
High Prevalence of Methicillin-Resistant Staphylococcus aureus among Healthcare Facilities and Its Related Factors in Myanmar (2018–2019)

 , ,
, ,
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Setting
2.2.1. General Setting
2.2.2. Specific Setting
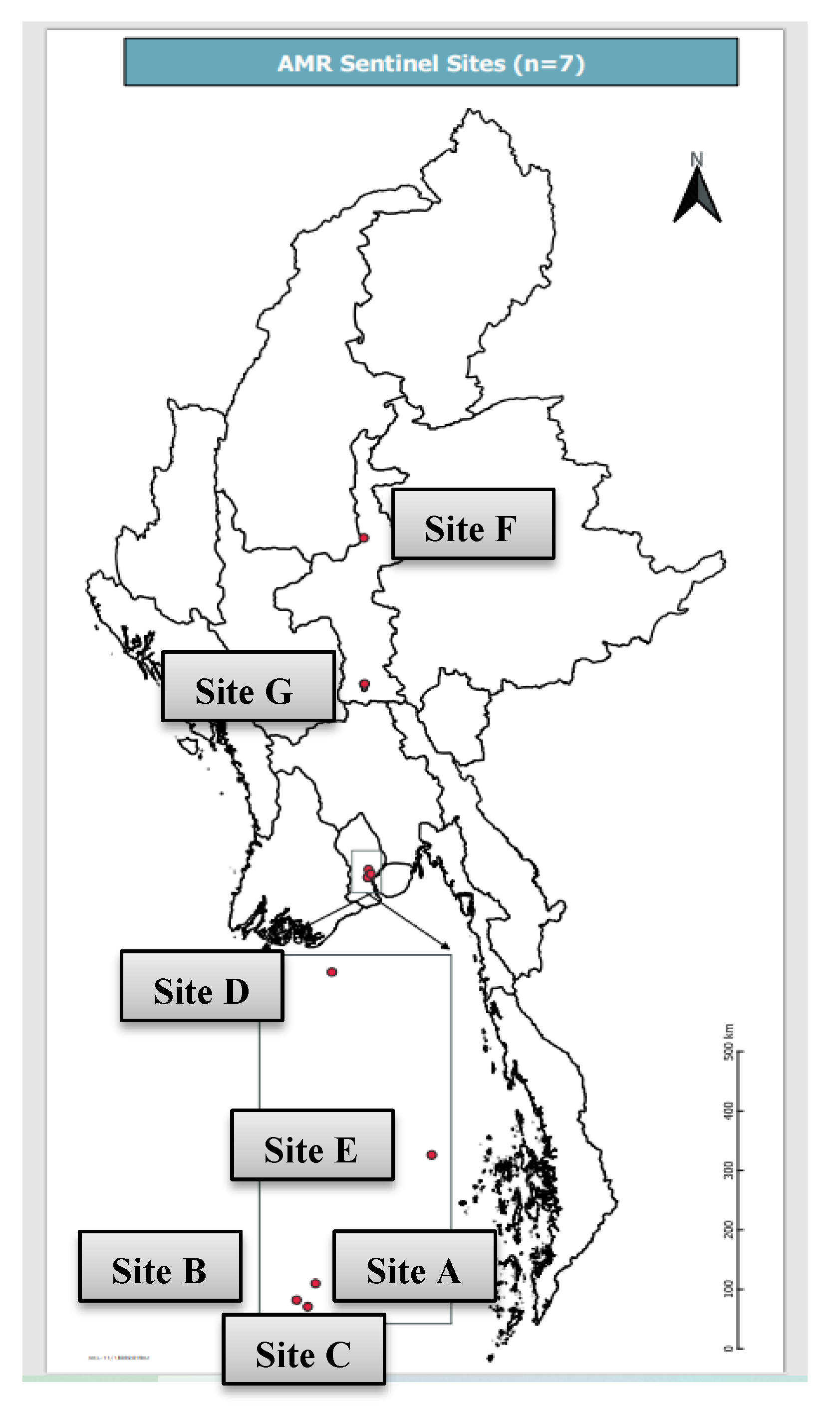
2.2.3. AMR Surveillance in Myanmar
2.2.4. Laboratory Procedure
2.3. Study Population and Period
2.4. Data Variables and Sources of Data
2.5. Data Collection, Analysis and Statistics
3. Results
3.1. Culture and Sensitivity of SA
3.2. Antibiotic Susceptibility Pattern of SA
3.3. Distribution of SA Infection among the Isolates
3.4. Prevalence of SA and MRSA in Seven AMR Sentinel Sites
3.5. Factors Associated with MRSA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef]
- Turner, N.A.; Sharma-Kuinkel, B.K.; Maskarinec, S.A.; Eichenberger, E.M.; Shah, P.P.; Carugati, M.; Holland, T.L.; Fowler, V.G. Methicillin-resistant Staphylococcus aureus: An overview of basic and clinical research. Nat. Rev. Microbiol. 2019, 17, 203–218. [Google Scholar] [CrossRef]
- Kourtis, A.P.; Hatfield, K.; Baggs, J.; Mu, Y.; See, I.; Epson, E.; Nadle, J.; Kainer, M.A.; Dumyati, G.; Petit, S.; et al. Vital Signs: Epidemiology and Recent Trends in Methicillin-Resistant and in Methicillin-Susceptible Staphylococcus aureus Bloodstream Infections—United States. MMWR Morb. Mortal. Wkly. Rep. 2019. [Google Scholar] [CrossRef]
- Mendes, R.E.; Mendoza, M.; Banga Singh, K.K.; Castanheira, M.; Bell, J.M.; Turnidge, J.D.; Lin, S.S.F.; Jones, R.N. Regional resistance surveillance program results for 12 Asia-Pacific nations (2011). Antimicrob. Agents Chemother. 2013, 57, 5721–5726. [Google Scholar] [CrossRef] [PubMed]
- Zhen, X.; Lundborg, C.S.; Zhang, M.; Sun, X.; Li, Y.; Hu, X.; Gu, S.; Gu, Y.; Wei, J.; Dong, H. Clinical and economic impact of methicillin-resistant Staphylococcus aureus: A multicentre study in China. Sci. Rep. 2020. [Google Scholar] [CrossRef]
- Tatokoro, M.; Kihara, K.; Masuda, H.; Ito, M.; Yoshida, S.; Kijima, T.; Yokoyama, M.; Saito, K.; Koga, F.; Kawakami, S.; et al. Successful reduction of hospital-acquired methicillin-resistant Staphylococcus aureus in a urology ward: A 10-year study. BMC Urol. 2013, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- Duerden, B.; Fry, C.; Johnson, A.P.; Wilcox, M.H. The Control of Methicillin-Resistant Staphylococcus aureus Blood Stream Infections in England. Open Forum Infect. Dis. 2015, 2. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, A.H.; Koirala, J. Methicillin Resistant Staphylococcus Aureus (MRSA); StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Marimuthu, K.; Pittet, D.; Harbarth, S. The effect of improved hand hygiene on nosocomial MRSA control. Antimicrob. Resist. Infect. Control 2014, 3, 1–6. [Google Scholar] [CrossRef]
- Aung, M.S.; Zi, H.; Nwe, K.M.; Maw, W.W.; Aung, M.T.; Min, W.W.; Nyein, N.; Kawaguchiya, M.; Urushibara, N.; Sumi, A.; et al. Drug resistance and genetic characteristics of clinical isolates of staphylococci in Myanmar: High prevalence of PVL among methicillin-susceptible Staphylococcus aureus belonging to various sequence types. New Microbes New Infect. 2016, 10, 58–65. [Google Scholar] [CrossRef]
- Aung, M.S.; San, T.; Aye, M.M.; Mya, S.; Maw, W.W.; Zan, K.N.; Htut, W.H.W.; Kawaguchiya, M.; Urushibara, N.; Kobayashi, N. Prevalence and Genetic Characteristics of Staphylococcus aureus and Staphylococcus argenteus Isolates Harboring Panton-Valentine Leukocidin, Enterotoxins, and TSST-1 Genes from Food Handlers in Myanmar. Toxins 2017, 9, 241. [Google Scholar] [CrossRef]
- Myaing, T.T.; Thaw, K.K.; Htun, L.L.; Mhon, M.M.; Bawm, S.; Linn, K.S.; Wai, S.S. Antimicrobial resistant pattern of methicillin-resistant Staphylococcus aureus isolated from stray dogs’ nasal swabs to fifteen antimicrobials in Myanmar. Int. J. Infect. Dis. 2016, 53, 48. [Google Scholar] [CrossRef][Green Version]
- Aung, M.S.; San, T.; Urushibara, N.; San, N.; Oo, W.M.; Soe, P.E.; Kyaw, Y.; Ko, P.M.; Thu, P.P.; Hlaing, M.S. Molecular Characterization of Methicillin-Susceptible and-Resistant Staphylococcus aureus Harboring Panton-Valentine Leukocidin-Encoding Bacteriophages in a Tertiary Care Hospital in Myanmar. Microb. Drug Resist. 2020, 26, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Myat, T.O.; Prasad, N.; Thinn, K.K.; Win, K.K.; Htike, W.W.; Zin, K.N.; Murdoch, D.R.; Crump, J.A. Bloodstream infections at a tertiary referral hospital in Yangon, Myanmar. Trans. R. Soc. Trop. Med. Hyg. 2014, 108, 692–698. [Google Scholar] [CrossRef]
- Ministry of Health and Sports. Hospital Infection Control Guidelines; Ministry of Health and Sports: Naypyitaw, Myanmar, 2016.
- CLSI CLSI M100-ED29: 2019 Performance Standards for Antimicrobial Susceptibility Testing, 29th ed.; Clinical and Laboratory: Standards Institute: Wayne, PA, USA, 2019; ISBN 9781684400324.
- Thi, K.S.; Moe, Z.W.; Thein, K.N. GP242 Early onset sepsis in extramural hospital of myanmar(burma). BMJ 2019, 104. [Google Scholar] [CrossRef]
- Myat, T.O.; Oo, K.M.; Mone, H.K.; Htike, W.W.; Biswas, A.; Hannaway, R.F.; Murdoch, D.R.; Ussher, J.E.; Crump, J.A. A prospective study of bloodstream infections among febrile adolescents and adults attending Yangon general hospital, Yangon, Myanmar. PLoS Negl. Trop. Dis. 2020. [Google Scholar] [CrossRef]
- Sapkota, J.; Sharma, M.; Jha, B.; Bhatt, C.P. Prevalence of staphylococcus aureus isolated from clinical samples in a tertiary care hospital: A descriptive cross-sectional study. J. Nepal Med. Assoc. 2019. [Google Scholar] [CrossRef]
- Abdelghafar, A.A.; Yousef, N.; Askora, M. Prevalence and antimicrobial susceptibility patterns of Staphylococcus aureus isolated from different clinical sources. Zagazig J. Pharm. Sci. 2020, 29, 1–8. [Google Scholar] [CrossRef]
- Wong, J.W.H.; Ip, M.; Tang, A.; Wei, V.W.I.; Wong, S.Y.S.; Riley, S.; Read, J.M.; Kwok, K.O. Prevalence and risk factors of community-associated methicillin-resistant staphylococcus aureus carriage in asia-pacific region from 2000 to 2016: A systematic review and meta-analysis. Clin. Epidemiol. 2018, 10, 1489. [Google Scholar] [CrossRef] [PubMed]
- Wi, Y.M.; Rhee, J.Y.; Kang, C.I.; Chung, D.R.; Song, J.H.; Peck, K.R. Clinical predictors of methicillin-resistance and their impact on mortality associated with Staphylococcus aureus bacteraemia. Epidemiol. Infect. 2018, 146, 1326–1336. [Google Scholar] [CrossRef]
- Khanal, L.K.; Adhikari, R.P.; Guragain, A. Prevalence of Methicillin Resistant Staphylococcus aureus and Antibiotic Susceptibility Pattern in a Tertiary Hospital in Nepal. J. Nepal Health Res. Counc. 2018. [Google Scholar] [CrossRef]
- Kaur Heyar, A.; Kaur Gill, A.; Mahajan, A.; Kaur, K. Prevalence and Antibiotic Sensitivity Pattern of Staphylococcus Aureus From All Clinical Samples With Emphasis on Mrsa in a Tertiary Care Hospital. J. Evol. Med. Dent. Sci. 2017, 6, 5857–5860. [Google Scholar] [CrossRef]
- National Health Laboratory Analysis Report on Hospital Antimicrobial Resistance in Myanmar 2016; National Health Laboratory: Yangon, Myanmar, 2018.
- National Health Laboratory Analysis Report on Hospital Antimicrobial Resistance in Myanmar 2017; National Health Laboratory: Yangon, Myanmar, 2019.
- Hanif, E.; Hassan, S.A. Evaluation of antibiotic resistance pattern in clinical isolates of Staphylococcus aureus. Pak. J. Pharm. Sci. 2019, 32, 1749–1753. [Google Scholar]
- Vamsi Muni Krishna, P.; Sreenivasulu Reddy, V.; Praveen Kumar, V.; Suresh, P. Antibiotic suscepyibility pattern of staphylococcus aureus and methicillin–resistant staphylococcus aureus isolated from various clinical specimens in a tertiary care teaching hospital, Pondicherry. Indian J. Public Heal. Res. Dev. 2019, 10, 266–271. [Google Scholar] [CrossRef]
- Shariati, A.; Dadashi, M.; Moghadam, M.T.; van Belkum, A.; Yaslianifard, S.; Darban-Sarokhalil, D. Global prevalence and distribution of vancomycin resistant, vancomycin intermediate and heterogeneously vancomycin intermediate Staphylococcus aureus clinical isolates: A systematic review and meta-analysis. Sci. Rep. 2020. [Google Scholar] [CrossRef] [PubMed]
- Pennell, L.M.; Galligan, C.L.; Fish, E.N. Sex affects immunity. J. Autoimmun. 2012, 38, J282–J291. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Wu, H.; Soe, M.; Pollock, D.; Edwards, J. Risk Factors Associated with Hospital-Onset MRSA Proportion—National Healthcare Safety Network, 2017–2018. Infect. Control Hosp. Epidemiol. 2020, 41, s375–s376. [Google Scholar] [CrossRef]
- Ghia, C.J.; Waghela, S.; Rambhad, G. A Systemic Literature Review and Meta-Analysis Reporting the Prevalence and Impact of Methicillin-Resistant Staphylococcus aureus Infection in India. Infect. Dis. Res. Treat. 2020, 13, 1178633720970569. [Google Scholar] [CrossRef]
- Abubakar, U.; Sulaiman, S.A.S. Prevalence, trend and antimicrobial susceptibility of Methicillin Resistant Staphylococcus aureus in Nigeria: A systematic review. J. Infect. Public Health 2018, 11, 763–770. [Google Scholar] [CrossRef]
- Nsofor, C.A. Prevalence and Antibiotic Susceptibility Pattern of Staphylococcus Aureus Isolated from Various Clinical Specimens in South East Nigeria. MOJ Cell Sci. Rep. 2016. [Google Scholar] [CrossRef]
- Hawkins, G.; Stewart, S.; Blatchford, O.; Reilly, J. Should healthcare workers be screened routinely for meticillin-resistant Staphylococcus aureus? A review of the evidence. J. Hosp. Infect. 2011, 77, 285–289. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Drug | Zone Diameter Breakpoints (mm) | MIC Breakpoints (µg/mL) | ||||
|---|---|---|---|---|---|---|
| S | I | R | S | I | R | |
| First-Line Drugs | ||||||
| Cefoxitin | ≥22 | - | ≤21 | ≤4 | - | ≥8 |
| Oxacillin | - | - | - | ≤2 | - | ≥4 |
| Penicillin | ≥29 | - | ≤28 | ≤0.12 | - | ≥0.25 |
| Clindamycin | ≥21 | 15–20 | ≤14 | ≤0.5 | 1–2 | ≥4 |
| Erythromycin | ≥23 | 14–22 | ≤13 | ≤0.5 | 1–4 | ≥8 |
| Cotrimoxazole | ≥16 | 11–15 | ≤10 | <2/38 | - | ≥4/76 |
| Nitrofurantoin | ≥17 | 15–16 | ≤14 | ≤32 | 64 | ≥128 |
| Second-Line Drugs | ||||||
| Linezolid | ≥21 | - | ≤20 | ≤4 | - | ≥8 |
| Tetracycline | ≥19 | 15–18 | ≤14 | ≤4 | 8 | ≥16 |
| Vancomycin | - | - | - | ≤2 | 4–8 | ≥8 |
| Rifampicin | ≥20 | 17–19 | ≤16 | ≤1 | 2 | ≥4 |
| Gentamicin | ≥15 | 13–14 | ≤12 | ≤4 | 8 | ≥16 |
| Ciprofloxacin | ≥21 | 16–20 | ≤15 | ≤1 | 2 | ≥4 |
| Levofloxacin | ≥19 | 16–18 | ≤15 | ≤1 | 2 | ≥4 |
| Antibiotic Name (n) | Sensitive | Intermediate | Resistant | |||
|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | |
| First-line drugs | ||||||
| Cefoxitin (n = 2753) | 1422 | (52) | 0 | (0) | 1331 | (48) |
| Penicillin (n = 1302) | 35 | (3) | 0 | (0) | 1267 | (97) |
| Clindamycin (n = 2755) | 1710 | (62) | 112 | (4) | 933 | (34) |
| Erythromycin (n = 2704) | 1211 | (45) | 206 | (8) | 1287 | (48) |
| Cotrimoxazole (n = 2678) | 1565 | (58) | 39 | (1) | 1074 | (40) |
| Nitrofurantoin (n = 1332) | 1287 | (97) | 12 | (1) | 33 | (2) |
| Second-line drugs | ||||||
| Linezolid (n = 2624) | 2375 | (91) | 0 | (0) | 249 | (9) |
| Tetracycline (n = 1426) | 833 | (58) | 6 | (0) | 587 | (41) |
| Vancomycin (n = 1249) | 1124 | (90) | 30 | (2) | 95 | (8) |
| Rifampicin (n = 1258) | 1032 | (82) | 54 | (4) | 172 | (14) |
| Gentamicin (n = 2754) | 1816 | (66) | 79 | (3) | 859 | (31) |
| Ciprofloxacin (n = 1409) | 1006 | (71) | 46 | (3) | 357 | (25) |
| Levofloxacin (n = 2765) | 1812 | (66) | 68 | (2) | 885 | (32) |
| Variable | Patients Whose Isolates Were Tested Positive with SA Infection (2018, n = 1324) | Patients Whose Isolates Were Tested Positive with SA Infection (2019, n = 1477) | ||
|---|---|---|---|---|
| n | (%) | N | (%) | |
| Age (years) | ||||
| <15 | 274 | (21) | 284 | (19) |
| 15–44 | 502 | (38) | 545 | (37) |
| 45–64 | 363 | (27) | 448 | (30) |
| ≥65 | 173 | (13) | 186 | (13) |
| Unknown | 12 | (1) | 14 | (1) |
| Gender | ||||
| Male | 711 | (54) | 802 | (54) |
| Female | 609 | (46) | 672 | (46) |
| Unknown | 4 | (0) | 3 | (0) |
| Type of Patient | ||||
| Inpatient | 1046 | (79) | 1324 | (90) |
| Outpatient | 229 | (17) | 101 | (7) |
| Unknown | 49 | (4) | 52 | (4) |
| Type of Specimen | ||||
| Blood | 282 | (21) | 474 | (32) |
| Sputum/Respiratory | 149 | (11) | 172 | (12) |
| Urine | 107 | (8) | 105 | (7) |
| Wound (pus/swab) | 664 | (50) | 647 | (44) |
| Body fluid | 30 | (2) | 8 | (1) |
| Miscellaneous | 92 | (7) | 71 | (5) |
| Source of patient | ||||
| Medical | 370 | (28) | 472 | (32) |
| Surgical | 443 | (33) | 494 | (33) |
| Paediatric | 55 | (4) | 150 | (10) |
| ICU | 61 | (5) | 57 | (4) |
| Dermatology | 133 | (10) | 99 | (7) |
| Emergency/OPD | 94 | (7) | 81 | (5) |
| Unknown | 89 | (7) | 80 | (5) |
| Others | 79 | (6) | 44 | (3) |
| Sites | 2018 | 2019 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Isolates | Gram-Positive (n, %) | SA (n, %) | MRSA (n, %) | Total Isolates | Gram-Positive (n, %) | SA (n, %) | MRSA (n, %) | |||||||
| Site A | 1773 | 398 | (22) | 87 | (22) | 23 | (26) | 1388 | 287 | (21) | 56 | (20) | 18 | (32) |
| Site B | 5028 | 1570 | (31) | 298 | (19) | 114 | (38) | 5484 | 1877 | (34) | 348 | (19) | 124 | (36) |
| Site C | 1355 | 182 | (13) | 48 | (26) | 20 | (42) | 1279 | 228 | (18) | 71 | (31) | 17 | (24) |
| Site D | 4088 | 629 | (15) | 186 | (30) | 78 | (42) | 3378 | 625 | (21) | 187 | (27) | 89 | (48) |
| Site E | 2967 | 278 | (9) | 140 | (50) | 55 | (39) | 2880 | 391 | (14) | 106 | (27) | 23 | (22) |
| Site F | 3294 | 628 | (19) | 508 | (81) | 388 | (76) | 3371 | 796 | (24) | 607 | (76) | 359 | (59) |
| Site G | 480 | 110 | (23) | 57 | (52) | 10 | (18) | 1033 | 175 | (17) | 102 | (58) | 13 | (13) |
| Total | 18,985 | 3795 | 1324 | 688 | 18,813 | 4397 | 1477 | 643 | ||||||
| Variable | Patients with SA Infection (N = 2801) | Patients with MRSA Infection (N = 1331) | Prevalence Ratio (95% CI) | Adjusted PR (95% CI) | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| n | n | (%) | ||||||
| Year | ||||||||
| 2018 | 1324 | 688 | (52) | Ref | Ref | |||
| 2019 | 1477 | 643 | (44) | 0.84 | (0.78–0.91) | 0.86 | (0.80–0.92) | <0.001 |
| Age (years) | ||||||||
| <15 | 558 | 256 | (46) | Ref | Ref | |||
| 15–44 | 1047 | 482 | (46) | 0.99 | (0.89–1.11) | 1.15 | (1.02–1.31) | 0.021 |
| 45–64 | 811 | 399 | (49) | 1.06 | (0.94–1.19) | 1.19 | (1.04–1.35) | <0.001 |
| ≥65 | 359 | 185 | (52) | 1.11 | (0.97–1.27) | 1.27 | (1.09–1.47) | 0.001 |
| Unknown | 26 | 9 | (35) | 0.73 | (0.43–1.25) | 0.80 | (0.46–1.40) | 0.451 |
| Gender | ||||||||
| Male | 1513 | 692 | (46) | 0.92 | (0.85–1.00) | 0.92 | (0.86–0.99) | 0.034 |
| Female | 1281 | 634 | (49) | Ref | ||||
| Unknown | 7 | 5 | (71) | 1.42 | (0.88–2.27) | 1.86 | (0.91–3.80) | 0.144 |
| Type of Patient | ||||||||
| Inpatient | 2370 | 1105 | (47) | Ref | Ref | |||
| Outpatient | 330 | 185 | (56) | 1.22 | (1.10–1.36) | 1.07 | (0.93–1.24) | 0.296 |
| Unknown | 101 | 41 | (41) | 0.85 | (0.67–1.08) | 0.86 | (0.66–1.11) | 0.265 |
| Type of Specimen | ||||||||
| Blood | 756 | 390 | (52) | Ref | Ref | |||
| Sputum/Respiratory | 321 | 172 | (54) | 1.03 | (0.91–1.16) | 1.00 | (0.89–1.13) | 0.870 |
| Urine | 212 | 143 | (68) | 1.35 | (1.20–1.50) | 1.21 | (1.08–1.36) | 0.001 |
| Wound (pus/swab) | 1311 | 524 | (40) | 0.78 | (0.71–0.86) | 0.98 | (0.88–1.09) | 0.754 |
| Body fluid | 38 | 17 | (45) | 0.86 | (0.60–1.23) | 0.77 | (0.53–1.11) | 0.164 |
| Miscellaneous | 163 | 85 | (52) | 1.02 | (0.87–1.20) | 1.15 | (0.97–1.35) | 0.088 |
| Source of Patient | ||||||||
| Medical | 842 | 413 | (49) | Ref | Ref | |||
| Surgical | 937 | 353 | (38) | 0.77 | (0.70–0.86) | 0.83 | (0.75–0.94) | 0.003 |
| Paediatric | 205 | 103 | (50) | 1.02 | (0.88–1.19) | 0.87 | (0.73–1.05) | 0.154 |
| ICU | 118 | 87 | (74) | 1.49 | (1.31–1.69) | 1.16 | (1.03–1.30) | 0.013 |
| Dermatology | 232 | 153 | (66) | 1.34 | (1.19–1.50) | 2.04 | (1.73–2.40) | <0.001 |
| OPD/Emergency | 175 | 90 | (51) | 1.06 | (0.90–1.24) | 0.91 | (0.74–1.11) | 0.388 |
| Unknown | 169 | 54 | (32) | 0.67 | (0.53–0.84) | 1.13 | (0.79–1.61) | 0.487 |
| Others | 123 | 78 | (63) | 1.32 | (0.14–1.53) | 1.17 | (1.01–1.36) | 0.037 |
| Laboratory Sites | ||||||||
| Site F | 1115 | 747 | (67) | Ref | Ref | |||
| Site A | 143 | 41 | (29) | 0.44 | (0.34–0.57) | 0.38 | (0.25–0.59) | <0.001 |
| Site B | 646 | 238 | (37) | 0.55 | (0.49–0.61) | 0.41 | (0.36–0.47) | <0.001 |
| Site C | 119 | 37 | (31) | 0.46 | (0.35–0.60) | 0.47 | (0.35–0.62) | <0.001 |
| Site D | 373 | 167 | (45) | 0.66 | (0.58–0.74) | 0.56 | (0.49–0.65) | <0.001 |
| Site E | 246 | 78 | (32) | 0.47 | (0.39–0.57) | 0.49 | (0.41–0.60) | <0.001 |
| Site G | 159 | 23 | (15) | 0.24 | (0.16–0.35) | 0.28 | (0.19–0.41) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soe, P.E.; Han, W.W.; Sagili, K.D.; Satyanarayana, S.; Shrestha, P.; Htoon, T.T.; Tin, H.H. High Prevalence of Methicillin-Resistant Staphylococcus aureus among Healthcare Facilities and Its Related Factors in Myanmar (2018–2019). Trop. Med. Infect. Dis. 2021, 6, 70. https://doi.org/10.3390/tropicalmed6020070
Soe PE, Han WW, Sagili KD, Satyanarayana S, Shrestha P, Htoon TT, Tin HH. High Prevalence of Methicillin-Resistant Staphylococcus aureus among Healthcare Facilities and Its Related Factors in Myanmar (2018–2019). Tropical Medicine and Infectious Disease. 2021; 6(2):70. https://doi.org/10.3390/tropicalmed6020070
Chicago/Turabian StyleSoe, Pan Ei, Wai Wai Han, Karuna D. Sagili, Srinath Satyanarayana, Priyanka Shrestha, Thi Thi Htoon, and Htay Htay Tin. 2021. "High Prevalence of Methicillin-Resistant Staphylococcus aureus among Healthcare Facilities and Its Related Factors in Myanmar (2018–2019)" Tropical Medicine and Infectious Disease 6, no. 2: 70. https://doi.org/10.3390/tropicalmed6020070
APA StyleSoe, P. E., Han, W. W., Sagili, K. D., Satyanarayana, S., Shrestha, P., Htoon, T. T., & Tin, H. H. (2021). High Prevalence of Methicillin-Resistant Staphylococcus aureus among Healthcare Facilities and Its Related Factors in Myanmar (2018–2019). Tropical Medicine and Infectious Disease, 6(2), 70. https://doi.org/10.3390/tropicalmed6020070