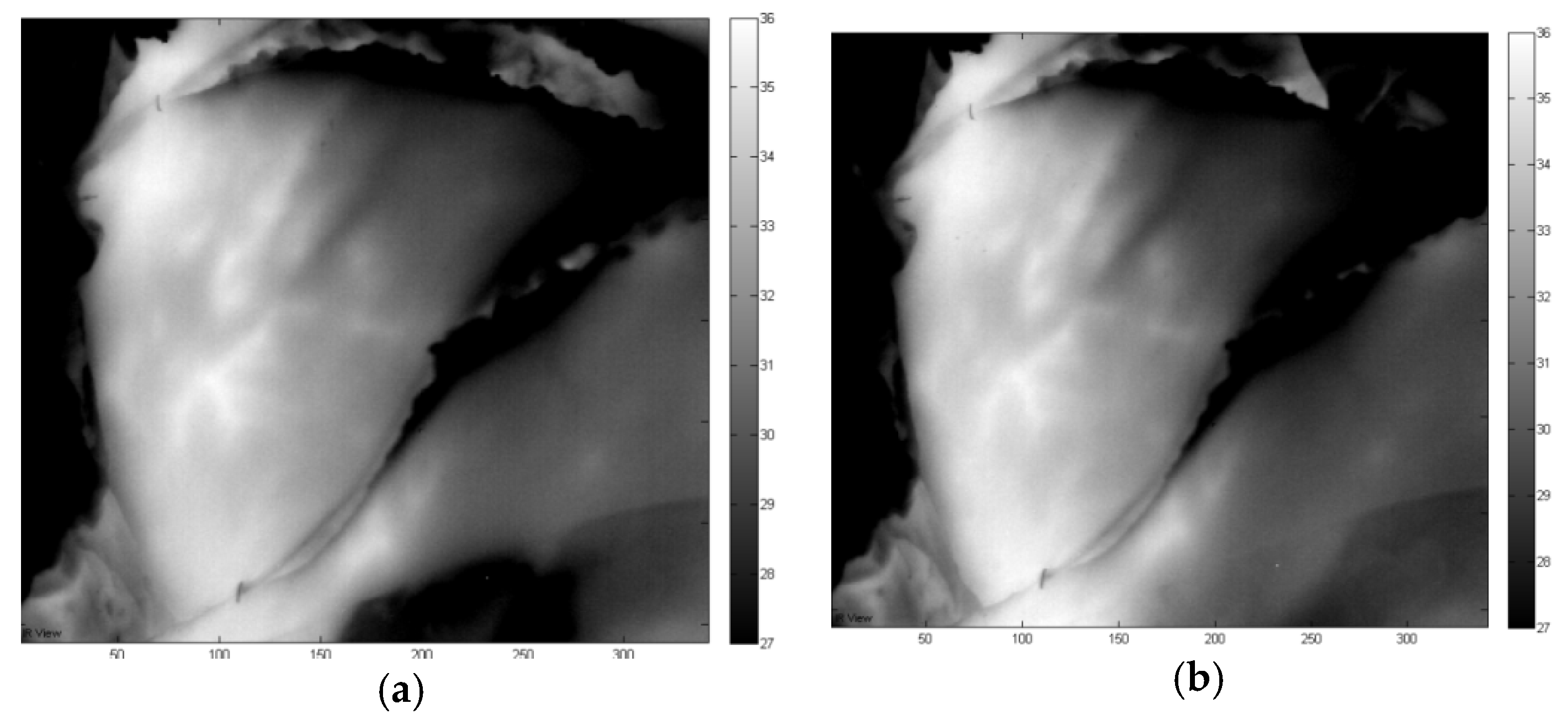
3.2. Left Flap in Rest: Vein A Closed and Vein B Open
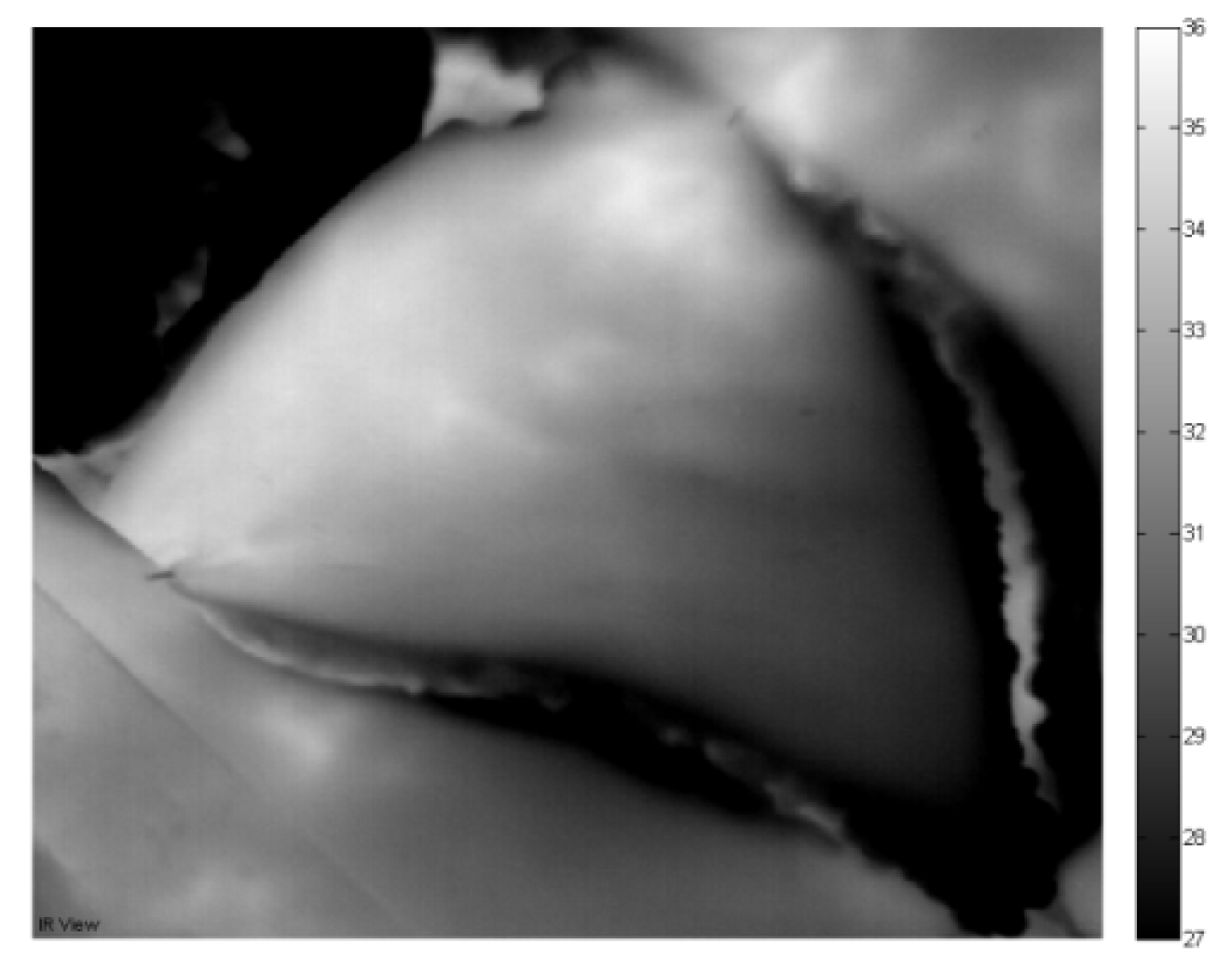
3.3. Left Flap in Rest: Perforator A Open and Perforator B Closed
4. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Weum, S.; Mercer, J.B.; de Weerd, L. Evaluation of dynamic infrared thermography as an alternative to CT angiography for perforator mapping in breast reconstruction: A clinical study. BMC Med. Imaging 2016, 16, 43. [Google Scholar]
- De Weerd, L.; Weum, S.; Mercer, J.B. Dynamic Infrared Thermography (DIRT) in the preoperative, intraoperative and postoperative phase of DIEP flap surgery. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 694–695. [Google Scholar]



© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steenackers, G.; Verstockt, J.; Cloostermans, B.; Thiessen, F.; Ribbens, B.; Tjalma, W. Infrared Thermography for DIEP Flap Breast Reconstruction Part I: Measurements †. Proceedings 2019, 27, 48. https://doi.org/10.3390/proceedings2019027048
Steenackers G, Verstockt J, Cloostermans B, Thiessen F, Ribbens B, Tjalma W. Infrared Thermography for DIEP Flap Breast Reconstruction Part I: Measurements †. Proceedings. 2019; 27(1):48. https://doi.org/10.3390/proceedings2019027048
Chicago/Turabian StyleSteenackers, Gunther, Jan Verstockt, Ben Cloostermans, Filip Thiessen, Bart Ribbens, and Wiebren Tjalma. 2019. "Infrared Thermography for DIEP Flap Breast Reconstruction Part I: Measurements †" Proceedings 27, no. 1: 48. https://doi.org/10.3390/proceedings2019027048
APA StyleSteenackers, G., Verstockt, J., Cloostermans, B., Thiessen, F., Ribbens, B., & Tjalma, W. (2019). Infrared Thermography for DIEP Flap Breast Reconstruction Part I: Measurements †. Proceedings, 27(1), 48. https://doi.org/10.3390/proceedings2019027048