

Antibiotic Consumption in Vanuatu before and during the COVID-19 Pandemic, 2018 to 2021: An Interrupted Time Series Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. The COVID-19 Pandemic
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Consumption before and during COVID-19
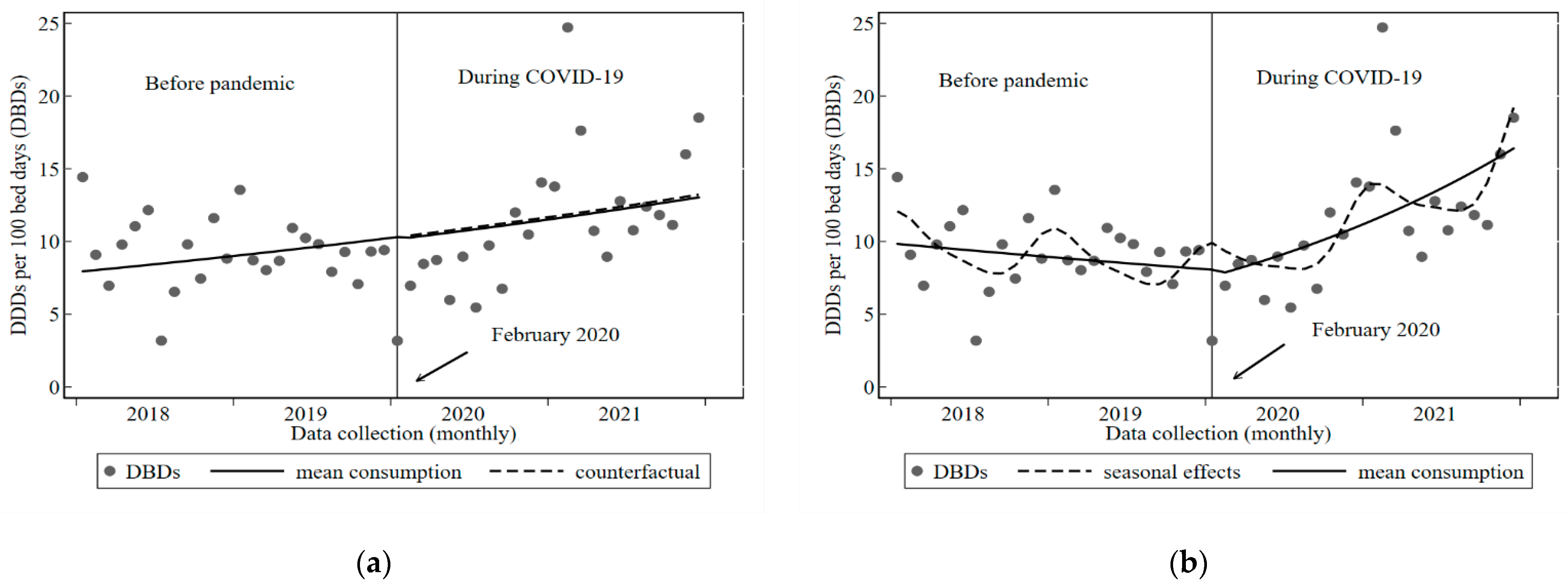
3.2. Inpatient Consumption
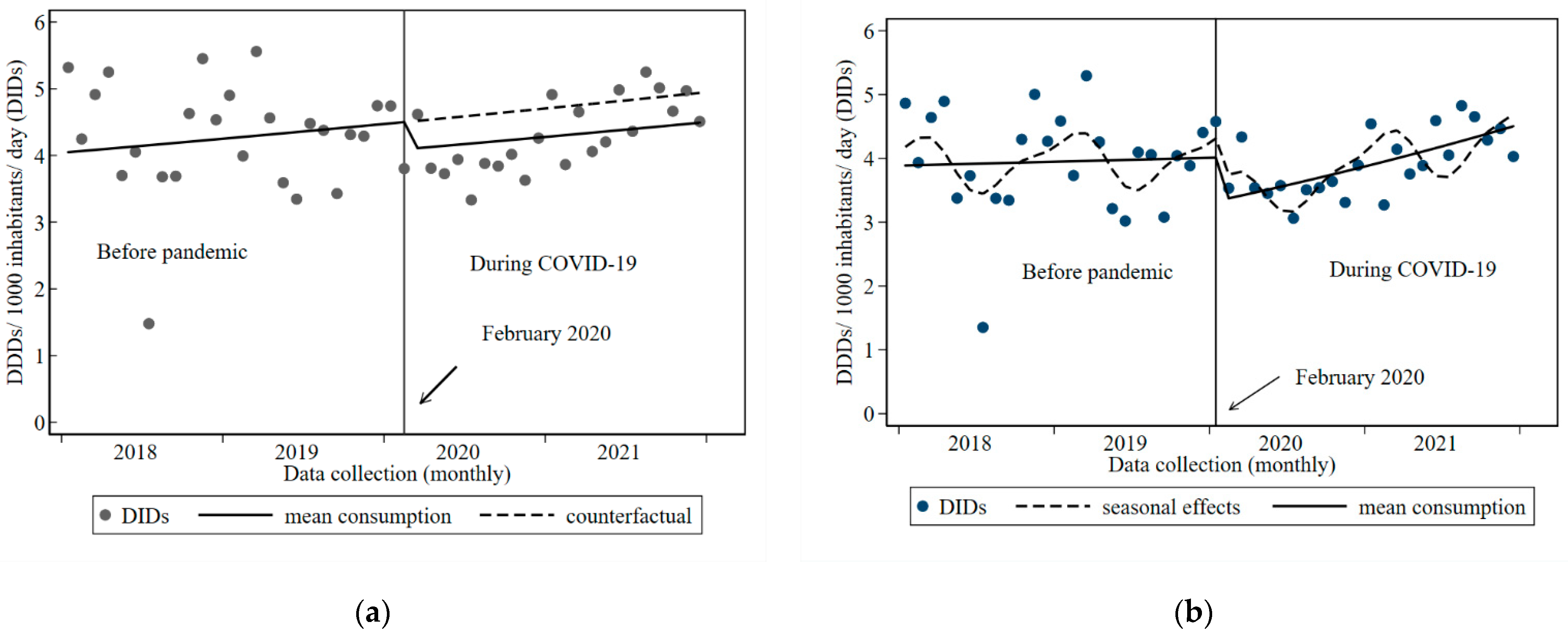
3.3. Outpatient Consumption
3.4. Influence of the COVID-19 Pandemic on Antibiotic Consumption
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Knight, G.M.; Glover, R.; McQuaid, C.F.; Olaru, I.D.; Gallandat, K.; Leclerc, Q.J.; Fuller, N.M.; Willcocks, S.J.; Hasan, R.; van Kleef, E.; et al. Antimicrobial resistance and COVID-19: Intersections and implications. eLife 2021, 10, e64139. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. COVID-19 Dashboard. 2022. Available online: https://covid19.who.int (accessed on 17 September 2022).
- Tomczyk, S.; Taylor, A.; Brown, A.; de Kraker, M.; El-Saed, A.; Alshamrani, M.; Hendriksen, R.S.; Jacob, M.; Löfmark, S.; Perovic, O.; et al. Impact of the COVID-19 pandemic on the surveillance, prevention and control of antimicrobial resistance: A global survey. J. Antimicrob. Chemother. 2021, 76, 3045–3058. [Google Scholar] [CrossRef] [PubMed]
- Mah-E-Muneer, S.; Hassan, M.Z.; Biswas, M.A.; Rahman, F.; Akhtar, Z.; Das, P.; Islam, M.A.; Chowdhury, F. Use of antimicrobials among suspected COVID-19 patients at selected hospitals, Bangladesh: Findings from the first wave of COVID-19 pandemic. Antibiotics 2021, 10, 738. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Hasan, S.S.; Bond, S.E.; Conway, B.R.; Aldeyab, M.A. Antimicrobial consumption in patients with COVID-19: A systematic review and meta-analysis. Expert Rev. Anti-Infect. Ther. 2021, 20, 749–772. [Google Scholar] [CrossRef]
- Hussein, R.R.; Rabie, A.S.I.; Bin Shaman, M.; Shaaban, A.H.; Fahmy, A.M.; Sofy, M.R.; Lattyak, E.; Abuelhana, A.; Naguib, I.; Ashour, A.M.; et al. Antibiotic consumption in hospitals during COVID-19 pandemic: A comparative study. J. Infect. Dev. Ctries. 2022, 16, 1679–1686. [Google Scholar] [CrossRef]
- Mustafa, Z.U.; Salman, M.; Aldeyab, M.; Kow, C.S.; Hasan, S.S. Antimicrobial consumption among hospitalized patients with COVID-19 in Pakistan. SN Compr. Clin. Med. 2021, 3, 1691–1695. [Google Scholar] [CrossRef]
- Daria, S.; Islam, R. Indiscriminate Use of Antibiotics for COVID-19 Treatment in South Asian Countries is a Threat for Future Pandemics Due to Antibiotic Resistance. Clin. Pathol. 2022, 15, 1–3. [Google Scholar] [CrossRef]
- Lucien, M.A.B.; Canarie, M.F.; Kilgore, P.E.; Jean-Denis, G.; Fénélon, N.; Pierre, M.; Cerpa, M.; Joseph, G.A.; Maki, G.; Zervos, M.J.; et al. Antibiotics and antimicrobial resistance in the COVID-19 era: Perspective from resource-limited settings. Int. J. Infect. Dis. 2021, 104, 250–254. [Google Scholar] [CrossRef]
- World Health Organisation. Library of AMR National Action Plans. Available online: https://www.who.int/teams/surveillance-prevention-control-AMR/national-action-plan-monitoring-evaluation/library-of-national-action-plans (accessed on 12 September 2022).
- World Health Organisation. GLASS Methodology for Surveillance of National Antimicrobial Consumption; WHO: Geneva, Switzerland, 2020.
- World Health Organisation. Global Action Plan on Antimicrobial Resistance; WHO: Geneva, Switzerland, 2016. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 15 September 2022).
- World Health Organisation. AWaRe Portal: WHO Antibiotic Characterisation; WHO: Geneva, Switzerland, 2016. Available online: https://aware.essentialmeds.org/groups (accessed on 2 October 2022).
- WHO Advisory Group on Integrated Surveillance of Antimicrobial Resistance (AGISAR). Critcally Important Antimicrobials for Human Medicine: Ranking of Medically Important Antimicrobials for Risk Management of Antimicrobial Resistance Due to Non-Human Use, 6th ed.; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Leung, V.; Langford, B.J.; Ha, R.; Schwartz, K.L. Metrics for evaluating antibiotic use and prescribing in outpatient settings. JAC-Antimicrob. Resist. 2021, 3, dlab098. [Google Scholar] [CrossRef]
- Bergman, U.; Grímsson, A.; Wahba, A.H.; Westerholm, B.; World Health Organization. Studies in Drug Utilization: Methods and Applications; World Health Organization: Geneva, Switzerland, 1979. [Google Scholar]
- Al-Azzam, S.; Mhaidat, N.; Banat, H.; Alfaour, M.; Ahmad, D.; Muller, A.; Al-Nuseirat, A.; Lattyak, E.; Conway, B.; Aldeyab, M. An Assessment of the Impact of Coronavirus Disease (COVID-19) Pandemic on National Antimicrobial Consumption in Jordan. Antibiotics 2021, 10, 690. [Google Scholar] [CrossRef]
- Andrews, A.; Budd, E.; Hendrick, A.; Ashiru-Oredope, D.; Beech, E.; Hopkins, S.; Gerver, S.; Muller-Pebody, B.; The AMU COVID-19 Stakeholder Group. Surveillance of Antibacterial Usage during the COVID-19 Pandemic in England, 2020. Antibiotics 2021, 10, 841. [Google Scholar] [CrossRef] [PubMed]
- Grau, S.; Echeverria-Esnal, D.; Gómez-Zorrilla, S.; Navarrete-Rouco, M.E.; Masclans, J.R.; Espona, M.; Gracia-Arnillas, M.P.; Duran, X.; Comas, M.; Horcajada, J.P.; et al. Evolution of Antimicrobial Consumption During the First Wave of COVID-19 Pandemic. Antibiotics 2021, 10, 132. [Google Scholar] [CrossRef] [PubMed]
- Beovic, B.; Doušak, M.; Ferreira-Coimbra, J.; Nadrah, K.; Rubulotta, F.; Belliato, M.; Berger-Estilita, J.; Ayoade, F.; Rello, J.; Erdem, H. Antibiotic use in patients with COVID-19: A ‘snapshot’ Infectious Diseases International Research Initiative (ID-IRI) survey. J. Antimicrob. Chemother. 2020, 75, 3386–33090. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation Western Pacific Region. Coronavirus Diseases 2019 (COVID-19) External Situation Report 86. COVID-19 Situation Report for The Western Pacific 2022. Available online: https://apps.who.int/iris/handle/10665/338523 (accessed on 1 October 2022).
- Vanuatu Ministry of Health. Coronavirus Disease 2019 (COVID-19) Vanuatu Situation Report: 59, 2021. Available online: http://covid-19.gov.vu/index.php/situation-reports (accessed on 5 October 2022).
- Vanuatu Ministry of Health. Coronavirus Disease 2019 (COVID-19) Vanuatu Situation Report: 12, 2020. Available online: http://covid-19.gov.vu/index.php/situation-reports (accessed on 5 October 2022).
- Vanuatu Ministry of Health. Coronavirus Disease 2019 (COVID-19) Vanuatu Situation Report: 8, 2020. Available online: http://covid-19.gov.vu/indez.php/situation-reports (accessed on 5 October 2022).
- Vanuatu Ministry of Health. Coronavirus Disease 2019 (COVID-19) Vanuatu Situation Report: 2, 2020. Available online: http://covid-19.gov.vu/index.php/situation=reports (accessed on 5 October 2022).
- South Pacific Community Statistics for Development Division. Republic of Vanuatu: Census and Surveys. Available online: https://sdd.spc.int/vu (accessed on 2 October 2022).
- Williams, W.; van Gemert, C.; Mariasua, J.; Iavro, E.; Fred, D.; Nausien, J.; Manwo, O.; Atua, V.; Pakoa, G.J.; Tassiets, A.; et al. Challenges to implementation and strengthening of initial COVID-19 surveillance in Vanuatu: January–April 2020. West. Pac. Surveill. Response J. 2021, 12, 57–64. [Google Scholar] [CrossRef]
- Kool, J.L.; Paterson, B.; Pavlin, B.I.; Durrheim, D.; Musto, J.; Kolbe, A. Pacific-wide simplified syndromic surveillance for early warning of outbreaks. Glob. Public Health 2012, 7, 670–681. [Google Scholar] [CrossRef]
- Tapo, P.S.; van Gemert, C.; Manwo, O.; Iavro, E.; Williams, W.; Maurice, R.; Harrison, G.; Cornish, M.; Benjamin, M.; Atua, V.; et al. Lessons from COVID-19-free Vanuatu: Intensive health operations for Phase 1 of repatriation and quarantine, May–July 2020. West. Pac. Surveill. Response J. 2021, 12, 61–68. [Google Scholar] [CrossRef]
- World Health Organization. Model List of Essential Medicines, 22nd List 2021. Available online: https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2021.02 (accessed on 20 September 2022 ).
- WHO Collaborating Centre for Drug Statistics Methodology. ATC/ DDD Index 2022. Available online: https://www.whocc.no/atc_ddd_index_and_guidelines/atc_ddd_index/ (accessed on 20 September 2022).
- Hollingworth, S.; Kairuz, T. Measuring Medicine Use: Applying ATC/DDD Methodology to Real-World Data. Pharmacy 2021, 9, 60. [Google Scholar] [CrossRef]
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar] [CrossRef]
- Ramsay, C.R.; Matowe, L.; Grilli, R.; Grimshaw, J.M.; Thomas, R.E. Interrupted time series designs in health technology assessment: Lessons from two systematic reviews of behavior change strategies. Int. J. Technol. Assess. Health Care 2003, 19, 613–623. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Gasparrini, A.; Hajat, S.; Smeeth, L.; Armstrong, B. Time series regression studies in environmental epidemiology. Leuk. Res. 2013, 42, 1187–1195. [Google Scholar] [CrossRef]
- Long, J.S.; Freese, J. Regression Models for Categorical Dependent Variables Using Stata, 3rd ed.; StataCorp: College Station, TX, USA, 2014. [Google Scholar]
- World Health Organization. WHO Report on Surveillance of Antibiotic Consumption: 2016–2018 Early Implementation; WHO: Geneva, Switzerland, 2018.
- Norris, P.; Nguyen, H.A. Consumption of antibiotics in a small Pacific Island nation: Samoa. Pharm. Pract. 2007, 5, 36–41. [Google Scholar] [CrossRef] [PubMed][Green Version]
- World Health Organisation. AWaRe Portal. Available online: https://adoptaware.org/ (accessed on 20 September 2022).
- Marcelin, J.R.; Chung, P.; Van Schooneveld, T.C. Antimicrobial stewardship in the outpatient setting: A review and proposed framework. Infect. Control Hosp. Epidemiol. 2020, 41, 833–840. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Antibiotic | Class | ATC Code | Route | DDD (g) | AWaRe Group |
|---|---|---|---|---|---|
| Amoxicillin | Penicillins | J01CA04 | 0ral | 1.5 | Access |
| Amoxicillin Clavulanate | Beta-lactam/beta-lactamase inhibitor | J01CR02 | 0ral | 0.625 | Access |
| Azithromycin | Macrolides | J01FA10 | 0ral | 0.3 | Watch |
| Ciprofloxacin | Fluoroquinolones | J01MA02 | 0ral | 1 | Watch |
| Cloxacillin | Penicillins | J01CF02 | 0ral | 2 | Access |
| Doxycycline | Tetracyclines | J01AA02 | 0ral | 0.1 | Access |
| Erythromycin | Macrolides | J01FA01 | 0ral | 1 | Watch |
| Metronidazole | Imidazole | J01XD01 | 0ral | 1.5 | Access |
| Phenoxymethylpenicillin | Penicillins | J01CE02 | 0ral | 2 | Access |
| Sulfamethoxazole/Trimethoprim | Sulphonamide/trimethoprim | J01EE01 | 0ral | 4 | Access |
| Antibiotic Consumption | Before the Pandemic Jan 2018–Jan 2019 | During COVID-19 Feb 2020–Dec 2021 |
|---|---|---|
| Inpatient oral antibiotic consumption | ||
| Total DDDs | 15,661 | 18,411 |
| Total DBDs | 226.97 | 266.82 |
| Mean monthly DBDs | 9.07 | 11.60 |
| Difference between mean monthly DBDs before and during COVID-19 | 2.66 p = 0.009 (95% CI 0.71; 4.61) | |
| Outpatient oral antibiotic consumption | ||
| Total DDDs | 314,004 | 295,508 |
| Total DIDs | 102.2 | 92.7 |
| Mean monthly DIDs | 4.09 | 4.03 |
| Difference between mean monthly DIDs before and during COVID-19 | 0.063 p = 0.74 (95% CI−0.33, 0.46) | |
| Antibiotics Prescribed (DDD Unit) | Before the Pandemic: Jan 2019–Jan 2020 | During COVID-19: Feb 2020–Dec 2021 |
|---|---|---|
| Inpatient DDDs/100 bed days (DBDs) (% total) | ||
| Amoxicillin (1.5 g) | 46.2 (20.3) | 53.9 (20.2) |
| Cloxacillin (2 g) | 84.6 (37.2) | 100.1 (37.5) |
| Penicillin V (2 g) | 8 (3.5) | 16.8 (6.3) |
| Amoxicillin/clavulanate (1.5 g) | 17.6 (7.7) | 23.8 (8.9) |
| Azithromycin (0.3 g) | 2.9 (1.3) | 2.7 (1) |
| Erythromycin (1 g) | 3.2 (1.4) | 2.8 (1) |
| Ciprofloxacin (1 g) | 10.1 (4.4) | 10.3 (3.9) |
| Doxycycline (0.1 g) | 5.2 (2.3) | 6.2 (2.3) |
| Sulfamethoxazole/Trimethoprim (4 g) | 0.7 (0.3) | 1.1 (0.4) |
| Metronidazole (1.5 g) | 48.5 (21.4) | 49.1 (18.4) |
| Total DBDs per period | 226.9 (100) | 266.8 (100) |
| Outpatient DDDs/1000 inhabitants/day (DIDs) (% total) | ||
| Amoxicillin (1.5 g) | 43.1 (42.2) | 35.7 (38.5) |
| Cloxacillin (2 g) | 14.1 (13.8) | 14.2 (15.3) |
| Penicillin V (2 g) | 13.8 (13.5) | 15.9 (17.1) |
| Amoxicillin/ clavulanate (1.5 g) | 6.7 (6.5) | 5.5 (5.5) |
| Azithromycin (0.3 g) | 2.3 (2.3) | 2.4 (2.5) |
| Erythromycin (1 g) | 1.02 (1.0) | 0.5 (0.6) |
| Ciprofloxacin (1 g) | 3.4 (3.3) | 1.9 (2.1) |
| Doxycycline (0.1 g) | 3.3 (3.2) | 2.9 (3.2) |
| Sulfamethoxazole/Trimethoprim (4 g) | 2.3 (2.2) | 1.6 (1.7) |
| Metronidazole (1.5 g) | 12.3 (12.1) | 12.12 (13.1) |
| Total DIDs per period | 102.2 (100) | 92.7 (100) |
| Antibiotic Prescription by Access Watch and Restrict Class (AWaRe) | ||
|---|---|---|
| AWaRe Classification | Before the Pandemic: Jan 2019–Jan 2020 | During COVID-19: Feb 2020–Dec 2021 |
| Inpatient DDDs/100 bed days (DBDs) (% total) | ||
| Watch class DBDs | 16.2 (7) | 15.8 (6) |
| Difference between mean monthly Watch DBDs before and during COVID-19 | 0.041 p = 0.54 (95% CI−0.18; 0.09) | |
| Access class DBDs | 210.7 (93) | 251 (94) |
| Difference between mean monthly DBDs before and during COVID-19 | 0.75 p = 0.49 (95% CI−2.93; 1.43) | |
| Outpatient DDDs/1000 inhabitants/day (DIDs) (% total) | ||
| Watch class DIDs | 6.9 (7) | 4.8 (5) |
| Difference between mean monthly DIDs before and during COVID-19 | 0.066 p = 0.002 (95% CI 0.03; 0.11) | |
| Access class DIDs | 95.5 (93) | 87.9 (95) |
| Difference between mean monthly DIDs before and during COVID-19 | 0.008 p = 0.96 (95% CI−0.36; 0.38) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foxlee, N.D.; Lui, A.; Mathias, A.; Townell, N.; Lau, C.L. Antibiotic Consumption in Vanuatu before and during the COVID-19 Pandemic, 2018 to 2021: An Interrupted Time Series Analysis. Trop. Med. Infect. Dis. 2023, 8, 23. https://doi.org/10.3390/tropicalmed8010023
Foxlee ND, Lui A, Mathias A, Townell N, Lau CL. Antibiotic Consumption in Vanuatu before and during the COVID-19 Pandemic, 2018 to 2021: An Interrupted Time Series Analysis. Tropical Medicine and Infectious Disease. 2023; 8(1):23. https://doi.org/10.3390/tropicalmed8010023
Chicago/Turabian StyleFoxlee, Nicola D., Amsaline Lui, Agnes Mathias, Nicola Townell, and Colleen L. Lau. 2023. "Antibiotic Consumption in Vanuatu before and during the COVID-19 Pandemic, 2018 to 2021: An Interrupted Time Series Analysis" Tropical Medicine and Infectious Disease 8, no. 1: 23. https://doi.org/10.3390/tropicalmed8010023
APA StyleFoxlee, N. D., Lui, A., Mathias, A., Townell, N., & Lau, C. L. (2023). Antibiotic Consumption in Vanuatu before and during the COVID-19 Pandemic, 2018 to 2021: An Interrupted Time Series Analysis. Tropical Medicine and Infectious Disease, 8(1), 23. https://doi.org/10.3390/tropicalmed8010023