
Periosteal Dry Needling for Carpometacarpal Osteoarthritis: A Prospective Case Series

 ,
, 
Abstract
1. Introduction
Background
2. Case Description
2.1. Patients
2.2. Treating Clinician
2.3. Evaluation Procedure
2.4. Outcome Measures
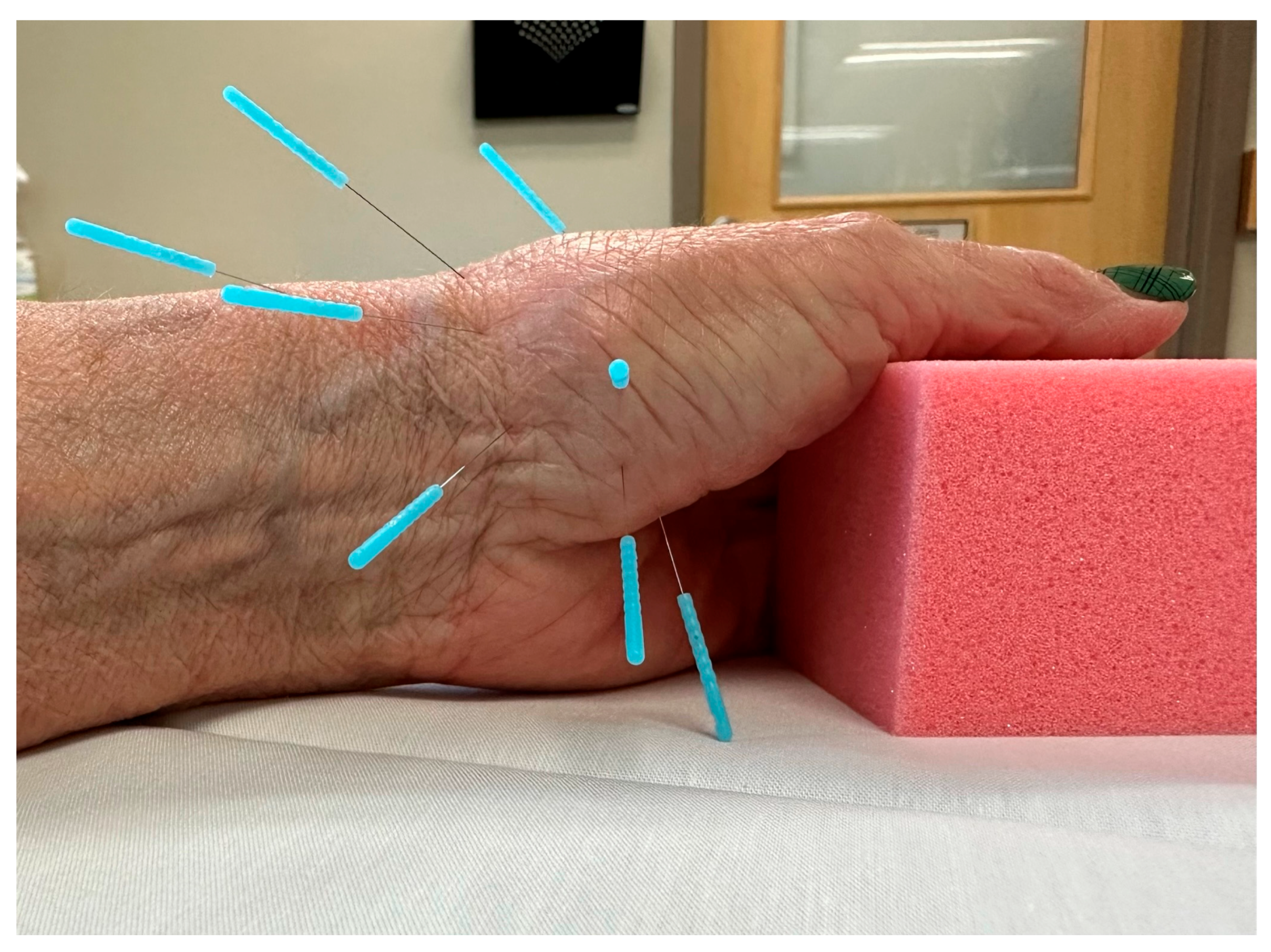
2.5. Intervention
2.6. Treatment Side Effects
2.7. Statistical Analysis
3. Results
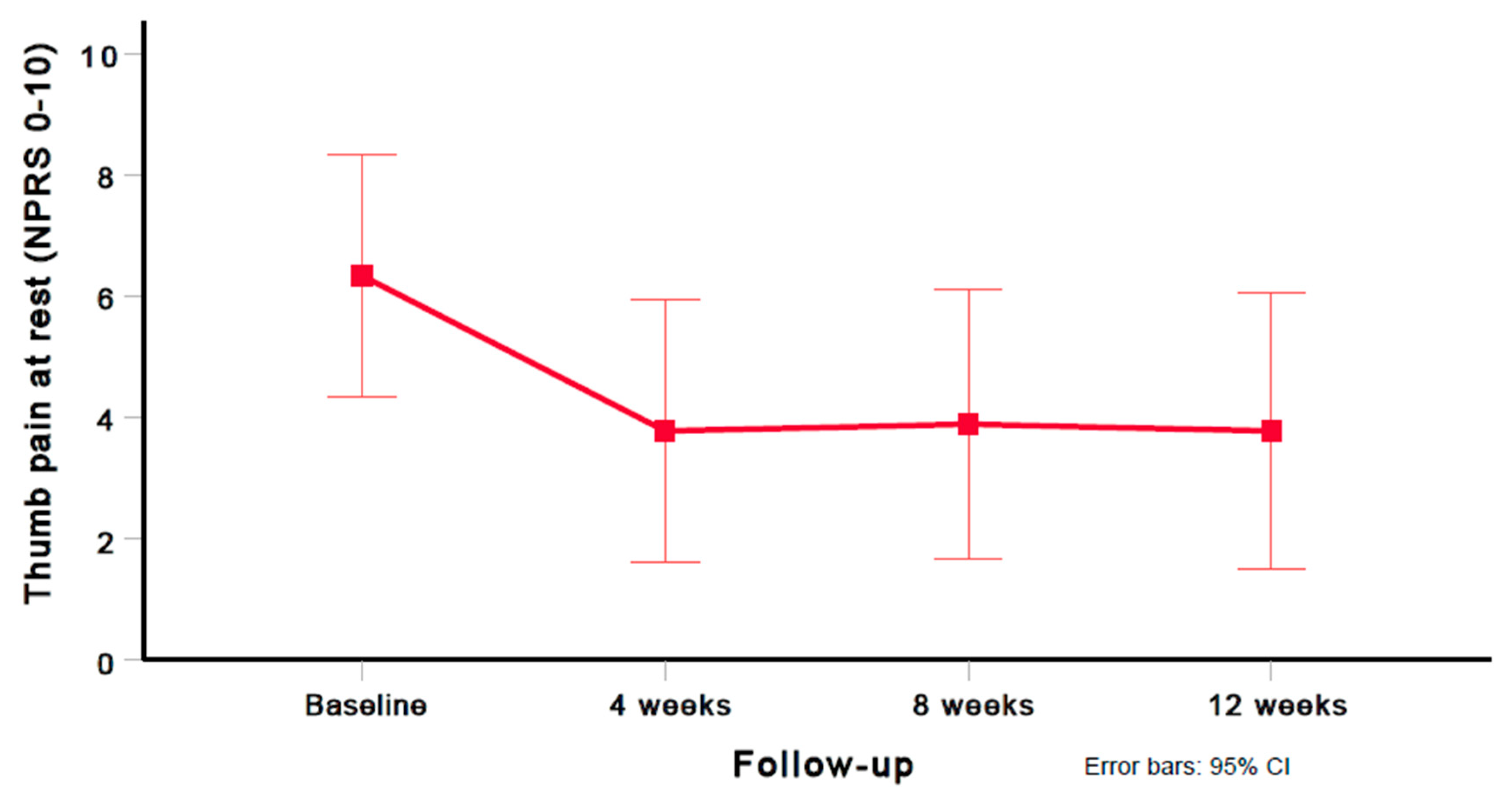
3.1. Thumb Pain (NPRS)
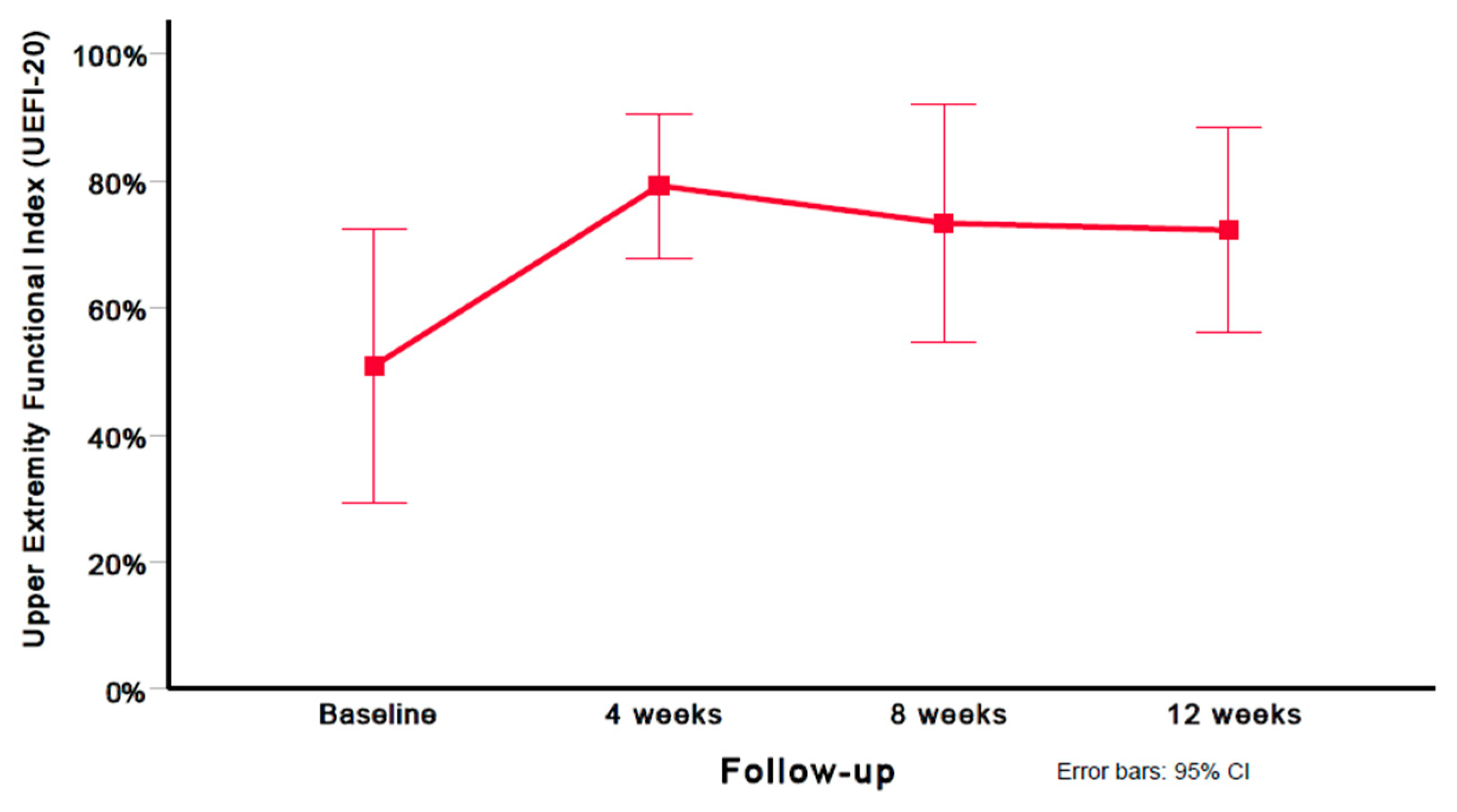
3.2. Upper Extremity Functional Index (UEFI-20)
3.3. Global Rating of Change (GROC)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Higgenbotham, C.; Boyd, A.; Busch, M.; Heaton, D.; Trumble, T. Optimal management of thumb basal joint arthritis: Challenges and solutions. Orthop. Res. Rev. 2017, 9, 93–99. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gillis, J.; Calder, K.; Williams, J. Review of thumb carpometacarpal arthritis classification, treatment and outcomes. Can. J. Plast. Surg. 2011, 19, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Riordan, E.; Robbins, S.; Deveza, L.; Duong, V.; Oo, W.; Wajon, A.; Bennell, K.; Eyles, J.; Jongs, R.; Linklater, J. Radial subluxation in relation to hand strength and radiographic severity in trapeziometacarpal osteoarthritis. Osteoarthr. Cartil. 2018, 26, 1506–1510. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.K.; White, C.P.; Li, Y.K.; White, C.P. Five things to know about...carpometacarpal osteoarthritis of the thumb. Can. Med. Assoc. J. CMAJ 2013, 185, 149. [Google Scholar] [CrossRef]
- Van Heest, A.E.; Kallemeier, P. Thumb carpal metacarpal arthritis. JAAOS-J. Am. Acad. Orthop. Surg. 2008, 16, 140–151. [Google Scholar] [CrossRef]
- Hussain, S.M.; Wang, Y.; Shaw, J.E.; Magliano, D.J.; Wong, T.-Y.; Wluka, A.E.; Graves, S.; Tapp, R.J.; Cicuttini, F.M. Retinal arteriolar narrowing and incidence of knee replacement for osteoarthritis: A prospective cohort study. Osteoarthr. Cartil. 2015, 23, 589–593. [Google Scholar] [CrossRef]
- Findlay, D. Vascular pathology and osteoarthritis. Rheumatology 2007, 46, 1763–1768. [Google Scholar] [CrossRef]
- Kietrys, D.M.; Palombaro, K.M.; Azzaretto, E.; Hubler, R.; Schaller, B.; Schlussel, J.M.; Tucker, M. Effectiveness of dry needling for upper-quarter myofascial pain: A systematic review and meta-analysis. J. Orthop. Sports Phys. Ther. 2013, 43, 620–634. [Google Scholar] [CrossRef]
- Fink, M.; Wipperman, B.; Gehrke, A. Non-specific effects of traditional Chinese acupuncture in osteoarthritis of the hip. Complement. Ther. Med. 2001, 9, 82–89. [Google Scholar] [CrossRef]
- Loaiza, L.A.; Yamaguchi, S.; Ito, M.; Ohshima, N. Electro-acupuncture stimulation to muscle afferents in anesthetized rats modulates the blood flow to the knee joint through autonomic reflexes and nitric oxide. Auton. Neurosci. 2002, 97, 103–109. [Google Scholar] [CrossRef]
- Ahsin, S.; Saleem, S.; Bhatti, A.M.; Iles, R.K.; Aslam, M. Clinical and endocrinological changes after electro-acupuncture treatment in patients with osteoarthritis of the knee. PAIN® 2009, 147, 60–66. [Google Scholar] [CrossRef]
- Haslam, R. A comparison of acupuncture with advice and exercises on the symptomatic treatment of osteoarthritis of the hip—A randomised controlled trial. Acupunct. Med. 2001, 19, 19–26. [Google Scholar] [CrossRef]
- Cagnie, B.; Barbe, T.; De Ridder, E.; Van Oosterwijck, J.; Cools, A.; Danneels, L. The influence of dry needling of the trapezius muscle on muscle blood flow and oxygenation. J. Manip. Physiol. Ther. 2012, 35, 685–691. [Google Scholar] [CrossRef]
- Takeda, W.; Wessel, J. Acupuncture for the treatment of pain of osteoarthritic knees. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1994, 7, 118–122. [Google Scholar] [CrossRef]
- Christensen, B.V.; Iuhl, I.; Vilbek, H.; Bülow, H.H.; Dreijer, N.; Rasmussen, H. Acupuncture treatment of severe knee osteoarthrosis: A long-term study. Acta Anaesthesiol. Scand. 1992, 36, 519–525. [Google Scholar] [CrossRef]
- Williamson, L.; Wyatt, M.; Yein, K.; Melton, J. Severe knee osteoarthritis: A randomized controlled trial of acupuncture, physiotherapy (supervised exercise) and standard management for patients awaiting knee replacement. Rheumatology 2007, 46, 1445–1449. [Google Scholar] [CrossRef]
- Trinh, K.; Zhou, F.; Belski, N.; Deng, J.; Wong, C.Y. The Effect of Acupuncture on Hand and Wrist Pain Intensity, Functional Status, and Quality of Life in Adults: A Systematic Review. Med. Acupunct. 2022, 34, 34–48. [Google Scholar] [CrossRef]
- Manheimer, E.; Cheng, K.; Linde, K.; Lao, L.; Yoo, J.; Wieland, S.; van der Windt, D.A.; Berman, B.M.; Bouter, L.M. Acupuncture for peripheral joint osteoarthritis. Cochrane Database Syst. Rev. 2010, 20, CD001977. [Google Scholar] [CrossRef]
- Lewit, K. The needle effect in the relief of myofascial pain. Pain 1979, 6, 83–90. [Google Scholar] [CrossRef]
- Weiner, D.K.; Moore, C.G.; Morone, N.E.; Lee, E.S.; Kwoh, C.K. Efficacy of periosteal stimulation for chronic pain associated with advanced knee osteoarthritis: A randomized, controlled clinical trial. Clin. Ther. 2013, 35, 1703–1720.e5. [Google Scholar] [CrossRef]
- Mavrommatis, C.I.; Argyra, E.; Vadalouka, A.; Vasilakos, D.G. Acupuncture as an adjunctive therapy to pharmacological treatment in patients with chronic pain due to osteoarthritis of the knee: A 3-armed, randomized, placebo-controlled trial. PAIN® 2012, 153, 1720–1726. [Google Scholar] [CrossRef]
- Ugreja, R.A.; Prem, V. Effectiveness of dry needling techniques in patients with knee osteoarthritis: A systematic review and meta-analysis. J. Bodyw. Mov. Ther. 2021, 27, 328–338. [Google Scholar] [CrossRef]
- McIndoe, A.; Young, K.; Bone, M. A comparison of acupuncture with intra-articular steroid injection as analgesia for osteoarthritis of the hip. Acupunct. Med. 1995, 13, 67–70. [Google Scholar] [CrossRef]
- Zhang, Y.; Bao, F.; Wang, Y.; Wu, Z. Influence of acupuncture in treatment of knee osteoarthritis and cartilage repairing. Am. J. Transl. Res. 2016, 8, 3995–4002. [Google Scholar]
- Liu, X.; Shen, L.; Wu, M.; Wu, B.; Gao, L.; Hu, W.; Zhang, A. Effects of acupuncture on myelogenic osteoclastogenesis and IL-6 mRNA expression. J. Tradit. Chin. Med. Chung I Tsa Chih Ying Wen Pan 2004, 24, 144–148. [Google Scholar]
- Li, Z.-D.; Cao, L.-H.; Wang, S.-C. Effect of moxibustion in treating knee joint osteoarthritis and its relation with contents of hyaluronic acid in serum and synovial fluid. Zhongguo Zhong Xi Yi Jie He Za Zhi Zhongguo Zhongxiyi Jiehe Zazhi Chin. J. Integr. Tradit. West. Med. 2009, 29, 883–885. [Google Scholar]
- Huang, J.; Zhuo, L.-S.; Wang, Y.-Y.; Peng, Z.-L.; Huang, Y.-R.; Wang, Y.; Yang, L. Effects of electroacupuncture on synovia IL-1beta and TNF-alpha contents in the rabbit with knee osteoarthritis. Zhen Ci Yan Jiu Acupunct. Res. 2007, 32, 115–118. [Google Scholar]
- Cao, S.; Wang, C.; Ma, X.; Wang, X.; Huang, J.; Zhang, C. Imaging diagnosis for chronic lateral ankle ligament injury: A systemic review with meta-analysis. J. Orthop. Surg. Res. 2018, 13, 122. [Google Scholar] [CrossRef]
- Dunning, J.; Butts, R.; Young, I.; Mourad, F.; Galante, V.; Bliton, P.; Tanner, M.; Fernandez-de-Las-Penas, C. Periosteal Electrical Dry Needling as an Adjunct to Exercise and Manual Therapy for Knee Osteoarthritis: A Multicenter Randomized Clinical Trial. Clin. J. Pain. 2018, 34, 1149–1158. [Google Scholar] [CrossRef]
- Barnard, A.; Jansen, V.; Swindells, M.G.; Arundell, M.; Burke, F.D. A randomized controlled trial of real versus sham acupuncture for basal thumb joint arthritis. J. Hand Surg. Eur. Vol. 2020, 45, 488–494. [Google Scholar] [CrossRef]
- Voss, M.R.; Donnay, R.L.; Homa, J.K. The effects of dry needling on the thumb: A case report. Hong Kong J. Occup. Ther. 2021, 34, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Villafañe, J.H.; Valdes, K.; Pedersini, P.; Berjano, P. Thumb carpometacarpal osteoarthritis: A musculoskeletal physiotherapy perspective. J. Bodyw. Mov. Ther. 2019, 23, 908–912. [Google Scholar] [CrossRef]
- Shridhar, V.; Williams, S. Basal thumb arthritis: Treatment strategies for managing pain. Aust. J. Gen. Pract. 2020, 49, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D. The CARE guidelines: Consensus-based clinical case reporting guideline development. Glob. Adv. Health Med. 2013, 2, 38–43. [Google Scholar] [CrossRef]
- Merritt, M.M.; Roddey, T.S.; Costello, C.; Olson, S. Diagnostic value of clinical grind test for carpometacarpal osteoarthritis of the thumb. J. Hand Ther. 2010, 23, 261–268. [Google Scholar] [CrossRef]
- Jensen, G.M.; Hack, L.M.; Nordstrom, T.; Gwyer, J.; Mostrom, E. National Study of Excellence and Innovation in Physical Therapist Education: Part 2—A Call to Reform. Phys. Ther. 2017, 97, 875–888. [Google Scholar] [CrossRef] [PubMed]
- Choa, R.; Parvizi, N.; Giele, H. A prospective case-control study to compare the sensitivity and specificity of the grind and traction-shift (subluxation-relocation) clinical tests in osteoarthritis of the thumb carpometacarpal joint. J. Hand Surg. Eur. Vol. 2014, 39, 282–285. [Google Scholar] [CrossRef]
- Jensen, M.P.; Karoly, P.; Braver, S. The measurement of clinical pain intensity: A comparison of six methods. Pain 1986, 27, 117–126. [Google Scholar] [CrossRef]
- Cleland, J.A.; Childs, J.D.; Whitman, J.M. Psychometric Properties of the Neck Disability Index and Numeric Pain Rating Scale in Patients with Mechanical Neck Pain. Arch. Phys. Med. Rehabil. 2008, 89, 69–74. [Google Scholar] [CrossRef]
- Young, I.A.; Cleland, J.A.; Michener, L.A.; Brown, C. Reliability, construct validity, and responsiveness of the neck disability index, patient-specific functional scale, and numeric pain rating scale in patients with cervical radiculopathy. Am. J. Phys. Med. Rehabil. 2010, 89, 831–839. [Google Scholar] [CrossRef]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, M.R. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Salaffi, F.; Stancati, A.; Silvestri, C.A.; Ciapetti, A.; Grassi, W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur. J. Pain 2004, 8, 283–291. [Google Scholar] [CrossRef]
- Chesworth, B.M.; Hamilton, C.B.; Walton, D.M.; Benoit, M.; Blake, T.A.; Bredy, H.; Burns, C.; Chan, L.; Frey, E.; Gillies, G. Reliability and validity of two versions of the upper extremity functional index. Physiother. Can. 2014, 66, 243–253. [Google Scholar] [CrossRef]
- Hamilton, C.B.; Chesworth, B.M. A Rasch-validated version of the upper extremity functional index for interval-level measurement of upper extremity function. Phys. Ther. 2013, 93, 1507–1519. [Google Scholar] [CrossRef]
- Jaeschke, R.; Singer, J.; Guyatt, G.H. Measurement of health status. Ascertaining the minimal clinically important difference. Control. Clin. Trials 1989, 10, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Dunning, J.; Butts, R.; Mourad, F.; Young, I.; Flannagan, S.; Perreault, T. Dry needling: A literature review with implications for clinical practice guidelines. Phys. Ther. Rev. 2014, 19, 252–265. [Google Scholar] [CrossRef] [PubMed]
- Carlesso, L.C. Standardization of adverse event terminology and reporting in orthopaedic physical therapy: Application to the cervical spine. J. Orthop. Sports Phys. Ther. 2010, 40, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Dickens, W.; Lewith, G.T. A single-blind, controlled and randomised clinical trial to evaluate the effect of acupuncture in the treatment of trapezio-metacarpal osteoarthirits. Complement. Med. Res. 1989, 3, 5–8. [Google Scholar]
- Weiner, D.K.; Rudy, T.E.; Morone, N.; Glick, R.; Kwoh, C.K. Efficacy of periosteal stimulation therapy for the treatment of osteoarthritis-associated chronic knee pain: An initial controlled clinical trial. J. Am. Geriatr. Soc. 2007, 55, 1541–1547. [Google Scholar] [CrossRef]
- McCarney, R.; Warner, J.; Iliffe, S.; van Haselen, R.; Griffin, M.; Fisher, P. The Hawthorne Effect: A randomised, controlled trial. BMC Med. Res. Methodol. 2007, 7, 30. [Google Scholar] [CrossRef]
- Kinney, M.; Seider, J.; Beaty, A.F.; Coughlin, K.; Dyal, M.; Clewley, D. The impact of therapeutic alliance in physical therapy for chronic musculoskeletal pain: A systematic review of the literature. Physiother. Theory Pract. 2020, 36, 886–898. [Google Scholar] [CrossRef] [PubMed]
- Rodeghero, J.; Wang, Y.-C.; Flynn, T.; Cleland, J.A.; Wainner, R.S.; Whitman, J.M. The impact of physical therapy residency or fellowship education on clinical outcomes for patients with musculoskeletal conditions. J. Orthop. Sports Phys. Ther. 2015, 45, 86–96. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Baseline Variable | Patients with CMC OA (n = 9) |
|---|---|
| Age (y) | 60.9 (7.7) |
| Sex: female, n (%) | 9 (100%) |
| Duration of symptoms (months) | 29.3 (20.9) |
| BMI (kg/m2) | 32.8 (10.9) |
| NPRS (0–10) | 6.3 (2.6) |
| UEFS (0–100%) | 50.9 (28.1) |
| Points | Anatomical Target Tissue | Location | Needle Angulation |
|---|---|---|---|
| Point 1 | Adductor pollicis | From a dorsal approach, needle through the first web space, staying close to the border of the first metacarpal | P to A slightly ulnar |
| Point 2 | Opponens pollicis; abductor pollicis brevis; recurrent branch of median nerve; base of CMC | Radial side of first metacarpal, within the proximal third of thenar eminence, close to the first metacarpal. Pass through the abductor pollicis brevis muscle and toward the bone into the opponens pollicis, which lies against the first metacarpal | Needle inserted A to P, angle toward base of CMC |
| Point 3 | Abductor pollicis brevis; base of CMC | Within the proximal third of the thenar eminence, one finger width medial to point 2 | Needle inserted A to P, angle toward base of CMC |
| Point 4 | Recurrent branch of median nerve; flexor pollicis brevis; base of CMC | Within the proximal third of the thenar eminence, one finger width medial to point 3 | Needle inserted A to P, angle toward base of CMC |
| Point 5 | Joint capsule of CMC; Superficial radial nerve | Within the anatomical snuff box between the tendons of EPL and EPB | Angle toward CMC joint |
| Point 6 | Capsule of the CMC joint; Superficial radial nerve | At the wrist crease on the radial side of the radial artery, under the APL tendon | Slide under the APL tendon |
| Point 7 | Superficial radial nerve; within tendon sheath of APL and EPB | Two finger widths proximal to the center of the anatomical snuff box, just proximal to radial aspect of styloid process of radius between and parallel to tendons of APL and EPB muscles | Tangential insertion by gripping and lifting the tissue; squeeze in using free insertion |
| Point 8 | Palmar aspect of first trapezio-metacarpal joint; median nerve | One finger width distal to the flexion wrist crease on the radial and palmar side at the base of the CMC joint | Perpendicular toward CMC joint |
| Variable | Preintervention | 4 Weeks | 8 Weeks | 12 Weeks |
|---|---|---|---|---|
| NPRS (0–10) | 6.3 (2.6) | 3.8 (2.8) | 3.9 (2.9) | 3.8 (2.9) |
| UEFS-20 (0–100%) | 50.9 (28.0) | 79.2 (14.8) | 73.3 (24.5) | 72.2 (21.1) |
| GROC (−7 to +7) | NA | 4.0 (2.1) | 2.4 (3.0) | 2.2 (2.9) |
| NPRS | Preintervention | 4 Weeks | 8 Weeks | 12 Weeks |
|---|---|---|---|---|
| Subject 1 | 4 | 4 | 3 | 3 |
| Subject 2 | 10 | 10 | 10 | 10 |
| Subject 3 | 6 | 5 | 6 | 6 |
| Subject 4 | 10 | 2 | 4 | 3 |
| Subject 5 | 7 | 3 | 2 | 3 |
| Subject 6 | 8 | 2 | 2 | 1 |
| Subject 7 | 3 | 0 | 0 | 0 |
| Subject 8 | 4 | 3 | 3 | 3 |
| Subject 9 | 5 | 5 | 5 | 5 |
| UEFI-20 | Preintervention | 4 Weeks | 8 Weeks | 12 Weeks |
|---|---|---|---|---|
| Subject 1 | 36 | 57 | 84 | 76 |
| Subject 2 | 64 | 64 | 64 | 64 |
| Subject 3 | 18 | 68 | 31 | 31 |
| Subject 4 | 20 | 92 | 36 | 50 |
| Subject 5 | 37 | 89 | 84 | 70 |
| Subject 6 | 31 | 68 | 85 | 88 |
| Subject 7 | 82 | 95 | 100 | 95 |
| Subject 8 | 84 | 94 | 90 | 90 |
| Subject 9 | 86 | 86 | 86 | 86 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staehli Wiser, A.; Dunning, J.; Charlebois, C.; Bliton, P.; Mourad, F. Periosteal Dry Needling for Carpometacarpal Osteoarthritis: A Prospective Case Series. J. Clin. Med. 2023, 12, 5678. https://doi.org/10.3390/jcm12175678
Staehli Wiser A, Dunning J, Charlebois C, Bliton P, Mourad F. Periosteal Dry Needling for Carpometacarpal Osteoarthritis: A Prospective Case Series. Journal of Clinical Medicine. 2023; 12(17):5678. https://doi.org/10.3390/jcm12175678
Chicago/Turabian StyleStaehli Wiser, Anna, James Dunning, Casey Charlebois, Paul Bliton, and Firas Mourad. 2023. "Periosteal Dry Needling for Carpometacarpal Osteoarthritis: A Prospective Case Series" Journal of Clinical Medicine 12, no. 17: 5678. https://doi.org/10.3390/jcm12175678
APA StyleStaehli Wiser, A., Dunning, J., Charlebois, C., Bliton, P., & Mourad, F. (2023). Periosteal Dry Needling for Carpometacarpal Osteoarthritis: A Prospective Case Series. Journal of Clinical Medicine, 12(17), 5678. https://doi.org/10.3390/jcm12175678