
“Together against Tuberculosis”: Cascade of Care of Patients Referred by the Private Health Care Providers in the Kyrgyz Republic

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
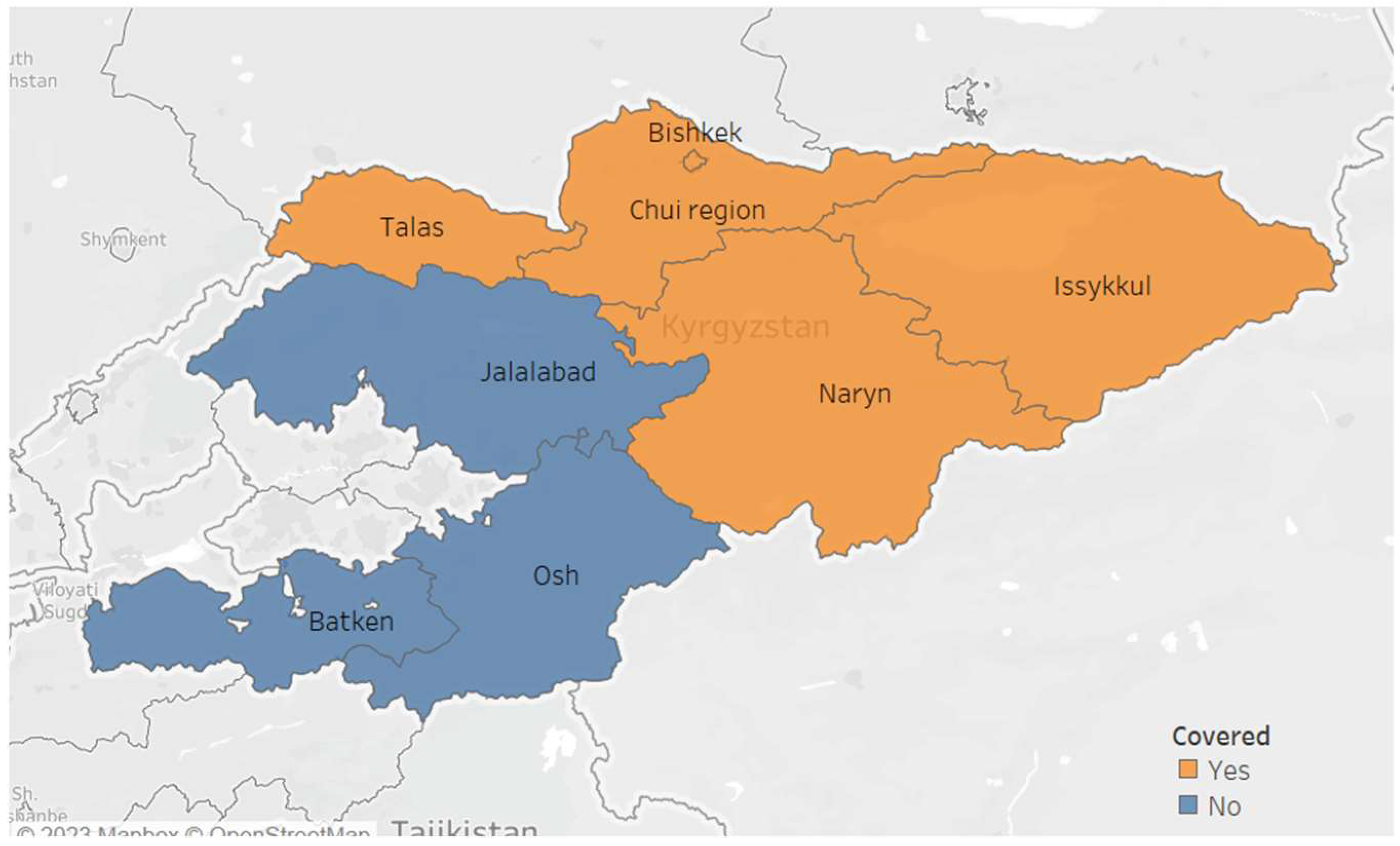
2.2. Study Setting
2.3. Specific Setting
2.3.1. Screening and Identification of Presumptive TB Patients
2.3.2. Sputum Collection and Transport
2.3.3. Diagnosis and Treatment of TB
2.3.4. Recording and Reporting of the Data
2.4. Study Population
2.5. Operational Definitions
2.6. Data Collection, Variables and Sources of Data
2.7. Data Entry and Analysis
3. Results
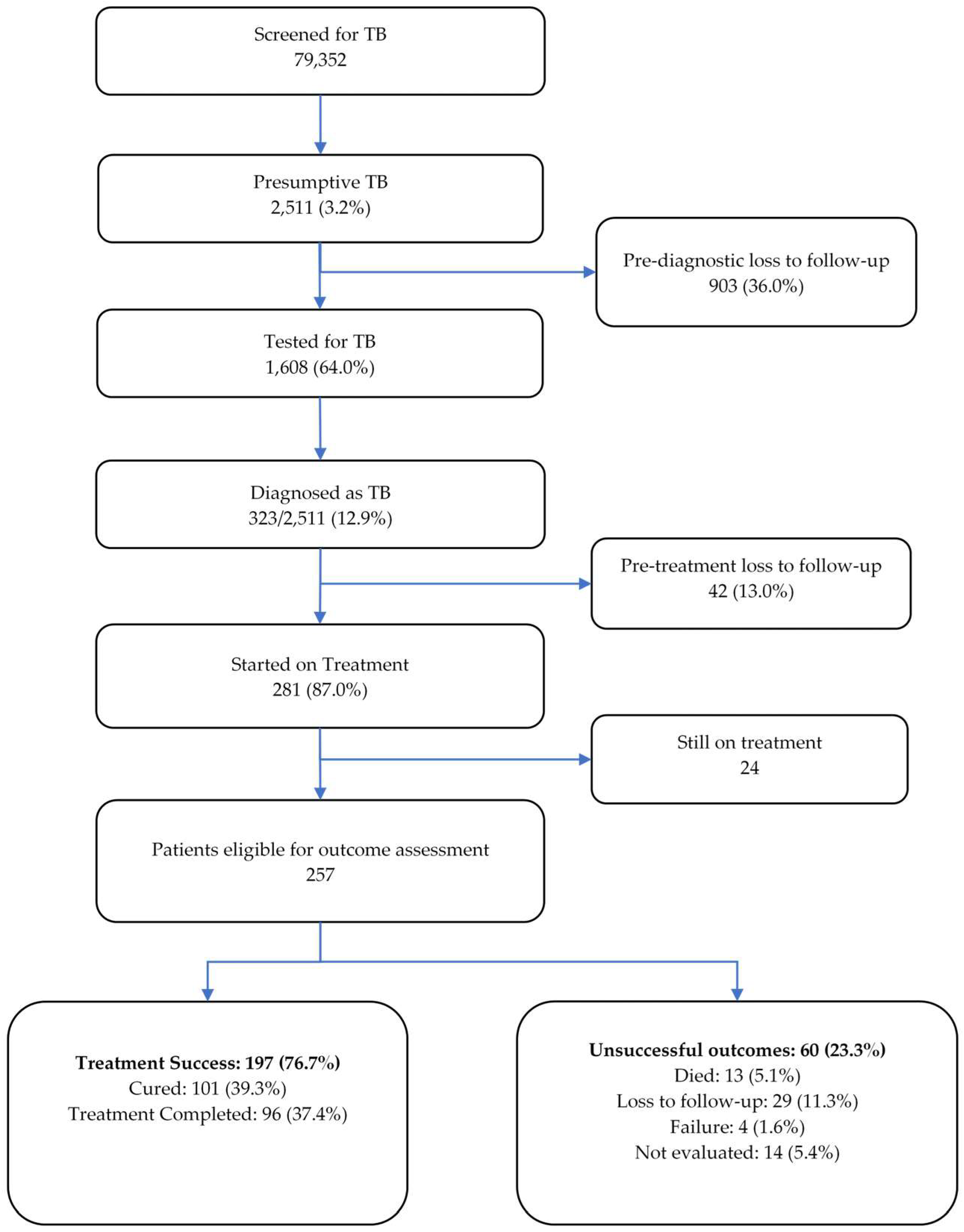
3.1. Cascade of Care
3.2. Demographic, Risk and Clinical Characteristics of TB Patients
3.3. Delays in Testing, Diagnosis and Initiation of Treatment
3.4. Factors Associated with Pre-Treatment Loss to Follow-Up
3.5. Factors Associated with Unsuccessful Treatment Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report. 2022. Available online: https://www.who.int/teams/global-tuberculosis-programme/data (accessed on 8 May 2023).
- Subbaraman, R.; Nathavitharana, R.R.; Satyanarayana, S.; Pai, M.; Thomas, B.E.; Chadha, V.K.; Rade, K.; Swaminathan, S.; Mayer, K.H. The Tuberculosis Cascade of Care in India’s Public Sector: A Systematic Review and Meta-Analysis. PLoS Med. 2016, 13, e1002149. [Google Scholar] [CrossRef] [PubMed]
- MacPherson, P.; Houben, R.M.; Glynn, J.R.; Corbett, E.L.; Kranzer, K. Pre-Treatment Loss to Follow-up in Tuberculosis Patients in Low- and Lower-Middle-Income Countries and High-Burden Countries: A Systematic Review and Meta-Analysis. Bull. World Health Organ. 2014, 92, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Padingani, M.; Kumar, A.; Tripathy, J.P.; Masuka, N.; Khumalo, S. Does Pre-Diagnostic Loss to Follow-up among Presumptive TB Patients Differ by Type of Health Facility? An Operational Research from Hwange, Zimbabwe in 2017. Pan. Afr. Med. J. 2018, 31, 196. [Google Scholar] [CrossRef] [PubMed]
- World Bank. The World Bank in the Kyrgyz Republic. Available online: https://www.worldbank.org/en/country/kyrgyzrepublic/overview (accessed on 8 May 2023).
- Trading Economics Kyrgyzstan GDP per Capita. Available online: https://tradingeconomics.com/kyrgyzstan/gdp-per-capita (accessed on 8 May 2023).
- Mohammed, H.; Oljira, L.; Roba, K.; Ngadaya, E.; Tesfaye, D.; Manyazewal, T.; Yimer, G. Impact of Early Chest Radiography on Delay in Pulmonary Tuberculosis Case Notification in Ethiopia. Int. J. Mycobacteriol. 2021, 10, 364. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, H.; Oljira, L.; Roba, K.T.; Ngadaya, E.; Manyazewal, T.; Ajeme, T.; Mnyambwa, N.P.; Fekadu, A.; Yimer, G. Tuberculosis Prevalence and Predictors Among Health Care-Seeking People Screened for Cough of Any Duration in Ethiopia: A Multicenter Cross-Sectional Study. Front. Public Health 2022, 9, 805726. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, P.; Theron, G.; Rangaka, M.X.; Chihota, V.N.; Vaughan, L.; Brey, Z.O.; Pillay, Y. The South African Tuberculosis Care Cascade: Estimated Losses and Methodological Challenges. J. Infect. Dis. 2017, 216, S702–S713. [Google Scholar] [CrossRef] [PubMed]
- Botha, E.; den Boon, S.; Lawrence, K.-A.; Reuter, H.; Verver, S.; Lombard, C.J.; Dye, C.; Enarson, D.A.; Beyers, N. From Suspect to Patient: Tuberculosis Diagnosis and Treatment Initiation in Health Facilities in South Africa. Int. J. Tuberc. Lung Dis. 2008, 12, 936–941. [Google Scholar] [PubMed]
- Khan, B.J.; Kumar, A.M.V.; Stewart, A.; Khan, N.M.; Selvaraj, K.; Fatima, R.; Samad, Z. Alarming Rates of Attrition among Tuberculosis Patients in Public-Private Facilities in Lahore, Pakistan. Public Health Action 2017, 7, 127–133. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Gopi, P.G.; Chandrasekaran, V.; Subramani, R.; Narayanan, P.R. Failure to Initiate Treatment for Tuberculosis Patients Diagnosed in a Community Survey and at Health Facilities under a DOTS Programme in a District of South India. Indian J. Tuberc. 2005, 52, 153–156. [Google Scholar]
- Thomas, B.E.; Suresh, C.; Lavanya, J.; Lindsley, M.M.; Galivanche, A.T.; Sellappan, S.; Ovung, S.; Aravind, A.; Lincy, S.; Raja, A.L.; et al. Understanding Pretreatment Loss to Follow-up of Tuberculosis Patients: An Explanatory Qualitative Study in Chennai, India. BMJ Glob. Health 2020, 5, e001974. [Google Scholar] [CrossRef] [PubMed]
- Squire, S.B.; Belaye, A.K.; Kashoti, A.; Salaniponi, F.M.L.; Mundy, C.J.F.; Theobald, S.; Kemp, J. “Lost” Smear-Positive Pulmonary Tuberculosis Cases: Where Are They and Why Did We Lose Them? Int. J. Tuberc. Lung Dis. 2005, 9, 25–31. [Google Scholar] [PubMed]
- Buu, T.N.; Lönnroth, K.; Quy, H.T. Initial Defaulting in the National Tuberculosis Programme in Ho Chi Minh City, Vietnam: A Survey of Extent, Reasons and Alternative Actions Taken Following Default. Int. J. Tuberc. Lung Dis. 2003, 7, 735–741. [Google Scholar] [PubMed]
- Botha, E.; Den Boon, S.; Verver, S.; Dunbar, R.; Lawrence, K.-A.; Bosman, M.; Enarson, D.A.; Toms, I.; Beyers, N. Initial Default from Tuberculosis Treatment: How Often Does It Happen and What Are the Reasons? Int. J. Tuberc. Lung Dis. 2008, 12, 820–823. [Google Scholar] [PubMed]
- Sai Babu, B.; Satyanarayana, A.V.; Venkateshwaralu, G.V.; Ramakrishna, U.; Vikram, P.; Sahu, S.; Wares, F.; Dewan, P.K.; Santosha, K.; Jyoti, J.; et al. Initial Default among Diagnosed Sputum Smear-Positive Pulmonary Tuberculosis Patients in Andhra Pradesh, India. Int. J. Tuberc. Lung Dis. 2008, 12, 1055–1058. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Term | Definition |
|---|---|
| Presumptive TB |
|
| Tested for TB |
|
| Diagnosis of TB |
|
| Rifampicin-Resistant TB (RR-TB) |
|
| Treatment for TB |
|
| Successful outcomes |
|
| Unsuccessful outcomes |
|
| Characteristics | N | (%) |
|---|---|---|
| Age | ||
| 0–14 | 44 | (13.6) |
| 15–34 | 136 | (42.1) |
| 35–64 | 107 | (33.1) |
| 65 and above | 36 | (11.1) |
| Gender | ||
| Male | 174 | (53.9) |
| Female | 149 | (46.1) |
| Region | ||
| Bishkek | 224 | (69.3) |
| Chuy | 77 | (23.8) |
| Talas | 15 | (4.6) |
| Naryn | 6 | (1.9) |
| Issyk-Kul | 1 | (0.3) |
| Risk factors * | ||
| Contact | 45 | (13.9) |
| Smoking | 27 | (8.4) |
| Alcohol use | 13 | (4) |
| Drug use | 0 | (0) |
| Homeless | 4 | (1.2) |
| Unemployed | 99 | (30.7) |
| Ex-Prisoner | 2 | (0.6) |
| Diabetes | 15 | (4.6) |
| External migrant | 19 | (5.9) |
| Internal migrant | 30 | (9.3) |
| HIV **-positive | 4 | (1.2) |
| Receipt of ART ** | 3 | (75) ** |
| Characteristics | N | (%) |
|---|---|---|
| Type of TB | ||
| Pulmonary | 280 | (86.7) |
| Extra pulmonary | 43 | (13.3) |
| Registration category | ||
| New | 295 | (91.3) |
| Relapse | 15 | (4.6) |
| Treatment after LTFU * | 1 | (0.3) |
| Treatment after Failure | 2 | (0.6) |
| Others | 7 | (2.3) |
| Not recorded | 3 | (0.9) |
| Clinical classification | ||
| Bacteriologically confirmed | 196 | (60.7) |
| Clinically diagnosed | 127 | (39.3) |
| Drug resistance | ||
| MDR-TB | 64 | (19.8) |
| XDR-TB | 1 | (0.3) |
| Poly resistant TB | 24 | (7.4) |
| Drug-sensitive TB * | 233 | (72.1) |
| Not recorded | 1 | (0.3) |
| Duration (Days) | Number Eligible | Number (%) with Valid Dates | Median (IQR) |
|---|---|---|---|
| Screening to sputum collection | 323 | 258 (80) | 1 (0–6) |
| Sputum collection to diagnosis | 323 | 211 (65) | 3 (1–8) |
| Diagnosis to start of treatment | 281 | 203 (72) | 0 (0–1) |
| Start of treatment to registration | 281 | 241 (86) | 0 (0–3) |
| Date of screening to registration | 281 | 269 (96) | 7 (3–19) |
| Variables | Total | PTLFU * | Crude RR | 95% CI | |
|---|---|---|---|---|---|
| N | (%) | ||||
| Total | 323 | 42 | (13.0) | ||
| Age group (years) | |||||
| 0–14 | 44 | 7 | (15.9) | 2.86 | 0.63–12.94 |
| 15–34 | 136 | 22 | (16.2) | 2.91 | 0.71–11.80 |
| 35–64 | 107 | 11 | (10.3) | 1.85 | 0.43–7.95 |
| 65 and above | 36 | 2 | (5.6) | Ref | |
| Sex | |||||
| Male | 174 | 28 | (16.1) | 1.71 | 0.94–3.13 |
| Female | 149 | 14 | (9.4) | Ref | |
| Region | |||||
| Bishkek | 224 | 32 | (14.3) | 1.41 | 0.72–2.76 |
| Others | 99 | 10 | (10.1) | Ref | |
| Contact | |||||
| No | 278 | 39 | (14.0) | 2.10 | 0.67–6.52 |
| Yes | 45 | 3 | (6.7) | Ref | |
| Smoking | |||||
| No | 296 | 42 | (14.2) | NA | NA |
| Yes | 27 | 0 | (0) | ||
| Alcohol use | |||||
| No | 310 | 42 | (13.5) | NA | NA |
| Yes | 13 | 0 | (0) | ||
| Drug use | |||||
| No | 323 | 42 | (13) | NA | NA |
| Yes | 0 | 0 | (0) | ||
| Homeless | |||||
| No | 319 | 42 | (13.6) | NA | NA |
| Yes | 4 | 0 | (0) | ||
| Unemployed | |||||
| No | 224 | 42 | (18.8) | NA | NA |
| Yes | 99 | 0 | (0) | ||
| Ex-prisoner | |||||
| No | 321 | 42 | (13.1) | NA | NA |
| Yes | 2 | 0 | (0) | ||
| Diabetes | |||||
| No | 308 | 42 | (13.6) | NA | NA |
| Yes | 15 | 0 | (0) | ||
| External Migration | |||||
| No | 304 | 38 | (12.5) | Ref | |
| Yes | 19 | 4 | (21.1) | 1.68 | 0.67–4.23 |
| Internal Migration | |||||
| No | 293 | 42 | (14.3) | NA | NA |
| Yes | 30 | 0 | (0) | ||
| HIV status | |||||
| No | 319 | 42 | (13.2) | NA | NA |
| Yes | 4 | 0 | (0) | ||
| Type of TB | |||||
| Pulmonary | 280 | 38 | (13.6) | 1.45 | 0.54–3.88 |
| Extra pulmonary | 43 | 4 | (9.3) | Ref | |
| Registration category | |||||
| New | 295 | 37 | (12.5) | 1.50 | 0.38–5.86 |
| Previously treated | 24 | 2 | (8.3) | Ref | |
| Clinical classification | |||||
| Bacteriologically confirmed | 196 | 18 | (9.2) | Ref | |
| Clinically diagnosed | 127 | 24 | (18.9) | 2.05 | 1.16–3.63 |
| Drug resistance | |||||
| DR-TB | 89 | 3 | (3.4) | Ref | |
| DS-TB | 233 | 38 | (16.3) | 4.84 | 1.53–15.28 |
| Factors | Total | Unsuccessful Outcomes * | Crude RR | 95% CI | |
|---|---|---|---|---|---|
| N | (%) | ||||
| Total | 195 | 46 | (23.6) | ||
| Age group (years) | |||||
| 0–14 | 24 | 3 | (12.5) | Ref | |
| 15–34 | 79 | 15 | (19.0) | 1.51 | 0.47–4.80 |
| 35–64 | 66 | 20 | (30.3) | 2.42 | 0.79–7.42 |
| 65 and above | 26 | 8 | (30.8) | 2.46 | 0.73–8.21 |
| Sex | |||||
| Male | 103 | 26 | (25.2) | 1.16 | 0.69–1.93 |
| Female | 92 | 20 | (21.7) | Ref | |
| Region | |||||
| Bishkek | 139 | 34 | (24.5) | Ref | |
| Others | 56 | 12 | (21.4) | 0.88 | 0.49–1.57 |
| Contact | |||||
| No | 168 | 41 | (24.4) | 1.31 | 0.57–3.03 |
| Yes | 27 | 5 | (18.5) | Ref | |
| Smoking | |||||
| No | 180 | 45 | (25.0) | 3.75 | 0.55–25.33 |
| Yes | 15 | 1 | (6.7) | Ref | |
| Alcohol use | |||||
| No | 186 | 42 | (22.6) | Ref | |
| Yes | 9 | 4 | (44.4) | 1.96 | 0.9–4.28 |
| Drug use | |||||
| No | 195 | 46 | (23.6) | NA | NA |
| Yes | |||||
| Homeless | |||||
| No | 192 | 45 | (23.4) | Ref | |
| Yes | 3 | 1 | (33.3) | 1.42 | 0.28–7.19 |
| Unemployed | |||||
| No | 132 | 33 | (25.0) | Ref | |
| Yes | 63 | 13 | (20.6) | 0.83 | 0.47–1.46 |
| Ex-prisoner | |||||
| No | 194 | 46 | (23.7) | NA | NA |
| Yes | 1 | 0 | (0) | ||
| Diabetes | |||||
| No | 185 | 43 | (23.2) | Ref | |
| Yes | 10 | 3 | (30.0) | 1.29 | 0.48–3.44 |
| External Migration | |||||
| No | 183 | 43 | (23.5) | Ref | |
| Yes | 12 | 3 | (25.0) | 1.06 | 0.38–2.93 |
| Internal Migration | |||||
| No | 174 | 44 | (25.3) | Ref | |
| Yes | 21 | 2 | (9.5) | 0.37 | 0.09–1.44 |
| HIV status | |||||
| No | 193 | 46 | (23.8) | NA | NA |
| Yes | 2 | 0 | (0) | ||
| Type of TB | |||||
| Pulmonary | 167 | 42 | (25.1) | 1.76 | 0.68–4.52 |
| Extra pulmonary | 28 | 4 | (14.3) | Ref | |
| Registration category | |||||
| New | 181 | 41 | (22.7) | Ref | |
| Previously treated | 14 | 5 | (35.7) | 1.57 | 0.74–3.34 |
| Clinical classification | |||||
| Bacteriologically confirmed | 106 | 30 | (28.3) | 1.57 | 0.91–2.69 |
| Clinically diagnosed | 89 | 16 | (18.0) | Ref | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madybaeva, D.; Duishekeeva, A.; Meteliuk, A.; Kulzhabaeva, A.; Kadyrov, A.; Shumskaia, N.; Kumar, A.M.V. “Together against Tuberculosis”: Cascade of Care of Patients Referred by the Private Health Care Providers in the Kyrgyz Republic. Trop. Med. Infect. Dis. 2023, 8, 316. https://doi.org/10.3390/tropicalmed8060316
Madybaeva D, Duishekeeva A, Meteliuk A, Kulzhabaeva A, Kadyrov A, Shumskaia N, Kumar AMV. “Together against Tuberculosis”: Cascade of Care of Patients Referred by the Private Health Care Providers in the Kyrgyz Republic. Tropical Medicine and Infectious Disease. 2023; 8(6):316. https://doi.org/10.3390/tropicalmed8060316
Chicago/Turabian StyleMadybaeva, Dinara, Aiymgul Duishekeeva, Anna Meteliuk, Aizat Kulzhabaeva, Abdullaat Kadyrov, Natalia Shumskaia, and Ajay M. V. Kumar. 2023. "“Together against Tuberculosis”: Cascade of Care of Patients Referred by the Private Health Care Providers in the Kyrgyz Republic" Tropical Medicine and Infectious Disease 8, no. 6: 316. https://doi.org/10.3390/tropicalmed8060316
APA StyleMadybaeva, D., Duishekeeva, A., Meteliuk, A., Kulzhabaeva, A., Kadyrov, A., Shumskaia, N., & Kumar, A. M. V. (2023). “Together against Tuberculosis”: Cascade of Care of Patients Referred by the Private Health Care Providers in the Kyrgyz Republic. Tropical Medicine and Infectious Disease, 8(6), 316. https://doi.org/10.3390/tropicalmed8060316