Genetic Testing for Inherited Thrombophilia: 20 Years of Experience in a University and Tertiary Care Centre †

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
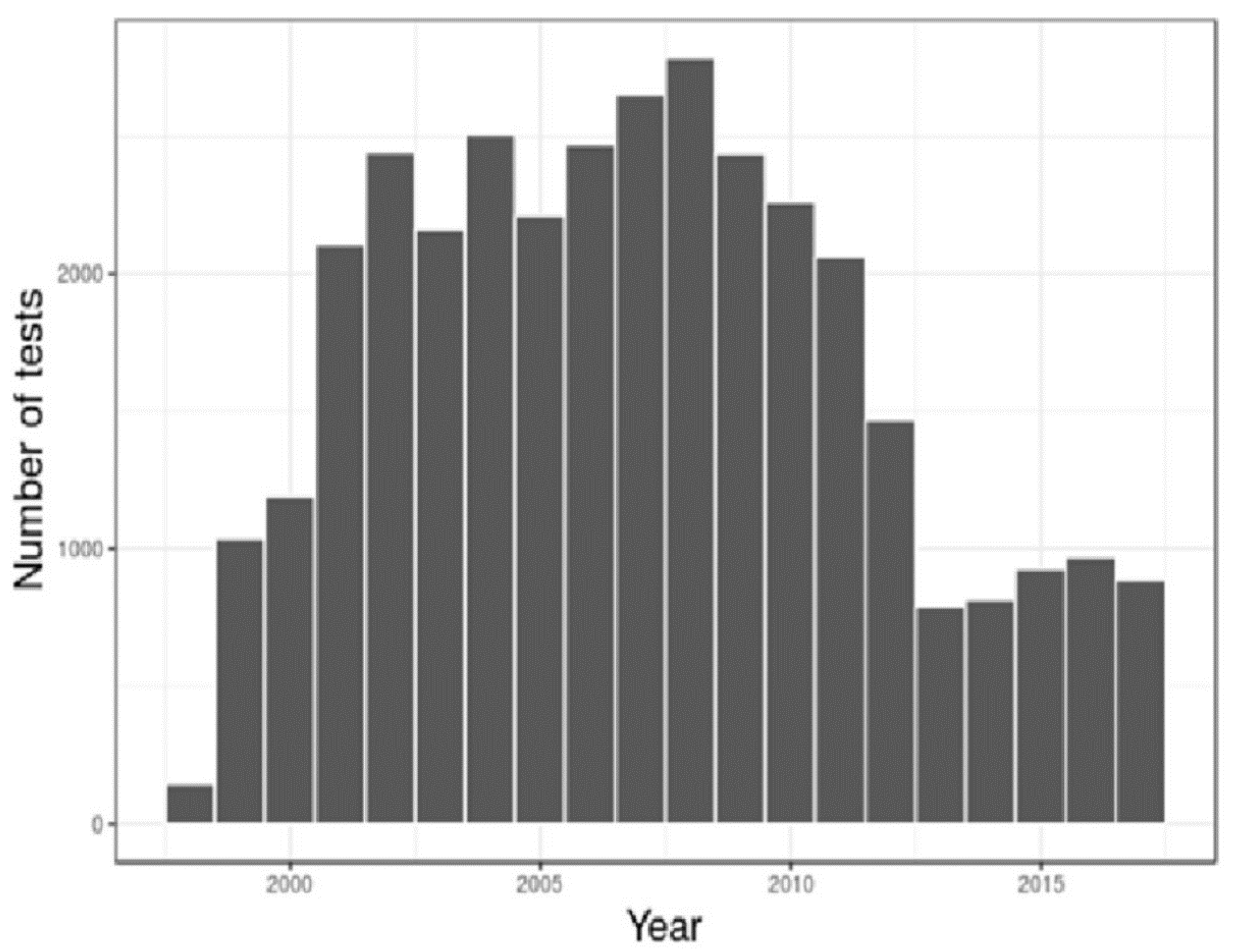
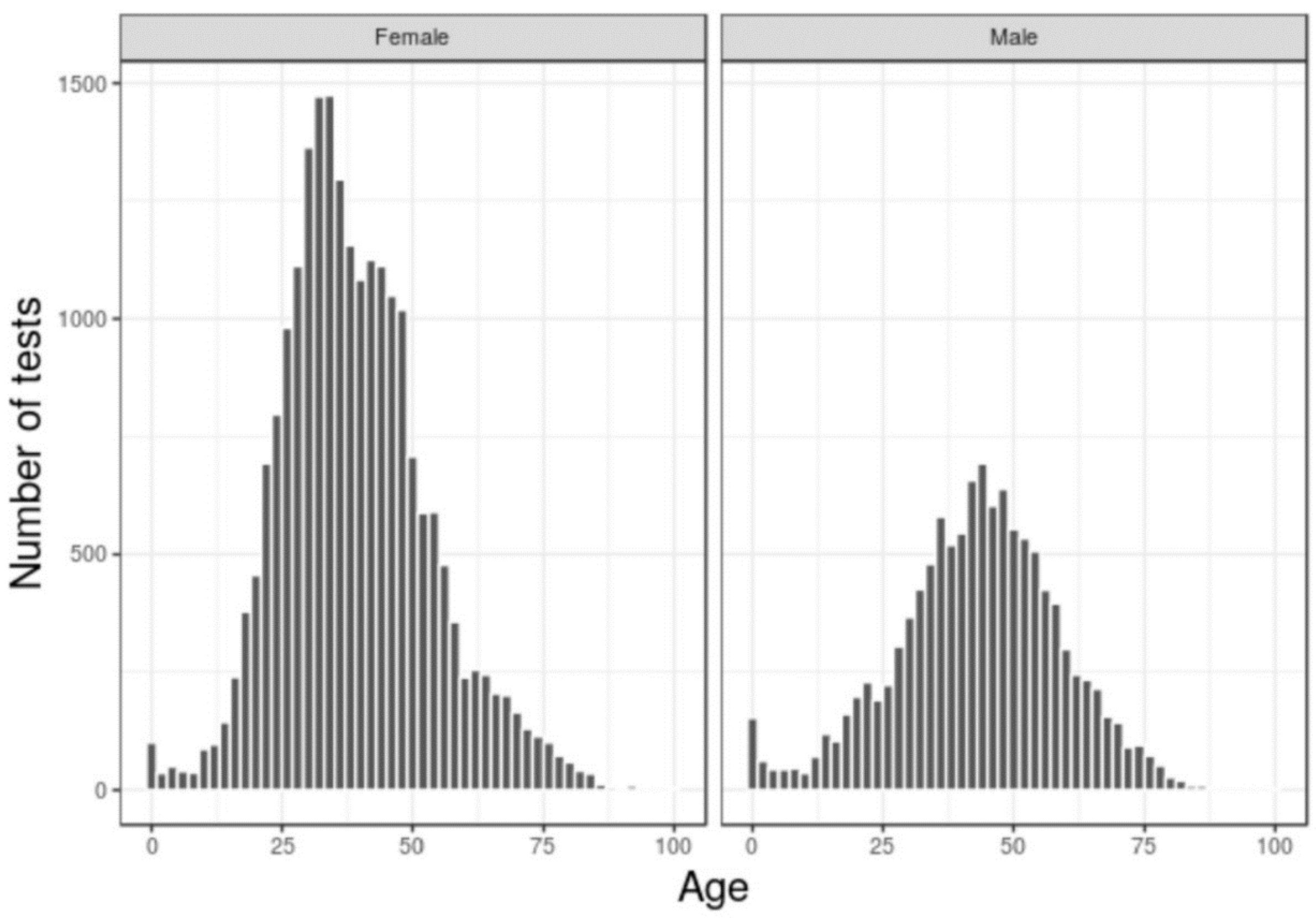
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Jean Connors, J.C. Thrombophilia Testing and Venous Thrombosis. N. Engl. J. Med. 2017, 377, 1177–1187. [Google Scholar] [CrossRef]
- Kearon, K.C.; Aki, E.A.; Comerota, A.J. Antithrombotic therapy for VTE disease: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2012, 141, e419S–e494S. [Google Scholar] [CrossRef]
- Kearon, K.C.; Aki, E.A.; Ornelas, J. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef] [PubMed]
- Hicks, L.K.; Bering, H.; Carson, K.R. The ASH Choosing Wisely campaign: Five hematologic tests and treatments to question. Blood 2013, 122, 3879–3883. [Google Scholar] [CrossRef] [PubMed]
- Venous Thromboembolic Diseases: The Management of Venous Thromboembolic Diseases and the Role of Thrombophilia Testing; National Clinical Guideline Centre, Royal College of Physicians: London, UK, 2012.
- Stevens, S.M.; Woller, S.C.; Bauer, K.A. Guidance for the evaluation and treatment of hereditary and acquired thrombophilia. J. Thromb. Thrombolysis 2016, 41, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Mark, S.H. Genetic Testing for Thrombophilia Mutations. Semin. Thromb. Hemost. 2005, 31, 33–38. [Google Scholar]

{kind=link}
{kind=link}
| Tests Performed N | Negative Tests N, % | Positive Tests | ||
|---|---|---|---|---|
| Homozygous Mutant N, % | Heterozygous N, % | |||
| FVL | 9.008 | 7.882 (87.5%) | 33 (0.37%) | 1.093 (12.1%) |
| PGM | 13.392 | 12.574 (93.9%) | 21 (0.16%) | 797 (6.0%) |
| MTHFR Gene mutation (C6677T) | 11.533 | 4.788 (41.5%) | 1.461 (12.7%) | 5.284 (45.8%) |
| MTHFR Gene mutation (A1298C) | 408 | 192 (47.1%) | 30 (7.35%) | 186 (45.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaz, C.; Bischoff, F.; Monteiro, F.; Lopes, M.; Vasconcelos, F.; Bastos, P.; Tavares, G.; Ferreira, M.; Amorim, A.; Koch, C. Genetic Testing for Inherited Thrombophilia: 20 Years of Experience in a University and Tertiary Care Centre. Proceedings 2018, 2, 527. https://doi.org/10.3390/proceedings2090527
Vaz C, Bischoff F, Monteiro F, Lopes M, Vasconcelos F, Bastos P, Tavares G, Ferreira M, Amorim A, Koch C. Genetic Testing for Inherited Thrombophilia: 20 Years of Experience in a University and Tertiary Care Centre. Proceedings. 2018; 2(9):527. https://doi.org/10.3390/proceedings2090527
Chicago/Turabian StyleVaz, Cláudia, Francisco Bischoff, Fátima Monteiro, Manuela Lopes, Filipe Vasconcelos, Pedro Bastos, Gilberto Tavares, Marina Ferreira, Ana Amorim, and Carmo Koch. 2018. "Genetic Testing for Inherited Thrombophilia: 20 Years of Experience in a University and Tertiary Care Centre" Proceedings 2, no. 9: 527. https://doi.org/10.3390/proceedings2090527
APA StyleVaz, C., Bischoff, F., Monteiro, F., Lopes, M., Vasconcelos, F., Bastos, P., Tavares, G., Ferreira, M., Amorim, A., & Koch, C. (2018). Genetic Testing for Inherited Thrombophilia: 20 Years of Experience in a University and Tertiary Care Centre. Proceedings, 2(9), 527. https://doi.org/10.3390/proceedings2090527