


Comparison of Four Real-Time Polymerase Chain Reaction Assays for the Detection of SARS-CoV-2 in Respiratory Samples from Tunja, Boyacá, Colombia

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Collection and Preservation
2.3. RNA Extraction
2.4. Real-Time Polymerase Chain Reaction (RT-qPCR)
2.5. Statistical Analysis
3. Results
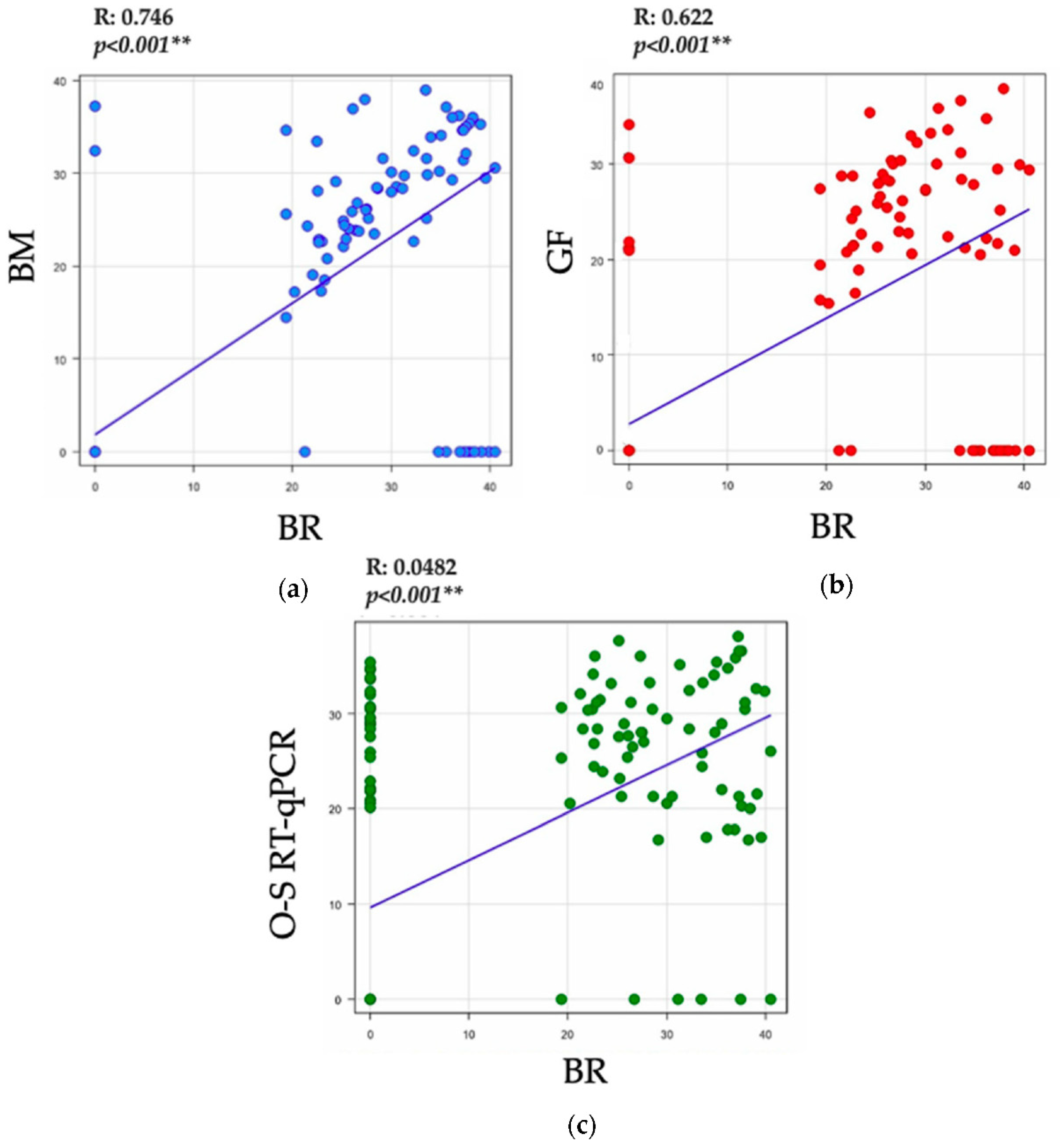
Comparison of the Results between the Four RT-qPCR Assays
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Wang, M.-Y.; Zhao, R.; Gao, L.-J.; Gao, X.-F.; Wang, D.-P.; Cao, J.-M. SARS-CoV-2: Structure, Biology, and Structure-Based Therapeutics Development. Front. Cell. Infect. Microbiol. 2020, 10, 587269. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Prasoon, P.; Kumari, C.; Pareek, V.; Faiq, M.A.; Narayan, R.K.; Kulandhasamy, M.; Kant, K. SARS-CoV-2-specific virulence factors in COVID-19. J. Med. Virol. 2021, 93, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Qin, C.; Liu, M.; Liu, J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: A systematic review and meta-analysis. Infect. Dis. Poverty 2021, 10, 132. [Google Scholar] [CrossRef] [PubMed]
- Ling, Y.; Zhong, J.; Luo, J. Safety and effectiveness of SARS-CoV-2 vaccines: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 6486–6495. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Jean, S.; Eltringham, R.; Madison, J.; Snyder, P.; Tu, H.; Jones, D.M.; Leber, A.L. Mutation-Specific SARS-CoV-2 PCR Screen: Rapid and Accurate Detection of Variants of Concern and the Identification of a Newly Emerging Variant with Spike L452R Mutation. J. Clin. Microbiol. 2021, 59, e00926-21. [Google Scholar] [CrossRef]
- Liu, M.; Li, Q.; Zhou, J.; Ai, W.; Zheng, X.; Zeng, J.; Liu, Y.; Xiang, X.; Guo, R.; Li, X.; et al. Value of swab types and collection time on SARS-CoV-2 detection using RT-PCR assay. J. Virol. Methods 2020, 286, 113974. [Google Scholar] [CrossRef] [PubMed]
- McAuley, J.; Fraser, C.; Paraskeva, E.; Trajcevska, E.; Sait, M.; Wang, N.; Bert, E.; Purcell, D.; Strugnell, R. Optimal preparation of SARS-CoV-2 viral transport medium for culture. Virol. J. 2021, 18, 53. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.L.L.; Rodríguez, R.B.; Mojica, F.I.L.; Andrade, J.L.C. Manual de Toma de Muestras para Análisis Microbiologico, 1st ed.; Saludcapital: Bogota, Colombia, 2015; Volume 2015. [Google Scholar]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.W.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef]
- Pecoraro, V.; Negro, A.; Pirotti, T.; Trenti, T. Estimate false-negative RT-PCR rates for SARS-CoV-2. A systematic review and meta-analysis. Eur. J. Clin. Investig. 2022, 52, e13706. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Zhou, Q.; Xu, J. Negative results in nucleic acid test of COVID-19 patients: Assessment from the perspective of clinical laboratories. Ann. Palliat. Med. 2020, 9, 4246–4251. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, H.; Horita, N.; Ushio, R.; Kato, I.; Nakajima, Y.; Ota, E.; Kaneko, T. Diagnostic test accuracy of antigenaemia assay for PCR-proven cytomegalovirus infection—systematic review and meta-analysis. Clin. Microbiol. Infect. 2017, 23, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Zhang, X.; Wei, C.; Yao, L.; Li, Y.; Xu, H.; Jia, Y.; Guo, R.; Wu, Y.; Yang, K.; et al. Diagnostic accuracy of in-house real-time PCR assay for Mycobacterium tuberculosis: A systematic review and meta-analysis. BMC Infect. Dis. 2019, 19, 701. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-K.; Oh, S.-H.; Yun, K.A.; Sung, H.; Kim, M.-N. Comparison of Anyplex II RV16 with the xTAG Respiratory Viral Panel and Seeplex RV15 for Detection of Respiratory Viruses. J. Clin. Microbiol. 2013, 51, 1137–1141. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gwyn, S.; Abubakar, A.; Akinmulero, O.; Bergeron, E.; Blessing, U.N.; Chaitram, J.; Coughlin, M.M.; Dawurung, A.B.; Dickson, F.N.; Esiekpe, M.; et al. Performance of SARS-CoV-2 Antigens in a Multiplex Bead Assay for Integrated Serological Surveillance of Neglected Tropical and Other Diseases. Am. J. Trop. Med. Hyg. 2022, 107, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Vogels, C.B.F.; Brito, A.F.; Wyllie, A.L.; Fauver, J.R.; Ott, I.M.; Kalinich, C.C.; Petrone, M.E.; Casanovas-Massana, A.; Muenker, M.C.; Moore, A.J.; et al. Analytical Sensitivity and Efficiency Comparisons of SARS-CoV-2 qRT-PCR Primer-Probe Sets. Nat. Microbiol. 2020, 5, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Zhou, J.; Niu, C.; Wang, Q.; Pan, Y.; Sheng, S.; Wang, X.; Zhang, Y.; Yang, J.; Liu, M.; et al. Highly accurate and sensitive diagnostic detection of SARS-CoV-2 by digital PCR. Talanta 2021, 224, 121726. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Feature | GF-TM | O-S RT-qPCR | BM | BR |
|---|---|---|---|---|
| Manufacturer | In Vitro Diagnostics | Vitro Master Diagnostica | Forest University | New England Biolabs |
| Sample types | Bronchoalveolar lavage fluid, nasopharyngeal swabs, oropharyngeal swabs, nasal swabs, mid-turbinate nasal swabs, or sputum specimens | Bronchoalveolar lavage fluid and nasopharyngeal swabs | Nasopharyngeal swabs and oropharyngeal swabs | Bronchoalveolar lavage fluid, nasopharyngeal swabs, and oropharyngeal swabs |
| Sample volume required | 5 μL | 8 μL | 5 μL | 5 μL |
| Extraction required | Yes | Yes | Yes | Yes |
| Target gene of SARS-CoV-2 | E, N, and RdRp | E and N | E and N | And |
| Internal quality control | RNAse P | RNAse P | RNAse P | RNAse P |
| Analytical sensitivity | RdRp: 10 copies/test | Gen N: 10 copies/test | Gen N: 10 copies/test | Gen N: 10 copies/test |
| N: 10 copies/test | Gen E: 10 copies/test | Gen E: 10 copies/test | Gen E: 10 copies/test | |
| E: 10 copies/test | ||||
| Analytical specificity | 1 | 1 | 1 | 1 |
| Maximum performance per kit | 100 samples | 100 samples | Not specified | 100 samples |
| Test run time | 1 h 35′ | 1 h 2′ | 1 h 5′ | 43′ |
| Recommended platform | Biosystems® 7500 Real-Time PCR Instrument (ABI 7500). StepOneTM Real-Time PCR System (Applied Biosystems). CFX96TM Real-Time PCR Detection System (Bio-Rad). | QuantStudioTM 3 Real-Time PCR System (Applied Biosystems). QuantStudioTM 5 Real-Time PCR System (Applied Biosystems). Biosystems® 7500 Real-Time PCR Instrument (ABI 7500). StepOne PlusTM Real-Time PCR System (Applied Biosystems). StepOneTM Real-Time PCR System (Applied Biosystems). CFX96TM Real-Time PCR Detection System (Bio-Rad). Rotor—Gene—Q (Qiagen). | CFX96TM Real-Time PCR Detection System (Bio-Rad). | CFX96TM Real-Time PCR Detection System (Bio-Rad). QuantStudioTM 5 Real-Time PCR System (Applied Biosystems). |
| Assay | BR Positive | BR Negative | Kappa (k) (±95% cL) | Sensitivity | Specificity | PPV | PNV | GIVES | |
|---|---|---|---|---|---|---|---|---|---|
| GF-TM | Positive | 69 | 6 | 0.92 | 100% | 92.70% | 92% | 100% | 96.05% |
| Negative | 0 | 77 | |||||||
| O-S RT-qPCR | Positive | 64 | 27 | 0.58 | 92.75% | 67.47% | 70.33% | 91.48% | 78.95% |
| Negative | 5 | 56 | |||||||
| BM | Positive | 69 | 3 | 0.96 | 100% | 96.39% | 100% | 95.87% | 98.30% |
| Negative | 0 | 80 | |||||||
| Test Result Variable | Area | Desv. Error a | Asymptotic Significance b | 95% Asymptotic Confidence Interval | |
|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||
| BM | 93.0% | 0.025 | <0.001 | 88% | 98% |
| GF-TM | 87.0% | 0.033 | <0.002 | 81% | 93% |
| O-S RT-qPCR | 79.7% | 0.037 | <0.003 | 72% | 87% |
| Gen/Reference Kit | Gen | Group/Kit | Normalized | Fold Change | Relative Expression | Error |
|---|---|---|---|---|---|---|
| E-BR | E | GF-TM | 2.75 | 0.00 | 1.00 | 8.26 |
| BM | 1.30 | −1.45 | 2.73 | 8.36 | ||
| E | GF-TM | 2.75 | 0.00 | 1.00 | 8.26 | |
| O-S RT-qPCR | 1.43 | −1.32 | 2.49 | 8.33 | ||
| E | BM | 1.30 | 0.00 | 1.00 | 8.36 | |
| O-S RT-qPCR | 1.43 | 0.13 | 0.91 | 8.33 | ||
| RNAse P-BR | RNAse P | GF-TM | 1.93 | 0.00 | 1.00 | 3.75 |
| BM | 0.61 | −1.32 | 2.50 | 2.75 | ||
| RNAse P | GF-TM | 1.93 | 0.00 | 1.00 | 3.75 | |
| O-S RT-qPCR | 1.40 | −0.53 | 1.44 | 6.54 | ||
| RNAse P | BM | 0.61 | 0.00 | 1.00 | 2.75 | |
| O-S RT-qPCR | 1.40 | 0.79 | 0.58 | 6.54 |
| RT-qPCR Assay | Advantages | Disadvantages |
|---|---|---|
| GF-TM | Identification of three target genes: genes E, N, and RdRp and their reagents | Dependency on commercial company |
| Kit for 100 tests | ||
| Easy-to-handle preparation of the reagents | High cost of market availability | |
| O-S RT-qPCR | Short amplification time compared to the other kits: 1 h 2’ | Dependence on commercial company |
| Identification of two gene targets: E and N | Kit for 100 tests | |
| BM | Identification of two target genes: E and N | Kit for 100 tests |
| Easy preparation of reagents for large volumes | High cost of market availability | |
| BR | Reference protocol for molecular detection developed by the Charité Virology Institute | Personnel required to prepare reagents |
| Recommended by PAHO for the universal monitoring of SARS-CoV-2 Kit for more than 1000 reactions | Manufacturer outside the country |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salamanca-Neita, L.H.; Carvajal, Ó.; Carvajal, J.P.; Forero-Castro, M.; Segura, N.A. Comparison of Four Real-Time Polymerase Chain Reaction Assays for the Detection of SARS-CoV-2 in Respiratory Samples from Tunja, Boyacá, Colombia. Trop. Med. Infect. Dis. 2022, 7, 240. https://doi.org/10.3390/tropicalmed7090240
Salamanca-Neita LH, Carvajal Ó, Carvajal JP, Forero-Castro M, Segura NA. Comparison of Four Real-Time Polymerase Chain Reaction Assays for the Detection of SARS-CoV-2 in Respiratory Samples from Tunja, Boyacá, Colombia. Tropical Medicine and Infectious Disease. 2022; 7(9):240. https://doi.org/10.3390/tropicalmed7090240
Chicago/Turabian StyleSalamanca-Neita, Lorenzo H., Óscar Carvajal, Juan Pablo Carvajal, Maribel Forero-Castro, and Nidya Alexandra Segura. 2022. "Comparison of Four Real-Time Polymerase Chain Reaction Assays for the Detection of SARS-CoV-2 in Respiratory Samples from Tunja, Boyacá, Colombia" Tropical Medicine and Infectious Disease 7, no. 9: 240. https://doi.org/10.3390/tropicalmed7090240
APA StyleSalamanca-Neita, L. H., Carvajal, Ó., Carvajal, J. P., Forero-Castro, M., & Segura, N. A. (2022). Comparison of Four Real-Time Polymerase Chain Reaction Assays for the Detection of SARS-CoV-2 in Respiratory Samples from Tunja, Boyacá, Colombia. Tropical Medicine and Infectious Disease, 7(9), 240. https://doi.org/10.3390/tropicalmed7090240