
Diagnostic Performance of Dengue NS1 and Antibodies by Serum Concentration Technique

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Specimens
2.2. Quantitative Reverse Transcription Polymerase Chain Reaction (qRT-PCR)
2.3. Serology
2.4. Concentration Method
2.5. Ethical Approval
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Diagnostic Performance of Tests
3.2.1. ELISA and RDT: Pre-Concentration (Pre-Con) Specimens
3.2.2. ELISA and RDT: Post-Concentrated (Post-Con) Specimens
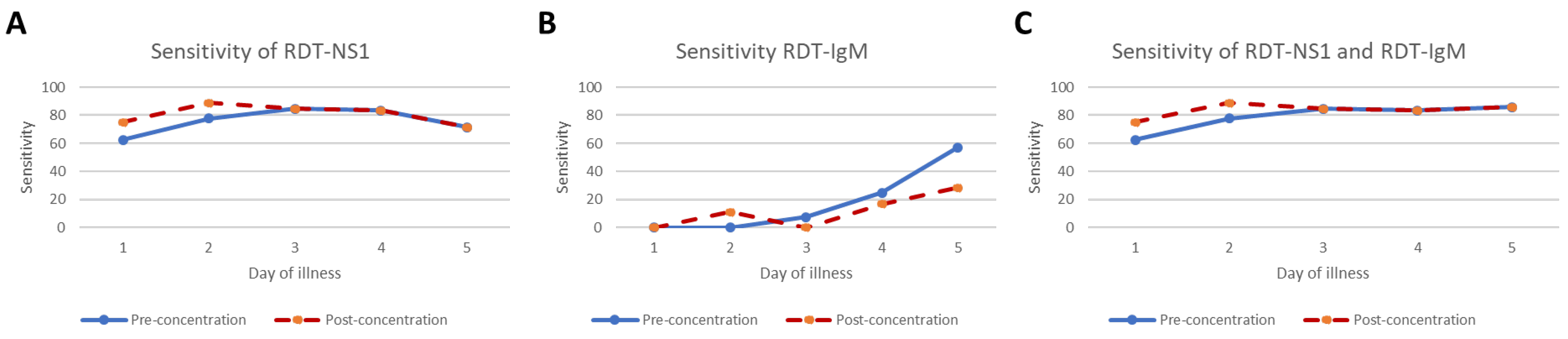
3.2.3. ELISA and RDT Sensitivity by Day of Onset of Illness: Pre- and Post-Con Specimens
3.3. The Results of False Negative RDT on NS1 Ag and DEV IgM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zeng, Z.; Zhan, J.; Chen, L.; Chen, H.; Cheng, S. Global, regional, and national dengue burden from 1990 to 2017: A systematic analysis based on the global burden of disease study 2017. EClinicalMedicine 2021, 32, 100712. [Google Scholar] [CrossRef] [PubMed]
- Simmons, C.P.; Farrar, J.J.; van Vinh Chau, N.; Wills, B. Dengue. N. Engl. J. Med. 2012, 366, 1423–1432. [Google Scholar] [CrossRef] [PubMed]
- Blacksell, S.D. Commercial dengue rapid diagnostic tests for point-of-care application: Recent evaluations and future needs? J. Biomed. Biotechnol. 2012, 2012, 151967. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, W.; Wang, J.; Peng, H.; Che, X.; Chen, X.; Zhou, Y. NS1-based tests with diagnostic utility for confirming dengue infection: A meta-analysis. Int. J. Infect. Dis. 2014, 26, 57–66. [Google Scholar] [CrossRef]
- Nisalak, A. Laboratory Diagnosis of Dengue Virus Infections. Southeast Asian J. Trop. Med. Public Health 2015, 46 (Suppl. S1), 55–76. [Google Scholar]
- Wang, S.M.; Sekaran, S.D. Early diagnosis of Dengue infection using a commercial Dengue Duo rapid test kit for the detection of NS1, IGM, and IGG. Am. J. Trop. Med. Hyg. 2010, 83, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Fishman, J.B.; Berg, E.A. Ammonium Sulfate Fractionation of Antibodies. Cold Spring Harb. Protoc. 2018, 2018, 472–474. [Google Scholar] [CrossRef] [PubMed]
- Tscheliessnig, A.; Satzer, P.; Hammerschmidt, N.; Schulz, H.; Helk, B.; Jungbauer, A. Ethanol precipitation for purification of recombinant antibodies. J. Biotechnol. 2014, 188, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Ho, N.T.; Fan, A.; Klapperich, C.M.; Cabodi, M. Sample concentration and purification for point-of-care diagnostics. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 2396–2399. [Google Scholar] [CrossRef]
- Russell, B.J.; Velez, J.O.; Laven, J.J.; Johnson, A.J.; Chang, G.J.; Johnson, B.W. A comparison of concentration methods applied to non-infectious flavivirus recombinant antigens for use in diagnostic serological assays. J. Virol. Methods 2007, 145, 62–70. [Google Scholar] [CrossRef]
- Luvira, V.; Silachamroon, U.; Piyaphanee, W.; Lawpoolsri, S.; Chierakul, W.; Leaungwutiwong, P.; Thawornkuno, C.; Wattanagoon, Y. Etiologies of Acute Undifferentiated Febrile Illness in Bangkok, Thailand. Am. J. Trop. Med. Hyg. 2019, 100, 622–629. [Google Scholar] [CrossRef]
- Negida, A.; Fahim, N.K.; Negida, Y. Sample Size Calculation Guide—Part 4: How to Calculate the Sample Size for a Diagnostic Test Accuracy Study based on Sensitivity, Specificity, and the Area under the ROC Curve. Adv. J. Emerg. Med. 2019, 3, e33. [Google Scholar] [CrossRef] [PubMed]
- Poltep, K.; Phadungsombat, J.; Nakayama, E.E.; Kosoltanapiwat, N.; Hanboonkunupakarn, B.; Wiriyarat, W.; Shioda, T.; Leaungwutiwong, P. Genetic Diversity of Dengue Virus in Clinical Specimens from Bangkok, Thailand, during 2018–2020: Co-Circulation of All Four Serotypes with Multiple Genotypes and/or Clades. Trop. Med. Infect. Dis. 2021, 6, 162. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Ryu, J.H.; Park, H.S.; Park, K.H.; Bae, H.; Yun, S.; Choi, A.R.; Cho, S.Y.; Park, C.; Lee, D.G.; et al. Comparison of Six Commercial Diagnostic Tests for the Detection of Dengue Virus Non-Structural-1 Antigen and IgM/IgG Antibodies. Ann. Lab. Med. 2019, 39, 566–571. [Google Scholar] [CrossRef]
- Jang, W.S.; Kwak, S.Y.; May, W.L.; Yang, D.J.; Nam, J.; Lim, C.S. Comparative evaluation of three dengue duo rapid test kits to detect NS1, IgM, and IgG associated with acute dengue in children in Myanmar. PLoS ONE 2019, 14, e0213451. [Google Scholar] [CrossRef]
- Hunsperger, E.A.; Yoksan, S.; Buchy, P.; Nguyen, V.C.; Sekaran, S.D.; Enria, D.A.; Vazquez, S.; Cartozian, E.; Pelegrino, J.L.; Artsob, H.; et al. Evaluation of commercially available diagnostic tests for the detection of dengue virus NS1 antigen and anti-dengue virus IgM antibody. PLoS Negl. Trop. Dis. 2014, 8, e3171. [Google Scholar] [CrossRef]
- Hang, V.T.; Nguyet, N.M.; Trung, D.T.; Tricou, V.; Yoksan, S.; Dung, N.M.; Van Ngoc, T.; Hien, T.T.; Farrar, J.; Wills, B.; et al. Diagnostic accuracy of NS1 ELISA and lateral flow rapid tests for dengue sensitivity, specificity and relationship to viraemia and antibody responses. PLoS Negl. Trop. Dis. 2009, 3, e360. [Google Scholar] [CrossRef]
- Mahapatra, D.; Sarangi, G.; Mahapatra, A.; Paty, B.P.; Das, P.; Chayani, N. NS1 Antigen Capture ELISA an Effective Method for Diagnosis of Early Dengue Infection—Report of an Outbreak at Angul District, Odisha, India. J. Clin. Diagn. Res. 2014, 8, DC08–DC10. [Google Scholar] [CrossRef] [PubMed]
- Moi, M.L.; Omatsu, T.; Tajima, S.; Lim, C.K.; Kotaki, A.; Ikeda, M.; Harada, F.; Ito, M.; Saijo, M.; Kurane, I.; et al. Detection of dengue virus nonstructural protein 1 (NS1) by using ELISA as a useful laboratory diagnostic method for dengue virus infection of international travelers. J. Travel Med. 2013, 20, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Haider, M.; Yousaf, S.; Zaib, A.; Sarfraz, A.; Sarfraz, Z.; Cherrez-Ojeda, I. Diagnostic Accuracy of Various Immunochromatographic Tests for NS1 Antigen and IgM Antibodies Detection in Acute Dengue Virus Infection. Int. J. Environ. Res. Public Health 2022, 19, 8756. [Google Scholar] [CrossRef] [PubMed]
- Vongpunsawad, S.; Intharasongkroh, D.; Thongmee, T.; Poovorawan, Y. Seroprevalence of antibodies to dengue and chikungunya viruses in Thailand. PLoS ONE 2017, 12, e0180560. [Google Scholar] [CrossRef]
- Blacksell, S.D.; Jarman, R.G.; Bailey, M.S.; Tanganuchitcharnchai, A.; Jenjaroen, K.; Gibbons, R.V.; Paris, D.H.; Premaratna, R.; de Silva, H.J.; Lalloo, D.G.; et al. Evaluation of six commercial point-of-care tests for diagnosis of acute dengue infections: The need for combining NS1 antigen and IgM/IgG antibody detection to achieve acceptable levels of accuracy. Clin. Vaccine Immunol. 2011, 18, 2095–2101. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.F.; Galula, J.U.; Chang, G.J.; Wu, H.C.; King, C.C.; Chao, D.Y. Improving dengue viral antigens detection in dengue patient serum specimens using a low pH glycine buffer treatment. J. Microbiol. Immunol. Infect. 2017, 50, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Buonora, S.N.; Dos Santos, F.B.; Daumas, R.P.; Passos, S.R.; da Silva, M.H.; de Lima, M.R.; Nogueira, R.M. Increased sensitivity of NS1 ELISA by heat dissociation in acute dengue 4 cases. BMC Infect. Dis. 2017, 17, 204. [Google Scholar] [CrossRef] [PubMed]
- Castro-Munoz, R.; Serna-Vazquez, J.; Garcia-Depraect, O. Current evidence in high throughput ultrafiltration toward the purification of monoclonal antibodies (mAbs) and biotechnological protein-type molecules. Crit. Rev. Biotechnol. 2022, 42, 827–837. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, K.; Scheibe, O.; Kocourek, A.; Muelich, J.; Jurkiewicz, E.; Pfeifer, A. Highly efficient concentration of lenti- and retroviral vector preparations by membrane adsorbers and ultrafiltration. BMC Biotechnol. 2011, 11, 55. [Google Scholar] [CrossRef]
- Miller, E.; Sikes, H.D. Addressing Barriers to the Development and Adoption of Rapid Diagnostic Tests in Global Health. Nanobiomedicine 2015, 2, 2–6. [Google Scholar] [CrossRef]
- Acosta, P.O.; Granja, F.; Meneses, C.A.; Nascimento, I.A.; Sousa, D.D.; Lima Junior, W.P.; Naveca, F.G. False-negative dengue cases in Roraima, Brazil: An approach regarding the high number of negative results by NS1 ag kits. Rev. Inst. Med. Trop. Sao Paulo 2014, 56, 447–450. [Google Scholar] [CrossRef]
- Grande, A.J.; Reid, H.; Thomas, E.; Foster, C.; Darton, T.C. Tourniquet Test for Dengue Diagnosis: Systematic Review and Meta-analysis of Diagnostic Test Accuracy. PLoS Negl. Trop. Dis. 2016, 10, e0004888. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Dengue PCR-Positive | Dengue PCR-Negative | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | |||
| Total | 86 | 51 | 35 | |||||
| Sex | ||||||||
| Female | 34 | 39.5 | 21 | 41.2 | 13 | 37.1 | 0.707 | |
| Male | 52 | 60.5 | 30 | 58.8 | 22 | 62.9 | ||
| Age Group | ||||||||
| 15–30 | 40 | 46.5 | 28 | 54.9 | 12 | 34.3 | 0.083 | |
| 31–45 | 24 | 27.9 | 14 | 27.5 | 10 | 28.6 | ||
| 46–61 | 22 | 25.6 | 9 | 17.6 | 13 | 37.1 | ||
| Day of Illness | ||||||||
| 1–3 | 44 | 51.2 | 30 | 58.8 | 14 | 40.0 | 0.001 | |
| 4–6 | 33 | 38.4 | 21 | 41.2 | 12 | 34.3 | ||
| 7–11 | 9 | 10.5 | 0 | 0 | 9 | 25.7 | ||
| Tourniquet test | ||||||||
| Not performed | 17 | 19.8 | 14 | 27.5 | 3 | 8.6 | 0.001 | |
| Negative | 46 | 53.5 | 19 | 37.3 | 27 | 77.1 | ||
| Positive | 23 | 26.7 | 18 | 35.3 | 5 | 14.3 | ||
| Dengue Serotype * | ||||||||
| 1 | 14 | 27.5 | ||||||
| 2 | 9 | 17.6 | ||||||
| 3 | 14 | 27.5 | ||||||
| 4 | 14 | 27.5 | ||||||
| Final Diagnosis * | ||||||||
| DF | 40 | 78.4 | 0 | 0 | ||||
| DHF | 11 | 21.6 | 0 | 0 | ||||
| Bacteremia | 0 | 0 | 5 | 14.3 | ||||
| Influenza | 0 | 0 | 10 | 28.6 | ||||
| Leptospirosis | 0 | 0 | 10 | 28.6 | ||||
| Murine typhus | 0 | 0 | 10 | 28.6 | ||||
| Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | Positive LR (95%CI) | Negative LR (95%CI) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Concentration | Post-Concentration | Pre-Concentration | Post-Concentration | Pre-Concentration | Post-Concentration | Pre-Concentration | Post-Concentration | Pre-Concentration | Post-Concentration | Pre-Concentration | Post-Concentration | |
| ELISA-NS1 | 82.4 (69.1–91.6) | 94.3 (80.8–99.3) | 95.5 (84.5–99.4) | 78.6 (63.2–89.7) | 14.4 (3.73–55.7) | 0.19 (0.10–0.34) | ||||||
| RDT-NS1 | 76.5 (62.5–87.2) | 80.4 (66.9–90.2) | 100.0 (90.0–100.0) | 100.0 (90.0–100.0) | 100.0 (91.0–100.0) | 100 (91.4–100.0) | 74.5 (59.7–86.1) | 77.8 (62.9–88.8) | NA | NA | 0.24 (0.14–0.39) | 0.20 (0.11–0.34) |
| ELISA-IgM | 27.5 (15.9–41.7) | 23.5 (12.8–37.5) | 91.4 (76.9–98.2) | 97.1 (85.1–99.9) | 82.4 (56.6–96.2) | 92.3 (64.0–99.8) | 46.4 (34.3–58.8) | 46.6 (34.8–58.6) | 3.2 (0.99–10.3) | 8.24 (1.12–60.5) | 0.79 (0.65–0.97) | 0.79 (0.67–0.93) |
| RDT-IgM | 17.9 (8.4–30.9) | 11.8 (4.44–23.9) | 97.1 (85.1–99.9) | 100.0 (90.0–100.0) | 90.0 (55.5–99.7) | 100.0 (54.1–100.0) | 44.7 (33.3–56.6) | 43.8 (32.7–55.3) | 6.18 (0.82–46.6) | NA | 0.85 (0.74–0.97) | 0.88 (0.80–0.98) |
| ELISA-IgG | 86.3 (73.7–94.3) | 86.3 (73.7–94.3) | 5.71 (0.7–19.2) | 5.71 (0.7–19.2) | 57.1 (45.4–68.4) | 57.1 (45.4–68.4) | 22.2 (2.8–60.0) | 22.2 (2.8–60.0) | 0.92 (0.80–1.05) | 0.92 (0.80–1.05) | 2.4 (0.53–10.9) | 2.4 (0.53–10.9) |
| RDT-IgG | 66.7 (52.1–79.2) | 62.7 (48.1–75.9) | 25.7 (12.5–43.3) | 34.3 (19.1–52.2) | 56.7 (43.2–69.4) | 58.2 (44.1–71.3) | 34.6 (17.2–55.7) | 38.7 (21.8–57.8) | 0.90 (0.68–1.18) | 0.96 (0.69–1.31) | 1.3 (0.65–2.57) | 1.09 (0.61–1.94) |
| RDT-NS1 and RDT-IgM | 78.4 (64.7–88.7) | 82.4 (69.1–91.6) | 97.1 (85.1–99.9) | 100.0 (90.0–100.0) | 97.6 (87.1–99.9) | 100.0 (91.6–100.0) | 75.6 (60.5–87.1) | 79.5 (64.7–90.2) | 27.5 (3.96–190.0) | NA | 0.22 (0.13–0.38) | 0.18 (0.10–0.32) |
| Sensitivity | Day of Illness | ||
|---|---|---|---|
| 1–3 N = 44 Sensitivity (95% CI) | 4–6 N = 33 Sensitivity (95% CI) | ||
| ELISA-NS1 | |||
| Pre-concentration | 83.3 (65.3–94.4) | 81.0 (58.1–94.6) | |
| Post-concentration | - | - | |
| RDT-NS1 | |||
| Pre-concentration | 76.7 (57.7–90.1) | 47.6 (25.7–70.2) | |
| Post-concentration | 83.3 (65.3–94.4) | 76.2 (52.8–91.8) | |
| ELISA-IgM | |||
| Pre-concentration | 13.3 (3.8–30.7) | 47.6 (25.7–70.2) | |
| Post-concentration | 16.7 (5.64–34.7) | 33.3 (14.6–57.0) | |
| RDT-IgM | |||
| Pre-concentration | 3.33 (0.08–17.2) | 38.1 (18.1–61.6) | |
| Post-concentration | 3.33 (0.08–17.2) | 23.8 (8.22–47.2) | |
| ELISA-IgG | |||
| Pre-concentration | 83.3 (65.3–94.4) | 90.5 (69.6–98.8) | |
| Post-concentration | 83.3 (65.3–94.4) | 90.5 (69.6–98.8) | |
| RDT-IgG | |||
| Pre-concentration | 56.7 (37.4–74.5) | 81 (58.1–94.6) | |
| Post-concentration | 53.3 (34.3–71.7) | 76.2 (52.8–91.8) | |
| RDT-NS1 and RDT-IgM | |||
| Pre-concentration | 76.7 (57.7–90.1) | 81.0 (58.1–94.6) | |
| Post-concentration | 83.3 (65.3–94.4) | 81.0 (58.1–94.6) | |
| Dengue PCR-Positive | ||||||
|---|---|---|---|---|---|---|
| RDT-Positive | RDT-Negative | p-Value | ||||
| N | (%) | N | (%) | |||
| Total | 40 | 11 | ||||
| Sex | ||||||
| Female | 18 | 45.0 | 3 | 27.3 | 0.328 * | |
| Male | 22 | 55.0 | 8 | 72.7 | ||
| Age Group | ||||||
| 15–30 | 22 | 55.0 | 6 | 54.5 | 0.525 * | |
| 31–45 | 12 | 30.0 | 2 | 18.2 | ||
| 46–61 | 6 | 15.0 | 3 | 27.3 | ||
| Day of Illness† | ||||||
| 1 | 5 | 12.5 | 3 | 27.3 | 0.698 * | |
| 2 | 7 | 17.5 | 2 | 18.2 | ||
| 3 | 11 | 27.5 | 2 | 18.2 | ||
| 4 | 10 | 25.0 | 2 | 18.2 | ||
| 5 | 6 | 15.0 | 1 | 9.1 | ||
| 6 | 1 | 2.5 | 1 | 9.1 | ||
| Tourniquet Test | ||||||
| Not performed | 12 | 30.0 | 2 | 18.2 | 0.513 * | |
| Negative | 13 | 32.5 | 6 | 54.5 | ||
| Positive | 15 | 37.5 | 3 | 27.3 | ||
| Dengue Serotype † | ||||||
| 1 | 12 | 30.0 | 2 | 18.2 | 0.183 * | |
| 2 | 9 | 22.5 | 0 | 0 | ||
| 3 | 9 | 22.5 | 5 | 45.5 | ||
| 4 | 10 | 25.0 | 4 | 36.4 | ||
| Final Diagnosis | ||||||
| DF | 30 | 75.0 | 10 | 90.9 | 0.418 * | |
| DHF | 10 | 25.0 | 1 | 9.1 | ||
| Serology | 1.00 | |||||
| Primary | 1 | 2.6 | 0 | 0 | ||
| Secondary | 38 | 97.4 | 11 | 100 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luvira, V.; Thawornkuno, C.; Lawpoolsri, S.; Thippornchai, N.; Duangdee, C.; Ngamprasertchai, T.; Leaungwutiwong, P. Diagnostic Performance of Dengue NS1 and Antibodies by Serum Concentration Technique. Trop. Med. Infect. Dis. 2023, 8, 117. https://doi.org/10.3390/tropicalmed8020117
Luvira V, Thawornkuno C, Lawpoolsri S, Thippornchai N, Duangdee C, Ngamprasertchai T, Leaungwutiwong P. Diagnostic Performance of Dengue NS1 and Antibodies by Serum Concentration Technique. Tropical Medicine and Infectious Disease. 2023; 8(2):117. https://doi.org/10.3390/tropicalmed8020117
Chicago/Turabian StyleLuvira, Viravarn, Charin Thawornkuno, Saranath Lawpoolsri, Narin Thippornchai, Chatnapa Duangdee, Thundon Ngamprasertchai, and Pornsawan Leaungwutiwong. 2023. "Diagnostic Performance of Dengue NS1 and Antibodies by Serum Concentration Technique" Tropical Medicine and Infectious Disease 8, no. 2: 117. https://doi.org/10.3390/tropicalmed8020117
APA StyleLuvira, V., Thawornkuno, C., Lawpoolsri, S., Thippornchai, N., Duangdee, C., Ngamprasertchai, T., & Leaungwutiwong, P. (2023). Diagnostic Performance of Dengue NS1 and Antibodies by Serum Concentration Technique. Tropical Medicine and Infectious Disease, 8(2), 117. https://doi.org/10.3390/tropicalmed8020117