


Real-Time Monitoring of Infectious Disease Outbreaks with a Combination of Google Trends Search Results and the Moving Epidemic Method: A Respiratory Syncytial Virus Case Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data
2.2. Correlation
2.3. The Moving Epidemic Method (MEM)
3. Results
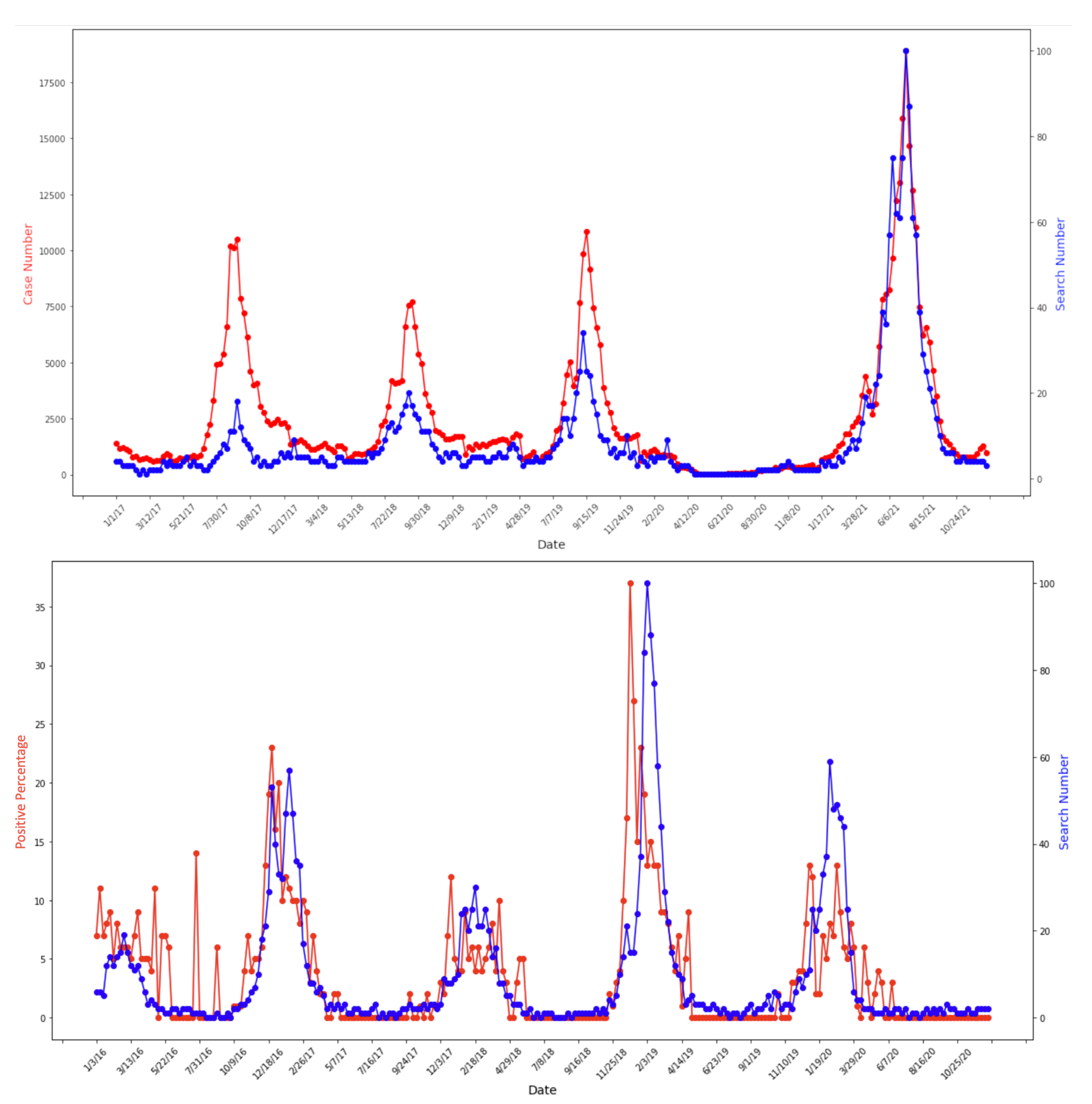
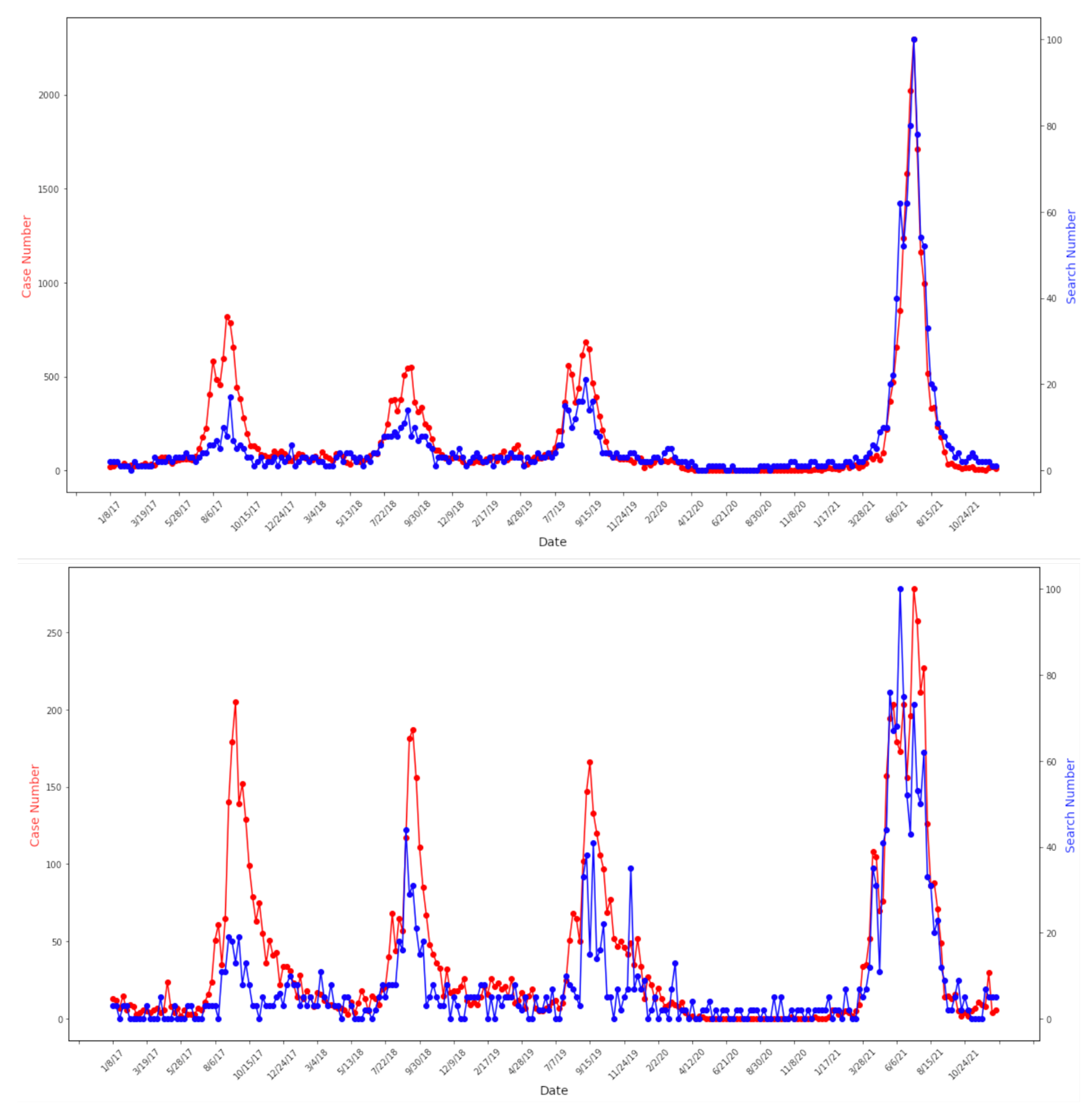
3.1. Identical Seasonal Patterns between Google Trends and Case Data
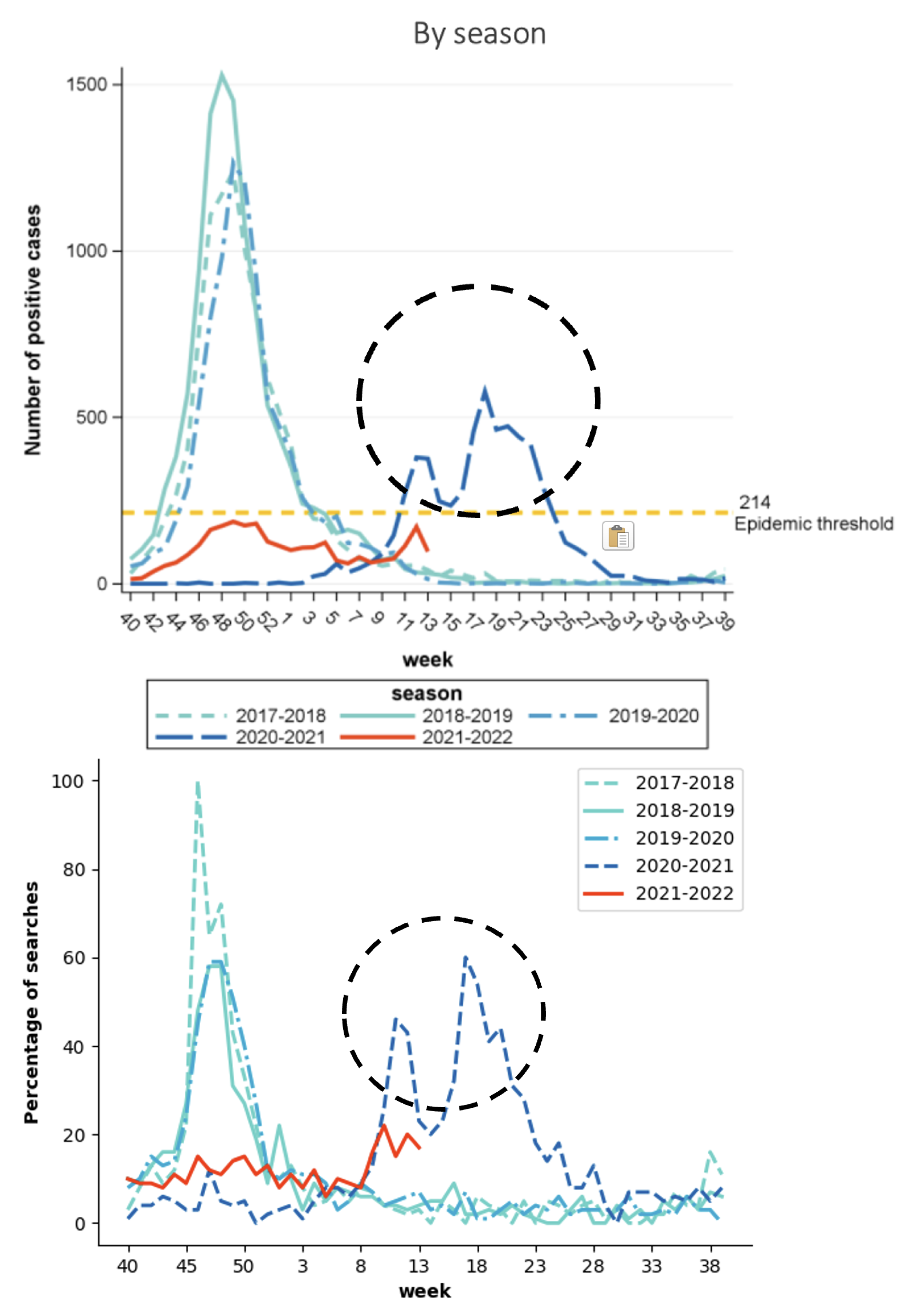
3.2. Identical Epidemiological Estimates from Case and Google Trends Data
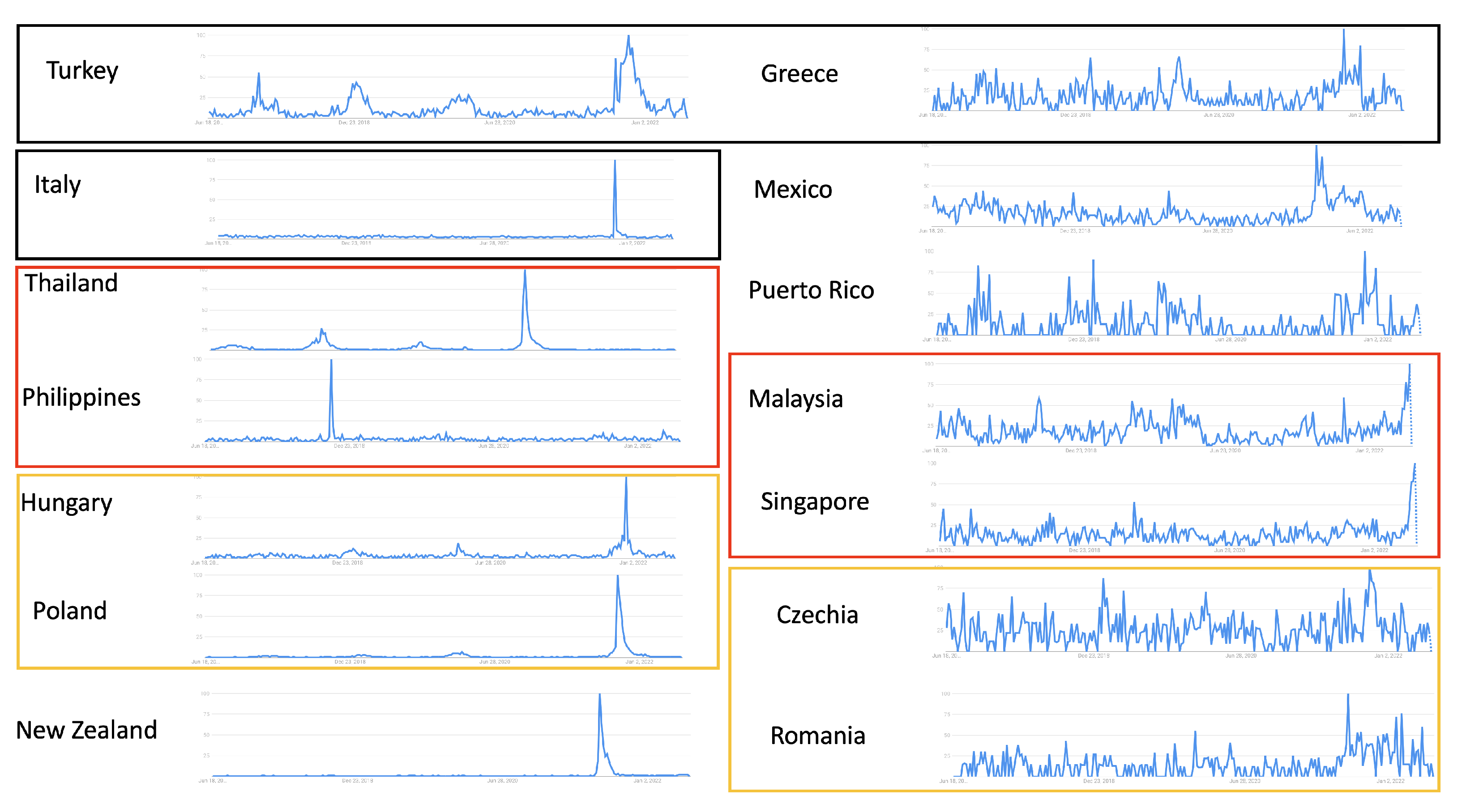
3.3. Epidemic Estimates from Google Trends Data in Countries with Limited Case Surveillance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease |
| RSV | Respiratory syncytial virus |
| MEM | Moving Epidemic Method |
References
- Coultas, J.A.; Smyth, R.; Openshaw, P.J. Respiratory syncytial virus (RSV): A scourge from infancy to old age. Thorax 2019, 74, 986–993. [Google Scholar] [CrossRef] [PubMed]
- Battles, M.B.; McLellan, J.S. Respiratory syncytial virus entry and how to block it. Nat. Rev. Microbiol. 2019, 17, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, L.; Sheppard, M.; Smith, A.; Dietz, S.; Jayanthi, P.; Yuan, Y.; Bull, L.; Wotiz, S.; Schwarze, T.; Azondekon, R.; et al. Changes in seasonal respiratory illnesses in the United States during the coronavirus disease 2019 (COVID-19) pandemic. Clin. Infect. Dis. 2021, 73, S110–S117. [Google Scholar] [CrossRef]
- Lee, H.; Lee, H.; Song, K.H.; Kim, E.S.; Park, J.S.; Jung, J.; Ahn, S.; Jeong, E.K.; Park, H.; Kim, H.B. Impact of public health interventions on seasonal influenza activity during the COVID-19 outbreak in Korea. Clin. Infect. Dis. 2021, 73, e132–e140. [Google Scholar] [CrossRef] [PubMed]
- Lei, H.; Xu, M.; Wang, X.; Xie, Y.; Du, X.; Chen, T.; Yang, L.; Wang, D.; Shu, Y. Nonpharmaceutical interventions used to control COVID-19 reduced seasonal influenza transmission in China. J. Infect. Dis. 2020, 222, 1780–1783. [Google Scholar] [CrossRef]
- Di Mattia, G.; Nenna, R.; Mancino, E.; Rizzo, V.; Pierangeli, A.; Villani, A.; Midulla, F. During the COVID-19 pandemic where has respiratory syncytial virus gone? Pediatr. Pulmonol. 2021, 56, 3106–3109. [Google Scholar] [CrossRef]
- Castagno, E.; Raffaldi, I.; Del Monte, F.; Garazzino, S.; Bondone, C. New epidemiological trends of respiratory syncytial virus bronchiolitis during COVID-19 pandemic. World J. Pediatr. 2022, 1–3. [Google Scholar] [CrossRef]
- Taylor, A.; Whittaker, E. The changing epidemiology of respiratory viruses in children during the COVID-19 pandemic: A Canary in a COVID Time. Pediatr. Infect. Dis. J. 2022, 41, e46. [Google Scholar] [CrossRef]
- Ohnishi, T.; Kawano, Y. Resurgence of respiratory syncytial virus infection during an atypical season in Japan. J. Pediatr. Infect. Dis. Soc. 2021, 10, 982–983. [Google Scholar] [CrossRef]
- Olsen, S.J.; Azziz-Baumgartner, E.; Budd, A.P.; Brammer, L.; Sullivan, S.; Pineda, R.F.; Cohen, C.; Fry, A.M. Decreased influenza activity during the COVID-19 pandemic—United States, Australia, Chile, and South Africa, 2020. Am. J. Transplant. 2020, 20, 3681–3685. [Google Scholar] [CrossRef]
- Agca, H.; Akalin, H.; Saglik, I.; Hacimustafaoglu, M.; Celebi, S.; Ener, B. Changing epidemiology of influenza and other respiratory viruses in the first year of COVID-19 pandemic. J. Infect. Public Health 2021, 14, 1186–1190. [Google Scholar] [CrossRef] [PubMed]
- Van Brusselen, D.; De Troeyer, K.; Ter Haar, E.; Vander Auwera, A.; Poschet, K.; Van Nuijs, S.; Bael, A.; Stobbelaar, K.; Verhulst, S.; Van Herendael, B.; et al. Bronchiolitis in COVID-19 times: A nearly absent disease? Eur. J. Pediatr. 2021, 180, 1969–1973. [Google Scholar] [CrossRef]
- Vittucci, A.C.; Piccioni, L.; Coltella, L.; Ciarlitto, C.; Antilici, L.; Bozzola, E.; Midulla, F.; Palma, P.; Perno, C.F.; Villani, A. The disappearance of respiratory viruses in children during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 9550. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.G.; Carlson, S.; Cheng, A.C.; Chilver, M.B.; Dwyer, D.E.; Irwin, M.; Kok, J.; Macartney, K.; MacLachlan, J.; Minney-Smith, C.; et al. Where has all the influenza gone? The impact of COVID-19 on the circulation of influenza and other respiratory viruses, Australia, March to September 2020. Eurosurveillance 2020, 25, 2001847. [Google Scholar] [CrossRef] [PubMed]
- Eden, J.S.; Sikazwe, C.; Xie, R.; Deng, Y.M.; Sullivan, S.G.; Michie, A.; Levy, A.; Cutmore, E.; Blyth, C.C.; Britton, P.N.; et al. Off-season RSV epidemics in Australia after easing of COVID-19 restrictions. Nat. Commun. 2022, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Saravanos, G.L.; Hu, N.; Homaira, N.; Muscatello, D.J.; Jaffe, A.; Bartlett, A.W.; Wood, N.J.; Rawlinson, W.; Kesson, A.; Lingam, R.; et al. RSV Epidemiology in Australia before and during COVID-19. Pediatrics 2022, 149. [Google Scholar] [CrossRef]
- Huang, Q.S.; Wood, T.; Jelley, L.; Jennings, T.; Jefferies, S.; Daniells, K.; Nesdale, A.; Dowell, T.; Turner, N.; Campbell-Stokes, P.; et al. Impact of the COVID-19 nonpharmaceutical interventions on influenza and other respiratory viral infections in New Zealand. Nat. Commun. 2021, 12, 1–7. [Google Scholar] [CrossRef]
- Varela, F.H.; Scotta, M.C.; Polese-Bonatto, M.; Sartor, I.T.S.; Ferreira, C.F.; Fernandes, I.R.; Zavaglia, G.O.; de Almeida, W.A.F.; Arakaki-Sanchez, D.; Pinto, L.A.; et al. Absence of detection of RSV and influenza during the COVID-19 pandemic in a Brazilian cohort: Likely role of lower transmission in the community. J. Glob. Health 2021, 11, 5007. [Google Scholar] [CrossRef]
- Goverment, N. Respiratory Syncytial Virus (RSV) Fact Sheet. Available online: https://www.health.nsw.gov.au/Infectious/factsheets/Pages/respiratory-syncytial-virus.aspx (accessed on 10 December 2022).
- Johnson, H.A.; Wagner, M.M.; Hogan, W.R.; Chapman, W.; Olszewski, R.T.; Dowling, J.; Barnas, G. Analysis of Web access logs for surveillance of influenza. In MEDINFO 2004; IOS Press: Amsterdam, The Netherlands, 2004; pp. 1202–1206. [Google Scholar]
- Eysenbach, G. Infodemiology: Tracking flu-related searches on the web for syndromic surveillance. In Proceedings of the AMIA Annual Symposium Proceedings, Washington, DC, USA, 11–15 November 2006; American Medical Informatics Association: Rockville, MD, USA, 2006; Volume 2006, p. 244. [Google Scholar]
- Polgreen, P.M.; Chen, Y.; Pennock, D.M.; Nelson, F.D.; Weinstein, R.A. Using internet searches for influenza surveillance. Clin. Infect. Dis. 2008, 47, 1443–1448. [Google Scholar] [CrossRef]
- Ginsberg, J.; Mohebbi, M.H.; Patel, R.S.; Brammer, L.; Smolinski, M.S.; Brilliant, L. Detecting influenza epidemics using search engine query data. Nature 2009, 457, 1012–1014. [Google Scholar] [CrossRef]
- Cho, S.; Sohn, C.H.; Jo, M.W.; Shin, S.Y.; Lee, J.H.; Ryoo, S.M.; Kim, W.Y.; Seo, D.W. Correlation between national influenza surveillance data and google trends in South Korea. PLoS ONE 2013, 8, e81422. [Google Scholar] [CrossRef] [PubMed]
- Pollett, S.; Boscardin, W.J.; Azziz-Baumgartner, E.; Tinoco, Y.O.; Soto, G.; Romero, C.; Kok, J.; Biggerstaff, M.; Viboud, C.; Rutherford, G.W. Evaluating Google Flu Trends in Latin America: Important lessons for the next phase of digital disease detection. Clin. Infect. Dis. 2016, 64, ciw657. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.T.; Gumel, A.; Thompson, L.H.; Strome, T.; Mahmud, S.M. “Google flu trends” and emergency department triage data predicted the 2009 pandemic H1N1 waves in Manitoba. Can. J. Public Health 2011, 102, 294–297. [Google Scholar] [CrossRef]
- Kang, M.; Zhong, H.; He, J.; Rutherford, S.; Yang, F. Using google trends for influenza surveillance in South China. PLoS ONE 2013, 8, e55205. [Google Scholar] [CrossRef] [PubMed]
- Olson, D.R.; Konty, K.J.; Paladini, M.; Viboud, C.; Simonsen, L. Reassessing Google Flu Trends data for detection of seasonal and pandemic influenza: A comparative epidemiological study at three geographic scales. PLoS Comput. Biol. 2013, 9, e1003256. [Google Scholar] [CrossRef]
- Dugas, A.F.; Hsieh, Y.H.; Levin, S.R.; Pines, J.M.; Mareiniss, D.P.; Mohareb, A.; Gaydos, C.A.; Perl, T.M.; Rothman, R.E. Google Flu Trends: Correlation with emergency department influenza rates and crowding metrics. Clin. Infect. Dis. 2012, 54, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Bakker, K.M.; Martinez-Bakker, M.E.; Helm, B.; Stevenson, T.J. Digital epidemiology reveals global childhood disease seasonality and the effects of immunization. Proc. Natl. Acad. Sci. USA 2016, 113, 6689–6694. [Google Scholar] [CrossRef] [PubMed]
- Tkachenko, N.; Chotvijit, S.; Gupta, N.; Bradley, E.; Gilks, C.; Guo, W.; Crosby, H.; Shore, E.; Thiarai, M.; Procter, R.; et al. Google Trends can improve surveillance of Type 2 diabetes. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef]
- Husnayain, A.; Fuad, A.; Lazuardi, L. Correlation between Google Trends on dengue fever and national surveillance report in Indonesia. Glob. Health Action 2019, 12, 1552652. [Google Scholar] [CrossRef]
- Strauss, R.; Lorenz, E.; Kristensen, K.; Eibach, D.; Torres, J.; May, J.; Castro, J. Investigating the utility of Google trends for Zika and Chikungunya surveillance in Venezuela. BMC Public Health 2020, 20, 1–6. [Google Scholar] [CrossRef]
- Johnson, A.K.; Bhaumik, R.; Tabidze, I.; Mehta, S.D. Nowcasting sexually transmitted infections in Chicago: Predictive modeling and evaluation study using Google Trends. JMIR Public Health Surveill. 2020, 6, e20588. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.; Hopkins, C.; Surda, P. Use of Google Trends to investigate loss-of-smell–related searches during the COVID-19 outbreak. In International Forum of Allergy & Rhinology; Wiley Online Library: Hoboken, NJ, USA, 2020; Volume 10, pp. 839–847. [Google Scholar]
- Mavragani, A.; Ochoa, G.; Tsagarakis, K.P. Assessing the methods, tools, and statistical approaches in Google Trends research: Systematic review. J. Med. Internet Res. 2018, 20, e9366. [Google Scholar] [CrossRef] [PubMed]
- Braun, T.; Harréus, U. Medical nowcasting using Google trends: Application in otolaryngology. Eur. Arch.-Oto-Rhino-Laryngol. 2013, 270, 2157–2160. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.G.; Song, W.J.; Choi, S.; Kim, H.; Ha, H.; Kim, S.H.; Cho, S.H.; Min, K.U.; Yoon, S.; Chang, Y.S. Google unveils a glimpse of allergic rhinitis in the real world. Allergy 2015, 70, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Seifter, A.; Schwarzwalder, A.; Geis, K.; Aucott, J. The utility of “Google Trends” for epidemiological research: Lyme disease as an example. Geospat. Health 2010, 4, 135–137. [Google Scholar] [CrossRef]
- Takada, K. Japanese interest in “Hotaru”(fireflies) and “Kabuto-Mushi”(japanese Rhinoceros beetles) corresponds with seasonality in visible abundance. Insects 2012, 3, 424–431. [Google Scholar] [CrossRef]
- Willson, T.J.; Lospinoso, J.; Weitzel, E.; McMains, K. Correlating regional aeroallergen effects on internet search activity. Otolaryngol.-Head Neck Surg. 2015, 152, 228–232. [Google Scholar] [CrossRef]
- Toosi, B.; Kalia, S. Seasonal and geographic patterns in tanning using real-time data from Google Trends. JAMA Dermatol. 2016, 152, 215–217. [Google Scholar] [CrossRef]
- Harsha, A.K.; Schmitt, J.E.; Stavropoulos, S.W. Know your market: Use of online query tools to quantify trends in patient information-seeking behavior for varicose vein treatment. J. Vasc. Interv. Radiol. 2014, 25, 53–57. [Google Scholar] [CrossRef]
- El-Sheikha, J. Global search demand for varicose vein information on the internet. Phlebology 2015, 30, 533–540. [Google Scholar] [CrossRef]
- Harsha, A.K.; Schmitt, J.E.; Stavropoulos, S.W. Match day: Online search trends reflect growing interest in IR training. J. Vasc. Interv. Radiol. 2015, 26, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Ingram, D.G.; Matthews, C.K.; Plante, D.T. Seasonal trends in sleep-disordered breathing: Evidence from Internet search engine query data. Sleep Breath. 2015, 19, 79–84. [Google Scholar] [CrossRef] [PubMed]
- DeVilbiss, E.A.; Lee, B.K. Brief report: Trends in US National autism awareness from 2004 to 2014: The impact of national autism awareness month. J. Autism Dev. Disord. 2014, 44, 3271–3273. [Google Scholar] [CrossRef] [PubMed]
- Plante, D.T.; Ingram, D.G. Seasonal trends in tinnitus symptomatology: Evidence from Internet search engine query data. Eur. Arch.-Oto-Rhino-Laryngol. 2015, 272, 2807–2813. [Google Scholar] [CrossRef]
- Sentana-Lledo, D.; Barbu, C.M.; Ngo, M.N.; Wu, Y.; Sethuraman, K.; Levy, M.Z. Seasons, searches, and intentions: What the internet can tell us about the bed bug (Hemiptera: Cimicidae) epidemic. J. Med. Entomol. 2016, 53, 116–121. [Google Scholar] [CrossRef]
- Zhang, Z.; Zheng, X.; Zeng, D.D.; Leischow, S.J. Tracking dabbing using search query surveillance: A case study in the United States. J. Med. Internet Res. 2016, 18, e5802. [Google Scholar] [CrossRef]
- Schootman, M.; Toor, A.; Cavazos-Rehg, P.; Jeffe, D.B.; McQueen, A.; Eberth, J.; Davidson, N.O. The utility of Google Trends data to examine interest in cancer screening. BMJ Open 2015, 5, e006678. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Dini, G.; Toletone, A.; Brigo, F.; Durando, P. Leveraging big data for exploring occupational diseases-related interest at the level of scientific community, media coverage and novel data streams: The example of silicosis as a pilot study. PLoS ONE 2016, 11, e0166051. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Watad, A.; Brigo, F.; Adawi, M.; Amital, H.; Shoenfeld, Y. Public health awareness of autoimmune diseases after the death of a celebrity. Clin. Rheumatol. 2017, 36, 1911–1917. [Google Scholar] [CrossRef]
- Gahr, M.; Uzelac, Z.; Zeiss, R.; Connemann, B.J.; Lang, D.; Schoenfeldt-Lecuona, C. Linking annual prescription volume of antidepressants to corresponding web search query data: A possible proxy for medical prescription behavior? J. Clin. Psychopharmacol. 2015, 35, 681–685. [Google Scholar] [CrossRef]
- Mavragani, A.; Sypsa, K.; Sampri, A.; Tsagarakis, K.P. Quantifying the UK online interest in substances of the EU watchlist for water monitoring: Diclofenac, estradiol, and the macrolide antibiotics. Water 2016, 8, 542. [Google Scholar] [CrossRef]
- Domnich, A.; Panatto, D.; Signori, A.; Lai, P.L.; Gasparini, R.; Amicizia, D. Age-related differences in the accuracy of web query-based predictions of influenza-like illness. PLoS ONE 2015, 10, e0127754. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.K.; Mehta, S.D. A comparison of Internet search trends and sexually transmitted infection rates using Google trends. Sex. Transm. Dis. 2014, 41, 61–63. [Google Scholar] [CrossRef]
- Wang, H.W.; Chen, D.R.; Yu, H.W.; Chen, Y.M. Forecasting the incidence of dementia and dementia-related outpatient visits with Google trends: Evidence from Taiwan. J. Med. Internet Res. 2015, 17, e264. [Google Scholar] [CrossRef]
- Crowson, M.G.; Schulz, K.; Tucci, D.L. National utilization and forecasting of ototopical antibiotics: Medicaid data versus “dr. google”. Otol. Neurotol. 2016, 37, 1049–1054. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Dini, G.; Toletone, A.; Brigo, F.; Durando, P. Infodemiological data concerning silicosis in the USA in the period 2004–2010 correlating with real-world statistical data. Data Brief 2017, 10, 457–464. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Bacigaluppi, S.; Robba, C.; Nardone, R.; Trinka, E.; Brigo, F. Infodemiology of status epilepticus: A systematic validation of the Google Trends-based search queries. Epilepsy Behav. 2016, 55, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Bragazzi, N.L. A Google Trends-based approach for monitoring NSSI. Psychol. Res. Behav. Manag. 2014, 7, 1. [Google Scholar] [CrossRef]
- Cavazos-Rehg, P.A.; Krauss, M.J.; Spitznagel, E.L.; Lowery, A.; Grucza, R.A.; Chaloupka, F.J.; Bierut, L.J. Monitoring of non-cigarette tobacco use using Google Trends. Tob. Control 2015, 24, 249–255. [Google Scholar] [CrossRef]
- Nuti, S.V.; Wayda, B.; Ranasinghe, I.; Wang, S.; Dreyer, R.P.; Chen, S.I.; Murugiah, K. The use of google trends in health care research: A systematic review. PLoS ONE 2014, 9, e109583. [Google Scholar] [CrossRef]
- Zhou, X.; Ye, J.; Feng, Y. Tuberculosis surveillance by analyzing Google trends. IEEE Trans. Biomed. Eng. 2011, 58, 2247–2254. [Google Scholar] [CrossRef] [PubMed]
- Rohart, F.; Milinovich, G.J.; Avril, S.M.; Lê Cao, K.A.; Tong, S.; Hu, W. Disease surveillance based on Internet-based linear models: An Australian case study of previously unmodeled infection diseases. Sci. Rep. 2016, 6, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Solano, P.; Ustulin, M.; Pizzorno, E.; Vichi, M.; Pompili, M.; Serafini, G.; Amore, M. A Google-based approach for monitoring suicide risk. Psychiatry Res. 2016, 246, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, H.A.; Mylonakis, E. Google trends: A web-based tool for real-time surveillance of disease outbreaks. Clin. Infect. Dis. 2009, 49, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- Uda, K.; Hagiya, H.; Yorifuji, T.; Koyama, T.; Tsuge, M.; Yashiro, M.; Tsukahara, H. Correlation Between National Surveillance and Search Engine Query Data on Respiratory Syncytial Virus Infections in Japan. Res. Sq. 2022. [Google Scholar] [CrossRef] [PubMed]
- Crowson, M.G.; Witsell, D.; Eskander, A. Using Google Trends to predict pediatric respiratory syncytial virus encounters at a major health care system. J. Med. Syst. 2020, 44, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Google Trends. Available online: https://trends.google.com/trends/ (accessed on 10 December 2022).
- NIID. IDWR Surveillance Data. Available online: https://www.niid.go.jp/niid/en/survaillance-data-table-english.html (accessed on 10 December 2022).
- Institute, R.K. Arbeitsgemeinschaft Influenza. Available online: https://influenza.rki.de (accessed on 10 December 2022).
- Sciensano. Weekly Flu Bulletin. Available online: https://www.sciensano.be/en/biblio/griep-bulletin-week-23-2022-bulletin-grippe-semaine-23-2022-weekly-flu-bulletin-week-23-2022 (accessed on 10 December 2022).
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef]
- World Health Organization. Pandemic Influenza Severity Assessment (PISA): A WHO Guide to Assess the Severity of Influenza in Seasonal Epidemics and Pandemics; Technical Report; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Vega, T.; Lozano, J.E.; Meerhoff, T.; Snacken, R.; Mott, J.; Ortiz de Lejarazu, R.; Nunes, B. Influenza surveillance in Europe: Establishing epidemic thresholds by the moving epidemic method. Influenza Other Respir. Viruses 2013, 7, 546–558. [Google Scholar] [CrossRef]
- Vega, T.; Lozano, J.E.; Meerhoff, T.; Snacken, R.; Beauté, J.; Jorgensen, P.; Ortiz de Lejarazu, R.; Domegan, L.; Mossong, J.; Nielsen, J.; et al. Influenza surveillance in E urope: Comparing intensity levels calculated using the moving epidemic method. Influenza Other Respir. Viruses 2015, 9, 234–246. [Google Scholar] [CrossRef]
- Broberg, E.K.; Waris, M.; Johansen, K.; Snacken, R.; Penttinen, P. Seasonality and geographical spread of respiratory syncytial virus epidemics in 15 European countries, 2010 to 2016. Eurosurveillance 2018, 23, 17-00284. [Google Scholar] [CrossRef]
- Bloom-Feshbach, K.; Alonso, W.J.; Charu, V.; Tamerius, J.; Simonsen, L.; Miller, M.A.; Viboud, C. Latitudinal variations in seasonal activity of influenza and respiratory syncytial virus (RSV): A global comparative review. PLoS ONE 2013, 8, e54445. [Google Scholar] [CrossRef] [PubMed]
- Obando-Pacheco, P.; Justicia-Grande, A.J.; Rivero-Calle, I.; Rodríguez-Tenreiro, C.; Sly, P.; Ramilo, O.; Mejías, A.; Baraldi, E.; Papadopoulos, N.G.; Nair, H.; et al. Respiratory syncytial virus seasonality: A global overview. J. Infect. Dis. 2018, 217, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Vos, L.M.; Teirlinck, A.C.; Lozano, J.E.; Vega, T.; Donker, G.A.; Hoepelman, A.I.; Bont, L.J.; Oosterheert, J.J.; Meijer, A. Use of the moving epidemic method (MEM) to assess national surveillance data for respiratory syncytial virus (RSV) in the Netherlands, 2005 to 2017. Eurosurveillance 2019, 24, 1800469. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.L.; Marques, D.F.; Cameron, R.L.; Potts, A.; Bishop, J.; von Wissmann, B.; William, N.; Reynolds, A.J.; Robertson, C.; McMenamin, J. Moving epidemic method (MEM) applied to virology data as a novel real time tool to predict peak in seasonal influenza healthcare utilisation. The Scottish experience of the 2017/18 season to date. Eurosurveillance 2018, 23, 18–00079. [Google Scholar] [CrossRef] [PubMed]
- Rakocevic, B.; Grgurevic, A.; Trajkovic, G.; Mugosa, B.; Grujicic, S.S.; Medenica, S.; Bojovic, O.; Alonso, J.E.L.; Vega, T. Influenza surveillance: Determining the epidemic threshold for influenza by using the Moving Epidemic Method (MEM), Montenegro, 2010/11 to 2017/18 influenza seasons. Eurosurveillance 2019, 24, 1800042. [Google Scholar] [CrossRef]
- Biggerstaff, M.; Kniss, K.; Jernigan, D.B.; Brammer, L.; Bresee, J.; Garg, S.; Burns, E.; Reed, C. Systematic assessment of multiple routine and near real-time indicators to classify the severity of influenza seasons and pandemics in the United States, 2003–2004 through 2015–2016. Am. J. Epidemiol. 2018, 187, 1040–1050. [Google Scholar] [CrossRef]
- Lozano, J.E. The Moving Epidemic Method Shiny Web Application. Available online: https://github.com/lozalojo/memapp (accessed on 10 December 2022).
- Burnett, E.; Parashar, U.D.; Winn, A.; Tate, J.E. Trends in Rotavirus Laboratory Detections and Internet Search Volume Before and After Rotavirus Vaccine Introduction and in the Context of the Coronavirus Disease 2019 Pandemic—United States, 2000–2021. J. Infect. Dis. 2022, 226, 967–974. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Japan | Germany | |||
|---|---|---|---|---|
| Data Source | Case | Google Trends | Case | Google Trends |
| Goodness (Matthews correlation coefficient) | 0.75 | 0.64 | 0.44 | 0.83 |
| Epidemic percentage | 61.03% | 54.76% | 71.95% | 75.28% |
| Average start week | 33 | 33 | 1 | 1 |
| Average length | 14 | 14 | 12 | 12 |
| Estimator | Surveillance | 2020–2021 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Country | Epidemic Percentage | Start Week | Aver. Length | Epidemic Threshold | Current (W25, 2022) | Above Threshold? | For How Long (Week)? | Start Week | End Week |
| Poland | 72.75 | 1 | 15 | 1.26 | 1.20 | NO | 38 | 50 | |
| Thailand | 62.33 | 31 | 15 | 4.02 | 1.06 | NO | 47 | 4 | |
| Turkey | 55.06 | 49 | 14 | 13.77 | 12.59 | NO | 40 | 1 | |
| New Zealand | 52.21 | 31 | 11 | 0.22 | 2.24 | YES | 11 | 36 | |
| Hungary | 44.25 | 6 | 12 | 4.46 | 3.51 | NO | 44 | 4 | |
| Philippines | 27.19 | 45 | 9 | 5.0 | 2.79 | NO | 33 | 37 | |
| Italy | 2.4 | 13 | 1 | 3.89 | 4.32 | YES | 40 | 51 | |
| Puerto Rico | 59.59 | 44 | 13 | 22.02 | 28.60 | YES | +1 | 45 | 2 |
| Greece | 34.97 | 2 | 10 | 23.93 | 10.52 | NO | 42 | 1 | |
| Malaysia | 22.19 | 33 | 7 | 40.45 | 79.61 | YES | +6 | 19 | now |
| Romania | 15.11 | 4 | 5 | 17.25 | 13.08 | NO | 35 | 35 | |
| Singapore | 9.27 | 26 | 3 | 21.12 | 88.83 | YES | +5 | 20 | now |
| Czechia | 8.5 | 5 | 3 | 36.16 | 27.30 | NO | 42 | 50 | |
| Mexico | 2.82 | 26 | 1 | 15.33 | 19.40 | NO | 31 | 37 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, D.; Guerra, A.; Wittke, F.; Lang, J.C.; Bakker, K.; Lee, A.W.; Finelli, L.; Chen, Y.-H. Real-Time Monitoring of Infectious Disease Outbreaks with a Combination of Google Trends Search Results and the Moving Epidemic Method: A Respiratory Syncytial Virus Case Study. Trop. Med. Infect. Dis. 2023, 8, 75. https://doi.org/10.3390/tropicalmed8020075
Wang D, Guerra A, Wittke F, Lang JC, Bakker K, Lee AW, Finelli L, Chen Y-H. Real-Time Monitoring of Infectious Disease Outbreaks with a Combination of Google Trends Search Results and the Moving Epidemic Method: A Respiratory Syncytial Virus Case Study. Tropical Medicine and Infectious Disease. 2023; 8(2):75. https://doi.org/10.3390/tropicalmed8020075
Chicago/Turabian StyleWang, Dawei, Andrea Guerra, Frederick Wittke, John Cameron Lang, Kevin Bakker, Andrew W. Lee, Lyn Finelli, and Yao-Hsuan Chen. 2023. "Real-Time Monitoring of Infectious Disease Outbreaks with a Combination of Google Trends Search Results and the Moving Epidemic Method: A Respiratory Syncytial Virus Case Study" Tropical Medicine and Infectious Disease 8, no. 2: 75. https://doi.org/10.3390/tropicalmed8020075
APA StyleWang, D., Guerra, A., Wittke, F., Lang, J. C., Bakker, K., Lee, A. W., Finelli, L., & Chen, Y.-H. (2023). Real-Time Monitoring of Infectious Disease Outbreaks with a Combination of Google Trends Search Results and the Moving Epidemic Method: A Respiratory Syncytial Virus Case Study. Tropical Medicine and Infectious Disease, 8(2), 75. https://doi.org/10.3390/tropicalmed8020075