
Epidemiological Differences in Hajj-Acquired Airborne Infections in Pilgrims Arriving from Low and Middle-Income versus High-Income Countries: A Systematised Review

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
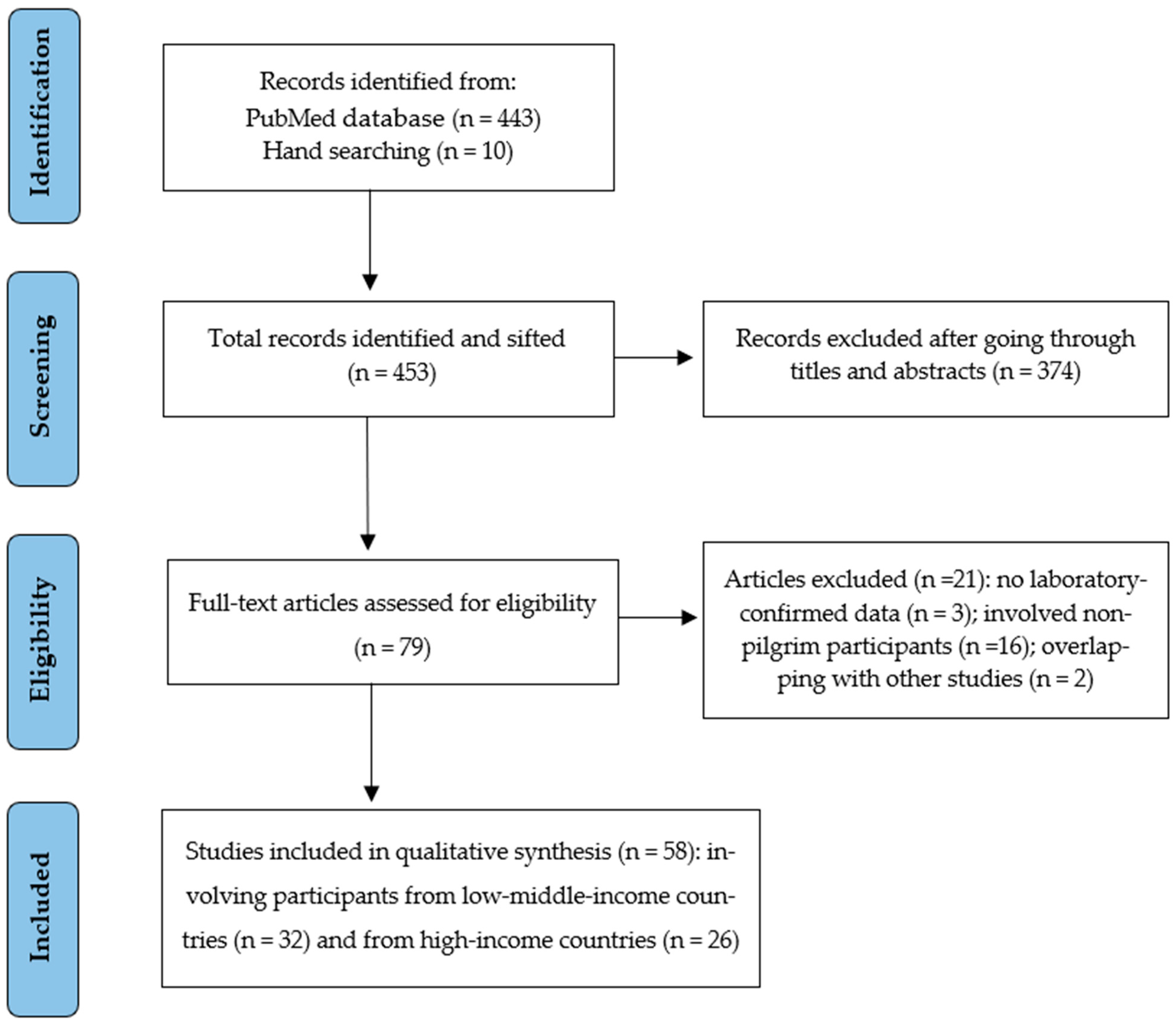
2.1. Search Strategy and Study Selection
2.2. Data Extraction and Synthesis
3. Results
3.1. General Description of Included Studies and Quality Assessment

{kind=link}
| Author, Publication Year | Study Year | Participants’ Nationalities (%) | Selection Method/Case Ascertainment | Testing Method | Sample Size | Mean/Median Age (Range) | Male: Female | Risk Factors (%) | Vaccine Uptake (%) | Detected Diseases Name | Disease Burden n (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| AlBarrak et al., 2018 [13] | 2016 | Majority from LMIC: Indonesian (22.3) Egyptian (10.2) Indian (9.8) | Adults with radiologically confirmed pneumonia admitted in general hospitals in Makkah and Al Madinah | Urine antigen test was used in addition to culture-based methods | 266 | 65.3 (30–90) | 2:1 | Diabetes (36) | NR | Community-acquired pneumonia | S. pneumoniae 48 (18) |
| Alborzi et al., 2009 [41] | 2006–2007 | Iranian | Pilgrims with symptoms of ARI at Shiraz airport on return from the Hajj | Direct fluorescent staining and viral culture were performed on nasal wash specimens. Rhinovirus and enterovirus tested by RT-PCR | 255 | 52.4 (19–82) | 1:1.1 | NR | Influenza vaccine (85.5) | Viral respiratory infections | Influenza 25 (9.8) Rhinovirus 15 (5.9) Other viruses 42 (16.4) |
| Alsayed et al., 2021 [14] | 2019 | Asian (64) African (30.3) European (2.7) North American (2.2) Oceanian (0.5) | Pilgrims with severe ARI symptoms who were initially hospitalised at seven healthcare facilities in Makkah, Arafat, and Mina at Hajj | Nasopharyngeal swabs were collected and tested using multiplex RT-PCR | 185 | 58 (2 d–88 y) | 1.9:1 | NR | NR | Viral respiratory infections | Rhinovirus 53 (42) Influenza 54 (29.2) Coronaviruses 35 (18.9) Other viruses 19 (10.2) MERS-CoV 0 (0) |
| Alzeer et al., 1998 [32] | 1994 | Middle Eastern (34) South-East Asian (31) Indian (23) African (11) | All pilgrims admitted with pneumonia to Al-Noor Specialist Hospital and King Abdulaziz Hospital, Makkah | Sputum samples or fibre optic bronchoscopy samples for microscopy and culture, blood chemistry | 64 | 63 | 2.6:1 | NR | NR | Pneumonia | Viruses: Influenza 3 (4.7) Parainfluenza 1 (1.6) Bacteria: M. tuberculosis 13 (20.3) S. pneumoniae 6 (9.4) K. pneumoniae 5 (7.8) H. influenzae 3 (4.7) S. aureus 2 (3.1) Other bacteria 11 (17.3) |
| Annan et al., 2015 [42] | 2013 | Ghanaian | Adult pilgrims at the Kotoka International Airport after Hajj | Nasopharyngeal specimens were tested by RT-PCR | 839 | 52 (21–85) | 1:1.2 | NR | NR | Viral respiratory infections | Rhinovirus 141 (16.8) RSV 43 (5.1) Influenza viruses 11 (1.3) MERS-CoV 0 (0) |
| Asghar et al., 2011 [15] | 2005 | Indonesian (18.4) Saudi (17.1) Pakistani (11.8) Indian (9.2) Egyptian (6.6) Malaysian (5.3) Syrian (4) Others (27.6) | Hajj pilgrims with suspected pneumonia who were admitted to hospitals in Makkah | Sputum samples were tested by routine culture, acid fast bacilli examination, and culture | 141 | >94% of cases were >50 y | 1.3:1 | Diabetes (55) | NR | Pneumonia | M. tuberculosis 1 (0.7) S. pneumoniae 5 (3.5) K. pneumoniae 8 (5.7) S. aureus 7 (5) Others 70 (50) |
| Ashshi et al., 2014 [36] | 2010 | 280 Indonesian 157 Algerian 188 Indian 101 Syrian 128 Ivorian 104 Sierra Leonean 113 Somalian 123 Nigerian 112 Turkish 89 Australian 99 American 97 British | Pilgrims entering Saudi Arabia via King Abdulaziz International Airport, Jeddah city | Throat swab analysed using RT-PCR | 1600 | 1309 aged > 40 291 aged ≤ 40 | 1.6:1 | NR | Influenza vaccine (93.4) | Influenza A | Influenza A 120 (7.5) |
| Baharoon et al., 2009 [16] | 2004 | Majority were South Asian | All pilgrims admitted with severe sepsis and septic shock among Hajj pilgrims in two major ICUs in Makkah: King Faisal and King Abdulaziz Hospitals | Clinical diagnosis of severe sepsis/septic shock. Confirmation of source of infection with X-ray and/or positive culture | 42 | 65.4 | 1.8:1 | Lung diseases (71) Hypertension/Cardiac (43) Diabetes (29) Kidney diseases (2) | NR | Bacterial sepsis | Community-acquired pneumonia 23 (54.8) |
| Bokhary et al., 2022 [17] | 2018 | Egyptian (22.3) Sudanese (14.9) Algerian (11.6) Moroccan (9.1) Libyan (2.6) Saudi (14.9) Indian (7.4) Pakistani (6.6) | Adult pilgrims who sought medical care for upper RTIs during Hajj | Oropharyngeal swabs were taken and tested by bacteriological culture method and automated VITEK 2 COMPACT system | 121 | 45 | 8.3:1 | NR | NR | Bacterial respiratory infections | H. influenzae 6 (4.9) S. pneumoniae 2 (1.6) S. aureus 1 (0.8) Others 1 (0.8) |
| El-Gamal et al., 1988 [19] | 1987 | Pakistani, Indian and Indonesian (50) | Suspected cases of meningitis were presented to the outpatient clinic at King Abdulaziz Hospital in Al Madinah city | CSF, blood and skin samples were examined. CSF samples were examined under microscope and by latex test | 229 | (30–70) | 2.3:1 | NR | NR | Meningococcal | Meningitis 188 (82) (177 serogroup A and 11 serogroup C) |
| El-Kafrawy et al., 2022 [20] | 2019 | 15 Indonesian 9 Indian 4 Moroccan 3 Somalian and Sudanese (each) 2 Saudi, Bangladeshi, and Nigerian (each) 13 others | Pilgrims with RTIs who presented to the healthcare facilities at Hajj sites in Makkah | Nasopharyngeal swabs were collected and tested by multiplex RT-PCR | 53 | Majority (58%) >60 years old | NR | NR | NR | Human rhinoviruses | Rhinoviruses 19 (36.8) |
| El-Sheikh et al., 1998 [21] | 1991–1992 | 30 different nationalities | Pilgrims who were referred to either Ajyad hospital or three dispensaries in Jeddah. Upon enrolment, all patients were diagnosed with upper or lower RTIs | Sputa were collected and examined microscopically. Throat swabs were collected for cell culture and virus identification by immunofluorescence | 1156 | (10–80) | NR | NR | NR | Viral and bacterial respiratory infections | Viruses: RSV 18 (2.4) Influenza 49 (6.4) Parainfluenza virus 45 (5.9) Adenovirus 36 (4.7) Bacteria: H. influenzae 42 (10.6) K. pneumoniae 31 (7.8) S. pneumoniae 27 (6.8) S. pyogenes 7 (2.4) S. aureus 11 (3.8) |
| Hashem et al., 2019 [22] | 2014 | Majority Indian and Indonesian | During the 5 days of Hajj, samples were collected from all pilgrims presenting with ARI symptoms and suspected of MERS-CoV infection at seven healthcare facilities in Makkah, Mina, and Arafat | Nasopharyngeal samples were collected and tested using RT-PCR and microarray | 132 | 61.85 (26–95) | 2:1 | NR | NR | Viral respiratory infections | Influenza 39 (29.5) Rhinoviruses 17 (12.1) Coronaviruses 24 (18.2) Other viruses 18 (13.6) MERS-CoV 0 (0) |
| Harimurti et al., 2021 [54] | 2015 | Indonesian | A multi-site longitudinal study collected data before the departure from Indonesia, and immediately upon arrival | Nasopharyngeal samples were collected pre- and post-Hajj and tested by culturing onto blood agar | 813 | 53.1 | 1:1 | Lung disease (2) Cardiovascular disease (0.8) Liver disease (0.2) Diabetes (5.8) | Pneumococcal vaccine (2) | Pneumococcal infection | S. pneumoniae (8.2) |
| Kandeel et al., 2011 [43] | 2009 | Egyptian | Random selection of pilgrims who returned by ship to Port Tawfiq. Non-random selection of returning pilgrims at Cairo International airport | Throat swabs analysed by RT-PCR | 551 | (12–65) | 1.3:1 | NR | Influenza vaccination (98) | Viral respiratory infections | Influenza A/H3N2 6 (1) |
| Karima et al., 2003 [23] | 2000 | Majority Pakistani (18) Indian (15) Indonesian (12) | All suspected and microbiologically confirmed cases of meningococcal disease referred to public and private hospitals and health centres in Makkah | CSF examination: Gram stain smears, latex agglutination and culture | 105 | 23% (61–70) 22% (41–50) | 1.9:1 | fourteen diabetes one ischemic heart disease one renal failure three hypertension | NR | Meningococcal | Meningitis A, B, W 67 (64) |
| Koul et al., 2018 [44] | 2014–2015 | Indian | Pilgrims were interviewed for respiratory symptoms and tested for respiratory viruses in Srinagar International Airport, Jammu and Kashmir, India | Nasopharyngeal and throat swabs tested by RT-PCR | 300 | 60 (26–60) | 1:1.1 | NR | Influenza vaccine (72) | Viral respiratory infections | Influenza 33 (11) Coronaviruses 52 (17.3) Rhinovirus 20 (6) Other viruses 20 (6) MERS-CoV 0 (0) |
| Lingappa et al., 2003 [24] | 2000 | African (35) Asian (42) Southwest Asian (26) European (4) Middle Eastern (19) | Case data from Ministry of Health surveillance records, regional health directories, clinical laboratory records and inpatient charts from all hospitals in Makkah, Al Madinah and Jeddah | Blood and CSF culture, latex agglutination of CSF | 253 | 40 (0.2–80) | 1.1:1 | NR | NR | Meningococcal | 253 confirmed cases among approx. 1.7 million pilgrims (0.015). Serogroups W 93 (37), A 60 (24), B 4 (2), C 4 (2) |
| Mandourah et al., 2012 [25] | 2009–2010 | Over 40 nationalities | All patients admitted to 15 hospitals in Makkah and Al Madinah | Sputum culture and blood culture | 452 | 64 | 1.8:1 | Diabetes (32.5) Lung diseases (17.1) | NR | Pneumonia | S. pneumoniae 3 (0.7) K. pneumoniae 5 (1.1) S. aureus 3 (0.7) Other bacteria 21 (4.6) |
| Mandourah et al., 2012 [26] | 2009 | East Asian (29.1) South Asian (24.6) Arab (30.9) Black (12.7) White (2.7) | All pilgrims admitted to ICUs of four key hospitals in Makkah | Nasal-swab specimens were tested by RT-PCR | 110 | 60.5 | 1.7:1 | Cardiovascular disease (28.2) Lung disease (20.9) Liver disease (6.4) Diabetes (28.2) Hypertension (31.8) | NR | Viral and bacterial respiratory infections | Influenza A/H1N1 * 24 (21.8) Community- acquired pneumonia 21 (19.3) Tuberculosis 1 (0.9) |
| Memish et al., 2012 [37] | 2009 | Middle Eastern (63) Asian or African (37) | On arrival of pilgrims just before Hajj, and before departure after Hajj at King Abdulaziz International Airport, Jeddah | Nasopharyngeal and throat swabs tested by xTAG Respiratory Viral Panel FAST assay. Specimens positive for influenza A but negative for seasonal H1 and H3 were subjected to additional PCR amplification to detect pandemic H1 and avian H5 | 3550 | 49.4 | 1.4:1 | NR | Influenza vaccine (53.3) | Viral respiratory infections | Influenza 11 (0.5) RSV 8 (0.3) Coronaviruses 10 (0.4) Entero-rhinovirus 351 (13) Other viruses 14 (0.7) |
| Memish et al., 2014 [38] | 2013 | Majority from Indonesia (32.4) Pakistan (18.9) India (10.8) | All pilgrims admitted to 15 healthcare facilities in Makkah and Al Madinah, who were diagnosed with pneumonia | Sputum samples screened for MERS-CoV by RT-PCR and respiratory multiplex array was used to detect up to 22 other viral and bacterial respiratory pathogens | 38 | 58.6 (25–83) | 2.2:1 | NR | NR | Viral and Bacterial respiratory infections | Viruses: Influenza 6 (15.8) Rhinoviruses 15 (39.5) Coronaviruses 5 (13.3) Others 2 (5.2) MERS-CoV 0 (0) Bacteria: S. pneumoniae 13 (34.2) H. influenzae 5 (13.2) Others 10 (26.3) |
| Memish et al., 2014 [39] | 2013 | Majority Indian (17.1) Indonesian (12.9) Pakistani (11.9) Turkish (10.7) | A random selection at the Hajj terminal of King Abdulaziz International Airport, Jeddah, of arriving and departing pilgrims | Nasal swabs analysed by RT-PCR | 5235 | 51.8 (18–93) | 1.2:1 | Diabetes (6.8), Hypertension (13.1) | Influenza vaccine (22), pneumococcal vaccine (4.4) | MERS-CoV | MERS-CoV 0 (0) |
| Memish et al., 2015 [66] | 2013 | African (44.2) Asian (40.2) American (8.4) European (7.2) | Pilgrims recruited upon entering Saudi Arabia at Jeddah International Airport and at Mina camps before leaving Saudi Arabia | Nasal swabs analysed by RT-PCR | 1206 | 50 (18–88) | 1.9:1 | NR | Influenza vaccine (21.9) Pneumococcal vaccine (1.2) | Viral and Bacterial respiratory infections | Viruses: Influenza (3.6) Rhinovirus (34.4) Coronaviruses (19.5) Others (2.4) Bacteria: Meningococcal (0.3) S. pneumoniae (12.7) K. pneumoniae (3.9) S. aureus (7.9) H. influenzae (11.7) |
| Moattari et al., 2012 [46] | 2009 | Iranian | Symptomatic Iranian pilgrims who arrived at Shiraz Airport Iran from Hajj | Throat swabs were collected and tested by virus culture and RT-PCR | 275 | 46 (20–70) | 1:1 | NR | Influenza vaccine (100) | Influenza viruses | Influenza A/H3N2 8 (2.9) Influenza A/H1N1 5 (1.8) Influenza B 20 (7.3) |
| Muraduzzaman et al., 2018 [47] | 2013–2016 | Bangladeshi | Pilgrims and other people returning from the Middle East presented with respiratory symptoms were recruited via active screening at the point of entry | Nasal and throat swabs and sputum tested by RT-PCR | 81 | 49 (14 m–81 y) | 1.2:1 | NR | NR | Viral respiratory infections | Influenza viruses 18 (22.2) Other viruses 6 (7.4) MERS-CoV 0 (0) |
| Refaey et al., 2017 [51] | 2012–2015 | Egyptian | A convenience sample of about 10% of pilgrims from each flight who returned at Cairo International Airport from Hajj | Nasopharyngeal swabs were collected from all participants while sputum specimens collected only from those with respiratory symptoms. Specimens were tested by RT-PCR | 3364 | 56 (0–105) | (1:1.1) | NR | Influenza vaccine (19.7) | Viral respiratory infections | All influenza viruses 484 (14.4) Influenza A/H1N1 117 (3.5) Influenza A/H3N2 187 (5.6) Influenza B 180 (5.4) MERS-CoV 0 (0) |
| Shirah et al., 2017 [30] | 2004–2013 | African (43.9) Asian (51.2) European (3.3) North African (0.7) South American (0.47) Oceanian (0.47) | Clinical data of pilgrims with confirmed pneumonia who attended emergency department of a general hospital in Al Madinah during Hajj | Chest X-ray, throat and nose swabs, sputum and blood culture | 1059 | 56.8 (48–64) | 2.9:1 | Lung disease (15) Diabetes (34.8) Cardiovascular disease (23.3) | NR | Pneumonia | K. pneumoniae 307 (29) S. pneumoniae 1 (1) S. aureus 382 (36) H. influenzae 257 (24) Other bacteria 102 (10) |
| Yavarian et al., 2018 [52] | 2013–2016 | Iranian | Specimens were taken from arriving pilgrims at Emam Khomeini Airport in Tehran | Throat swabs were collected and tested by using one-step RT-PCR | 3840 | NR | NR | NR | NR | Influenza viruses | All influenza viruses 499 (13) Influenza A/H1N1 258 (51.7) Influenza A/H3N2 100 (20) Influenza B 135 (27) MERS-CoV 0 (0) |
| Yezli et al., 2017 [35] | 2015 | Afghan (27.1) Pakistani (25.9) Bangladeshi (19.1) Nigerian (15.1) South African (12.7) | Non-hospitalised adult pilgrims were enrolled during Hajj who had coughs and could voluntarily produce sputum samples | Sputum samples were processed using the Xpert MTB-RIF assay | 1164 | 54.5 (18–94) | 2.6:1 | Hypertension (58.8) Diabetes (42.2) Kidney disease (2) Lung disease (4.4) Liver disease (2.4) Cardiovascular disease (15.9) | NR | Tuberculosis | M. tuberculosis 15 (1.4) |
| Yousuf et al., 2000 [40] | 1992–1993 | Pakistani (53.3) Algerian (13.3) Indonesian, Thai, Syrian, American, and Congolese (6.7) | All patients admitted to King Abdulaziz Hospital, Al Madinah with a diagnosis of meningococcal disease | CSF culture and smear | 15 | NR | 2.7:1 | NR | NR | Meningococcal | Meningococcal infection A and C 8 (53.3) |
| Ziyaeyan et al., 2012 [53] | 2009 | Iranian | One in ten individuals passing through the passport checkout at Shiraz International Airport was selected | Pharyngeal swabs were collected and tested by using RT-PCR | 305 | 49.2 (24–65) | 1:1.3 | NR | Influenza vaccine (97.7) | Influenza viruses | Influenza A/H1N1 4 (1.6) Other influenza A viruses 8 (2.6) |
| Author, Publication Year | Study Year | Participants’ Nationalities (%) | Selection Method/Case Ascertainment | Testing Method | Sample Size | Mean/Median Age (Range) | Male: Female | Risk Factors (%) | Vaccine Uptake (%) | Detected Diseases Name | Disease Burden n (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Aberle et al., 2015 [55] | 2014 | Austrian | Returning Hajj pilgrims who had sought medical care in different Austrian hospitals/medical centres | Sera, sputa, throat swabs, or bronchoalveolar lavage samples were collected and tested by RT-PCR | 7 | 54 (47–66) | (2.5:1) | Diabetes (43) Hypertension (43) Cardiovascular diseases (12.5) Lung disease (12.5) | NR | Viral respiratory infections | Influenza B 3 (43) Influenza A 2 (29) Rhinovirus 2 (29) MERS-CoV 0 (0) |
| Aguilera et al., 2002 [56] | 2000 | French and British | Hospitalised cases identified by National Surveillance Centres in Europe: only cases in France and UK were used for analysis | Cases were diagnosed by soluble antigen detection or PCR | 90 | 51 | (1:1.1) | NR | NR | Meningococcal | 90 cases of meningococcal W135 disease: pilgrims 12 (13) |
| Al-Abdallat et al., 2017 [57] | 2014 | Jordanian | Returning Hajj pilgrims with symptoms of RTIs were instructed to present to sentinel health facilities in the south, north, and central regions of Jordan | Nasopharyngeal and oropharyngeal swabs were collected and tested by RT-PCR | 125 | 51.5 (25–86) | (1.6:1) | Hypertension (22) Diabetes (14) Cardiovascular disease (8) Kidney disease (1) Lung disease (2) | NR | Viral respiratory infections | Rhino/enterovirus 59 (47) Coronavirus 16 (13) Influenza 6 (5) Other viruses 5 (4) MERS-CoV 0 (0) |
| Alahmari et al., 2022 [67] | 2021 | 100 different nationalities | Records of pilgrims who did the PCR test were collected from the official database of the Saudi Ministry of Health | PCR-based surveillance with paired-swab samples (pre-Hajj and post-Hajj) | 58428 | NR | (1:1) | NR | NR | COVID-19 infection | SARS-CoV-2 41 (0.1) |
| Alfelali et al., 2020 [31] | 2013–2015 | Saudi and Qatari (91) Australian (9) | Pilgrims were randomised to ‘facemask’ or ‘no facemask’ by tents in Mina, Makkah | Nasal swabs were collected and tested using a multiplex RT-PCR | 7687 | 34 (18–95) | (1:1.1) | NR | Influenza vaccine: intervention group (49.9) vs. control group (49.4) | Viral respiratory infections | Rhinovirus (35.1) Influenza A/H1N1 and H3N2 (4.5) Parainfluenza (1.7) |
| Alzeer et al., 2023 [70] | 2018 | NR | Samples were collected voluntarily from pilgrims who resided in the study tents | Nasopharyngeal swabs were collected and tested by multiplex RT-PCR | 32 | NR | NR | NR | NR | Viral and bacterial respiratory infections | Viruses: Rhinovirus 5 (15.62) Coronavirus 3 (9.4) Influenza 3 (9.4) Other viruses 7 (21.9) Bacteria: K. pneumoniae 20 (62.5) S. aureus 10 (31.3) S. pneumoniae 5 (15.6) H. influenzae 1 (3.1) Other bacteria 3 (9.4) |
| Atabani et al., 2016 [58] | 2013–2015 | British | UK travellers/pilgrims who returned from the Middle East and presented to hospitals in the Midlands, the Southwest, and North of England with RTI symptoms were actively investigated | Nose and throat swabs, nasopharyngeal aspirates, sputum and bronchoalveolar lavage samples were collected and tested by RT-PCR | 202 | 54 (4 m–85 y) | (1.4:1) | NR | NR | Viral respiratory infections | Influenza 41 (20.3) Rhinovirus 29 (14.4) Other viruses 20 (9.9) MERS-CoV 0 (0) |
| Balkhy et al., 2004 [18] | 2003 | Saudi (46.8) | Patients presented to the National Guard Mina hospital outpatient clinic, on days 10 and 11 of Hajj | Throat swabs were inoculated onto MDCK, A549 and LL19Ks cell lines using conventional methodology, and screened by immunofluorescence for viruses | 500 | Majority (20–40) | (1.1:1) | NR | Influenza vaccine (4.4) | Viral respiratory infections | Influenza 30 (7) Other viruses 24 (4.8) |
| Barasheed et al., 2014 [33] | 2013 | Australian, Saudi, and Qatari | Pilgrims were recruited during the first day of Hajj and followed closely for four days | Nasopharyngeal swabs were collected and tested by multiplex RT-PCR | 112 | 35 (18–75) | (1:1.3) | Lung disease (68) Diabetes (41) Cardiovascular disease (4) Kidney disease (4) | Influenza vaccine (68.8) | Viral respiratory infections | Rhinovirus 28 (25) Influenza 5 (4) Coronavirus 2 (2) Other viruses 5 (4) |
| Barasheed et al., 2014 [34] | 2011 | Australian | Tents were randomised to ‘supervised mask use’ versus ‘no supervised mask use’. Pilgrims with ILI symptoms for ≤3 days were recruited as ‘cases’ and those who slept within 2 m of them as ‘contacts’ | Nasal swabs were taken and tested using Quick-Vue A+B point-of-care test and NAT for influenza viruses | 164 | 44.1 (17–80) | (1:1.3) | NR | NR | Viral respiratory infections | Rhinovirus 39 (23.8) Influenza 7 (4.3) Other viruses 2 (1.2) |
| Benkouiten et al., 2013 [60] | 2012 | French | A prospective survey among a cohort of pilgrims departing from Marseille, France, to Makkah for Hajj | Nasal swabs were collected and tested by RT-PCR | 154 | 59.3 (21–83) | (1:1.6) | Diabetes (27.5) Hypertension (26.3) Lung disease (7.8) Cardiovascular disease (7.2) | Influenza vaccine (45.6) Pneumococcal vaccine (35.9) | Viral respiratory infections | Rhinovirus 13 (8.4) Influenza 2 (1.3) Other viruses 4 (2.6) |
| Benkouiten et al., 2014 [61] | 2013 | French | Pilgrims were recruited at a private specialised travel agency in Marseille, France. participants were sampled and followed up before departing from France and before leaving Saudi Arabia | Paired nasal and throat swab specimens were collected and tested by RT-PCR | 129 | 61.7 (34–85) | (1:1.5) | NR | Influenza vaccine (0) Pneumococcal vaccine (51.2) | Viral and bacterial respiratory infections | Viruses: Influenza 10 (7.8) Coronavirus 27 (20.9) Rhinovirus 19 (14.7) MERS-CoV 0(0) Bacteria: S. pneumoniae 80 (62) |
| El Bashir et al., 2004 [65] | 2003 | British | A cohort of pilgrims from the East End of London who participated in Hajj | Blood samples were collected pre-and post-Hajj, and tested by haemagglutination inhibition | 115 | NR | NR | NR | Influenza vaccine (26) | Influenza viruses | All influenza viruses 44 (38) Influenza A/H3N2 42 (37) Influenza A/H1N1 1 (0.9) Influenza B 1 (0.9) |
| Erdem et al., 2016 [59] | 201–2015 | Turkish | In patients with a diagnosis of a travel-associated infection needing hospitalisation after returning from the Arabian Peninsula. Data were collected retrospectively from infectious diseases departments of 15 Turkish referral centres | Microbiological cultures were used for bacteria and Multiplex/RT-PCR was used for viruses | 185 | 60.3 | (1:1.1) | Diabetes (24.3) Hypertension (8.6) Cardiovascular disease (10.8) Liver disease (1.1) Kidney disease (0.54) Lung disease (14.1) | NR | Viral and bacterial respiratory infections | Viruses: Influenza 15 (8.1) Coronavirus 1 (0.5) Rhinovirus 1 (0.5) Other viruses 3 (1.6) Bacteria: S. pneumoniae 1 (0.5) H. influenzae 1 (0.5) Other bacteria 1 (0.5) |
| Hoang et al., 2022 [62] | 2014–2018 | French | Hajj pilgrims from Marseille, France, were recruited through a private specialised travel agency and were systematically sampled before departing and upon their return from Hajj | Nasopharyngeal swabs were collected and tested by RT-PCR | 207 | NR | NR | Diabetes (32.4) Hypertension (28) Lung disease (15) Cardiovascular disease (9.7) Kidney disease (1.9) | Influenza vaccine (29.5) Pneumococcal vaccine (30.9) | Viral and bacterial respiratory infections | Viruses: Rhinovirus (40.6) Coronavirus (15.5) Influenza (2.9) Bacteria: S. aureus (35.8) H. influenzae (30.4) K. pneumoniae (17.4) S. pneumoniae (3.9) |
| Jones et al., 1990 [68] | 1987–1988 | British | Meningococcal Reference Laboratory | Nasal swabs were cultured | 39 | NR | NR | NR | NR | Meningococcal | Meningococcal A (0.18) |
| Ma et al., 2017 [45] | 2013–2015 | Chinese | Randomly selected returning pilgrims arriving at Xinjiang and Gansu airports | Viral infection samples collected and tested by RT-PCR | 847 | 2.24 | (1.4:1) | NR | Influenza vaccine (100) | Viral respiratory infections | Influenza 48 (5.7) Coronavirus 3 (0.3) MERS-CoV 0 (0) |
| Marglani et al., 2016 [27] | 2014 | Gulf (58) Asian (12.4) South Asian (11.9) North African (11.5) African (3.5) European (2.2) American (0.5) | Patients presented to the emergency or outpatient departments of Alnoor Specialised Hospital in Makkah | Bacteriological culture and isolation, and antimicrobial susceptibility testing (AST) were performed using MicroScan Walk Away System ID/AST | 226 | 34.6 (9–77) | (3.5:1) | NR | NR | Bacterial acute rhinosinusitis | S. aureus 46 (20.3) |
| Matsika-Claquin et al., 2001 [69] | 2000 | French | Standardised questionnaire used to interrogate study subjects | A case was considered to be confirmed when the strain isolated from usually sterile media was found to be identical to the epidemic strain (W135, 2a: P1-2.5--clonal complex ET37) | 27 | (2 m–87 y) | (1:1.2) | NR | NR | Meningococcal | Meningococcal W (0.002) |
| Nik Zuraina et al., 2018 [48] | 2016 | Malaysian | Hajj pilgrims who returned to the arrival hall of Sultan Ismail Airport, Kota Bharu, Kelantan, Malaysia with RTI symptoms, including productive cough | Bacteriological culture method and Vitek II system | 297 | 57.4 (27–82) | (1:1) | NR | NR | Bacterial respiratory infections | H. influenzae 123 (44.4) K. pneumoniae 11 (3.7) S. pneumoniae 2 (0.7) Other bacteria 28 (9.4) |
| Nik Zuraina et al., 2022 [49] | 2016 | Malaysian | Hajj pilgrims who returned to Sultan Ismail Petra Airport, Kelantan, Malaysia with RTI symptoms during Hajj | Sputum specimens were collected and tested by culture and thermostabilized, multiplex PCR | 202 | 56.7 (26–80) | (1:1.1) | NR | NR | Bacterial respiratory infections | H. influenzae 88 (43.5) K. pneumoniae 1 (0.5) S. pneumoniae 2 (1) Other bacteria 20 (9.9) |
| Novelli et al., 1987 [50] | 1987 | Qatari | Returning pilgrims or their contacts admitted to Hamad General Hospital, Doha, Qatar | Blood and/or CSF culture and/or latex test for meningococcal antigen in CSF | 15 | 40 | NR | NR | NR | Meningococcal | Meningococcal A 6 (40) |
| Rashid et al., 2008 [28] | 2005 | British | Pilgrims attending the British Hajj Delegation Medical Clinic in Makkah and in tents in Mina with symptoms of upper RTI | Two nasal swabs taken and tested by testing using PoCT and RT-PCR | 202 | 44 (1.5–83) | (9.1:1) | Diabetes, chronic heart, lung or kidney disease, all high-risk conditions together (26) | Influenza vaccine (28) | Viral respiratory infections | Influenza 28 (13.9) RSV 9 (4) |
| Rashid et al., 2008 [29] | 2006 | British | Hajj pilgrims with upper RTI who attended British Hajj Delegation Clinic in Makkah and Mina | Two nasal swabs taken and tested by testing using PoCT and RT-PCR | 150 | 41 (14–81) | (11.5:1) | Diabetes (62) Lung disease (23) Cardiovascular disease (12) | Influenza vaccine (37.3) | Viral respiratory infections | Influenza 17 (11) Rhinovirus 19 (12.7) Other viruses 2 (1.3) |
| Wilder-Smith et al., 2003 [63] | 2002 | Singaporean | Referred by travel agencies, pilgrims were recruited at a Muslim centre in Singapore that performs mass vaccinations and following a few months after Hajj | Paired blood samples were collected pre- and post-Hajj, and IgG antibodies for pertussis whole-cell antigen were measured | 358 | 48 (16–75) | (1:1.7) | NR | NR | Pertussis | Bordetella pertussis 5 (1.4) |
| Wilder-Smith et al., 2005 [64] | 2002 | Singaporean | Pilgrims were consecutively recruited at mass pre-travel vaccination sites before Hajj and following a few months after Hajj | A whole-blood assay (Quanti- FERON TB assay) prior to departure and 3 months after return from Hajj | 365 | 49.2 (18–75) | (1:1.6) | Diabetes (8.8) | NR | Tuberculosis | M. tuberculosis 139 (38) |
3.2. Comparative Variables and Attack Rates of Hajj-Acquired Airborne Infections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gatrad, A.R.; Sheikh, A. Hajj: Journey of a lifetime. BMJ 2005, 330, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, A.S.; Alshahrani, A.M.; Rashid, H. Health Issues of Mass Gatherings in the Middle East. In Handbook of Healthcare in the Arab World; Laher, I., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 1183–1198. [Google Scholar]
- Cobbin, J.C.A.; Alfelali, M.; Barasheed, O.; Taylor, J.; Dwyer, D.E.; Kok, J.; Booy, R.; Holmes, E.C.; Rashid, H. Multiple Sources of Genetic Diversity of Influenza A Viruses during the Hajj. J. Virol. 2017, 91, e00096-17. [Google Scholar] [CrossRef] [PubMed]
- Almehmadi, M.; Alqahtani, J.S. Healthcare Research in Mass Religious Gatherings and Emergency Management: A Comprehensive Narrative Review. Healthcare 2023, 11, 244. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, A.S.; Tashani, M.; Ridda, I.; Gamil, A.; Booy, R.; Rashid, H. Burden of clinical infections due to S. pneumoniae during Hajj: A systematic review. Vaccine 2018, 36, 4440–4446. [Google Scholar] [CrossRef]
- Gautret, P.; Benkouiten, S. Circulation of respiratory pathogens at mass gatherings, with special focus on the Hajj pilgrimage. In The Microbiology of Respiratory System Infections; Academic Press: Cambridge, MA, USA, 2016; Volume 1, pp. 81–93. [Google Scholar]
- Basahel, S.; Alsabban, A.; Yamin, M. Hajj and Umrah management during COVID-19. Int. J. Inf. Technol. 2021, 13, 2491–2495. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Benkouiten, S.; Memish, Z.A. A systematic review of emerging respiratory viruses at the Hajj and possible coinfection with Streptococcus pneumoniae. Travel. Med. Infect. Dis. 2018, 23, 6–13. [Google Scholar] [CrossRef]
- Benkouiten, S.; Al-Tawfiq, J.A.; Memish, Z.A.; Albarrak, A.; Gautret, P. Clinical respiratory infections and pneumonia during the Hajj pilgrimage: A systematic review. Travel. Med. Infect. Dis. 2019, 28, 15–26. [Google Scholar] [CrossRef]
- Safarpour, H.; Safi-Keykaleh, M.; Farahi-Ashtiani, I.; Bazyar, J.; Daliri, S.; Sahebi, A. Prevalence of Influenza Among Hajj Pilgrims: A Systematic Review and Meta-Analysis. Disaster Med. Public Health Prep. 2022, 16, 1221–1228. [Google Scholar] [CrossRef]
- Gautret, P.; Benkouiten, S.; Al-Tawfiq, J.A.; Memish, Z.A. Hajj-associated viral respiratory infections: A systematic review. Travel. Med. Infect. Dis. 2016, 14, 92–109. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- AlBarrak, A.; Alotaibi, B.; Yassin, Y.; Mushi, A.; Maashi, F.; Seedahmed, Y.; Alshaer, M.; Altaweel, A.; Elshiekh, H.; Turkistani, A.; et al. Proportion of adult community-acquired pneumonia cases attributable to Streptococcus pneumoniae among Hajj pilgrims in 2016. Int. J. Infect. Dis. 2018, 69, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, S.M.; Alandijany, T.A.; El-Kafrawy, S.A.; Hassan, A.M.; Bajrai, L.H.; Faizo, A.A.; Mulla, E.A.; Aljahdali, L.S.; Alquthami, K.M.; Zumla, A.; et al. Pattern of Respiratory Viruses among Pilgrims during 2019 Hajj Season Who Sought Healthcare Due to Severe Respiratory Symptoms. Pathogens 2021, 10, 315. [Google Scholar] [CrossRef] [PubMed]
- Asghar, A.H.; Ashshi, A.M.; Azhar, E.I.; Bukhari, S.Z.; Zafar, T.A.; Momenah, A.M. Profile of bacterial pneumonia during Hajj. Indian. J. Med. Res. 2011, 133, 510–513. [Google Scholar] [PubMed]
- Baharoon, S.; Al-Jahdali, H.; Al Hashmi, J.; Memish, Z.A.; Ahmed, Q.A. Severe sepsis and septic shock at the Hajj: Etiologies and outcomes. Travel. Med. Infect. Dis. 2009, 7, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Bokhary, H.; Research Team, H.; Barasheed, O.; Othman, H.B.; Saha, B.; Rashid, H.; Hill-Cawthorne, G.A.; Abd El Ghany, M. Evaluation of the rate, pattern and appropriateness of antibiotic prescription in a cohort of pilgrims suffering from upper respiratory tract infection during the 2018 Hajj season. Access Microbiol. 2022, 4, 000338. [Google Scholar] [CrossRef] [PubMed]
- Balkhy, H.H.; Memish, Z.A.; Bafaqeer, S.; Almuneef, M.A. Influenza a common viral infection among Hajj pilgrims: Time for routine surveillance and vaccination. J. Travel. Med. 2004, 11, 82–86. [Google Scholar] [CrossRef][Green Version]
- El-Gamal, S.A.; Saleh, L.H. An outbreak of meningococcal infection at the time of pilgrimage in Saudi Arabia. J. Egypt. Public Health Assoc. 1988, 63, 263–274. [Google Scholar]
- El-Kafrawy, S.A.; Alsayed, S.M.; Alandijany, T.A.; Bajrai, L.H.; Faizo, A.A.; Al-Sharif, H.A.; Hassan, A.M.; Alquthami, K.M.; Al-Tawfiq, J.A.; Zumla, A.; et al. High genetic diversity of human rhinovirus among pilgrims with acute respiratory tract infections during the 2019 Hajj pilgrimage season. Int. J. Infect. Dis. 2022, 121, 130–137. [Google Scholar] [CrossRef]
- El-Sheikh, S.M.; El-Assouli, S.M.; Mohammed, K.A.; Albar, M. Bacteria and viruses that cause respiratory tract infections during the pilgrimage (Haj) season in Makkah, Saudi Arabia. Trop. Med. Int. Health 1998, 3, 205–209. [Google Scholar]
- Hashem, A.M.; Al-Subhi, T.L.; Badroon, N.A.; Hassan, A.M.; Bajrai, L.H.M.; Banassir, T.M.; Alquthami, K.M.; Azhar, E.I. MERS-CoV, influenza and other respiratory viruses among symptomatic pilgrims during 2014 Hajj season. J. Med. Virol. 2019, 91, 911–917. [Google Scholar] [CrossRef]
- Karima, T.M.; Bukhari, S.Z.; Fatani, M.I.; Yasin, K.A.; Al-Afif, K.A.; Hafiz, F.H. Clinical and microbiological spectrum of meningococcal disease in adults during Hajj 2000: An implication of quadrivalent vaccination policy. J. Pak. Med. Assoc. 2003, 53, 3–7. [Google Scholar] [PubMed]
- Lingappa, J.R.; Al-Rabeah, A.M.; Hajjeh, R.; Mustafa, T.; Fatani, A.; Al-Bassam, T.; Badukhan, A.; Turkistani, A.; Makki, S.; Al-Hamdan, N.; et al. Serogroup W-135 meningococcal disease during the Hajj, 2000. Emerg. Infect. Dis. 2003, 9, 665–671. [Google Scholar] [CrossRef]
- Mandourah, Y.; Al-Radi, A.; Ocheltree, A.H.; Ocheltree, S.R.; Fowler, R.A. Clinical and temporal patterns of severe pneumonia causing critical illness during Hajj. BMC Infect. Dis. 2012, 12, 117. [Google Scholar] [CrossRef] [PubMed]
- Mandourah, Y.; Ocheltree, A.; Al Radi, A.; Fowler, R. The epidemiology of Hajj-related critical illness: Lessons for deployment of temporary critical care services. Crit. Care Med. 2012, 40, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Marglani, O.A.; Alherabi, A.Z.; Herzallah, I.R.; Saati, F.A.; Tantawy, E.A.; Alandejani, T.A.; Faidah, H.S.; Bawazeer, N.A.; Marghalani, A.A.; Madani, T.A. Acute rhinosinusitis during Hajj season 2014: Prevalence of bacterial infection and patterns of antimicrobial susceptibility. Travel Med. Infect. Dis. 2016, 14, 583–587. [Google Scholar] [CrossRef]
- Rashid, H.; Shafi, S.; Booy, R.; El Bashir, H.; Ali, K.; Zambon, M.; Memish, Z.; Ellis, J.; Coen, P.; Haworth, E. Influenza and respiratory syncytial virus infections in British Hajj pilgrims. Emerg. Health Threats J. 2008, 1, e2. [Google Scholar] [CrossRef]
- Rashid, H.; Shafi, S.; Haworth, E.; El Bashir, H.; Memish, Z.A.; Sudhanva, M.; Smith, M.; Auburn, H.; Booy, R. Viral respiratory infections at the Hajj: Comparison between UK and Saudi pilgrims. Clin. Microbiol. Infect. 2008, 14, 569–574. [Google Scholar] [CrossRef]
- Shirah, B.H.; Zafar, S.H.; Alferaidi, O.A.; Sabir, A.M.M. Mass gathering medicine (Hajj Pilgrimage in Saudi Arabia): The clinical pattern of pneumonia among pilgrims during Hajj. J. Infect. Public Health 2017, 10, 277–286. [Google Scholar] [CrossRef]
- Alfelali, M.; Haworth, E.A.; Barasheed, O.; Badahdah, A.M.; Bokhary, H.; Tashani, M.; Azeem, M.I.; Kok, J.; Taylor, J.; Barnes, E.H.; et al. Facemask against viral respiratory infections among Hajj pilgrims: A challenging cluster-randomized trial. PLoS ONE 2020, 15, e0240287. [Google Scholar] [CrossRef]
- Alzeer, A.; Mashlah, A.; Fakim, N.; Al-Sugair, N.; Al-Hedaithy, M.; Al-Majed, S.; Jamjoom, G. Tuberculosis is the commonest cause of pneumonia requiring hospitalization during Hajj (pilgrimage to Makkah). J. Infect. 1998, 36, 303–306. [Google Scholar] [CrossRef]
- Barasheed, O.; Almasri, N.; Badahdah, A.M.; Heron, L.; Taylor, J.; McPhee, K.; Ridda, I.; Haworth, E.; Dwyer, D.E.; Rashid, H.; et al. Pilot Randomised Controlled Trial to Test Effectiveness of Facemasks in Preventing Influenza-like Illness Transmission among Australian Hajj Pilgrims in 2011. Infect. Disord. Drug Targets 2014, 14, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Barasheed, O.; Rashid, H.; Alfelali, M.; Tashani, M.; Azeem, M.; Bokhary, H.; Kalantan, N.; Samkari, J.; Heron, L.; Kok, J.; et al. Viral respiratory infections among Hajj pilgrims in 2013. Virol. Sin. 2014, 29, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Yezli, S.; Zumla, A.; Yassin, Y.; Al-Shangiti, A.M.; Mohamed, G.; Turkistani, A.M.; Alotaibi, B. Undiagnosed Active Pulmonary Tuberculosis among Pilgrims during the 2015 Hajj Mass Gathering: A Prospective Cross-sectional Study. Am. J. Trop. Med. Hyg. 2017, 97, 1304–1309. [Google Scholar] [CrossRef][Green Version]
- Ashshi, A.; Azhar, E.; Johargy, A.; Asghar, A.; Momenah, A.; Turkestani, A.; Alghamdi, S.; Memish, Z.; Al-Ghamdi, A.; Alawi, M.; et al. Demographic distribution and transmission potential of influenza A and 2009 pandemic influenza A H1N1 in pilgrims. J. Infect. Dev. Ctries. 2014, 8, 1169–1175. [Google Scholar] [CrossRef]
- Memish, Z.A.; Assiri, A.M.; Hussain, R.; Alomar, I.; Stephens, G. Detection of respiratory viruses among pilgrims in Saudi Arabia during the time of a declared influenza A(H1N1) pandemic. J. Travel. Med. 2012, 19, 15–21. [Google Scholar] [CrossRef]
- Memish, Z.A.; Assiri, A.; Almasri, M.; Alhakeem, R.F.; Turkestani, A.; Al Rabeeah, A.A.; Al-Tawfiq, J.A.; Alzahrani, A.; Azhar, E.; Makhdoom, H.Q.; et al. Prevalence of MERS-CoV nasal carriage and compliance with the Saudi health recommendations among pilgrims attending the 2013 Hajj. J. Infect. Dis. 2014, 210, 1067–1072. [Google Scholar] [CrossRef]
- Memish, Z.A.; Assiri, A.; Turkestani, A.; Yezli, S.; Al Masri, M.; Charrel, R.; Drali, T.; Gaudart, J.; Edouard, S.; Parola, P.; et al. Mass gathering and globalization of respiratory pathogens during the 2013 Hajj. Clin. Microbiol. Infect. 2015, 21, 571.e1–571.e8. [Google Scholar] [CrossRef] [PubMed]
- Yousuf, M.; Nadeem, A. Meningococcal infection among pilgrims visiting Madinah Al-Munawarah despite prior A-C vaccination. J. Pak. Med. Assoc. 2000, 50, 184–186. [Google Scholar]
- Alborzi, A.; Aelami, M.H.; Ziyaeyan, M.; Jamalidoust, M.; Moeini, M.; Pourabbas, B.; Abbasian, A. Viral etiology of acute respiratory infections among Iranian Hajj pilgrims, 2006. J. Travel Med. 2009, 16, 239–242. [Google Scholar] [CrossRef]
- Annan, A.; Owusu, M.; Marfo, K.S.; Larbi, R.; Sarpong, F.N.; Adu-Sarkodie, Y.; Amankwa, J.; Fiafemetsi, S.; Drosten, C.; Owusu-Dabo, E.; et al. High prevalence of common respiratory viruses and no evidence of Middle East respiratory syndrome coronavirus in Hajj pilgrims returning to Ghana, 2013. Trop. Med. Int. Health 2015, 20, 807–812. [Google Scholar] [CrossRef]
- Kandeel, A.; Deming, M.; Elkreem, E.A.; El-Refay, S.; Afifi, S.; Abukela, M.; Earhart, K.; El-Sayed, N.; El-Gabay, H. Pandemic (H1N1) 2009 and Hajj Pilgrims who received Predeparture Vaccination, Egypt. Emerg. Infect. Dis. 2011, 17, 1266–1268. [Google Scholar] [CrossRef] [PubMed]
- Koul, P.A.; Mir, H.; Saha, S.; Chadha, M.S.; Potdar, V.; Widdowson, M.A.; Lal, R.B.; Krishnan, A. Respiratory viruses in returning Hajj & Umrah pilgrims with acute respiratory illness in 2014–2015. Indian J. Med. Res. 2018, 148, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Liu, F.; Liu, L.; Zhang, L.; Lu, M.; Abudukadeer, A.; Wang, L.; Tian, F.; Zhen, W.; Yang, P.; et al. No MERS-CoV but positive influenza viruses in returning Hajj pilgrims, China, 2013–2015. BMC Infect. Dis. 2017, 17, 715. [Google Scholar] [CrossRef]
- Moattari, A.; Emami, A.; Moghadami, M.; Honarvar, B. Influenza viral infections among the Iranian Hajj pilgrims returning to Shiraz, Fars province, Iran. Influenza Other Respir. Viruses 2012, 6, e77–e79. [Google Scholar] [CrossRef] [PubMed]
- Muraduzzaman, A.K.M.; Khan, M.H.; Parveen, R.; Sultana, S.; Alam, A.N.; Akram, A.; Rahman, M.; Shirin, T. Event based surveillance of Middle East Respiratory Syndrome Coronavirus (MERS- CoV) in Bangladesh among pilgrims and travelers from the Middle East: An update for the period 2013–2016. PLoS ONE 2018, 13, e0189914. [Google Scholar] [CrossRef]
- Nik Zuraina, N.M.N.; Sarimah, A.; Suharni, M.; Hasan, H.; Suraiya, S. High frequency of Haemophilus influenzae associated with respiratory tract infections among Malaysian Hajj pilgrims. J. Infect. Public Health 2018, 11, 878–883. [Google Scholar] [CrossRef]
- Noor Nik Zuraina, N.M.; Hasan, H.; Mohamad, S.; Suraiya, S. Diagnostic detection of intended bacteria associated with respiratory tract infections among Kelantanese Malaysian Hajj pilgrims by a ready-to-use, thermostable multiplex PCR assay. Saudi J. Biol. Sci. 2022, 29, 103349. [Google Scholar] [CrossRef]
- Novelli, V.M.; Lewis, R.G.; Dawood, S.T. Epidemic group A meningococcal disease in Haj pilgrims. Lancet 1987, 2, 863. [Google Scholar] [CrossRef]
- Refaey, S.; Amin, M.M.; Roguski, K.; Azziz-Baumgartner, E.; Uyeki, T.M.; Labib, M.; Kandeel, A. Cross-sectional survey and surveillance for influenza viruses and MERS-CoV among Egyptian pilgrims returning from Hajj during 2012–2015. Influenza Other Respir. Viruses 2017, 11, 57–60. [Google Scholar] [CrossRef]
- Yavarian, J.; Shafiei Jandaghi, N.Z.; Naseri, M.; Hemmati, P.; Dadras, M.; Gouya, M.M.; Mokhtari Azad, T. Influenza virus but not MERS coronavirus circulation in Iran, 2013–2016: Comparison between pilgrims and general population. Travel Med. Infect. Dis. 2018, 21, 51–55. [Google Scholar] [CrossRef]
- Ziyaeyan, M.; Alborzi, A.; Jamalidoust, M.; Moeini, M.; Pouladfar, G.R.; Pourabbas, B.; Namayandeh, M.; Moghadami, M.; Bagheri-Lankarani, K.; Mokhtari-Azad, T. Pandemic 2009 influenza A (H1N1) infection among 2009 Hajj Pilgrims from Southern Iran: A real-time RT-PCR-based study. Influenza Other Respir. Viruses 2012, 6, e80–e84. [Google Scholar] [CrossRef] [PubMed]
- Harimurti, K.; Saldi, S.R.F.; Dewiasty, E.; Alfarizi, T.; Dharmayuli, M.; Khoeri, M.M.; Paramaiswari, W.T.; Salsabila, K.; Tafroji, W.; Halim, C.; et al. Streptococcus pneumoniae carriage and antibiotic susceptibility among Indonesian pilgrims during the Hajj pilgrimage in 2015. PLoS ONE 2021, 16, e0246122. [Google Scholar] [CrossRef]
- Aberle, J.H.; Popow-Kraupp, T.; Kreidl, P.; Laferl, H.; Heinz, F.X.; Aberle, S.W. Influenza A and B Viruses but Not MERS-CoV in Hajj Pilgrims, Austria, 2014. Emerg. Infect. Dis. 2015, 21, 726–727. [Google Scholar] [CrossRef] [PubMed]
- Aguilera, J.F.; Perrocheau, A.; Meffre, C.; Hahne, S.; Group, W.W. Outbreak of serogroup W135 meningococcal disease after the Hajj pilgrimage, Europe, 2000. Emerg. Infect. Dis. 2002, 8, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Al-Abdallat, M.M.; Rha, B.; Alqasrawi, S.; Payne, D.C.; Iblan, I.; Binder, A.M.; Haddadin, A.; Nsour, M.A.; Alsanouri, T.; Mofleh, J.; et al. Acute respiratory infections among returning Hajj pilgrims-Jordan, 2014. J. Clin. Virol. 2017, 89, 34–37. [Google Scholar] [CrossRef]
- Atabani, S.F.; Wilson, S.; Overton-Lewis, C.; Workman, J.; Kidd, I.M.; Petersen, E.; Zumla, A.; Smit, E.; Osman, H. Active screening and surveillance in the United Kingdom for Middle East respiratory syndrome coronavirus in returning travellers and pilgrims from the Middle East: A prospective descriptive study for the period 2013-2015. Int. J. Infect. Dis. 2016, 47, 10–14. [Google Scholar] [CrossRef]
- Erdem, H.; Ak, O.; Elaldi, N.; Demirdal, T.; Hargreaves, S.; Nemli, S.A.; Cag, Y.; Ulug, M.; Naz, H.; Gunal, O.; et al. Infections in travellers returning to Turkey from the Arabian peninsula: A retrospective cross-sectional multicenter study. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 903–910. [Google Scholar] [CrossRef]
- Benkouiten, S.; Charrel, R.; Belhouchat, K.; Drali, T.; Nougairede, A.; Salez, N.; Memish, Z.A.; Al Masri, M.; Fournier, P.E.; Raoult, D.; et al. Respiratory viruses and bacteria among pilgrims during the 2013 Hajj. Emerg. Infect. Dis. 2014, 20, 1821–1827. [Google Scholar] [CrossRef]
- Benkouiten, S.; Charrel, R.; Belhouchat, K.; Drali, T.; Salez, N.; Nougairede, A.; Zandotti, C.; Memish, Z.A.; Al Masri, M.; Gaillard, C.; et al. Circulation of respiratory viruses among pilgrims during the 2012 Hajj pilgrimage. Clin. Infect. Dis. 2013, 57, 992–1000. [Google Scholar] [CrossRef]
- Hoang, V.T.; Dao, T.L.; Ly, T.D.A.; Drali, T.; Yezli, S.; Parola, P.; Pommier de Santi, V.; Gautret, P. Respiratory pathogens among ill pilgrims and the potential benefit of using point-of-care rapid molecular diagnostic tools during the Hajj. Acta Microbiol. Immunol. Hung. 2022, 69, 283–289. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Earnest, A.; Ravindran, S.; Paton, N.I. High incidence of pertussis among Hajj pilgrims. Clin. Infect. Dis. 2003, 37, 1270–1272. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Foo, W.; Earnest, A.; Paton, N.I. High risk of Mycobacterium tuberculosis infection during the Hajj pilgrimage. Trop. Med. Int. Health 2005, 10, 336–339. [Google Scholar] [CrossRef] [PubMed]
- El Bashir, H.; Haworth, E.; Zambon, M.; Shafi, S.; Zuckerman, J.; Booy, R. Influenza among U.K. pilgrims to hajj, 2003. Emerg. Infect. Dis. 2004, 10, 1882–1883. [Google Scholar] [CrossRef] [PubMed]
- Memish, Z.A.; Almasri, M.; Turkestani, A.; Al-Shangiti, A.M.; Yezli, S. Etiology of severe community-acquired pneumonia during the 2013 Hajj-part of the MERS-CoV surveillance program. Int. J. Infect. Dis. 2014, 25, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Alahmari, A.A.; Khan, A.A.; Alamri, F.A.; Almuzaini, Y.S.; Alradini, F.A.; Almohamadi, E.; Alsaeedi, S.; Asiri, S.; Motair, W.; Almadah, A.; et al. Hajj 2021: Role of mitigation measures for health security. J. Infect. Public Health 2022, 15, 1350–1354. [Google Scholar] [CrossRef]
- Jones, D.M.; Sutcliffe, E.M. Group A meningococcal disease in England associated with the Haj. J. Infect. 1990, 21, 21–25. [Google Scholar] [CrossRef]
- Matsika-Claquin, M.D.; Perrocheau, A.; Taha, M.K.; Levy-Bruhl, D.; Renault, P.; Alonso, J.M.; Desenclos, J.C. Meningococcal W135 infection epidemics associated with pilgrimage to Mecca in 2000. Presse Med. 2001, 30, 1529–1534. [Google Scholar]
- Alzeer, A.H.; Somily, A.; Aldosari, K.M.; Ahamed, S.S.; Saadon, A.H.A.; Mohamed, D.H. Microbial surveillance of Hajj tents: Bioaerosol sampling coupled with real-time multiplex PCR. Am. J. Infect. Control 2023, 51, 199–204. [Google Scholar] [CrossRef]
- Alharbi, N.S.; Al-Barrak, A.M.; Al-Moamary, M.S.; Zeitouni, M.O.; Idrees, M.M.; Al-Ghobain, M.O.; Al-Shimemeri, A.A.; Al-Hajjaj, M.S. The Saudi Thoracic Society pneumococcal vaccination guidelines-2016. Ann. Thorac. Med. 2016, 11, 93–102. [Google Scholar] [CrossRef]
- Alsuhebany, N.; Alowais, S.A.; Aldairem, A.; Almohareb, S.N.; Bin Saleh, K.; Kahtani, K.M.; Alnashwan, L.I.; Alay, S.M.; Alamri, M.G.; Alhathlol, G.K.; et al. Identifying gaps in vaccination perception after mandating the COVID-19 vaccine in Saudi Arabia. Vaccine 2023, 41, 3611–3616. [Google Scholar] [CrossRef]
- Rashid, H.; Abdul Muttalif, A.R.; Mohamed Dahlan, Z.B.; Djauzi, S.; Iqbal, Z.; Karim, H.M.; Naeem, S.M.; Tantawichien, T.; Zotomayor, R.; Patil, S.; et al. The potential for pneumococcal vaccination in Hajj pilgrims: Expert opinion. Travel. Med. Infect. Dis. 2013, 11, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Albutti, A.; Mahdi, H.A.; Alwashmi, A.S.; Alfelali, M.; Barasheed, O.; Barnes, E.H.; Shaban, R.Z.; Booy, R.; Rashid, H. The relationship between hand hygiene and rates of acute respiratory infections among Umrah pilgrims: A pilot randomised controlled trial. J. Infect. Public Health, 2023; in press. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, Q.A.; Memish, Z.A. Hajj 2022 and the post pandemic mass gathering: Epidemiological data and decision making. New Microbes New Infect. 2022, 49–50, 101033. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic (accessed on 27 May 2023).
- Alarabiya News. Saudi Arabia to Host Pre-Pandemic Numbers for 2023 Hajj Pilgrimage Season. Available online: https://english.alarabiya.net/News/saudi-arabia/2023/01/09/Saudi-Arabia-to-host-pre-pandemic-numbers-for-2023-Hajj-pilgrimage-season (accessed on 27 May 2023).

| Variables | Low and Middle-Income Countries | High-Income Countries |
|---|---|---|
| Demographics | ||
| Pooled study sample | 27,799 | 70,865 |
| Age (range) | 2 d–105 y | 2 m–95 y |
| Male: Female | 1.3:1 | 1:1 |
| Vaccination uptake (%) | ||
| Influenza vaccination | 19.7–100 | 0–100 |
| Pneumococcal vaccination | 1.2–4.4 | 30.9–51.2 |
| Risk factors (%) | ||
| Diabetes | 5.8–36 | 0.9–32.4 |
| Hypertension | 2.9–43 | 8.6–28 |
| Cardiovascular disease | 0.8–43 | 0.1–10.8 |
| Chronic lung disease | 1.1–71 | 1.4–15 |
| Chronic kidney disease | 0.5–2 | 0.1–1.9 |
| Chronic liver disease | 0.2–6.4 | 1.1 |
| Attack rate of viral airborne infections (%) | ||
| Influenza | 0.5–29.5 | 1.3–38 |
| Human rhinovirus | 5.9–39.5 | 0.5–47 |
| Human coronavirus | 0.4–19.5 | 0.1–20.9 |
| Other viruses | 0.7–16.4 | 0.7–21.9 |
| Attack rate of bacterial airborne infections (%) | ||
| Meningococci | 0.015–82 | 0.002–40 |
| M. tuberculosis | 0.7–20.3 | 38 |
| S. pneumoniae | 1–54.8 | 0.5–62 |
| K. pneumoniae | 1.1–29 | 0.5–62.5 |
| H. influenza | 4.7–24 | 0.5–44.4 |
| S. aureus | 0.7–36 | 20.3–35.8 |
| Other bacteria | 0.8–50 | 0.5–9.9 |
| Studies | Selection (Max 4 Stars) | Comparability (Max 2 Stars) | Outcome/Exposure (Max 3 Stars) | Total Score |
|---|---|---|---|---|
| High-income countries (HIC) | ||||
| Aberle et al., 2015 [55] | ** | – | ** | 4 |
| Aguilera et al., 2002 [56] | *** | – | *** | 6 |
| Al-Abdallat et al., 2017 [57] | ** | – | ** | 4 |
| Alahmari et al., 2022 [67] | *** | – | *** | 6 |
| Alfelali et al., 2020 [31] | *** | * | ** | 6 |
| Alzeer et al., 2023 [70] | *** | – | ** | 5 |
| Atabani et al., 2016 [58] | ** | – | ** | 4 |
| Balkhy et al., 2004 [18] | ** | – | ** | 4 |
| Barasheed et al., 2014 [33] | *** | * | ** | 6 |
| Barasheed et al., 2014 [34] | *** | * | ** | 6 |
| Benkouiten et al., 2013 [60] | *** | – | *** | 6 |
| Benkouiten et al., 2014 [61] | *** | – | *** | 6 |
| El Bashir et al., 2004 [65] | *** | – | *** | 6 |
| Erdem et al., 2016 [59] | ** | – | *** | 5 |
| Hoang et al., 2022 [62] | *** | – | *** | 6 |
| Jones et al., 1990 [68] | ** | – | ** | 4 |
| Ma et al., 2017 [45] | ** | – | *** | 5 |
| Marglani et al., 2016 [27] | ** | – | ** | 4 |
| Matsika-Claquin et al., 2001 [69] | ** | – | ** | 4 |
| Nik Zuraina et al., 2018 [48] | ** | – | ** | 4 |
| Nik Zuraina et al., 2022 [49] | ** | – | ** | 4 |
| Novelli et al., 1987 [50] | ** | – | ** | 4 |
| Rashid et al., 2008 [28] | ** | – | *** | 5 |
| Rashid et al., 2008 [29] | ** | – | *** | 5 |
| Wilder-Smith et al., 2003 [63] | *** | – | ** | 5 |
| Wilder-Smith et al., 2005 [64] | *** | – | ** | 5 |
| Low and middle-income countries (LMIC) | ||||
| AlBarrak et al., 2018 [13] | ** | – | ** | 4 |
| Alborzi et al., 2009 [41] | ** | – | ** | 4 |
| Alsayed et al., 2021 [14] | ** | – | ** | 4 |
| Alzeer et al., 1998 [32] | ** | – | ** | 4 |
| Annan et al., 2015 [42] | ** | – | ** | 4 |
| Asghar et al., 2011 [15] | ** | – | ** | 4 |
| Ashshi et al., 2014 [36] | ** | – | ** | 4 |
| Baharoon et al., 2009 [16] | ** | – | ** | 4 |
| Bokhary et al., 2022 [17] | ** | – | * | 3 |
| El-Gamal et al., 1988 [19] | ** | – | ** | 4 |
| El-Kafrawy et al., 2022 [20] | ** | – | ** | 4 |
| El-Sheikh et al., 1998 [21] | ** | – | ** | 4 |
| Hashem et al., 2019 [22] | ** | – | ** | 4 |
| Harimurti et al., 2021 [54] | *** | – | *** | 6 |
| Kandeel et al., 2011 [43] | ** | – | ** | 4 |
| Karima et al., 2003 [23] | ** | – | ** | 4 |
| Koul et al., 2018 [44] | ** | – | ** | 4 |
| Lingappa et al., 2003 [24] | ** | – | ** | 4 |
| Mandourah et al., 2012 [25] | ** | – | ** | 4 |
| Mandourah et al., 2012 [26] | ** | – | ** | 4 |
| Memish et al., 2012 [37] | *** | – | *** | 6 |
| Memish et al., 2014 [38] | ** | – | ** | 4 |
| Memish et al., 2014 [66] | *** | – | *** | 6 |
| Memish et al., 2015 [39] | *** | – | *** | 6 |
| Moattari et al., 2012 [46] | ** | – | ** | 4 |
| Muraduzzaman et al., 2018 [47] | ** | – | ** | 4 |
| Refaey et al., 2017 [51] | *** | – | ** | 5 |
| Shirah et al., 2017 [30] | ** | – | ** | 4 |
| Yavarian et al., 2018 [52] | ** | – | ** | 4 |
| Yezli et al., 2017 [35] | ** | – | ** | 4 |
| Yousuf et al., 2000 [40] | ** | – | ** | 4 |
| Ziyaeyan et al., 2012 [53] | ** | – | ** | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahdi, H.A.; Alluhidan, M.; Almohammed, A.B.; Alfelali, M.; Shaban, R.Z.; Booy, R.; Rashid, H. Epidemiological Differences in Hajj-Acquired Airborne Infections in Pilgrims Arriving from Low and Middle-Income versus High-Income Countries: A Systematised Review. Trop. Med. Infect. Dis. 2023, 8, 418. https://doi.org/10.3390/tropicalmed8080418
Mahdi HA, Alluhidan M, Almohammed AB, Alfelali M, Shaban RZ, Booy R, Rashid H. Epidemiological Differences in Hajj-Acquired Airborne Infections in Pilgrims Arriving from Low and Middle-Income versus High-Income Countries: A Systematised Review. Tropical Medicine and Infectious Disease. 2023; 8(8):418. https://doi.org/10.3390/tropicalmed8080418
Chicago/Turabian StyleMahdi, Hashim A., Mohammed Alluhidan, Abdulrahman B. Almohammed, Mohammad Alfelali, Ramon Z. Shaban, Robert Booy, and Harunor Rashid. 2023. "Epidemiological Differences in Hajj-Acquired Airborne Infections in Pilgrims Arriving from Low and Middle-Income versus High-Income Countries: A Systematised Review" Tropical Medicine and Infectious Disease 8, no. 8: 418. https://doi.org/10.3390/tropicalmed8080418
APA StyleMahdi, H. A., Alluhidan, M., Almohammed, A. B., Alfelali, M., Shaban, R. Z., Booy, R., & Rashid, H. (2023). Epidemiological Differences in Hajj-Acquired Airborne Infections in Pilgrims Arriving from Low and Middle-Income versus High-Income Countries: A Systematised Review. Tropical Medicine and Infectious Disease, 8(8), 418. https://doi.org/10.3390/tropicalmed8080418