
Main Predictors of COVID-19 Vaccination Uptake among Italian Healthcare Workers in Relation to Variable Degrees of Hesitancy: Result from a Cross-Sectional Online Survey
 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
- -
- if they would accept the vaccination again;
- -
- if they have had any side effects after vaccination, and if these symptoms have led to the loss of working days.
- -
- if they believe vaccination is the best way to achieve an immune response;
- -
- if the vaccines currently available are safe and effective;
- -
- if the vaccination policies (currently decided by the government) are in their best interest;
- -
- if vaccines could have adverse effects on the immune system;
- -
- if the information received on vaccines and their safety was complete and reassuring;
- -
- if the authorities maintained a transparent attitude regarding the possible side effects of vaccination;
- -
- if it is important to be vaccinated to protect people who cannot be;
- -
- if information heard/read in the media or on social networks influenced their choice;
- -
- if they have been motivated to get vaccinated by previous vaccination experience;
- -
- whether they trust in the information received regarding the vaccine;
- -
- if they are aware that many of the vaccine-preventable diseases are serious;
- -
- whether the possibility of vaccination side effects made them question their decision;
- -
- whether they think the new vaccines have been tested to the same rigorous standard that normally applies to various drugs;
- -
- if they have been vaccinated by law;
- -
- if they are afraid of losing their job or of being suspended without pay in case of refusal.
2.3. Statistical Analysis
3. Results
3.1. Demographic and Job Characteristics
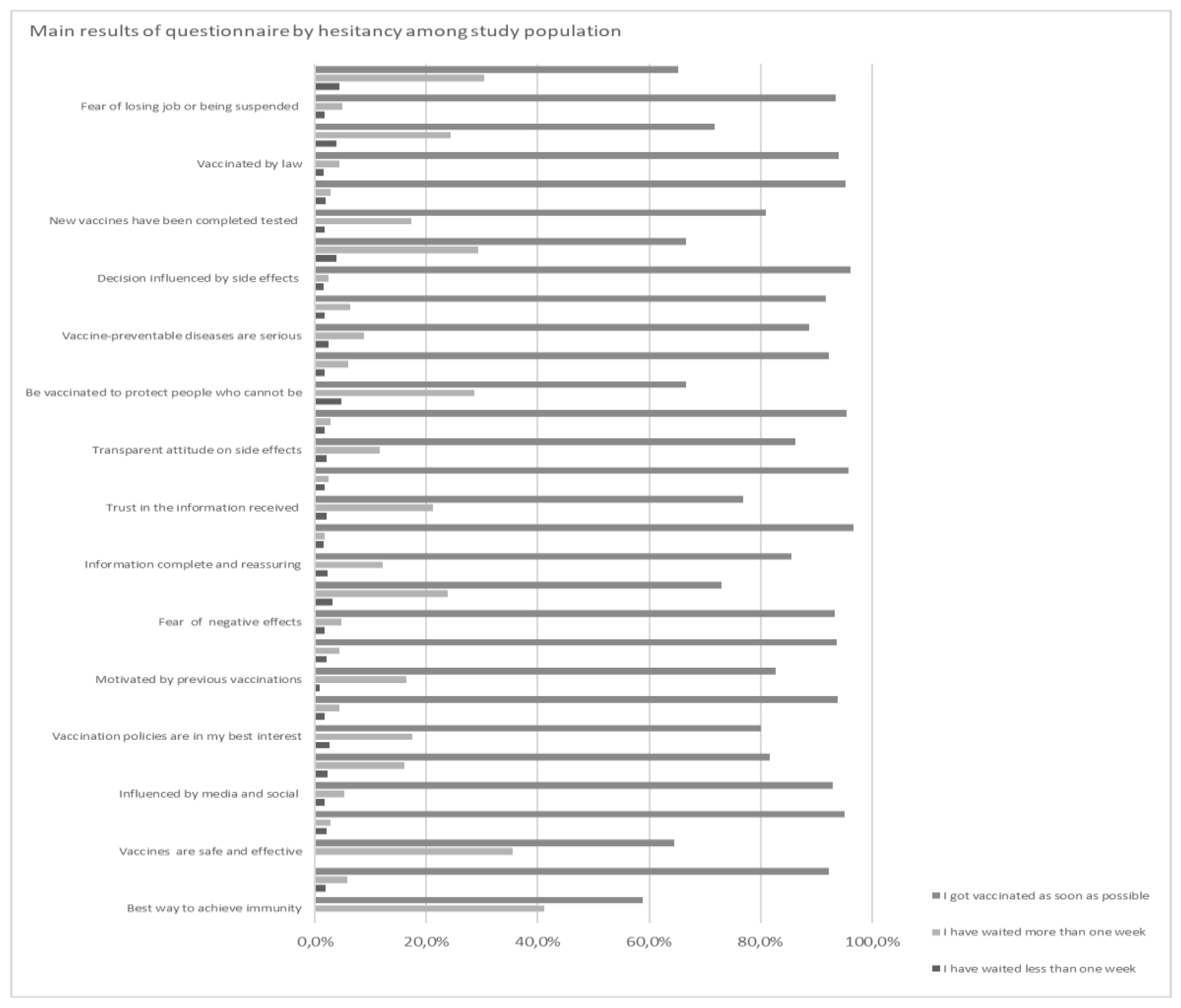
3.2. Results of the Questionnaire
3.3. Factors Associated with Vaccine Hesitancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharma, A.; Tiwari, S.; Deb, M.K.; Marty, J.L. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): A global pandemic and treatment strategies. Int. J. Antimicrob. Agents 2020, 56, 106054. [Google Scholar] [CrossRef] [PubMed]
- WHO. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 11 August 2022).
- Njoga, E.O.; Awoyomi, O.J.; Onwumere-Idolor, O.S.; Awoyomi, P.O.; Ugochukwu, I.C.I.; Ozioko, S.N. Persisting Vaccine Hesitancy in Africa: The Whys, Global Public Health Consequences and Ways-Out—COVID-19 Vaccination Acceptance Rates as Case-in-Point. Vaccines 2022, 10, 1934. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Umakanthan, S.; Lawrence, S. Predictors of COVID-19 vaccine hesitancy in Germany: A cross-sectional, population-based study. Postgrad. Med. J. 2022, 981164, 756–764. [Google Scholar] [CrossRef]
- MacDonald, N.E. SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar]
- CDC. COVID-19 Treatments and Medications. Available online: https://www.cdc.gov/coronavirus/2019-ncov/your-health/treatments-for-severe-illness.html (accessed on 1 September 2022).
- ECDC. Risk of SARS-CoV-2 Transmission from Newly Infected Individuals with Documented Previous Infection or Vaccination; Technical Report; ECDC: Solna, Sweden, 2021.
- Marks, M.; Millat-Martinez, P.; Ouchi, D.; Roberts, C.H.; Alemany, A.; Corbacho-Monné, M.; Ubals, M.; Tobias, A.; Tebé, C.; Ballana, E.; et al. Transmission of COVID-19 in 282 clusters in Catalonia, Spain: A cohort study. Lancet Infect Dis. 2021, 21, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Emary, K.R.W.; Golubchik, T.; Aley, P.K.; Ariani, C.V.; Angus, B.; Bibi, S.; Blane, B.; Bonsall, D.; Cicconi, P.; Charlton, S.; et al. COVID-19 Genomics UK consortium; AMPHEUS Project; Oxford COVID-19 Vaccine Trial Group. Efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS-CoV-2 variant of concern 202012/01 (B.1.1.7): An exploratory analysis of a randomised controlled trial. Lancet 2021, 397, 1351–1362. [Google Scholar] [CrossRef]
- Levine-Tiefenbrun, M.; Yelin, I.; Alapi, H.; Herzel, E.; Kuint, J.; Chodick, G.; Gazit, S.; Patalon, T.; Kishony, R. Waning of SARS-CoV-2 booster viral-load reduction effectiveness. Nat. Commun. 2022, 13, 1237. [Google Scholar] [CrossRef]
- Li, M.; Luo, Y.; Watson, R.; Zheng, Y.; Ren, J.; Tang, J.; Chen, Y. Healthcare workers’ (HCWs) attitudes and related factors towards COVID-19 vaccination: A rapid systematic review. Postgrad. Med. J. 2021, in press. [Google Scholar] [CrossRef]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.; Failla, G.; Ricciardi, W. Attitudes, acceptance and hesitancy among the general population worldwide to receive the COVID-19 vaccines and their contributing factors: A systematic review. EClinicalMedicine 2021, 40, 101113. [Google Scholar] [CrossRef]
- Woolf, K.; McManus, I.C.; Martin, C.A.; Nellums, L.B.; Guyatt, A.L.; Melbourne, C.; Bryant, L.; Gogoi, M.; Wobi, F.; Al-Oraibi, A.; et al. Ethnic differences in SARS-CoV-2 vaccine hesitancy in United Kingdom healthcare workers: Results from the UK-REACH prospective nationwide cohort study. Lancet Reg. Health Eur. 2021, 9, 100180. [Google Scholar] [CrossRef]
- Umakanthan, S.; Bukelo, M.M.; Gajula, S.S. The Commonwealth Caribbean COVID-19: Regions Resilient Pathway During Pandemic. Front. Public Health 2022, 10, 844333. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, F.P.; Stefanizzi, P.; Brescia, N.; Lattanzio, S.; Martinelli, A.; Tafuri, S. COVID-19 vaccination hesitancy in Italian healthcare workers: A systematic review and meta-analysis. Expert Rev. Vaccines 2022, 21, 1289–1300. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità. PASSI e PASSI d’Argento e la Pandemia COVID-19. National Tecnical Group “PASSI e PASSI d’Argento 2021”, ii, 39 p. ISS Report COVID-19 n. 5/2021. 2021. Available online: https://www.iss.it/documents/20126/0/Rapporto+ISS+COVID-19+5_2021.pdf (accessed on 6 March 2021).
- Petravić, L.; Arh, R.; Gabrovec, T.; Jazbec, L.; Rupčić, N.; Starešinič, N.; Zorman, L.; Pretnar, A.; Srakar, A.; Zwitter, M.; et al. Factors Affecting Attitudes towards COVID-19 Vaccination: An Online Survey in Slovenia. Vaccines 2021, 9, 247. [Google Scholar] [CrossRef]
- WHO. The Gender Pay Gap in the Health and Care Sector: A Global Analysis in the Time of COVID-19; World Health Organization: Geneva, Switzerland; International Labour Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Trabucco Aurilio, M.; Mennini, F.S.; Gazzillo, S.; Massini, L.; Bolcato, M.; Feola, A.; Ferrari, C.; Coppeta, L. Intention to Be Vaccinated for COVID-19 among Italian Nurses during the Pandemic. Vaccines 2021, 9, 500. [Google Scholar] [CrossRef]
- WHO. COVID-19 Weekly Epidemiological Update Data as Received by WHO from National Authorities as of 14 February, 2.0.2.1.; 10 am, C.E.T. Weekly Epidemiological Update. 16 February 2021. Available online: file:///C:/Users/HP/Downloads/20210216_Weekly_Epi_Update_27.pdf (accessed on 11 August 2022).
- Bolcato, M.; Aurilio, M.T.; Aprile, A.; Di Mizio, G.; Della Pietra, B.; Feola, A. Take-Home Messages from the COVID-19 Pandemic: Strengths and Pitfalls of the Italian National Health Service from a Medico-Legal Point of View. Healthcare 2020, 9, 17. [Google Scholar] [CrossRef]
- Brborović, O.; Brborović, H.; Hrain, L. The COVID-19 Pandemic Crisis and Patient Safety Culture: A Mixed-Method Study. Int. J. Env. Res. Public Health 2022, 19, 2237. [Google Scholar] [CrossRef] [PubMed]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M.; Gagnon, D.; Robitaille, L.; Cook, E.; Caron, I.; Talib, A.; Parkes, L.; et al. Covid-19 vaccine acceptance, hesitancy, and refusal among Canadian healthcare workers: A multicenter survey. Am. J. Infect Control 2021, 49, 1152–1157. [Google Scholar] [CrossRef] [PubMed]
- Alvarado-Socarras, J.L.; Vesga-Varela, A.L.; Quintero-Lesmes, D.C.; Fama-Pereira, M.M.; Serrano-Diaz, N.C.; Vasco, M.; Carballo-Zarate, V.; Zambrano, L.I.; Paniz-Mondolfi, A.; Rodriguez-Morales, A.J. Perception of COVID-19 Vaccination Amongst Physicians in Colombia. Vaccines 2021, 9, 287. [Google Scholar] [CrossRef]
- Dias-Godói, I.P.; Tadeu Rocha Sarmento, T.; Afonso Reis, E.; Peres Gargano, L.; Godman, B.; de Assis Acurcio, F.; Alvares-Teodoro, J.; Guerra Júnior, A.A.; Mariano Ruas, C. Acceptability and willingness to pay for a hypothetical vaccine against SARS CoV-2 by the Brazilian consumer: A cross-sectional study and the implications. Expert Rev. Pharm. Outcomes Res. 2022, 22, 119–129. [Google Scholar] [CrossRef]
- Adeniyi, O.V.; Stead, D.; Singata-Madliki, M.; Batting, J.; Wright, M.; Jelliman, E.; Abrahams, S.; Parrish, A. Acceptance of COVID-19 Vaccine among the Healthcare Workers in the Eastern Cape, South Africa: A Cross Sectional Study. Vaccines 2021, 9, 666. [Google Scholar] [CrossRef] [PubMed]
- Kozak, A.; Nienhaus, A. COVID-19 Vaccination: Status and Willingness to Be Vaccinated among Employees in Health and Welfare Care in Germany. Int. J. Environ. Res. Public Health 2021, 18, 6688. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, F.; Murri, R.; Segala, F.V.; Cerruti, L.; Abdulle, A.; Saracino, A.; Bavaro, D.F.; Fantoni, M. Attitudes towards Anti-SARS-CoV2 Vaccination among Healthcare Workers: Results from a National Survey in Italy. Viruses 2021, 13, 371. [Google Scholar] [CrossRef]
- Tran, V.D.; Pak, T.V.; Gribkova, E.I.; Galkina, G.A.; Loskutova, E.E.; Dorofeeva, V.V.; Dewey, R.S.; Nguyen, K.T.; Pham, D.T. Determinants of covid-19 vaccine acceptance in a high infection-rate country: A cross-sectional study in Russia. Pharm. Pract. 2021, 19, 2276. [Google Scholar] [CrossRef]
- Jennings, W.; Stoker, G.; Bunting, H.; Valgarðsson, V.O.; Gaskell, J.; Devine, D.; McKay, L.; Mills, M.C. Lack of Trust, Conspiracy Beliefs, and Social Media Use Predict COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 593. [Google Scholar] [CrossRef]
- Caserotti, M.; Gavaruzzi, T.; Girardi, P.; Tasso, A.; Buizza, C.; Candini, V.; Zarbo, C.; Chiarotti, F.; Brescianini, S.; Calamandrei, G.; et al. Who is likely to vacillate in their COVID-19 vaccination decision? Free-riding intention and post-positive reluctance. Prev. Med. 2021, 154, 106885. [Google Scholar] [CrossRef]
- Allington, D.; McAndrew, S.; Moxham-Hall, V.; Duffy, B. Coronavirus conspiracy suspicions, general vaccine attitudes, trust and coronavirus information source as predictors of vaccine hesitancy among UK residents during the COVID-19 pandemic. Psychol. Med. 2021, 12, 1–12. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors associated with COVID-19 vaccine hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef] [PubMed]
- Diament, S.M.; Kaya, A.; Magenheim, E.B. Frames that matter: Increasing the willingness to get the COVID-19 vaccines. Soc. Sci. Med. 2022, 292, 114562. [Google Scholar] [CrossRef] [PubMed]
- Prematunge, C.; Corace, K.; McCarthy, A.; Nair, R.C.; Pugsley, R.; Garber, G. Factors influencing pandemic influenza vaccination of healthcare workers—A systematic review. Vaccine 2012, 30, 4733–4743. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 and Mandatory Vaccination: Ethical Considerations and Caveats: Policy Brief. 2021. Available online: https://apps.who.int/iris/handle/10665/340841 (accessed on 11 August 2022).
- Mills, M.C.; Rüttenauer, T. The effect of mandatory COVID-19 certificates on vaccine uptake: Synthetic-control modelling of six countries. Lancet Public Health 2022, 7, e15–e22. [Google Scholar] [CrossRef] [PubMed]
- Scientific Advisory Group for Emergencies (SAGE): Ethnicity Sub-Group. Factors Influencing COVID-19 Vaccine Uptake among Minority Ethnic Groups. 2021. Available online: https://www.gov.uk/government/publications/factors-influencing-covid-19-vaccine-uptake-among-minority-ethnic-groups-17-december-2020 (accessed on 11 August 2022).

{kind=link}
| Did You Get Vaccinated as Soon as You Were Offered the Vaccine or did You Take Some Time to Think about it? | ||||||||
|---|---|---|---|---|---|---|---|---|
| I Have Waited Less Than One Week | I Have Waited More Than One Week | I Got Vaccinated as Soon as Possible | ||||||
| Count | Row Valid N % | Count | Row Valid N % | Count | Row Valid N % | p Value | ||
| Vaccination is the best way to achieve an immune response | No | 0 | 0.00% | 7 | 41.20% | 10 | 58.80% | p < 0.01 |
| Yes | 12 | 1.90% | 36 | 5.80% | 578 | 92.30% | ||
| Vaccines currently available are safe and effective | No | 0 | 0.00% | 27 | 35.50% | 49 | 64.50% | p < 0.01 |
| Yes | 12 | 2.10% | 16 | 2.80% | 539 | 95.10% | ||
| The information heard/read on the media or on social networks influenced the choice | No | 10 | 1.80% | 29 | 5.20% | 516 | 93.00% | p < 0.01 |
| Yes | 2 | 2.30% | 14 | 16.10% | 71 | 81.60% | ||
| The vaccination policies currently decided by the government are in my best interest | No | 3 | 2.60% | 20 | 17.40% | 92 | 80.00% | p < 0.01 |
| Yes | 9 | 1.70% | 23 | 4.40% | 496 | 93.90% | ||
| Motivated to get vaccinated by previous experiences with vaccinations | No | 1 | 0.80% | 21 | 16.40% | 106 | 82.80% | p < 0.01 |
| Yes | 11 | 2.10% | 22 | 4.30% | 482 | 93.60% | ||
| Vaccines can have negative effects on the immune system | No | 10 | 1.70% | 28 | 4.80% | 540 | 93.40% | p < 0.01 |
| Yes | 2 | 3.20% | 15 | 23.80% | 46 | 73.00% | ||
| The information received on vaccines and their safety was complete and reassuring | No | 7 | 2.30% | 37 | 12.20% | 260 | 85.50% | p < 0.01 |
| Yes | 5 | 1.50% | 6 | 1.80% | 327 | 96.70% | ||
| Trust in the information received regarding the vaccine | No | 3 | 2.00% | 31 | 21.10% | 113 | 76.90% | p < 0.01 |
| Yes | 9 | 1.80% | 12 | 2.40% | 474 | 95.80% | ||
| The authorities have maintained a transparent attitude regarding the possible side effects of vaccination | No | 6 | 2.10% | 33 | 11.70% | 244 | 86.20% | p < 0.01 |
| Yes | 6 | 1.70% | 10 | 2.80% | 342 | 95.50% | ||
| It is important to be vaccinated to protect people who cannot be | No | 1 | 4.80% | 6 | 28.60% | 14 | 66.70% | p < 0.01 |
| Yes | 11 | 1.80% | 37 | 6.00% | 573 | 92.30% | ||
| Aware that many of the vaccine-preventable diseases are serious | No | 2 | 2.50% | 7 | 8.80% | 71 | 88.80% | p < 0.05 |
| Yes | 10 | 1.80% | 36 | 6.40% | 515 | 91.80% | ||
| The possibility of side effects from vaccination made you question your decision | No | 8 | 1.50% | 13 | 2.40% | 518 | 96.10% | p < 0.01 |
| Yes | 4 | 3.90% | 30 | 29.40% | 68 | 66.70% | ||
| Think that the new vaccines have been tested with the same rigorous standard that normally applies to various drugs | No | 3 | 1.70% | 30 | 17.30% | 140 | 80.90% | p < 0.01 |
| Yes | 9 | 1.90% | 13 | 2.80% | 446 | 95.30% | ||
| Vaccinated by law | No | 9 | 1.60% | 24 | 4.30% | 531 | 94.10% | p < 0.01 |
| Yes | 3 | 3.80% | 19 | 24.40% | 56 | 71.80% | ||
| Fear of losing job or being suspended without salary in case of refusal | No | 10 | 1.70% | 29 | 4.90% | 557 | 93.50% | p < 0.01 |
| Yes | 2 | 4.30% | 14 | 30.40% | 30 | 65.20% | ||
| Did You Get Vaccinated as Soon as you Were Offered the Vaccine or did You Take Some Time to Think about it? | ||||||||
|---|---|---|---|---|---|---|---|---|
| I Have Waited Less Than One Week | I Have Waited More Than One Week | I Got Vaccinated as Soon as Possible | ||||||
| Count | Row Valid N % | Count | Row Valid N % | Count | Row Valid N % | p Value | ||
| Gender | Female | 9 | 1.80% | 35 | 6.80% | 443 | 86.70% | p < 0.05 |
| Male | 3 | 1.20% | 14 | 5.70% | 225 | 91.50% | ||
| Age | >45 | 5 | 1.80% | 13 | 4.70% | 249 | 89.20% | p < 0.05 |
| <45 | 7 | 1.50% | 36 | 7.60% | 416 | 87.60% | ||
| Nurse | No | 8 | 1.30% | 41 | 6.70% | 539 | 88.20% | p < 0.05 |
| Yes | 4 | 2.70% | 8 | 5.50% | 129 | 88.40% | ||
| High risk setting | No | 0 | 0.00% | 0 | 0.00% | 8 | 1.80% | p < 0.05 |
| Yes | 0 | 0.00% | 0 | 0.00% | 11 | 3.60% | ||
| Working area | Clinic | 1 | 1.10% | 6 | 6.30% | 85 | 89.50% | p = 0.29 |
| Home Assistance | 1 | 4.50% | 3 | 13.60% | 17 | 77.30% | ||
| Nursing Homes | 0 | 0.00% | 3 | 15.00% | 17 | 85.00% | ||
| Hospital | 4 | 1.40% | 13 | 4.50% | 267 | 92.10% | ||
| COVID-19 areas | 0 | 0.00% | 0 | 0.00% | 14 | 100.00% | ||
| Other | 6 | 1.90% | 24 | 7.60% | 268 | 84.80% | ||
| Regions | Abruzzo | 0 | 0.00% | 0 | 0.00% | 5 | 100.00% | p = 0.73 |
| Sicilia | 0 | 0.00% | 0 | 0.00% | 4 | 100.00% | ||
| Basilicata | 0 | 0.00% | 0 | 0.00% | 15 | 100.00% | ||
| Calabria | 0 | 0.00% | 1 | 16.70% | 5 | 83.30% | ||
| Campania | 2 | 1.00% | 18 | 8.90% | 172 | 85.10% | ||
| Emilia Romagna | 0 | 0.00% | 2 | 14.30% | 11 | 78.60% | ||
| Friuli Venezia Giulia | 0 | 0.00% | 2 | 13.30% | 13 | 86.70% | ||
| Lazio | 5 | 2.50% | 12 | 5.90% | 185 | 90.70% | ||
| Liguria | 0 | 0.00% | 0 | 0.00% | 6 | 100.00% | ||
| Lombardia | 0 | 0.00% | 3 | 10.00% | 24 | 80.00% | ||
| Marche | 0 | 0.00% | 0 | 0.00% | 2 | 100.00% | ||
| Molise | 2 | 1.20% | 5 | 3.00% | 150 | 88.80% | ||
| Piemonte | 1 | 11.10% | 0 | 0.00% | 8 | 88.90% | ||
| Puglia | 0 | 0.00% | 0 | 0.00% | 7 | 100.00% | ||
| Sardegna | 1 | 6.30% | 2 | 12.50% | 13 | 81.30% | ||
| Toscana | 1 | 2.70% | 2 | 5.40% | 34 | 91.90% | ||
| Valle d’Aosta | 0 | 0.00% | 0 | 0.00% | 1 | 100.00% | ||
| Veneto | 0 | 0.00% | 2 | 13.30% | 13 | 86.70% | ||
| Profession | Nurse | 4 | 2.70% | 8 | 5.50% | 129 | 88.40% | p < 0.05 |
| Medical doctor | 6 | 1.90% | 17 | 5.30% | 290 | 90.60% | ||
| Psychologist | 0 | 0.00% | 17 | 11.60% | 118 | 80.30% | ||
| Student | 0 | 0.00% | 4 | 4.40% | 86 | 94.50% | ||
| Other HCWs | 2 | 3.80% | 3 | 5.70% | 45 | 84.90% | ||
| B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for EXP(B) | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Age < 45 years | 0.244 | 0.384 | 0.403 | 1 | 0.526 | 10.276 | 0.244 | 0.384 |
| Male gender | −0.028 | 0.396 | 0.005 | 1 | 0.944 | 0.973 | −0.028 | 0.396 |
| Vaccination is the best way to achieve an immune response | 0.268 | 0.680 | 0.156 | 1 | 0.693 | 10.308 | 0.268 | 0.680 |
| Vaccines currently available are safe and effective | −10.075 | 0.476 | 50.095 | 1 | 0.024 | 0.341 | −10.075 | 0.476 |
| The information heard/read on the media or on social networks influenced the choice | 0.448 | 0.394 | 10.288 | 1 | 0.256 | 10.565 | 0.448 | 0.394 |
| The vaccination policies currently decided by the government are in my best interest | 0.004 | 0.426 | 0.000 | 1 | 0.993 | 10.004 | 0.004 | 0.426 |
| Motivated to get vaccinated by previous experiences with vaccinations | −0.015 | 0.395 | 0.001 | 1 | 0.969 | 0.985 | −0.015 | 0.395 |
| Vaccines can have negative effects on the immune system | 0.399 | 0.440 | 0.823 | 1 | 0.364 | 10.490 | 0.399 | 0.440 |
| The information received on vaccines and their safety was complete and reassuring | −0.253 | 0.489 | 0.267 | 1 | 0.605 | 0.777 | −0.253 | 0.489 |
| Trust in the information received regarding the vaccine | −0.295 | 0.492 | 0.359 | 1 | 0.549 | 0.745 | −0.295 | 0.492 |
| The authorities have maintained a transparent attitude regarding the possible side effects of vaccination | −0.222 | 0.404 | 0.301 | 1 | 0.583 | 0.801 | −0.222 | 0.404 |
| It is important to be vaccinated to protect people who cannot be | −0.848 | 0.672 | 10.589 | 1 | 0.207 | 0.428 | −0.848 | 0.672 |
| Aware that many of the vaccine-preventable diseases are serious | 0.348 | 0.481 | 0.522 | 1 | 0.470 | 10.416 | 0.348 | 0.481 |
| The possibility of side effects from vaccination made you question your decision | 10.522 | 0.405 | 140.134 | 1 | 0.000 | 40.581 | 10.522 | 0.405 |
| Think that the new vaccines have been tested with the same rigorous standard that normally applies to various drugs | 0.040 | 0.435 | 0.008 | 1 | 0.927 | 10.041 | 0.040 | 0.435 |
| Vaccinated by law | 0.444 | 0.448 | 0.982 | 1 | 0.322 | 10.559 | 0.444 | 0.448 |
| Fear of losing job or being suspended without salary in case of refusal | 0.236 | 0.510 | 0.214 | 1 | 0.644 | 10.266 | 0.236 | 0.510 |
| Nurse job | 0.344 | 0.436 | 0.623 | 1 | 0.430 | 10.411 | 0.344 | 0.436 |
| Profession | Total | |||||
|---|---|---|---|---|---|---|
| Medical Doctor | Nurse | Other HCWs | ||||
| Vaccinated | No | Count | 7 | 5 | 15 | 27 |
| % within profession | 2.2% | 3.4% | 5.2% | 3.6% | ||
| Yes | Count | 313 | 141 | 276 | 730 | |
| % within profession | 97.8% | 96.6% | 94.8% | 96.4% | ||
| Total | Count | 320 | 146 | 291 | 757 | |
| % within profession | 100.0% | 100.0% | 100.0% | 100.0% | ||
| Chi-Square Tests | ||||||
| Value | df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) | Exact Sig. (1-sided) | Point Probability | |
| Pearson Chi-Square | 3.912 | 2 | 0.141 | 0.138 | ||
| Likelihood Ratio | 3.936 | 2 | 0.140 | 0.133 | ||
| Fisher’s Exact Test | 3.836 | 0.132 | ||||
| Linear-by-Linear Association | 3.886 | 1 | 0.049 | 0.050 | 0.031 | 0.013 |
| N of Valid Cases | 757 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trabucco Aurilio, M.; Mennini, F.S.; Ferrari, C.; Somma, G.; Di Giampaolo, L.; Bolcato, M.; De-Giorgio, F.; Muscatello, R.; Magrini, A.; Coppeta, L. Main Predictors of COVID-19 Vaccination Uptake among Italian Healthcare Workers in Relation to Variable Degrees of Hesitancy: Result from a Cross-Sectional Online Survey. Trop. Med. Infect. Dis. 2022, 7, 419. https://doi.org/10.3390/tropicalmed7120419
Trabucco Aurilio M, Mennini FS, Ferrari C, Somma G, Di Giampaolo L, Bolcato M, De-Giorgio F, Muscatello R, Magrini A, Coppeta L. Main Predictors of COVID-19 Vaccination Uptake among Italian Healthcare Workers in Relation to Variable Degrees of Hesitancy: Result from a Cross-Sectional Online Survey. Tropical Medicine and Infectious Disease. 2022; 7(12):419. https://doi.org/10.3390/tropicalmed7120419
Chicago/Turabian StyleTrabucco Aurilio, Marco, Francesco Saverio Mennini, Cristiana Ferrari, Giuseppina Somma, Luca Di Giampaolo, Matteo Bolcato, Fabio De-Giorgio, Roberto Muscatello, Andrea Magrini, and Luca Coppeta. 2022. "Main Predictors of COVID-19 Vaccination Uptake among Italian Healthcare Workers in Relation to Variable Degrees of Hesitancy: Result from a Cross-Sectional Online Survey" Tropical Medicine and Infectious Disease 7, no. 12: 419. https://doi.org/10.3390/tropicalmed7120419
APA StyleTrabucco Aurilio, M., Mennini, F. S., Ferrari, C., Somma, G., Di Giampaolo, L., Bolcato, M., De-Giorgio, F., Muscatello, R., Magrini, A., & Coppeta, L. (2022). Main Predictors of COVID-19 Vaccination Uptake among Italian Healthcare Workers in Relation to Variable Degrees of Hesitancy: Result from a Cross-Sectional Online Survey. Tropical Medicine and Infectious Disease, 7(12), 419. https://doi.org/10.3390/tropicalmed7120419