
A Retrospective Analysis of Culture-Confirmed Enterococci Bloodstream Infections in South Africa, 2016–2020: A Cross-Sectional Study




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Population and Setting
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Laboratory Procedures
2.5. Data Source
2.6. Data Analysis
3. Results
3.1. Patient Demographic and Clinical Characteristics
3.2. Cases of ESKAPE Bloodstream Infections in South Africa
3.3. Cases of Enterococci Bloodstream Infections in South Africa
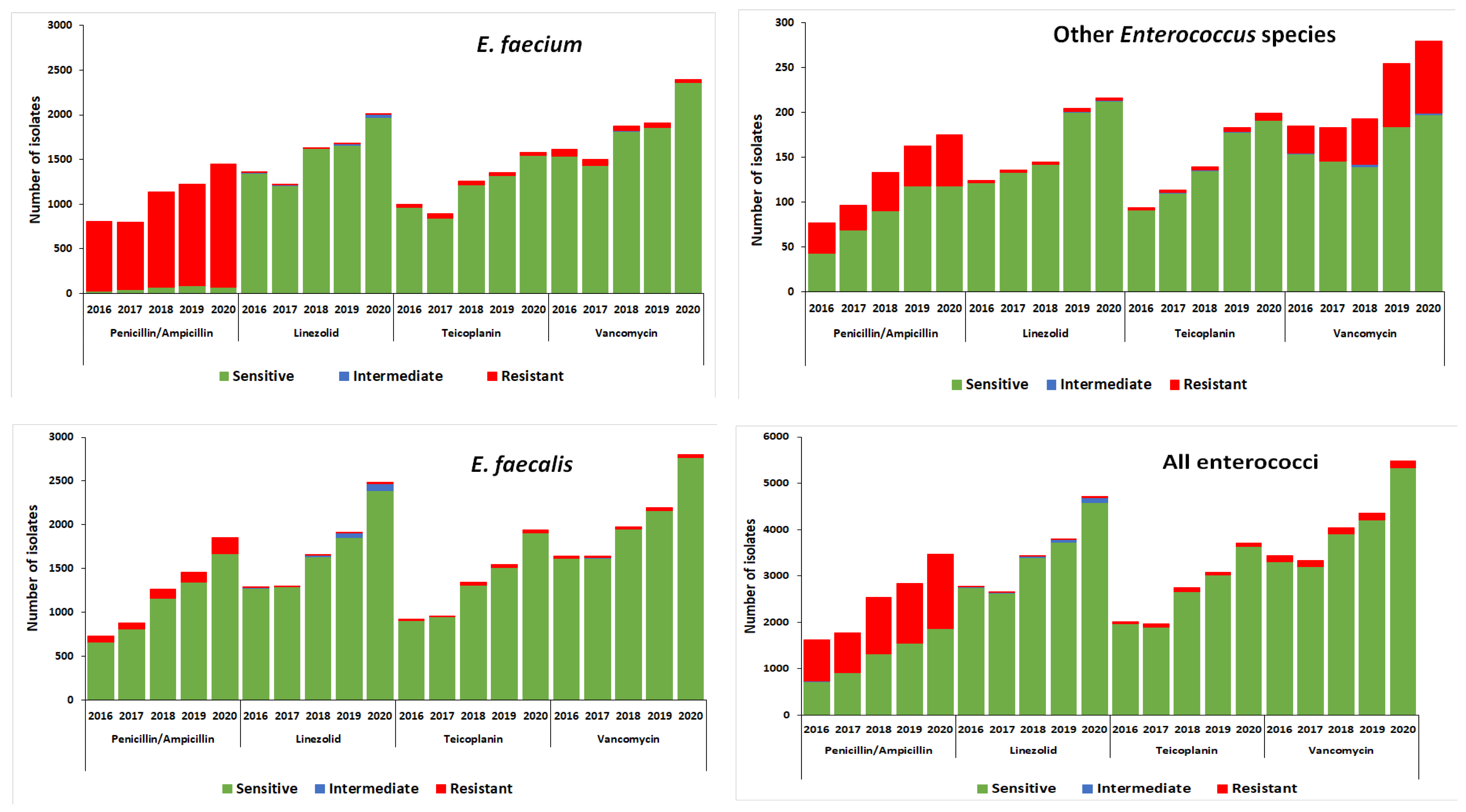
3.4. Antimicrobial Susceptibility Profiles of Enterococci Bloodstream Infection Isolates in South Africa
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Santajit, S.; Indrawattana, N. Mechanisms of antimicrobial resistance in ESKAPE pathogens. Biomed. Res. Int. 2016, 2016, 2475067. [Google Scholar] [CrossRef] [PubMed]
- Laurentiu, T.A.; Nicoleta, M.; Octav, P.; Irina, G.; Marcela, P.; Otilia, B.; Corina, C.V.; Carmen, M.C.; Veronica, L.; Marutescu, L. Resistance features of Pseudomonas aeruginosa strains isolated from patients with infectious complications of cardiovascular surgery. Biointerface Res. Appl. Chem. 2017, 7, 2004–2008. [Google Scholar]
- Fisher, K.; Phillips, C. The ecology, epidemiology and virulence of Enterococcus. Microbiology 2009, 155, 1749–1757. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. 2021 Antibacterial Agents in Clinical and Preclinical Development: An Overview and Analysis; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- World Health Organization. Global Antimicrobial Resistance Surveillance System (GLASS) Report Early Implementation 2017–2018; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Ahmed, M.O.; Baptiste, K.E. Vancomycin-Resistant Enterococci: A Review of Antimicrobial Resistance Mechanisms and Perspectives of Human and Animal Health. Microb. Drug Resist. 2018, 24, 590–606. [Google Scholar] [CrossRef]
- Rice, L.B. Federal funding for the study of antimicrobial resistance in nosocomial pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef]
- Suetens, C.; Latour, K.; Kärki, T.; Ricchizzi, E.; Kinross, P.; Moro, M.L.; Jans, B.; Hopkins, S.; Hansen, S.; Lyytikäinen, O.; et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities. Results from two European point prevalence surveys, 2016 to 2017. Eur. Surveill. 2018, 23, 1800516. [Google Scholar] [CrossRef]
- Llaca-Díaz, J.M.; Mendoza-Olazarán, S.; Camacho-Ortiz, A.; Flores, S.; Garza-González, E. One-year surveillance of ESKAPE pathogens in an Intensive Care Unit of Monterrey, Mexico. Chemotherapy 2012, 58, 475–481. [Google Scholar] [CrossRef]
- Lebreton, F.; Willems, R.J.L.; Gilmore, M.S. Enterococcus Diversity, Origins in Nature, and Gut Colonization. In Enterococci from Commensals to Leading Causes Drug Resistant Infection; Massachusetts Eye and Ear Infirmary: Boston, MA, USA, 2014; pp. 1–59. Available online: https://www.ncbi.nlm.nih.gov/books/NBK190427/ (accessed on 1 November 2022).
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. World health organization releases global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. JMS J. Med. Soc. 2018, 32, 76–77. [Google Scholar] [CrossRef]
- CDC. Antibiotic resistance threats in the United States. In Atlanta (GA): Antibiotic Resistance Coordination and Strategy Unit within the Division of Healthcare Quality Promotion, National Center for Emerging and Zoonotic Infectious Diseases; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019. [Google Scholar]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations; Government of the United Kingdom: London, UK, 2016. [Google Scholar]
- National Health Laboratory Services. Standard Operating Procedures: Reporting of Notifiable medical conditions (NMC) version 2.0; National Health Laboratory Services: Johannesburg, South Africa, 2018. [Google Scholar]
- Suppli, M.R.; Aabenhus, Z.B.; Harboe, L.P.; Andersen, M.; Tvede, J.-U.S. Jensen. Mortality in enterococcal bloodstream infections increases with inappropriate antimicrobial therapy. Clin. Microbiol. Infect. 2011, 17, 1078–1083. [Google Scholar] [CrossRef]
- Edmond, M.B.; Ober, J.F.; Dawson, J.D.; Weinbaum, D.L.; Wenzel, R.P. Vancomycin-resistant enterococcal bacteremia: Natural history and attributable mortality. Clin. Infect. Dis. 1996, 23, 1234–1239. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Surveillance Report of Antimicrobial Resistance and Consumption of Antibiotics in South Africa; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- García-Solache, M.; Rice, L.B. The Enterococcus: A model of adaptability to its environment. Clin. Microbiol. Rev. 2019, 32, e00058-18. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, T.; Crank, C.W. Vancomycin-resistant enterococcal infections: Epidemiology, clinical manifestations, and optimal management. Infect. Drug Resist. 2015, 8, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Diekema, D.J.; Hsueh, P.R.; Mendes, R.E.; Pfaller, M.A.; Rolston, K.V.; Sader, H.S.; Jones, R.N. The microbiology of bloodstream infection: 20-year trends from the SENTRY antimicrobial surveillance program. Antimicrob. Agents Chemother. 2019, 63, e00355-19. [Google Scholar] [CrossRef] [PubMed]
- De Kraker, M.E.A.; Jarlier, V.; Monen, J.C.M.; Heuer, O.E.; Van De Sande, N.; Grundmann, H. The changing epidemiology of bacteraemias in Europe: Trends from the European Antimicrobial Resistance Surveillance System. Clin. Microbiol. Infect. 2013, 19, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, 13th Information Supplement; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2019. [Google Scholar]
- Abera, A.; Tilahun, M.; Tekele, S.G.; Belete, M.A. Prevalence, antimicrobial susceptibility patterns, and risk factors associated with enterococci among pediatric patients at Dessie Referral Hospital, Northeastern Ethiopia. BioMed. Res. Int. 2021, 2021, 5549847. [Google Scholar] [CrossRef] [PubMed]
- Alotaibi, F.E.; Bukhari, E.E. Emergence of Vancomycin-resistant Enterococci at a teaching hospital, Saudi Arabia. Chin. Med. J. 2017, 130, 340–346. [Google Scholar] [CrossRef]
- Gagetti, P.; Bonofiglio, L.; García Gabarrot, G.; Kaufman, S.; Mollerach, M.; Vigliarolo, L.; von Specht, M.; Toresani, I.; Lopardo, H.A. Resistencia a los β-lactámicos en enterococos. Rev. Argent. Microbiol. 2019, 51, 179–183. [Google Scholar]
- Kristich, C.J.; Rice, L.B.; Arias, C.A. Enterococcal infection-treatment and antibiotic resistance. Enterococci: From Commensals to Leading Causes of Drug Resistant Infection; Massachusetts Eye and Ear Infirmary: Boston, MA, USA, 2014. [Google Scholar]
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Resistance in Europe-Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net) 2017; ECDC: Stockholm, Sweden, 2018. [Google Scholar]
- Olawale, K.O.; Fadiora, S.O.; Taiwo, S.S. Prevalence of hospital acquired enterococci infections in two primary-care hospitals in Osogbo, Southwestern Nigeria. Afr. J. Infect. Dis. 2011, 5. [Google Scholar] [CrossRef]
- Ferede, Z.T.; Tullu, K.D.; Derese, S.G.; Yeshanew, A.G. Prevalence and antimicrobial susceptibility pattern of Enterococcus species isolated from different clinical samples at Black Lion Specialized Teaching Hospital, Addis Ababa, Ethiopia. BMC Res. Notes 2018, 11, 793. [Google Scholar] [CrossRef]
- Abebe, W.; Endris, M.; Tiruneh, M.; Moges, F. Prevalence of vancomycin resistant Enterococci and associated risk factors among clients with and without HIV in Northwest Ethiopia: A cross-sectional study. BMC Public Health 2014, 14, 185. [Google Scholar] [CrossRef]
- Solomon, F.B.; Wadilo, F.W.; Arota, A.A.; Abraham, Y.L. Antibiotic resistant airborne bacteria and their multidrug resistance pattern at University teaching referral Hospital in South Ethiopia. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 29. [Google Scholar] [CrossRef]
- Toru, M.; Beyene, G.; Kassa, T.; Gizachew, Z.; Howe, R.; Yeshitila, B. Prevalence and phenotypic characterization of Enterococcus species isolated from clinical samples of pediatric patients in Jimma University Specialized Hospital, south west Ethiopia. BMC Res. Notes 2018, 11, 281. [Google Scholar] [CrossRef]
- Billington, E.O.; Phang, S.H.; Gregson, D.B.; Pitout, J.D.; Ross, T.; Church, D.L.; Laupland, K.B.; Parkins, M.D. 2 incidence, risk factors, and outcomes of enterococcus spp. blood stream 3 infections: A population-based study. Int. J. Infect. Dis. 2014, 30, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Surveillance Report for Antimicrobial Resistance and Consumption of Antimicrobials in South Africa. 2021. Available online: https://www.knowledgehub.org.za/elibrary/surveillance-antimicrobial-resistance-and-consumption-antimicrobials-south-africa-2021 (accessed on 13 December 2022).
- Tedim, A.P.; Ruiz-Garbajosa, P.; Corander, J.; Rodríguez, C.M.; Cantón Willems, R.J.; Baquero, F.; Coque, T.M. Population biology of intestinal Enterococcus isolates from hospitalized and nonhospitalized individuals in different age groups. Appl. Environ. Microbiol. 2015, 81, 1820–1831. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, L.; Randhawa, V.S.; Deb, M. Antimicrobial resistance of enterococcal blood isolates at a pediatric care hospital in India. Jpn. J. Infect. Dis. 2005, 58, 101–103. [Google Scholar]
- Shrestha, L.B.; Baral, R.; Poudel, P.; Khanal, B. Clinical, etiological and antimicrobial susceptibility profile of pediatric urinary tract infections in a tertiary care hospital of Nepal. BMC Paediatr. 2019, 19, 36. [Google Scholar] [CrossRef]
- Anteneh, A.; Zeleke, G.; Demissie, A.; Setegn, E. Antimicrobial resistance pattern of bacterial isolates from different clinical specimens in Southern Ethiopia: A three-year retrospective study. Afr. J. Bacteriol. Res. 2017, 9, 1–8. [Google Scholar]
- Miller, W.R.; Munita, J.M.; Arias, C.A. Mechanisms of antibiotic resistance in enterococci. Expert Rev. Anti-Infect. Ther. 2014, 12, 1221–1236. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number of Cases (N = 21,339) | |
|---|---|---|
| n | % | |
| Year | ||
| 2016 | 3552 | 16.7 |
| 2017 | 3513 | 16.5 |
| 2018 | 4240 | 19.9 |
| 2019 | 4451 | 20.9 |
| 2020 | 5583 | 26.2 |
| Sex | ||
| Female | 10,319 | 48.4 |
| Male | 10,073 | 47.2 |
| Unknown | 947 | 4.4 |
| Age categories (in years) | ||
| Median age (range) | 2 (0–115) | |
| <1 | 9132 | 42.8 |
| 1–5 | 1266 | 5.9 |
| 6–17 | 582 | 2.7 |
| 18–64 | 6745 | 31.6 |
| >65 | 1773 | 8.3 |
| Unknown | 1841 | 8.6 |
| Province | ||
| Eastern Cape | 1953 | 9.2 |
| Free State | 1513 | 7.1 |
| Gauteng | 9415 | 44.1 |
| KwaZulu-Natal | 4576 | 21.4 |
| Limpopo | 829 | 3.9 |
| Mpumalanga | 666 | 3.1 |
| North West | 535 | 2.5 |
| Northern Cape | 200 | 0.9 |
| Western Cape | 1600 | 7.5 |
| Unknown | 52 | 0.2 |
| Enterococci distribution | ||
| E. avium | 71 | 0.3 |
| E. casselifalvus | 143 | 0.7 |
| E. cecorum | 7 | 0.0 |
| E. columbae | 5 | 0.0 |
| E. durans | 105 | 0.5 |
| E. durans/hirae | 2 | 0.0 |
| E. faecalis | 10,668 | 50.0 |
| E. faecium | 9486 | 44.5 |
| E. gallinarum | 357 | 1.7 |
| E. hirae | 67 | 0.3 |
| E. raffinosus | 22 | 0.1 |
| E. species | 406 | 1.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mogokotleng, R.; Ismail, H.; Perovic, O.; Jallow, S. A Retrospective Analysis of Culture-Confirmed Enterococci Bloodstream Infections in South Africa, 2016–2020: A Cross-Sectional Study. Trop. Med. Infect. Dis. 2023, 8, 19. https://doi.org/10.3390/tropicalmed8010019
Mogokotleng R, Ismail H, Perovic O, Jallow S. A Retrospective Analysis of Culture-Confirmed Enterococci Bloodstream Infections in South Africa, 2016–2020: A Cross-Sectional Study. Tropical Medicine and Infectious Disease. 2023; 8(1):19. https://doi.org/10.3390/tropicalmed8010019
Chicago/Turabian StyleMogokotleng, Ruth, Husna Ismail, Olga Perovic, and Sabelle Jallow. 2023. "A Retrospective Analysis of Culture-Confirmed Enterococci Bloodstream Infections in South Africa, 2016–2020: A Cross-Sectional Study" Tropical Medicine and Infectious Disease 8, no. 1: 19. https://doi.org/10.3390/tropicalmed8010019
APA StyleMogokotleng, R., Ismail, H., Perovic, O., & Jallow, S. (2023). A Retrospective Analysis of Culture-Confirmed Enterococci Bloodstream Infections in South Africa, 2016–2020: A Cross-Sectional Study. Tropical Medicine and Infectious Disease, 8(1), 19. https://doi.org/10.3390/tropicalmed8010019