1. Introduction
Accuracy, speed, and economy of effort are crucial determinants of surgical skills. However, quick reaction performance, team coordination in the context of long procedures, and trade-offs between service and safety still have a high potential of error for a surgeon [
1]. Reports published in recent years ([
2,
3]) have documented the same observation: there’s an important annual number of medical adverse events. It costs a lot in terms of hospital expenses and patients satisfaction.
Therefore, surgery evaluation methods are being more demanded, especially for laparoscopy that is more challenging compared to open surgery. Indeed, surgeons must operate in a three-dimensional space through a two-dimensional projection on a monitor, which results in a loss of depth perception. Also, the length of the instruments induces a loss of precision, as well as a lack of tactile feedback. Thus, reinforced training must be carried out, whether for already experienced abdominal surgeons or for residents, because of the longer traditional learning curve.
Beyond the limits of current traditional methods (cadavers, animals, box-trainers), an open problem remains to dispose of a robust method to objectively quantify resident’s apprenticeship. Virtual Reality (VR) simulators aim to complement traditional training tasks by providing high quality simulations in surgery exercises. It has been proved to be efficient for laparoscopic training. The more sophisticated VR simulators measure the trainee performance through haptic devices that capture movements but not fine movements that could be captured with an Instrumented Glove [
4].
2. Materials and Methods
2.1. The Instrumented Glove [4]
The IGlove is made of two parts: an elastic-textile glove with textile small pockets for the sensors, and a hub, strapped to the wrist, for the signal acquisition. The sensors are Inertial Measurement Units (IMU, model MPU-9250, InvenSense) and embed a 3-axis accelerometer, a 3-axis gyroscope and a 3-axis magnetometer. Up to 8 channels can be used at the same time, for capturing different phalanges’ motion. In this study, when analyzing the hand and fingers displacements during laparoscopic exercises, four sites were chosen: thumb, index, middle finger and upper hand face.
2.2. Study Characteristics
The study was designed by referring to a survey paper [
5] reviewing laparoscopic Simulation-Based Training studies, from 1997 to 2011. The hired population were nine engineering students (19 to 28 years old, including 3 men, all right-handed), with no prior knowledge in laparoscopy.
Their skill improvement was assessed during a month on different LapSim tasks. Each participant had ten training sessions, with only four recorded sessions. Each session was conducted as follows: two warming exercises (Camera navigation, Instrument navigation) and three recorded exercises (Coordination, Grasping, Cutting). They are Basic Skills tasks of the LapSim software.
The chosen parameters were the mainly found in the literature, namely task duration, path length (in rotation and translation) and number of movements.
2.3. IGlove Data Processing
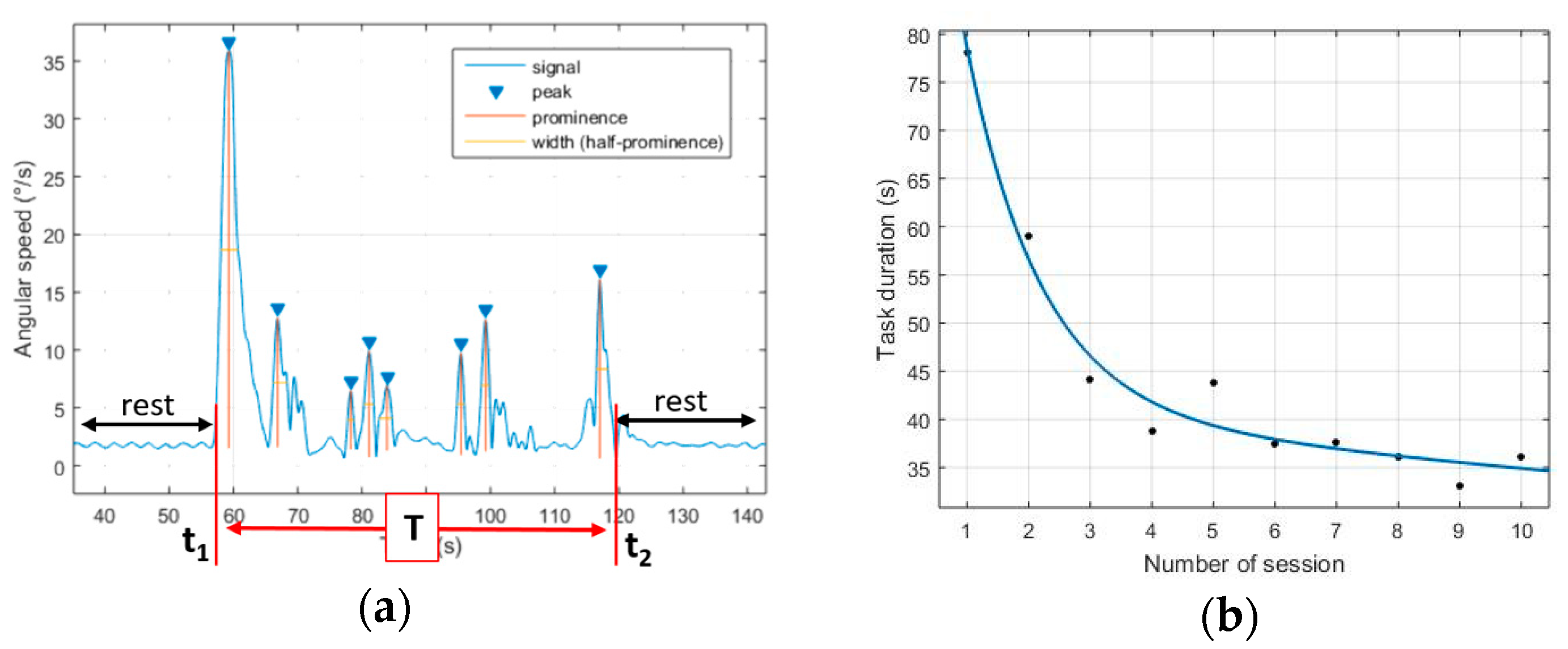
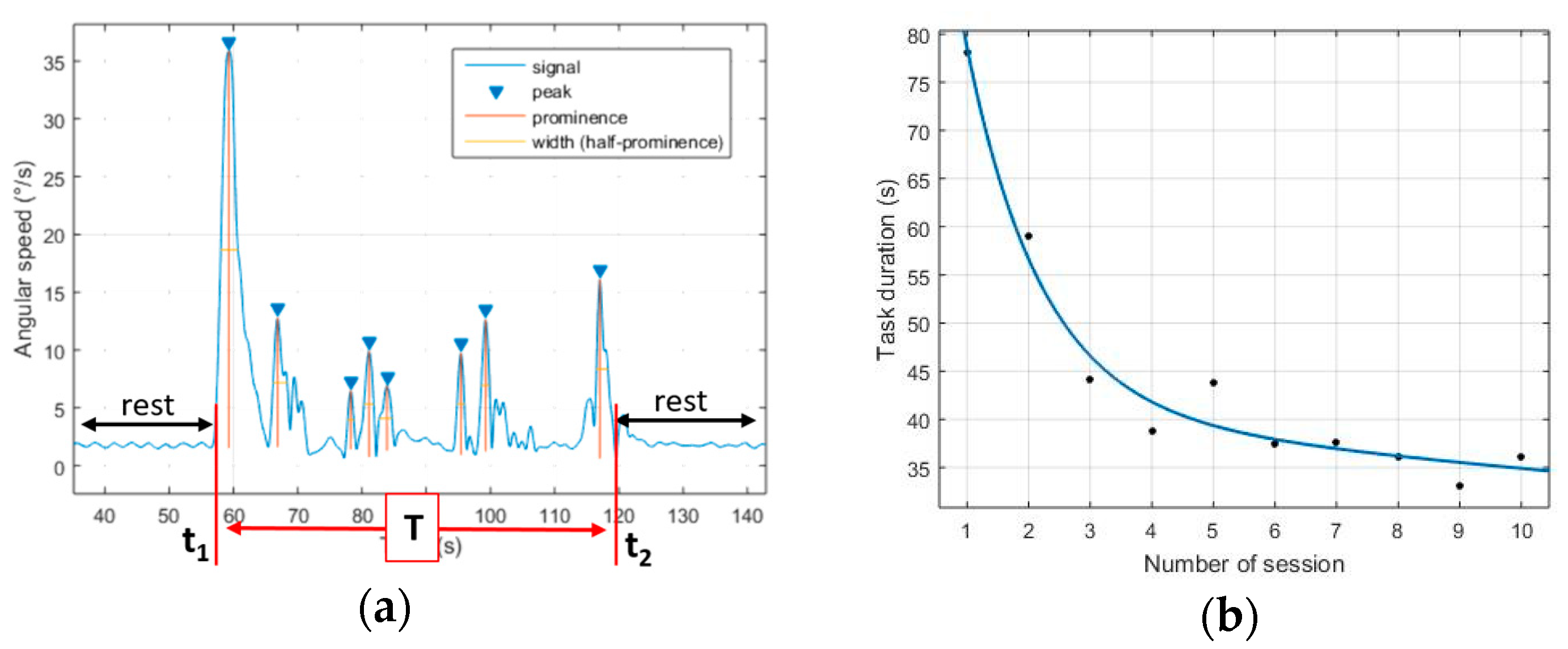
The selected parameters were extracted from the IMU’s thanks to a MATLAB data processing. The mainly used sensor was the gyroscope. A sliding-hanning-window filter was used to smooth the signals (width: 2 s). The task duration (time between first and last movement) was deduced from the number of peaks as described in
Figure 1a. The angular path (path taken by the sensor of the hand, in degrees) was calculated by estimating the integration of the gyroscope signal.
2.4. Validation of the IGlove
The extracted data were compared with two parameters from the LapSim reference data: the task duration and the angular path length. Different analyses can be conducted: to compare the parameters’ value, to compare the parameters’ evolution and to compare the participants’ ranking.
Comparison of the parameters’ value. The parameters’ error
was defined as the average difference between the IGlove values and the LapSim values, for one parameter, such as:
where
is the number of participants,
the number of sessions,
the value of the parameter recorded by the IGlove and
the value of the parameter recorded by the LapSim.
was obtained using only sensor 1. The smaller
is, the closer to the LapSim is the IGlove.
Comparison of the parameters’ evolution. The ratio between the first and the last session of each participant, for the two parameters was calculated. It gives a first idea of how well the IGlove evaluates the total improvement of a parameter, after 10 sessions of repetition.
Another way to assess the evolution of the parameters is to fit them to a known trend line. Then, the trend lines have coefficients that are elements of comparison between the IGlove and the LapSim. A four-parameter decreasing exponential (
Figure 1b) fits best the data (R
2 = 0.9726),
Therefore, to compare the IGlove assessment with the LapSim assessment, the different coefficients A, B, C and D are evaluated and compared for both equipment. The closer to the LapSim it is, the better the IGlove is to assess the participants’ evolution.
Comparison of the participants’ rank. Outcome of each participant is compared to a reference.
For assessing their evolution, this reference is their first session, equal to 1. The ratios between session 1 and session x is displayed at each step of the training. It is a way of evaluating objectively the speed of apprenticeship and the situation of the trainee in his skill acquisition curve. The curves are elements of comparison between the IGlove and the LapSim.
For assessing their best performance, the reference is an experienced surgeon in laparoscopy (8 years of practice) whose outcomes are rated as a 100%. The closer to this score a participant is, the higher it will be in a rank for one given parameter. Those ranks are also elements of comparison.
3. Results
Comparison of the parameters’ value. For the parameter task duration, the estimated error of the IGlove is of 23.5%. For the parameter angular path, the estimated error of the IGlove is of 72.2%.
Comparison of the parameters’ evolution. The ratios between the first and last session of each task for the parameters task duration and angular path are presented in
Table 1. The different modelling parameters A, B, C and D were calculated for the parameters task duration and angular path, and the percentages of difference between the IGlove and the LapSim outcomes were calculated, being the coefficients with the lower differences between IGlove and LapSim the B and D, and the more similar results were obtained in the task Grasping.
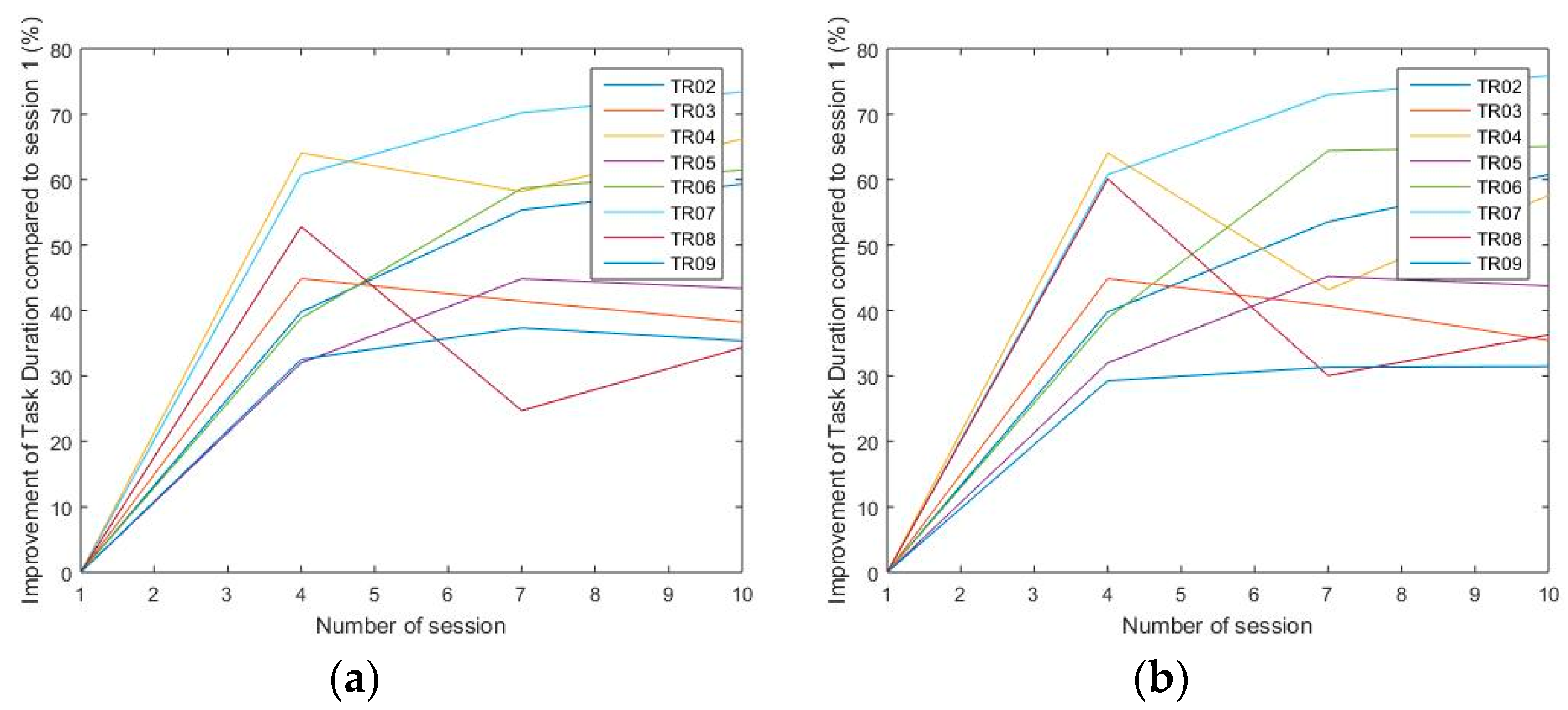
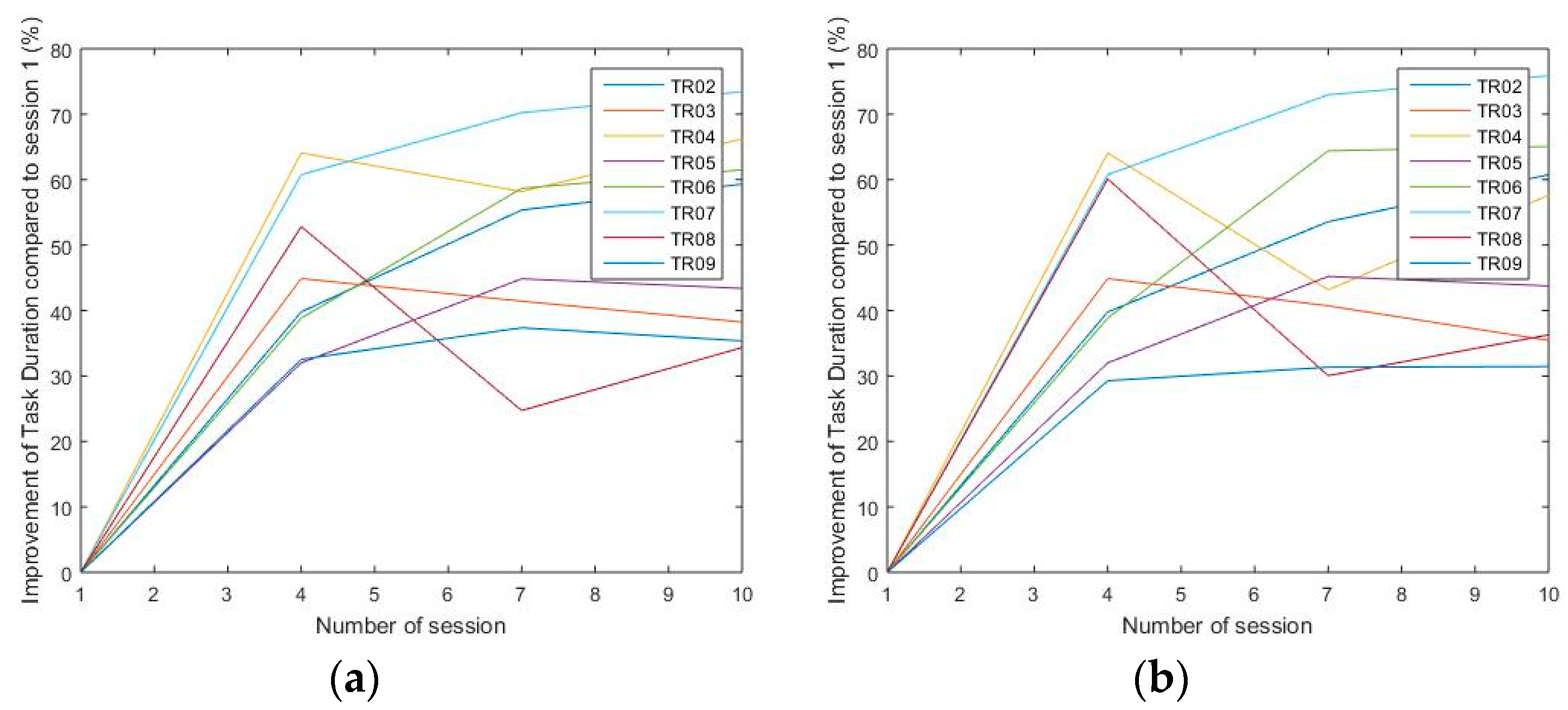
Comparison of the parameters ranking. In
Figure 2 is presented an example of the curves of apprenticeship calculated from the IGlove and the LapSim, for the task
Grasping (participants TR02 to TR09).
Table 2 displays one of the possible ranking of the participants (task
Grasping).
4. Discussion
The selected tasks were basic enough for every participant to achieve a quantifiable improvement. The selected parameters extracted from the IGlove sensors seemed all relevant to show how the participants went towards a more economical gesture. Their absence of knowledge or skills in laparoscopy made their progression clearly identifiable. The IMU sensors give a lot of information, their place on the IGlove has to be well chosen to balance redundant and additional information. Finally, the physical and psychological discomfort has to be taken into account as it appeared the participants felt much more at ease practicing without being observed and measured.
The IGlove outcomes are always higher than the LapSim data. It is because of the movement detection method: it takes into account additional movements that are not parts of the exercise itself, while the LapSim software doesn’t. The comparison of the curves of apprenticeship shows a good correlation, it leads to validate the IGlove as a good equipment to anticipate the dynamic of learning. If the exponential approximation of the apprenticeship curves seems reliable, the comparison of the coefficients shows that it can be improved to have the IGlove and LapSim models match. With regard to the obtained classifications of the trainees, there are mainly consistent between both equipment. A more advanced method of classification could be designed, by weighting certain parameters and determining the number of common points less arbitrarily.
5. Conclusions
As a preliminary study, it appears that the IGlove is able to assess an evolution of dexterity as the LapSim software would do. A model of curve of apprenticeship can be extracted and used to predict the learning dynamics of a trainee. The data process can be improved for more accuracy. Its design can also be reconsidered, as its ergonomics directly influences the outcome of an exercise.
This work shows that the possibilities of utilizing IMU sensors for surgical skills assessment are immense, particularly in those simulators that don’t have haptic parts. The good correlation between IGlove and LapSim suggests possibilities to be used as complementary tools including sophisticated processing techniques in those tasks that include fine movements. It also shows that still a lot of work can be done for discovering all the ways of assessing a surgeon gesture.



{kind=link}
{kind=link}