

Mpox, Caused by the MPXV of the Clade IIb Lineage, Goes Global


Abstract
1. Introduction
2. Methods
2.1. Data Sources
2.2. Phylogenetic Analysis of 175 Genomes of MPXV
3. Results
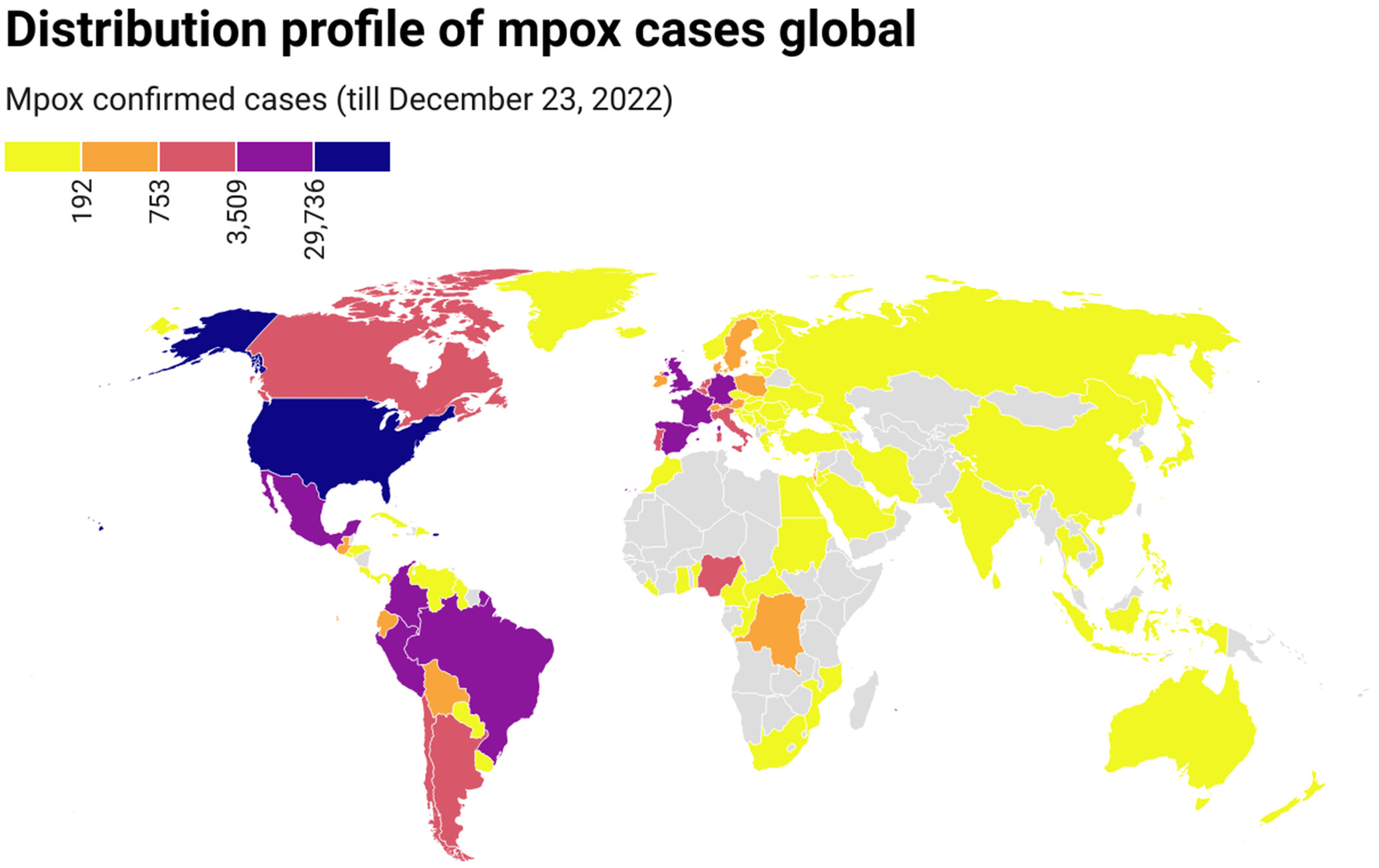
3.1. Persistent Geographic Expansion of Mpox Worldwide
3.2. Age, Clinical Symptoms, and Transmission Profile in Available Data
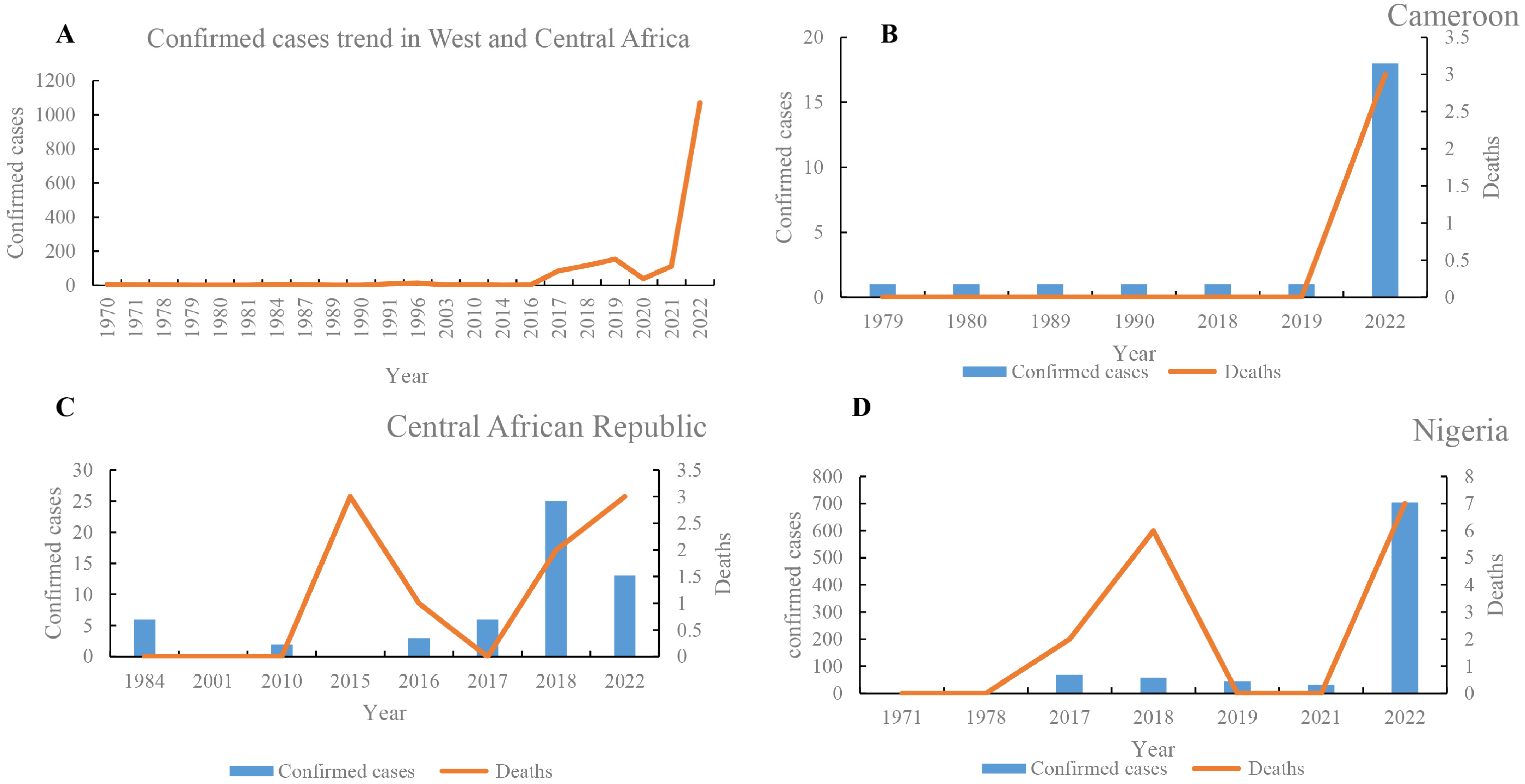
3.3. Trends of Mpox Cases in West and Central Africa
3.4. The Role of West African Mpox in the Global Spread
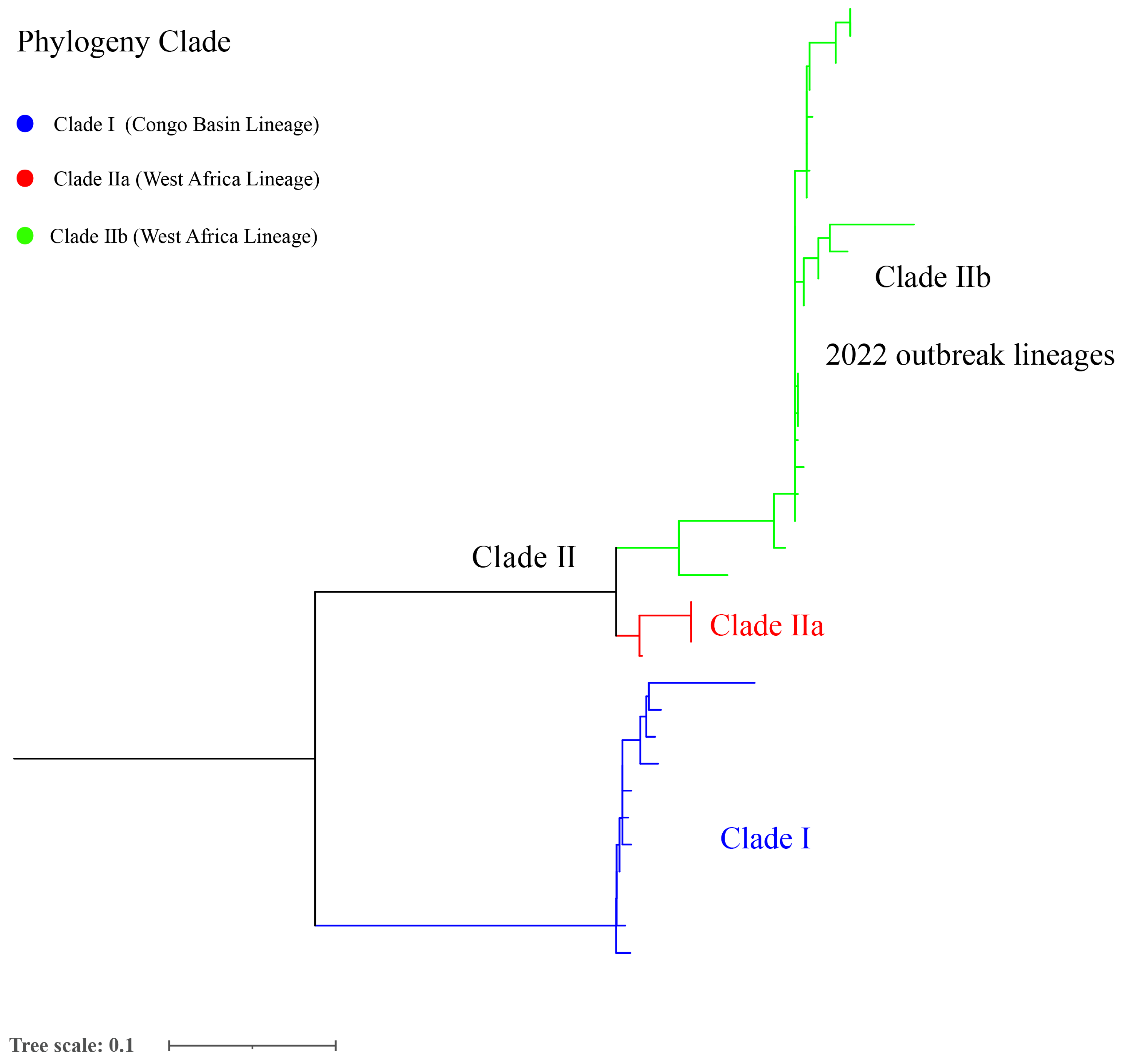
3.5. Geographical Distribution and Host Distribution of Mpox Genomes and Phylogenetic Analysis
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Damon, I.K. Status of human monkeypox: Clinical disease, epidemiology and research. Vaccine 2011, 29 (Suppl. S4), D54–D59. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.; Abubakar, I.; Ihekweazu, C.; Heymann, D.; Ntoumi, F.; Blumberg, L.; Asogun, D.; Mukonka, V.; Lule, S.A.; Bates, M.; et al. Monkeypox-Enhancing public health preparedness for an emerging lethal human zoonotic epidemic threat in the wake of the smallpox post-eradication era. Int. J. Infect. Dis. 2019, 78, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, A.; Adhikari, S.; Kaya, D.; Islam, M.A.; Malla, B.; Sherchan, S.P.; Al-Mustapha, A.I.; Kumar, M.; Aggarwal, S.; Bhattacharya, P.; et al. Monkeypox outbreak: Wastewater and environmental surveillance perspective. Sci. Total Environ. 2023, 856, 159166. [Google Scholar] [CrossRef]
- Foster, S.O.; Brink, E.W.; Hutchins, D.L.; Pifer, J.M.; Lourie, B.; Moser, C.R.; Cummings, E.C.; Kuteyi, O.E.; Eke, R.E.; Titus, J.B.; et al. Human monkeypox. Bull. World Health Organ. 1972, 46, 569–576. [Google Scholar] [PubMed]
- Ladnyj, I.D.; Ziegler, P.; Kima, E. A human infection caused by monkeypox virus in Basankusu Territory, Democratic Republic of the Congo. Bull. World Health Organ. 1972, 46, 593–597. [Google Scholar] [PubMed]
- Mahase, E. Monkeypox: What do we know about the outbreaks in Europe and North America? BMJ 2022, 377, o1274. [Google Scholar] [CrossRef]
- Jezek, Z.; Szczeniowski, M.; Paluku, K.M.; Mutombo, M. Human monkeypox: Clinical features of 282 patients. J. Infect. Dis. 1987, 156, 293–298. [Google Scholar] [CrossRef]
- WHO. 2022 Mpox (Monkeypox) Outbreak: Global Trends; WHO: Geneva, Switzerland, 2023. [Google Scholar]
- Islam, M.A.; Sangkham, S.; Tiwari, A.; Vadiati, M.; Hasan, M.N.; Noor, S.T.A.; Mumin, J.; Bhattacharya, P.; Sherchan, S.P. Association between Global Monkeypox Cases and Meteorological Factors. Int. J. Environ. Res. Public Health 2022, 19, 5638. [Google Scholar] [CrossRef]
- Chakraborty, S.; Mohapatra, R.K.; Chandran, D.; Alagawany, M.; Sv, P.; Islam, M.A.; Chakraborty, C.; Dhama, K. Monkeypox vaccines and vaccination strategies: Current knowledge and advances. An update - Correspondence. Int. J. Surg. 2022, 105, 106869. [Google Scholar] [CrossRef]
- Rizk, J.G.; Lippi, G.; Henry, B.M.; Forthal, D.N.; Rizk, Y. Prevention and Treatment of Monkeypox. Drugs 2022, 82, 957–963. [Google Scholar] [CrossRef]
- Brown, K.; Leggat, P.A. Human Monkeypox: Current State of Knowledge and Implications for the Future. Trop. Med. Infect. Dis. 2016, 1, 8. [Google Scholar] [CrossRef] [PubMed]
- McCollum, A.M.; Damon, I.K. Human Monkeypox. Clinical Infectious Diseases 2013, 58, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Khodakevich, L.; Jezek, Z.; Messinger, D. Monkeypox virus: Ecology and public health significance. Bull. World Health Organ. 1988, 66, 747–752. [Google Scholar] [PubMed]
- Petersen, E.; Kantele, A.; Koopmans, M.; Asogun, D.; Yinka-Ogunleye, A.; Ihekweazu, C.; Zumla, A. Human Monkeypox: Epidemiologic and Clinical Characteristics, Diagnosis, and Prevention. Infect. Dis. Clin. North Am. 2019, 33, 1027–1043. [Google Scholar] [CrossRef]
- Happi, C.; Adetifa, I.; Mbala, P.; Njouom, R.; Nakoune, E.; Happi, A.; Ndodo, N.; Ayansola, O.; Mboowa, G.; Bedford, T.; et al. Urgent need for a non-discriminatory and non-stigmatizing nomenclature for monkeypox virus. PLoS Biol. 2022, 20, e3001769. [Google Scholar] [CrossRef]
- Alakunle, E.; Moens, U.; Nchinda, G.; Okeke, M.I. Monkeypox Virus in Nigeria: Infection Biology, Epidemiology, and Evolution. Viruses 2020, 12, 1257. [Google Scholar] [CrossRef]
- Kozlov, M. Monkeypox goes global: Why scientists are on alert. Nature 2022, 606, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.; Phillippy, A.; Delcher, A.L.; Smoot, M.; Shumway, M.; Antonescu, C.; Salzberg, S.L. Versatile and open software for comparing large genomes. Genome Biol. 2004, 5, R12. [Google Scholar] [CrossRef]
- Chiaromonte, F.; Yap, V.B.; Miller, W. Scoring pairwise genomic sequence alignments. In Proceedings of the Pacific Symposium on Biocomputing 2002, Kauai, HI, USA, 3–7 January 2002; pp. 115–126. [Google Scholar] [CrossRef]
- Letunic, I.; Bork, P. Interactive Tree Of Life (iTOL) v5: An online tool for phylogenetic tree display and annotation. Nucleic Acids Res. 2021, 49, W293–W296. [Google Scholar] [CrossRef]
- Mahase, E. Seven monkeypox cases are confirmed in England. BMJ 2022, 377, o1239. [Google Scholar] [CrossRef]
- Moyo, E.; Musuka, G.; Murewanhema, G.; Moyo, P.; Dzinamarira, T. Monkeypox outbreak: A perspective on Africa’s diagnostic and containment capacity. Int J Infect Dis 2022, 123, 127–130. [Google Scholar] [CrossRef]
- WHO. Monkeypox-United States of America; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- WHO. Outbreaks and Emergencies Bulletin, Week 25: 13-19 June 2022; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Reynolds, M.G.; Yorita, K.L.; Kuehnert, M.J.; Davidson, W.B.; Huhn, G.D.; Holman, R.C.; Damon, I.K. Clinical manifestations of human monkeypox influenced by route of infection. J. Infect. Dis. 2006, 194, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Erez, N.; Achdout, H.; Milrot, E.; Schwartz, Y.; Wiener-Well, Y.; Paran, N.; Politi, B.; Tamir, H.; Israely, T.; Weiss, S.; et al. Diagnosis of Imported Monkeypox, Israel, 2018. Emerg. Infect. Dis. 2019, 25, 980–983. [Google Scholar] [CrossRef]
- Vaughan, A.; Aarons, E.; Astbury, J.; Balasegaram, S.; Beadsworth, M.; Beck, C.R.; Chand, M.; O’Connor, C.; Dunning, J.; Ghebrehewet, S.; et al. Two cases of monkeypox imported to the United Kingdom, September 2018. Euro Surveill. 2018, 23. [Google Scholar] [CrossRef]
- England, P.H. Monkeypox Case Confirmed in England. Available online: https://www.gov.uk/government/news/monkeypox-case-confirmed-in-england (accessed on 4 December 2019).
- Hobson, G.; Adamson, J.; Adler, H.; Firth, R.; Gould, S.; Houlihan, C.; Johnson, C.; Porter, D.; Rampling, T.; Ratcliffe, L.; et al. Family cluster of three cases of monkeypox imported from Nigeria to the United Kingdom, May 2021. Euro Surveill. 2021, 26. [Google Scholar] [CrossRef]
- UK Health Security Agency. Monkeypox Cases Confirmed in England–Latest Updates; UK Health Security Agency: London, UK, 2022. [Google Scholar]
- Kyaw, W.M.; Vasoo, S.; Ho, H.J.A.; Chan, M.; Yeo, T.W.; Manauis, C.M.; Ang, H.; Pratim De, P.; Ang, B.S.P.; Chow, A.L.P. Monitoring healthcare professionals after monkeypox exposure: Experience from the first case imported to Asia. Infect. Control Hosp. Epidemiol. 2020, 41, 373–375. [Google Scholar] [CrossRef]
- Rao, A.K.; Schulte, J.; Chen, T.H.; Hughes, C.M.; Davidson, W.; Neff, J.M.; Markarian, M.; Delea, K.C.; Wada, S.; Liddell, A.; et al. Monkeypox in a Traveler Returning from Nigeria - Dallas, Texas, July 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Costello, V.; Sowash, M.; Gaur, A.; Cardis, M.; Pasieka, H.; Wortmann, G.; Ramdeen, S. Imported Monkeypox from International Traveler, Maryland, USA, 2021. Emerg. Infect. Dis. 2022, 28, 1002–1005. [Google Scholar] [CrossRef] [PubMed]
- The UAE’s Ministry of Health. UAE Reports First Case of Monkeypox in the Gulf. Available online: https://english.alarabiya.net/News/gulf/2022/05/24/UAE-reports-first-case-of-monkeypox-in-the-country (accessed on 22 May 2015).
- Lynch, J. Virginia Reports First Presumed Case of Monkeypox. Available online: https://wfirnews.com/news/virginia-reports-first-presumed-case-of-monkeypox (accessed on 27 May 2022).
- León-Figueroa, D.A.; Bonilla-Aldana, D.K.; Pachar, M.; Romaní, L.; Saldaña-Cumpa, H.M.; Anchay-Zuloeta, C.; Diaz-Torres, M.; Franco-Paredes, C.; Suárez, J.A.; Ramirez, J.D.; et al. The never-ending global emergence of viral zoonoses after COVID-19? The rising concern of monkeypox in Europe, North America and beyond. Travel Med. Infect. Dis. 2022, 49, 102362. [Google Scholar] [CrossRef]
- Tambo, E.; Al-Nazawi, A.M. Combating the global spread of poverty-related Monkeypox outbreaks and beyond. Infect. Dis. Poverty 2022, 11, 80. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Confidence in managing human monkeypox cases in Asia: A cross-sectional survey among general practitioners in Indonesia. Acta Trop. 2020, 206, 105450. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, R.P.; Dessie, Z.G.; Noreddin, A.; El Zowalaty, M.E. Systematic Review of Important Viral Diseases in Africa in Light of the ’One Health’ Concept. Pathogens 2020, 9, 301. [Google Scholar] [CrossRef] [PubMed]
- Dhama, K.; Chandran, D.; Chakraborty, S.; Yatoo, M.I.; Islam, M.A.; Bhattacharya, M.; Chakraborty, C.; Harapan, H.; Chaicumpa, W. Zoonotic concerns of Marburg virus: Current knowledge and counteracting strategies including One Health approach to limit animal-human interface: An update. Int. J. Surg. 2022, 106, 106941. [Google Scholar] [CrossRef]
- Chakraborty, S.; Chandran, D.; Mohapatra, R.K.; Islam, M.A.; Alagawany, M.; Bhattacharya, M.; Chakraborty, C.; Dhama, K. Langya virus, a newly identified Henipavirus in China - Zoonotic pathogen causing febrile illness in humans, and its health concerns: Current knowledge and counteracting strategies – Correspondence. Int. J. Surg. 2022, 105, 106882. [Google Scholar] [CrossRef]
- Islam, M.A.; Haque, M.A.; Rahman, M.A.; Hossen, F.; Reza, M.; Barua, A.; Marzan, A.A.; Das, T.; Kumar Baral, S.; He, C.; et al. A Review on Measures to Rejuvenate Immune System: Natural Mode of Protection Against Coronavirus Infection. Front. Immunol. 2022, 13, 837290. [Google Scholar] [CrossRef]
- Jakariya, M.; Ahmed, F.; Islam, M.A.; Al Marzan, A.; Hasan, M.N.; Hossain, M.; Ahmed, T.; Hossain, A.; Reza, H.M.; Hossen, F.; et al. Wastewater-based epidemiological surveillance to monitor the prevalence of SARS-CoV-2 in developing countries with onsite sanitation facilities. Environ. Pollut. 2022, 311, 119679. [Google Scholar] [CrossRef]
- Islam, M.A.; Hossen, F.; Rahman, M.A.; Sultana, K.F.; Hasan, M.N.; Haque, M.A.; Sosa-Hernández, J.E.; Oyervides-Muñoz, M.A.; Parra-Saldívar, R.; Ahmed, T.; et al. An opinion on Wastewater-Based Epidemiological Monitoring (WBEM) with Clinical Diagnostic Test (CDT) for detecting high-prevalence areas of community COVID-19 infections. Curr. Opin. Environ. Sci. Health 2023, 31, 100396. [Google Scholar] [CrossRef]
- Ahmed, F.; Islam, M.A.; Kumar, M.; Hossain, M.; Bhattacharya, P.; Islam, M.T.; Hossen, F.; Hossain, M.S.; Islam, M.S.; Uddin, M.M.; et al. First detection of SARS-CoV-2 genetic material in the vicinity of COVID-19 isolation Centre in Bangladesh: Variation along the sewer network. Sci. Total Environ. 2021, 776, 145724. [Google Scholar] [CrossRef] [PubMed]
- Hemati, S.; Mohammadi-Moghadam, F. A systematic review on environmental perspectives of monkeypox virus. Rev. Environ. Health, 2023; ahead of print. [Google Scholar] [CrossRef]
- El Eid, R.; Allaw, F.; Haddad, S.F.; Kanj, S.S. Human monkeypox: A review of the literature. PLoS Pathog. 2022, 18, e1010768. [Google Scholar] [CrossRef] [PubMed]
- Al-Mandhari, A.; Kodama, C.; Abubakar, A.; Hajjeh, R.; Brennan, R. Monkeypox outbreak and response efforts in the Eastern Mediterranean Region. East Mediterr. Health J. 2022, 28, 465–468. [Google Scholar] [CrossRef] [PubMed]
- Kumbhar, N.; Agarwala, P. The lurking threat of monkeypox in current times. Indian J. Med. Microbiol. 2022, 40, 475–476. [Google Scholar] [CrossRef] [PubMed]
- Souza, M.J. One health: Zoonoses in the exotic animal practice. Vet. Clin. North Am. Exot. Anim. Pract. 2011, 14, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Isidro, J.; Borges, V.; Pinto, M.; Sobral, D.; Santos, J.D.; Nunes, A.; Mixão, V.; Ferreira, R.; Santos, D.; Duarte, S.; et al. Phylogenomic characterization and signs of microevolution in the 2022 multi-country outbreak of monkeypox virus. Nat. Med. 2022, 28, 1569–1572. [Google Scholar] [CrossRef] [PubMed]
- Kugelman, J.R.; Johnston, S.C.; Mulembakani, P.M.; Kisalu, N.; Lee, M.S.; Koroleva, G.; McCarthy, S.E.; Gestole, M.C.; Wolfe, N.D.; Fair, J.N.; et al. Genomic variability of monkeypox virus among humans, Democratic Republic of the Congo. Emerg. Infect. Dis. 2014, 20, 232–239. [Google Scholar] [CrossRef]
- Forni, D.; Molteni, C.; Cagliani, R.; Sironi, M. Geographic structuring and divergence time frame of monkeypox virus in the endemic region. J. Infect. Dis. 2022; ahead of print. [Google Scholar] [CrossRef]
- Kindrachuk, J.; Arsenault, R.; Kusalik, A.; Kindrachuk, K.N.; Trost, B.; Napper, S.; Jahrling, P.B.; Blaney, J.E. Systems kinomics demonstrates Congo Basin monkeypox virus infection selectively modulates host cell signaling responses as compared to West African monkeypox virus. Mol. Cell Proteom. 2012, 11, M111.015701. [Google Scholar] [CrossRef]
- Realegeno, S.; Puschnik, A.S.; Kumar, A.; Goldsmith, C.; Burgado, J.; Sambhara, S.; Olson, V.A.; Carroll, D.; Damon, I.; Hirata, T.; et al. Monkeypox Virus Host Factor Screen Using Haploid Cells Identifies Essential Role of GARP Complex in Extracellular Virus Formation. J. Virol. 2017, 91. [Google Scholar] [CrossRef]
- Yinka-Ogunleye, A.; Aruna, O.; Dalhat, M.; Ogoina, D.; McCollum, A.; Disu, Y.; Mamadu, I.; Akinpelu, A.; Ahmad, A.; Burga, J.; et al. Outbreak of human monkeypox in Nigeria in 2017-18: A clinical and epidemiological report. Lancet Infect. Dis. 2019, 19, 872–879. [Google Scholar] [CrossRef]
- Schlagenhauf, P.; Weld, L.; Goorhuis, A.; Gautret, P.; Weber, R.; von Sonnenburg, F.; Lopez-Vélez, R.; Jensenius, M.; Cramer, J.P.; Field, V.K.; et al. Travel-associated infection presenting in Europe (2008-12): An analysis of EuroTravNet longitudinal, surveillance data, and evaluation of the effect of the pre-travel consultation. Lancet Infect. Dis. 2015, 15, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Kiang, M.V.; Chin, E.T.; Huynh, B.Q.; Chapman, L.A.C.; Rodríguez-Barraquer, I.; Greenhouse, B.; Rutherford, G.W.; Bibbins-Domingo, K.; Havlir, D.; Basu, S.; et al. Routine asymptomatic testing strategies for airline travel during the COVID-19 pandemic: A simulation study. Lancet Infect. Dis. 2021, 21, 929–938. [Google Scholar] [CrossRef]
- Hutin, Y.J.F.; Williams, R.J.; Malfait, P.; Pebody, R.; Loparev, V.; Ropp, S.; Rodriguez, M.; Knight, J.C.; Tshioko, F.; Khan, A.S.; et al. Outbreak of Human Monkeypox, Democratic Republic of Congo, 1996 to 1997. Emerg. Infect. Dis. J. 2001, 7, 434. [Google Scholar] [CrossRef]
- Salzer, J.S.; Carroll, D.S.; Rwego, I.B.; Li, Y.; Falendysz, E.A.; Shisler, J.L.; Karem, K.L.; Damon, I.K.; Gillespie, T.R. Serologic evidence for circulating orthopoxviruses in peridomestic rodents from rural Uganda. J. Wildl. Dis. 2013, 49, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Perez Duque, M.; Ribeiro, S.; Martins, J.V.; Casaca, P.; Leite, P.P.; Tavares, M.; Mansinho, K.; Duque, L.M.; Fernandes, C.; Cordeiro, R.; et al. Ongoing monkeypox virus outbreak, Portugal, 29 April to 23 May 2022. Euro Surveill. 2022, 27. [Google Scholar] [CrossRef]
- Riopelle, J.C.; Munster, V.J.; Port, J.R. Atypical and Unique Transmission of Monkeypox Virus during the 2022 Outbreak: An Overview of the Current State of Knowledge. Viruses 2022, 14, 2012. [Google Scholar] [CrossRef]
- Hemati, S.; Farhadkhani, M.; Sanami, S.; Mohammadi-Moghadam, F. A review on insights and lessons from COVID-19 to the prevent of monkeypox pandemic. Travel Med. Infect. Dis. 2022, 50, 102441. [Google Scholar] [CrossRef]
- Dimitrakoff, J. Monkeypox Virus Infection across 16 Countries-April-June 2022. N. Engl. J. Med. 2022, 387, e69. [Google Scholar] [CrossRef]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: A prospective observational cohort study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef]
- Sklenovská, N.; Van Ranst, M. Emergence of Monkeypox as the Most Important Orthopoxvirus Infection in Humans. Front. Public Health 2018, 6, 241. [Google Scholar] [CrossRef]
- Luna, N.; Ramírez, A.L.; Muñoz, M.; Ballesteros, N.; Patiño, L.H.; Castañeda, S.A.; Bonilla-Aldana, D.K.; Paniz-Mondolfi, A.; Ramírez, J.D. Phylogenomic analysis of the monkeypox virus (MPXV) 2022 outbreak: Emergence of a novel viral lineage? Travel Med. Infect. Dis. 2022, 49, 102402. [Google Scholar] [CrossRef] [PubMed]
- Antunes, F.; Virgolino, A. Monkeypox Mysteries of the New Outbreak in Non-Endemic Areas. Int. J. Environ. Res. Public Health 2022, 19, 4881. [Google Scholar] [CrossRef] [PubMed]
- Desingu, P.A.; Rubeni, T.P.; Sundaresan, N.R. Evolution of monkeypox virus from 2017 to 2022: In the light of point mutations. Front. Microbiol. 2022, 13, 1037598. [Google Scholar] [CrossRef] [PubMed]
- Jolly, B.; Scaria, V. A distinct phylogenetic cluster of Monkeypox genomes suggests an early and cryptic spread of the virus. J. Infect. 2023, 86, e24–e26. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Zheng, C.; Shi, Q.; Wang, L.; Tia, A.; Ngobeh, J.; Liu, Z.; Dong, X.; Li, Z. Multiple introduced lineages and the single native lineage co-driving the four waves of the COVID-19 pandemic in West Africa. Front Public Health 2022, 10, 957277. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Export Pattern | ID | Exporting Country | Importing Country | Time | No. | Transmission Route (Potential) | Ref. |
|---|---|---|---|---|---|---|---|
| Exported in Africa | 1 | DRC | South Sudan | 2005 | 10 | Unknown | [24] |
| 2 | Congo | 2010 | 2 | Refugee migration | [24] | ||
| 3 | Nigeria | Benin | 1978 | 1 | Close contact with a confirmed case | [24] | |
| 4 | 2022.6 | 1 | Travel history | [25] | |||
| 5 | 2022.6 | 1 | Travel history | [25] | |||
| Exported outside Africa | 1 | Ghana | USA | 2003 | 47 | Close contact with pet dogs | [26] |
| 2 | Nigeria | Israel | 2018.9.17 | 1 | Travel history | [27] | |
| 3 | UK | 2018.9.7 | 1 | Travel history | [28] | ||
| 4 | 2018.9.11 | 1 | Travel history | [28] | |||
| 5 | 2018.9.26 | 1 | Close contact with a confirmed case | [28] | |||
| 6 | 2019.12 | 1 | Travel history | [29] | |||
| 7 | 2021.5.25 | 1 | Travel history | [30] | |||
| 8 | 2021.5.31 | 1 | Travel history | [30] | |||
| 9 | 2021.6.15 | 1 | Travel history | [30] | |||
| 10 | 2022.5.6 | 1 | Travel history | [31] | |||
| 11 | Singapore | 2019.5.8 | 1 | Travel history | [32] | ||
| 12 | USA | 2021.7.15 | 1 | Travel history | [33] | ||
| 13 | 2021.11.16 | 1 | Travel history | [34] | |||
| 14 | WA | United Arab Emirates | 2022.5.24 | 1 | Travel history | [35] | |
| 15 | Africa | USA | 2022.5.26 | 1 | Travel history | [36] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, L.; Shi, Q.; Dong, X.; Wang, M.; Liu, Z.; Li, Z. Mpox, Caused by the MPXV of the Clade IIb Lineage, Goes Global. Trop. Med. Infect. Dis. 2023, 8, 76. https://doi.org/10.3390/tropicalmed8020076
Gao L, Shi Q, Dong X, Wang M, Liu Z, Li Z. Mpox, Caused by the MPXV of the Clade IIb Lineage, Goes Global. Tropical Medicine and Infectious Disease. 2023; 8(2):76. https://doi.org/10.3390/tropicalmed8020076
Chicago/Turabian StyleGao, Liping, Qi Shi, Xiaoping Dong, Miao Wang, Zhiguo Liu, and Zhenjun Li. 2023. "Mpox, Caused by the MPXV of the Clade IIb Lineage, Goes Global" Tropical Medicine and Infectious Disease 8, no. 2: 76. https://doi.org/10.3390/tropicalmed8020076
APA StyleGao, L., Shi, Q., Dong, X., Wang, M., Liu, Z., & Li, Z. (2023). Mpox, Caused by the MPXV of the Clade IIb Lineage, Goes Global. Tropical Medicine and Infectious Disease, 8(2), 76. https://doi.org/10.3390/tropicalmed8020076