1. Introduction: An Outline of Healing Concrete History
The history of autonomous self-healing concrete can be separated in three phases. In the early 1990s the concept is introduced by the pioneering work of Dry designing a configuration that permits repair chemicals release in time from fibers embedded into the cement matrix (Phase 1) [
1]. The study ends with a series of queries that remained unanswered until a decade after. Inspired by the study of White et al. that launched the first autonomously healed polymer, research towards the same direction searching for an autonomously healed concrete system has flourished in the 2000s (Phase 2) [
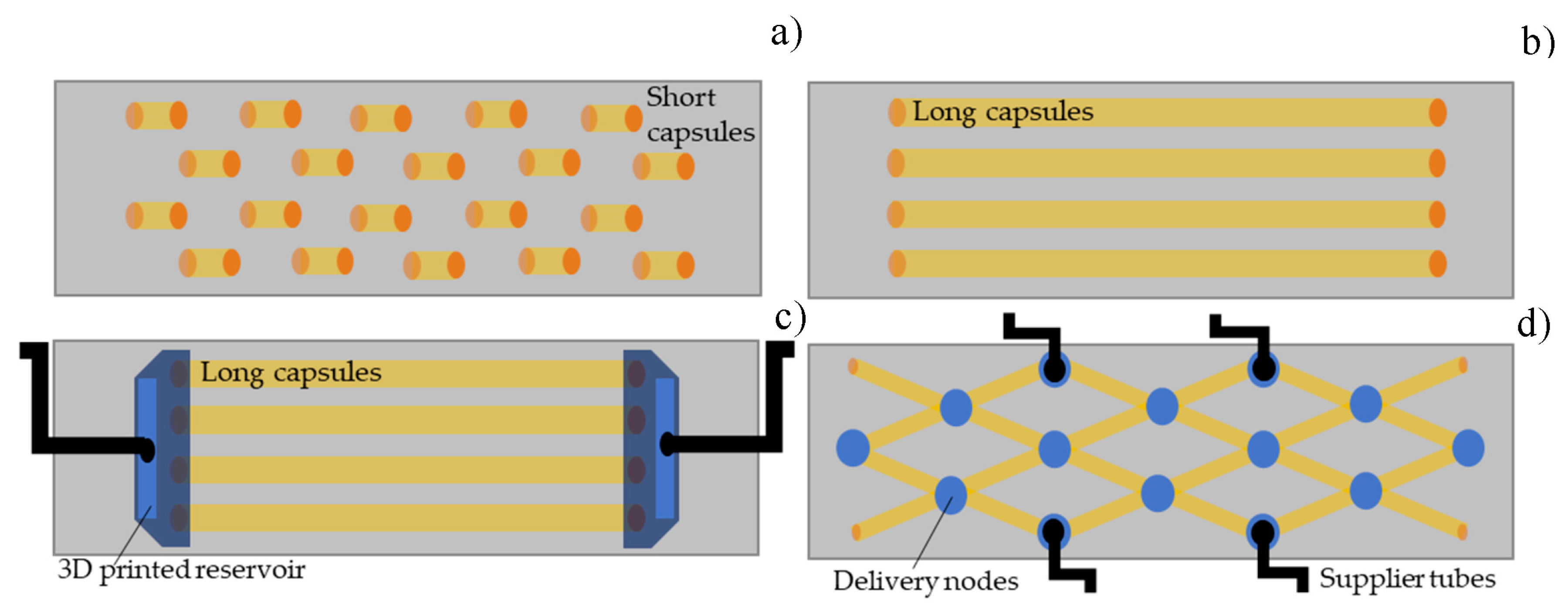
2]. By 2010, the research community agreed that the optimal healing design consists of an one-dimensional array of tubular capsules that carry polymer-based healing agent and are embedded into concrete during casting (illustrated in
Figure 1 and
Figure 2a) [
3]. The capsules are ruptured under stress releasing the agent that fills the crack void achieving in this way almost instant crack sealing and mechanical restoration [
4]. The capsules nature was selected so as to be brittle enough to break under cracking, but strong enough to survive concrete mixing procedures and also the aggressive concrete chemical environment [
5].
The path has been etched towards autonomous healing concrete, though the ideal configuration was still being sought. Numerous parametric studies have been emerged evaluating the capsules geometry [
6] (thickness, length (
Figure 2b) [
7], inner/outer diameter [
8]), the capsules nature [
9] (from soft elastomers and polymers [
10] to brittle glass, ceramics and cement [
8]), the healing agent chemistry [
11,
12], the capsules-concrete interface bonding, the crack-healing agent interaction [
13].
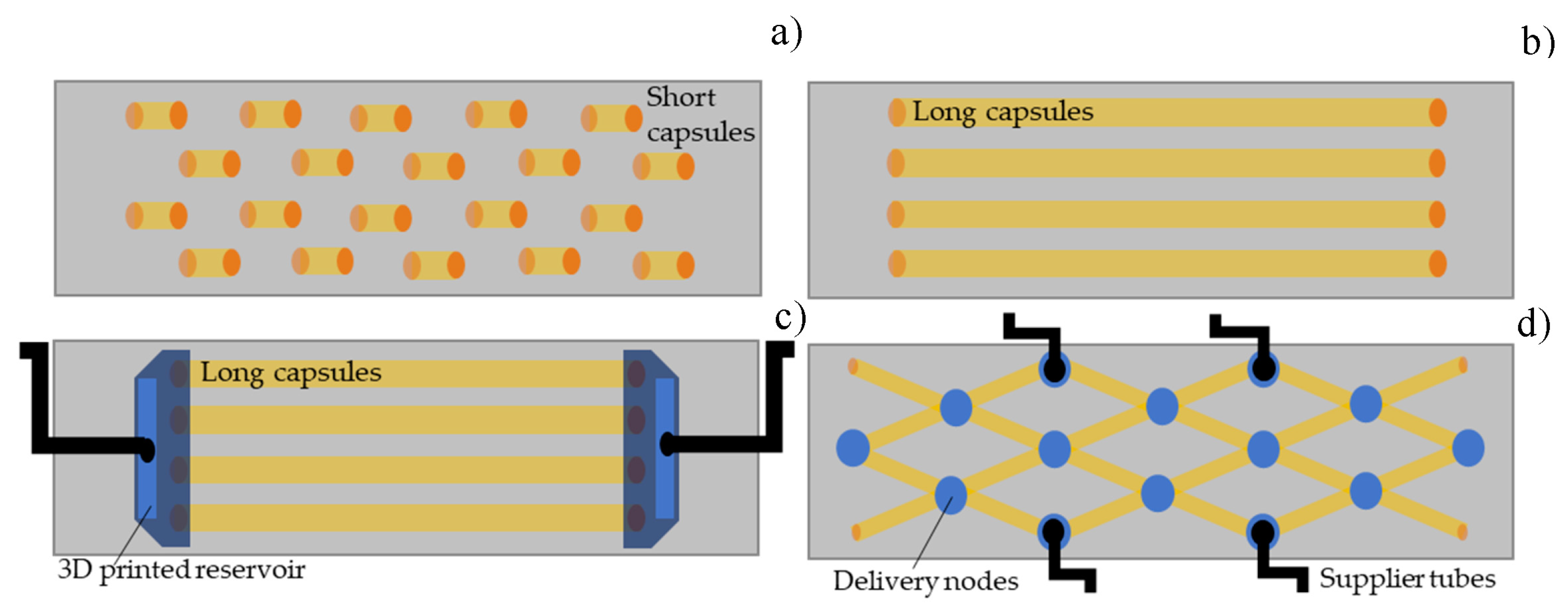
The dawn of a new era in self-healing concrete is set around 2015 with a series of feasibility studies and projects that investigate the design of vascular networks carrying healing agent aiming to provide repetitive sealing and mechanical repair this time in real-size construction elements (1D/2D slab, beam, wall) [
14,
15,
16]. The agent is partly stored into long thin capsules [
17] that additionally provide beneficial impact on concrete toughness and partly into reservoirs connected to the capsules and attached to the concrete element (
Figure 2c,d). Internal pressure controls the agent release in the presence of the cracks that break the capsule. The agent circulates into the capsule network due to capillary forces achieving simultaneous cracks healing at different locations in concrete. Repeatable healing is feasible since additional healing agent can be delivered through the reservoirs. This optimized healing system permits two crack scenarios:
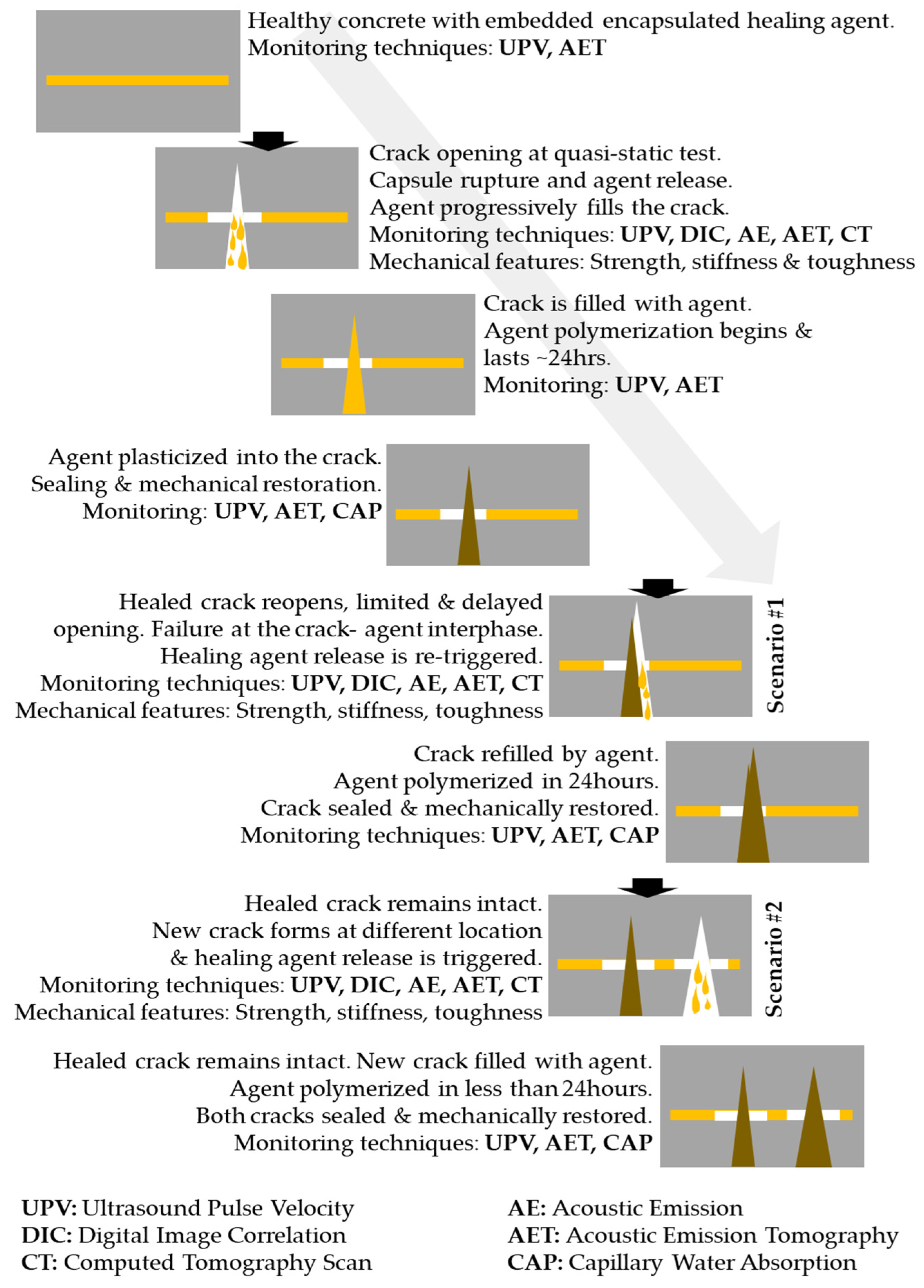
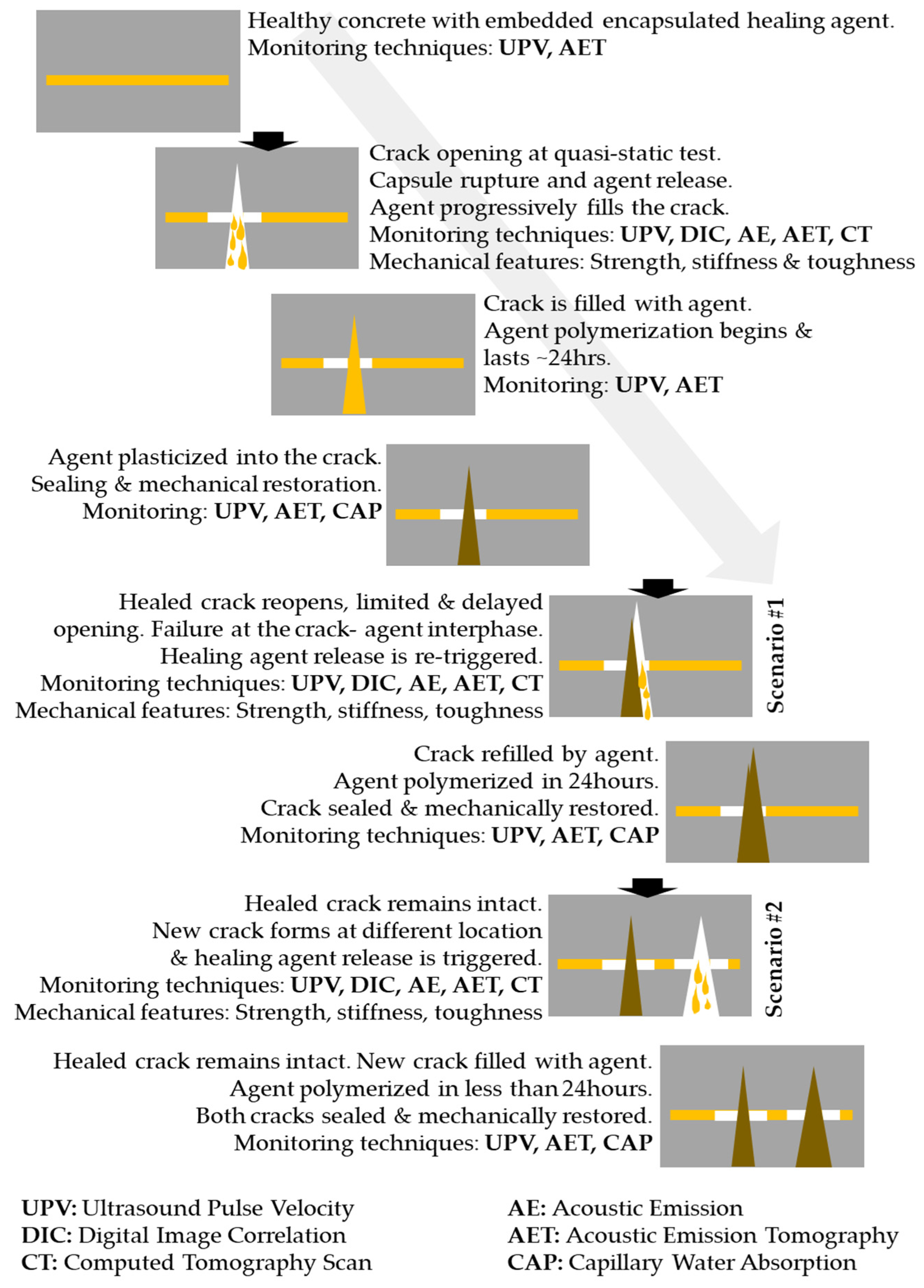
- Cracks are sealed and mechanically restored, therefore material continuity is reinstated and concrete is again a homogeneous robust media. Under service loads, a crack forms at different position (not at the effectively healed region). Crack redistribution permits stress release and enhances the fracture toughness.
- The healed crack reopens under service loads, but crack propagation is arrested or significantly delayed due to the presence of polymerized agent that interlocks between the fractured concrete surfaces. Fracture toughness increases due to the development of new crack surfaces.
2. Sensing of Autonomous Healing
The use of advanced monitoring methods is the key behind the fast progress of concrete healing technology. Traditionally, mechanical test analysis was accompanied by fracture theories or models and monitoring methods to understand the cracking phenomena in concrete. Constitutive laws and fracture models can describe in detail the way that concrete responds to fracture.
However, ‘healing revolution’ introduces the reverse to fracture process: crack closure and mechanical restoration. The autonomous repair procedure introduces a condition that cannot be assessed based on conventional fracture mechanics tools, standardized material laws or traditional experimental techniques. The material response after healing remains a black box and advanced or modified experimental tools are urged to verify repair and decode its mechanisms.
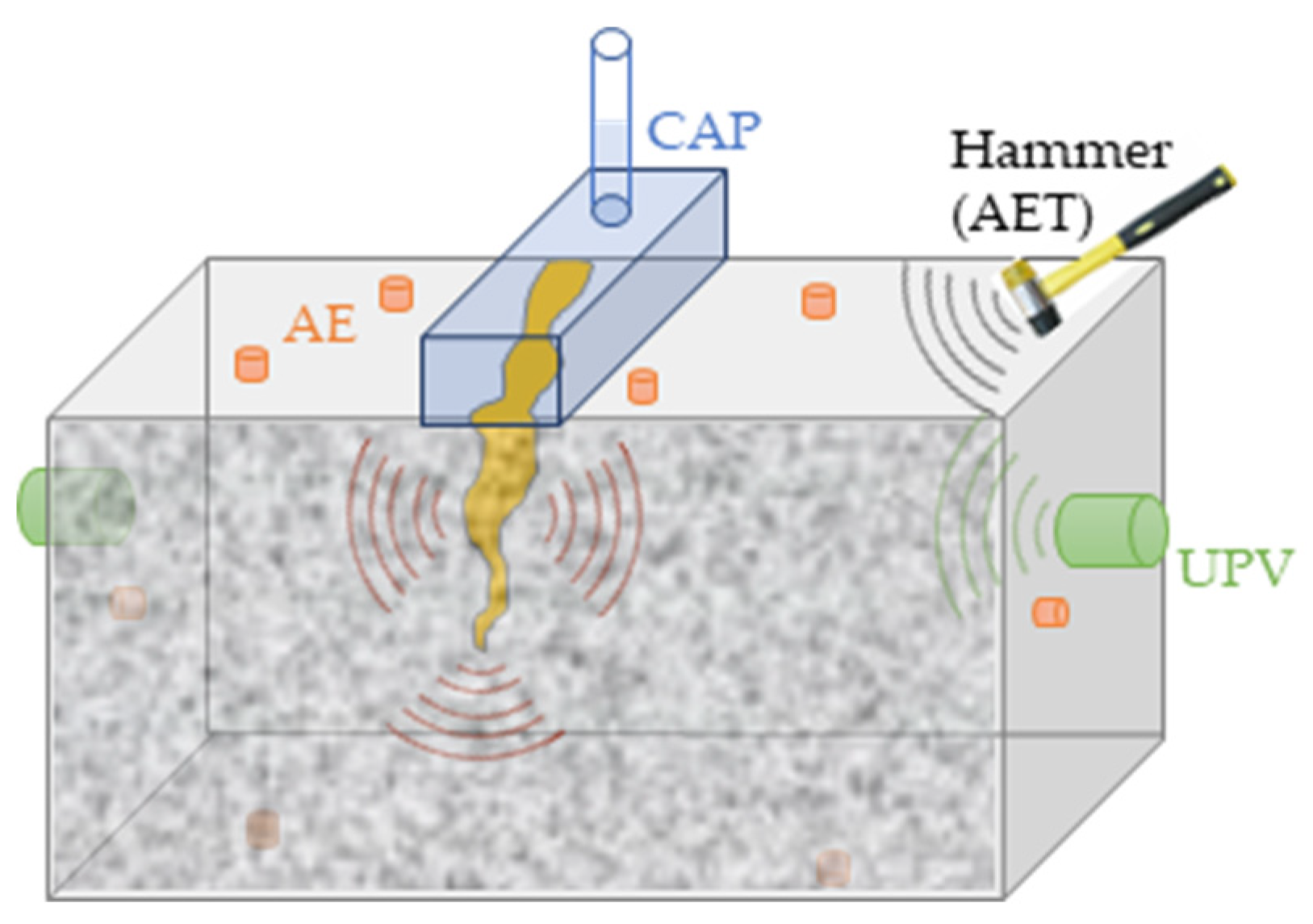
Phase 2 and 3 progresses on healing technology go along with the redesign and establishment of advanced integrated monitoring systems. It is imperative to configure a link between experimentally measured fracture variables (strength, stiffness, toughness, fracture energy) and the continuous monitoring using numerous non-destructive and other advanced methods. Acoustic Emission (AE), Acoustic Emission tomography (AET), Ultrasound Pulse Velocity (UPV), Digital Image Correlation (DIC), Computed Tomography scan (CT), Capillary Water Absorption (CAP) are invoked. It is shown that the synergy of different methods provides a comprehensive understanding of autonomous repair in concrete. Each method contributes at a distinctive moment of testing. For instance, DIC measures the crack reopening after healing. AE detects the capsules rupture and sets the healing triggering moment. UPV verifies crack closure and material restoration. Each method’s contribution is briefly and critically presented in the following section.
In most of the studies assessing the healing efficiency an established test procedure is followed as illustrated in
Figure 1. Regardless the encapsulation design (
Figure 2), bending (crack opening) mode is used and the load is applied in loading/reloading cycles:
- At the first test cycle a unique or several cracks form and propagate triggering capsules rupture and activating the healing mechanism. The test is crack controlled and stops when a macro-crack of few hundred millimeters is formed. Initial strength, stiffness and fracture toughness are measured.
- An up to 24 h pause is required to permit the agent polymerization into the crack void. Later, the bending test is repeated. The healing efficiency is calculated based on the stiffness, strength and toughness regain. The loading/reloading regime can be repeatedly applied when capsules networks are used and agent refilling is possible through reservoir suppliers (
Figure 2c,d).
3. Main Contributions of Advanced Experimental Techniques
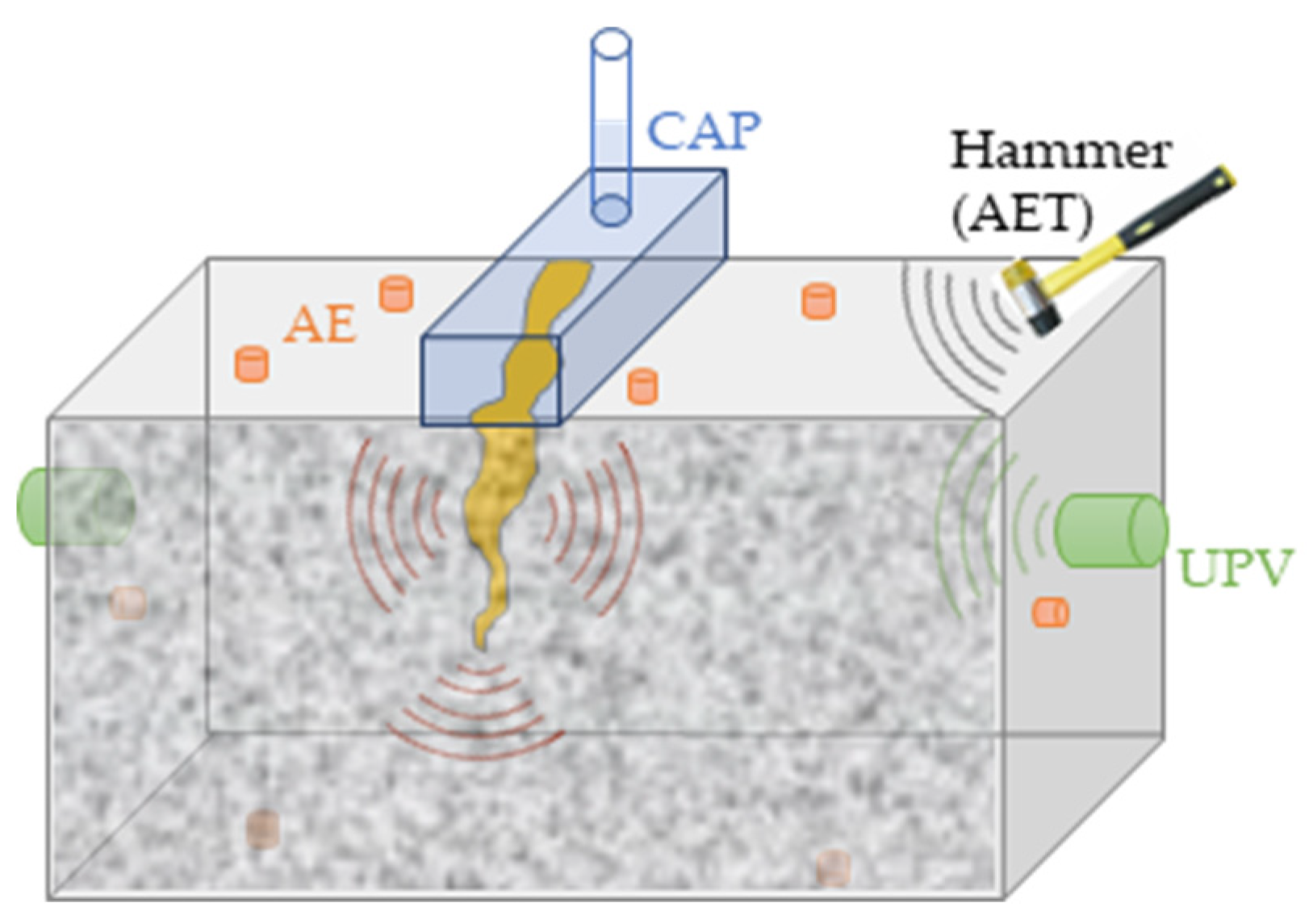
The contributions overview of each monitoring method applied in self-healing concrete studies is illustrated in the configuration in
Figure 3 and briefly described at the following paragraphs.
Acoustic Emission (AE). An array of acoustic transducers mounted to the concrete surface can capture the elastic waves emitted in the presence of a crack that forms, widens or reopens after healing [
18]. The wave arrival time, magnitude and shape can be indicative of fracture source localization and mode. AE contributes by detecting in time and in space the capsules rupture, therefore the healing triggering mechanism [
19,
20]. AE events population can highlight the zones being active at the loading cycle and carrying delayed acoustic activity after healing, therefore the zones where effective repair leads to crack reopening arrest and reversely detect new cracks formed only after healing. The latter is important in large scale samples where the location of newly formed damage is crucial for the re-distribution of the healing agent through vascular capsules networks.
Digital Image Correlation (DIC). Plane strain and deformation maps are key tools to detect cracking onset, opening and closure after healing. Studies on both small and large-scale samples using a pair of high-resolution cameras and post-processing speckle-pattern image analysis software successfully detected new cracks formed after healing and healed cracks reopening delayed in time. Additionally, DIC analysis has been accompanied by AE to detect healing agent response to cracking and detect debonding at the agent-concrete cracked surface.
Ultrasound Pulse Velocity (UPV). Ultrasound velocity is measured using an emitter-receiver transducers pair before and after each loading/reloading cycle and during the healing agent polymerization process (discrete measurements during curing). The velocity is associated to the structural health condition of the sample. The measurement is straight-forward in the case of small-scale samples carrying a unique bending crack: velocity increase after healing triggering indicates effective crack repair [
21]. The healed zone size can be quantified by performing UPV measurements along the crack’s height. The analysis becomes more complex in larger concrete samples carrying several cracks. In the latter case, only qualitative conclusions can be drawn regarding the global efficiency of the healing system. UPV is successfully used to verify DIC and AE findings.
Ultrasound Pulse Velocity using embedded piezoelectric transducers (SMAG). A more advanced UPV technology was recently applied to assess healing efficiency from the concrete interior. In detail, the piezoelectric transducers are not mounted on the concrete surface, instead are embedded into concrete during casting [
22]. This way wave distortion due to surface effects is eliminated and the measurement is focused on local zones where healing is present. The studies have proven that SMAG measurements are effective in gauge length up to 1 m [
23]. The performance of the method on large-scale concrete slabs carrying capsules networks still needs to be tested.
Acoustic Emission Tomography (AET) [24,25]. A preliminary study done in collaboration with the University of Kyoto (ITIL Laboratory) has shown that AET wave velocity maps can highlight the material homogeneity restoration after healing. Three-dimensional volume maps built up to date can indicate the mechanical restoration (translated to velocity regain after healing) on small-scale concrete beams but the analysis spatial accuracy remains limited. For this reason, the results are not communicated. In future, an experimental campaign should be launched assessing healing efficiency on large scale concrete structures where macro-cracks are healed by vascular capsules networks.
Computed tomography scan (CT). Pioneering work of Van Tittelboom et al. has shown that capsule rupture and healing agent release into the crack void can be visualized by advanced scanning techniques [
3]. In post-mortem stage and in small-size samples, the volume of the concrete crack that is sealed was measured and related to the agent rheology [
7]. However, the method cannot be applied in real-size structures since the volume under investigation can be only up to few hundred millimeters. Analysis of macro-cracks using this method remains cost-ineffective.
Capillary Water Absorption (CAP). CAP was previously applied to assess the sealing of cracks after healing in small-scale concrete samples [
7,
26]. The method obtains robust and quantitative results in the case that a unique crack has been formed, but it is less effective in large scale concrete samples where multiple connected cracks interact. The latter cracks form several alternatives to main flow paths, therefore the water flow into the concrete volume cannot be accurately mapped. Additionally, a modified CAP test performed on large-scale concrete beams has proven that water penetration can affect the healing process since hydration modifies the fracture process zone and interferes with the agent polymerization.
4. Discussion
The brief overview of advanced monitoring methods has shown that the transition from small- to large-scale concrete introduces challenges for the monitoring process. Techniques that are successfully applied on small-scale samples are less efficient in voluminous concrete structures. In any case, experience obtained at both scales provides a great feedback for the design of a healing systems applied on real concrete elements. Future studies should focus on the performance of concrete elements carrying vascular networks and tested under repetitive incremental and/or dynamic loading. This way, the feasibility of autonomous healing is evaluated in realistic loading configurations, reaching progressively the construction materials market [
27]. The monitoring methods synergy invokes a main observation: only by optimally combining different experimental techniques and building an autonomous sensing ability, self-healing concrete can be realized.
Author Contributions
E.T., D.G.A., N.D.B., T.S. and D.V.H. conceived and designed the experiments; E.T. performed the experiments and analyzed the data; D.G.A., N.D.B., T.S. and D.V.H. contributed reagents/materials/analysis tools; E.T. wrote the paper.
Acknowledgments
Financial support of the Research Foundation Flanders (FWO-Vlaanderen, Project No 28976) and SIM-SECEMIN research project under the program SHE for this study is gratefully acknowledged.
Conflicts of Interest
Declare conflicts of interest or state. The authors declare no conflict of interest. The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
References
- Dry, C.M. Three designs for the internal release of sealants, adhesives, and waterproofing chemicals into concrete to reduce permeability. Cem. Concr. Res. 2000, 30, 1969–1977. [Google Scholar] [CrossRef]
- White, S.R.; Sottos, N.R.; Geubelle, P.H.; Moore, J.S.; Kessler, M.; Siriam, S.R.; Brown, E.N.; Viswanathan, S. Autonomic healing of polymer composites. Nature 2001, 409, 794. [Google Scholar] [CrossRef] [PubMed]
- Van Tittelboom, K.; De Belie, N.; Van Loo, D.; Jacobs, P. Self-healing efficiency of cementitious materials containing tubular capsules filled with healing agent. Cem. Concr. Compos. 2011, 33, 497–505. [Google Scholar] [CrossRef]
- Wu, M.; Johanneson, B.; Geiker, M. A review: Self-healing in cementitious materials and engineered cementitious composite as a self-healing material. Constr. Build. Mater. 2012, 28, 571–583. [Google Scholar] [CrossRef]
- Van Tittelboom, K.; De Belie, N. Self-healing in cementitious materials-A review. Materials 2013, 6, 2182–2217. [Google Scholar] [CrossRef] [PubMed]
- Kanellopoulos, A.; Giannaros, P.; Palmer, D.; Kerr, A.; Al-Tabbaa, A. Polymeric microcapsules with switchable mechanical properties for self-healing concrete: Synthesis, characterization and proof of concept. Smart Mater. Struct. 2017, 26, 045025. [Google Scholar] [CrossRef]
- Van Tittelboom, K.; Tsangouri, E.; Van Hemelrijck, D.; De Belie, N. The efficiency of self-healing concrete using alternative manufacturing procedures and more realistic crack patterns. Cem. Concr. Compos. 2015, 57, 142–152. [Google Scholar] [CrossRef]
- Tsangouri, E.; Gilabert, F.A.; Aggelis, D.G.; De Belie, N.; Van Hemelrijck, D. Concrete Fracture Energy Increase by Embedding Capsules with Healing Ability: The Effect of Capsules Nature. Proceedings of 2nd International RILEM/COST Conference on Early Age Cracking and Serviceability in Cement-based Materials and Structures, Brussels, Belgium, 12–14 September 2017. [Google Scholar]
- Kanellopoulos, A.; Litina, A.; Giannaros, P.; Al-Tabbaa, A. Effect of Different Types of Polymeric Microcapsules on the Self-Healing Efficiency of Cement Based Composites. In Proceedings of the FraMCos-9, Berkley, CA, USA, 29 May–1 June 2016. [Google Scholar]
- Hilloulin, B.; Van Tittelboom, K.; Gruyaert, E.; De Belie, N.; Loukili, A. Design of polymeric capsules for self-healing concrete. Cem. Concr. Compos. 2015, 55, 298–307. [Google Scholar] [CrossRef]
- Van Tittelboom, K.; Adesanya, K.; Dubruel, P.; Van Puyvelde, P.; De Belie, N. Methyl methacrylate as a healing agent for self-healing cementitious materials. Smart Mater. Struct. 2011, 20, 125016. [Google Scholar] [CrossRef]
- Kanelllopoulos, A.; Qureshi, T.S.; Al-Tabbaa, A. Glass encapsulated minerals for self-healing in cement based composites. Constr. Build. Mater. 2015, 98, 780–791. [Google Scholar] [CrossRef]
- Feiteira, J.; Tsangouri, E.; Gruyaert, E.; Lors, C.; Louis, G.; De Belie, N. Monitoring crack movement in polymer-based self-healing concrete through digital image correlation, acoustic emission analysis and SEM in-situ loading. Mater. Des. 2017, 115, 238–246. [Google Scholar] [CrossRef]
- Minnebo, P.; Thierens, G.; De Valck, G.; Van Tittelboom, K.; De Belie, N.; Van Hemelrijck, D.; Tsangouri, E. Novel Design of Autonomously Healed Concrete: Towards Vascular Healing Network. Materials 2017, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Materials4Life. Available online: http://m4l.engineering.cf.ac.uk/ (accessed on 2 May 2018).
- Huang, H.; Ye, G.; Shui, Z. Feasibility of self-healing in cementitious materials–By using capsules or a vascular system? Constr. Build. Mater. 2014, 63, 108–118. [Google Scholar] [CrossRef]
- Sangadji, S.; Schlangen, E. Self-Healing of Concrete Structures-Novel approach using porous network concrete. J. Adv. Concr. Technol. 2012, 10, 185–194. [Google Scholar] [CrossRef]
- Grosse, C.; Malm, F. Combination of inspection and monitoring techniques for the detection of fractures in concrete with self-healing properties. In Proceedings of the FraMCoS-9, Berkley, CA, USA, 29 May–1 June 2016. [Google Scholar]
- Tsangouri, E.; Aggelis, D.G.; Van Tittelboom, K.; De Belie, N.; Van Hemelrijck, D. Detecting the activation of a self-healing mechanism in concrete by acoustic emission and digital image correlation. Sci. World J. 2013, 2013, 424560. [Google Scholar] [CrossRef] [PubMed]
- Van Tittelboom, K.; De Belie, N.; Lehmann, F.; Grosse, C.U. Acoustic emission analysis for the quantification of autonomous crack healing in concrete. Constr. Build. Mater. 2012, 28, 333–341. [Google Scholar] [CrossRef]
- Gruyaert, E.; Feiteira, J.; De Belie, N.; Malm, M.; Grosse, C.U.; Tziviloglou, E.; Schlangen, E.; Tsangouri, E. Non-destructive testing techniques to evaluate the healing efficiency of self-healing concrete at lab-scale. Proceedings of 6th International Conference on Emerging Technologies in Non-Destructive Testing, Brussels, Belgium, 27–29 May 2015. [Google Scholar]
- Tsangouri, E.; Karaiskos, G.; Aggelis, D.G.; Deraemaeker, A.; Van Hemelrijck, D. Crack sealing and damage recovery monitoring of a concrete healing system using embedded piezoelectric transducers. Struct. Health Monit. 2015, 14, 462–474. [Google Scholar] [CrossRef]
- Karaiskos, G.; Tsangouri, E.; Aggelis, D.G.; Deraemaeker, A.; Van Hemelrijck, D. Damage detection monitoring applications in self-healing concrete structures using embedded piezoelectric transducers and recovery. JPCS 2015, 628, 012110. [Google Scholar] [CrossRef]
- Shiotani, T.; Okude, N.; Momoki, S.; Kobayashi, Y. Proposal of assessment method for infrastructures by AE tomography. Proceedings of National Conference on Acoustic Emission, Kyoto, Japan, 5–8 December 2011. (In Japanese). (In Japanese). [Google Scholar]
- Kobayashi, Y.; Shiotani, T. Seismic tomography with estimation of source location for concrete structure. Proceedings of Structural Faults and Repair, Edinburgh, UK, 3–5 July 2012. [Google Scholar]
- Li, W.; Jiang, Z.; Yang, Z.; Zhao, N.; Yuan, W. Self-healing efficiency of cementitious materials containing microcapsules filled with healing adhesive: Mechanical restoration and healing process monitored by water absorption. PLoS ONE 2013, 8, 81616. [Google Scholar] [CrossRef] [PubMed]
- Van Breugel, K. Is there a market for self-healing cement-based materials? In Proceedings of the 1st International Conference on Self-healing Materials, Noordwijk Aan Zee, The Netherlands, 18–20 April 2007. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 



{kind=link}
{kind=link}
{kind=link}