Effects of Meglumine Antimoniate Treatment on Cytokine Production in a Patient with Mucosal Leishmaniasis and Chagas Diseases Co-Infection

 ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
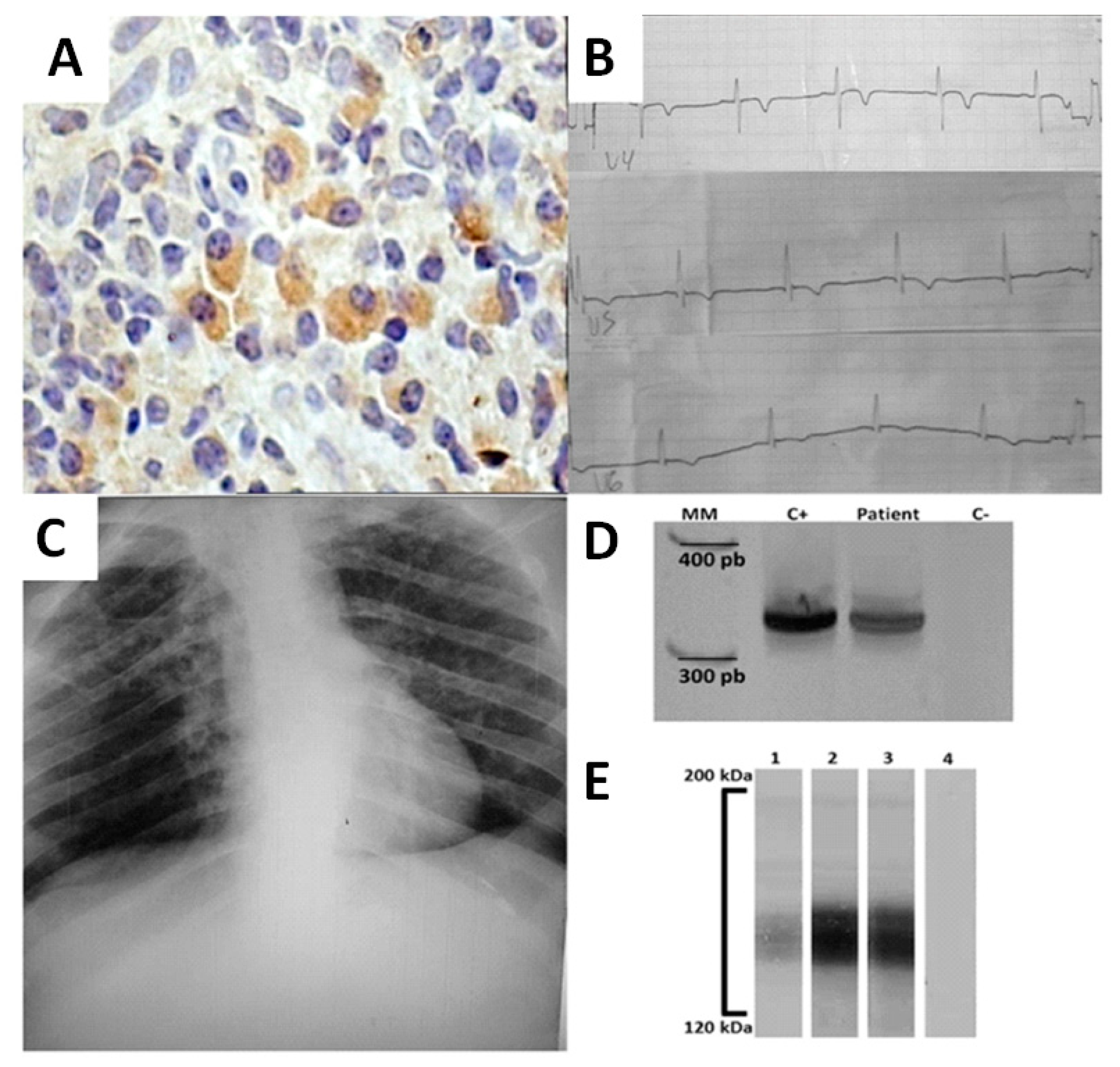
2. Case Report
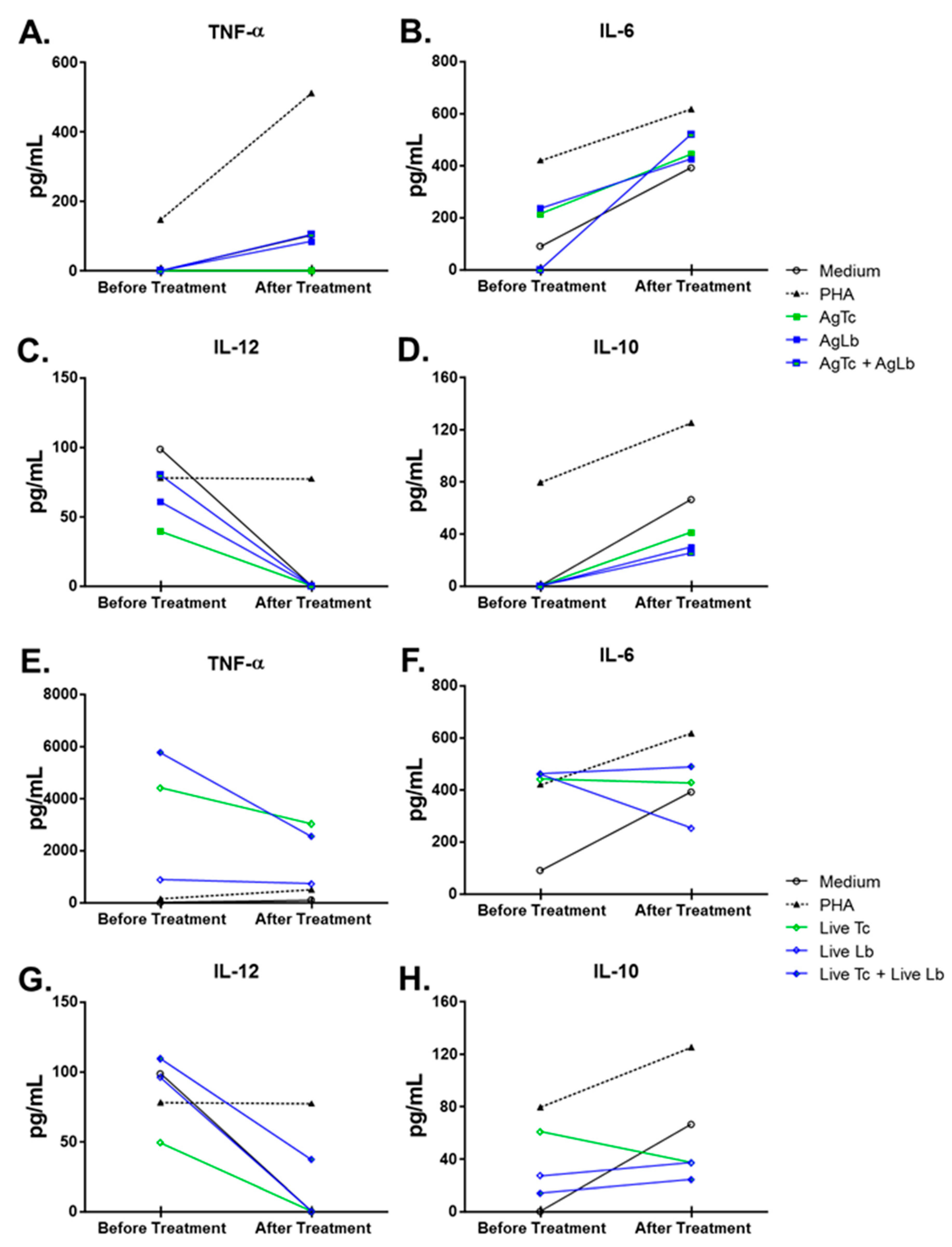
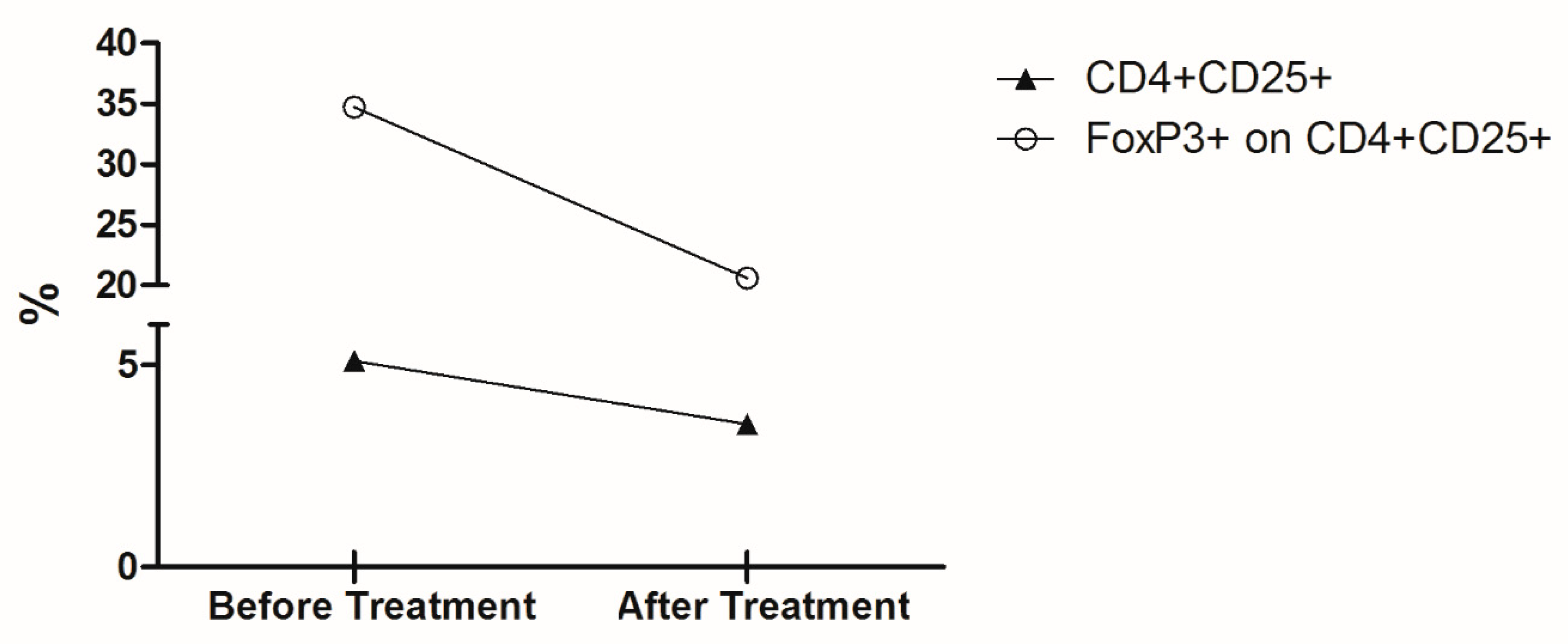
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Sustaining the Drive to Overcome the Global Impact of Neglected Tropical Diseases: Second WHO Report on Neglected Diseases; WHO: Geneva, Switzerland, 2013; p. 138. [Google Scholar]
- Coura, J.R.; Borges-Pereira, J. Chagas disease. What is known and what should be improved: A systemic review. Rev. Soc. Bras. Med. Trop. 2012, 45, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Reithinger, R.; Dujardin, J.C.; Louzir, H.; Pirmez, C.; Alexander, B.; Brooker, S. Cutaneous leishmaniasis. Lancet Infect. Dis. 2007, 7, 581–596. [Google Scholar] [CrossRef]
- Malchiodi, E.L.; Chiaramonte, M.G.; Taranto, N.J.; Zwirner, N.W.; Margni, R.A. Cross-reactivity studies and differential serodiagnosis of human infections caused by Trypanosoma cruzi and Leishmania spp; use of immunoblotting and ELISA with a purified antigen (Ag163B6). Clin. Exp. Immunol. 1994, 97, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Chiaramonte, M.G.; Zwirner, N.W.; Caropresi, S.L.; Taranto, N.J.; Malchiodi, E.L. Trypanosoma cruzi and Leishmania spp. human mixed infection. Am. J. Trop. Med. Hyg. 1996, 54, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Chiaramonte, M.G.; Frank, F.M.; Furer, G.M.; Taranto, N.J.; Margni, R.A.; Malchiodi, E.L. Polymerase chain reaction reveals Trypanosoma cruzi infection suspected by serology in cutaneous and mucocutaneous leishmaniasis patients. Acta Trop. 1999, 72, 295–308. [Google Scholar] [CrossRef]
- Passos, V.M.; Volpini, A.C.; Braga, E.M.; Lacerda, P.A.; Ouaissi, A.; Lima-Martins, M.V.; Krettli, A.U. Differential serodiagnosis of human infections caused by Trypanosoma cruzi and Leishmania spp. using ELISA with a recombinant antigen (rTc24). Mem. Inst. Oswaldo Cruz 1997, 92, 791–793. [Google Scholar] [CrossRef] [PubMed]
- Frank, F.M.; Fernandez, M.M.; Taranto, N.J.; Cajal, S.P.; Margni, R.A.; Castro, E.; Thomaz-Soccol, V.; Malchiodi, E.L. Characterization of human infection by Leishmania spp. in the Northwest of Argentina: Immune response, double infection with Trypanosoma cruzi and species of Leishmania involved. Parasitology 2003, 126, 31–39. [Google Scholar] [CrossRef]
- Gil, J.; Cimino, R.; Lopez Quiroga, I.; Cajal, S.; Acosta, N.; Juarez, M.; Zacca, R.; Orellana, V.; Krolewiecki, A.; Diosque, P.; et al. [Reactivity of GST-SAPA antigen of Trypanosoma cruzi against sera from patients with Chagas disease and leishmaniasis]. Medicina 2011, 71, 113–119. [Google Scholar]
- Wincker, P.; Bosseno, M.F.; Britto, C.; Yaksic, N.; Cardoso, M.A.; Morel, C.M.; Breniere, S.F. High correlation between Chagas’ disease serology and PCR-based detection of Trypanosoma cruzi kinetoplast DNA in Bolivian children living in an endemic area. FEMS Microbiol. Lett. 1994, 124, 419–423. [Google Scholar] [CrossRef]
- Castellano, L.R.; Filho, D.C.; Argiro, L.; Dessein, H.; Prata, A.; Dessein, A.; Rodrigues, V. Th1/Th2 immune responses are associated with active cutaneous leishmaniasis and clinical cure is associated with strong interferon-gamma production. Hum. Immunol. 2009, 70, 383–390. [Google Scholar] [CrossRef]
- Rezende-Oliveira, K.; Sarmento, R.R.; Rodrigues, V., Jr. Production of cytokine and chemokines by human mononuclear cells and whole blood cells after infection with Trypanosoma cruzi. Rev. Soc. Bras. Med. Trop. 2012, 45, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Salhi, A.; Rodrigues, V., Jr.; Santoro, F.; Dessein, H.; Romano, A.; Castellano, L.R.; Sertorio, M.; Rafati, S.; Chevillard, C.; Prata, A.; et al. Immunological and genetic evidence for a crucial role of IL-10 in cutaneous lesions in humans infected with Leishmania braziliensis. J. Immunol. 2008, 180, 6139–6148. [Google Scholar] [CrossRef] [PubMed]
- Campanelli, A.P.; Roselino, A.M.; Cavassani, K.A.; Pereira, M.S.; Mortara, R.A.; Brodskyn, C.I.; Goncalves, H.S.; Belkaid, Y.; Barral-Netto, M.; Barral, A.; et al. CD4+CD25+ T cells in skin lesions of patients with cutaneous leishmaniasis exhibit phenotypic and functional characteristics of natural regulatory T cells. J. Infect. Dis. 2006, 193, 1313–1322. [Google Scholar] [CrossRef] [PubMed]
- de Araujo, F.F.; Correa-Oliveira, R.; Rocha, M.O.; Chaves, A.T.; Fiuza, J.A.; Fares, R.C.; Ferreira, K.S.; Nunes, M.C.; Keesen, T.S.; Damasio, M.P.; et al. Foxp3+CD25(high) CD4+ regulatory T cells from indeterminate patients with Chagas disease can suppress the effector cells and cytokines and reveal altered correlations with disease severity. Immunobiology 2012, 217, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Da-Cruz, A.M.; Bittar, R.; Mattos, M.; Oliveira-Neto, M.P.; Nogueira, R.; Pinho-Ribeiro, V.; Azeredo-Coutinho, R.B.; Coutinho, S.G. T-cell-mediated immune responses in patients with cutaneous or mucosal leishmaniasis: Long-term evaluation after therapy. Clin. Diagn. Lab. Immunol. 2002, 9, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Brelaz-de-Castro, M.C.; de Almeida, A.F.; de Oliveira, A.P.; de Assis-Souza, M.; da Rocha, L.F.; Pereira, V.R. Cellular immune response evaluation of cutaneous leishmaniasis patients cells stimulated with Leishmania (Viannia) braziliensis antigenic fractions before and after clinical cure. Cell. Immunol. 2012, 279, 180–186. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Matos, G.I.; Covas Cde, J.; Bittar Rde, C.; Gomes-Silva, A.; Marques, F.; Maniero, V.C.; Amato, V.S.; Oliveira-Neto, M.P.; Mattos Mda, S.; Pirmez, C.; et al. IFNG +874T/A polymorphism is not associated with American tegumentary leishmaniasis susceptibility but can influence Leishmania induced IFN-gamma production. BMC Infect. Dis. 2007, 7, 33. [Google Scholar] [CrossRef]
- Cabrera, M.; Shaw, M.A.; Sharples, C.; Williams, H.; Castes, M.; Convit, J.; Blackwell, J.M. Polymorphism in tumor necrosis factor genes associated with mucocutaneous leishmaniasis. J. Exp. Med. 1995, 182, 1259–1264. [Google Scholar] [CrossRef]
- de Saldanha, R.R.; Martins-Papa, M.C.; Sampaio, R.N.; Muniz-Junqueira, M.I. Meglumine antimonate treatment enhances phagocytosis and TNF-alpha production by monocytes in human cutaneous leishmaniasis. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 596–603. [Google Scholar] [CrossRef]
- Guedes, P.M.; Gutierrez, F.R.; Silva, G.K.; Dellalibera-Joviliano, R.; Rodrigues, G.J.; Bendhack, L.M.; Rassi, A., Jr.; Rassi, A.; Schmidt, A.; Maciel, B.C.; et al. Deficient regulatory T cell activity and low frequency of IL-17-producing T cells correlate with the extent of cardiomyopathy in human Chagas’ disease. PLoS Negl. Trop. Dis. 2012, 6, e1630. [Google Scholar] [CrossRef]
- Wanidworanun, C.; Strober, W. Predominant role of tumor necrosis factor-alpha in human monocyte IL-10 synthesis. J. Immunol. 1993, 151, 6853–6861. [Google Scholar] [PubMed]
- Pissetti, C.W.; Correia, D.; de Oliveira, R.F.; Llaguno, M.M.; Balarin, M.A.; Silva-Grecco, R.L.; Rodrigues, V., Jr. Genetic and functional role of TNF-alpha in the development Trypanosoma cruzi infection. PLoS Negl. Trop. Dis. 2011, 5, e976. [Google Scholar] [CrossRef] [PubMed]
- Reis, D.D.; Jones, E.M.; Tostes, S., Jr.; Lopes, E.R.; Gazzinelli, G.; Colley, D.G.; McCurley, T.L. Characterization of inflammatory infiltrates in chronic chagasic myocardial lesions: Presence of tumor necrosis factor-alpha+ cells and dominance of granzyme A+, CD8+ lymphocytes. Am. J. Trop. Med. Hyg. 1993, 48, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Rocha Rodrigues, D.B.; dos Reis, M.A.; Romano, A.; Pereira, S.A.; Teixeira Vde, P.; Tostes, S., Jr.; Rodrigues, V., Jr. In situ expression of regulatory cytokines by heart inflammatory cells in Chagas’ disease patients with heart failure. Clin. Dev. Immunol. 2012, 2012, 361730. [Google Scholar] [CrossRef] [PubMed]
- Sadeghian, G.; Ziaei, H.; Sadeghi, M. Electrocardiographic changes in patients with cutaneous leishmaniasis treated with systemic glucantime. Ann. Acad. Med. Singap. 2008, 37, 916–918. [Google Scholar]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rezende-Oliveira, K.; Gómez-Hernández, C.; Silva, M.V.d.; Faria de Oliveira, R.; Reis Machado, J.; de Almeida Silva Teixeira, L.; Castellano, L.R.C.; Correia, D.; Rodrigues, V. Effects of Meglumine Antimoniate Treatment on Cytokine Production in a Patient with Mucosal Leishmaniasis and Chagas Diseases Co-Infection. Trop. Med. Infect. Dis. 2020, 5, 69. https://doi.org/10.3390/tropicalmed5020069
Rezende-Oliveira K, Gómez-Hernández C, Silva MVd, Faria de Oliveira R, Reis Machado J, de Almeida Silva Teixeira L, Castellano LRC, Correia D, Rodrigues V. Effects of Meglumine Antimoniate Treatment on Cytokine Production in a Patient with Mucosal Leishmaniasis and Chagas Diseases Co-Infection. Tropical Medicine and Infectious Disease. 2020; 5(2):69. https://doi.org/10.3390/tropicalmed5020069
Chicago/Turabian StyleRezende-Oliveira, Karine, Cesar Gómez-Hernández, Marcos Vinícius da Silva, Rafael Faria de Oliveira, Juliana Reis Machado, Luciana de Almeida Silva Teixeira, Lúcio Roberto Cançado Castellano, Dalmo Correia, and Virmondes Rodrigues. 2020. "Effects of Meglumine Antimoniate Treatment on Cytokine Production in a Patient with Mucosal Leishmaniasis and Chagas Diseases Co-Infection" Tropical Medicine and Infectious Disease 5, no. 2: 69. https://doi.org/10.3390/tropicalmed5020069
APA StyleRezende-Oliveira, K., Gómez-Hernández, C., Silva, M. V. d., Faria de Oliveira, R., Reis Machado, J., de Almeida Silva Teixeira, L., Castellano, L. R. C., Correia, D., & Rodrigues, V. (2020). Effects of Meglumine Antimoniate Treatment on Cytokine Production in a Patient with Mucosal Leishmaniasis and Chagas Diseases Co-Infection. Tropical Medicine and Infectious Disease, 5(2), 69. https://doi.org/10.3390/tropicalmed5020069