Meningococcal Vaccine for Hajj Pilgrims: Compliance, Predictors, and Barriers

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. Survey Design
2.3. Statistical Methods
3. Results
3.1. Participant Characteristics
3.2. Meningococcal Vaccine Uptake
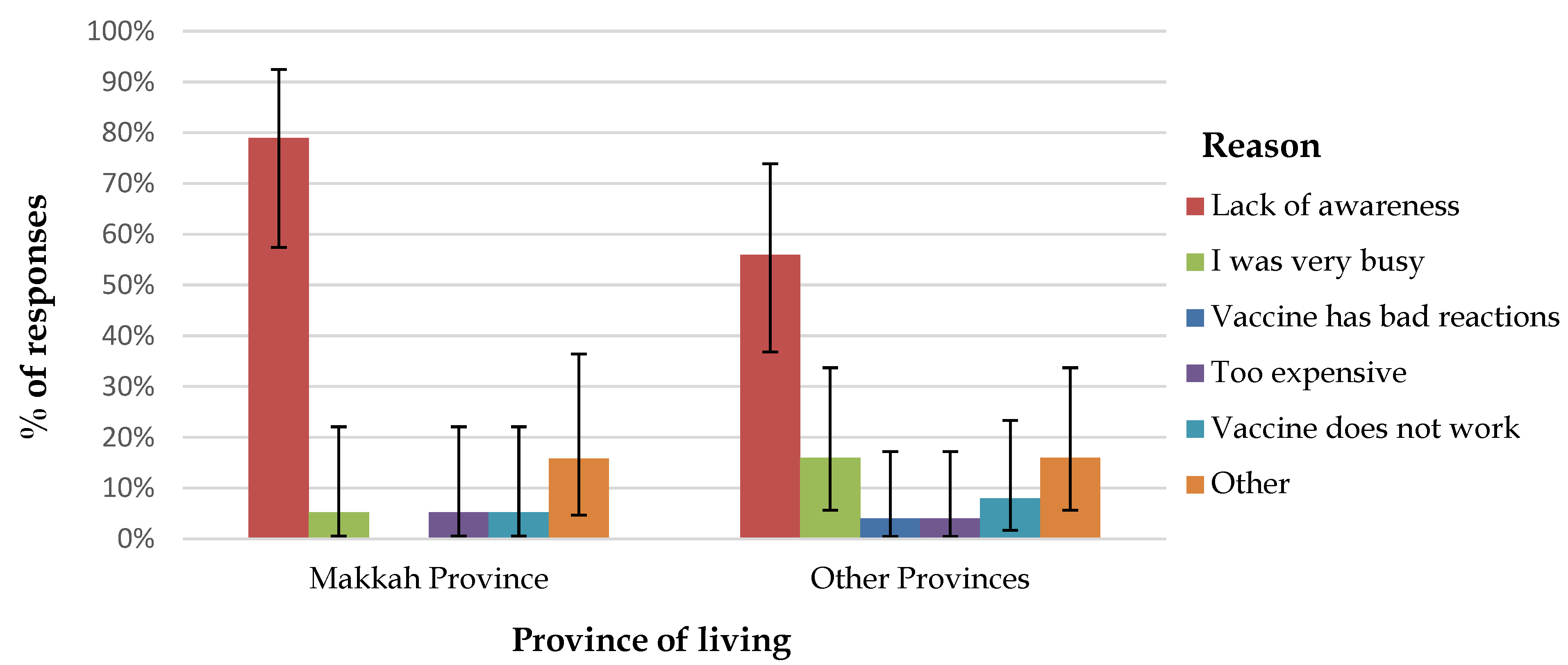
3.3. Participant Adherence to Vaccination Policy
3.4. Vaccination Venues
3.5. Cost of Vaccination
3.6. Receipt of Pre-Hajj Advice
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Al-Tawfiq, J.A.; Gautret, P.; Memish, Z.A. Expected immunizations and health protection for Hajj and Umrah 2018—An overview. Travel Med. Infect. Dis. 2017, 19, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Memish, Z.A.; Zumla, A.; Alhakeem, R.F.; Assiri, A.; Turkestani, A.; Al Harby, K.D.; Alyemni, M.; Dhafar, K.; Gautret, P.; Barbeschi, M.; et al. Hajj: Infectious disease surveillance and control. Lancet 2014, 383, 2073–2082. [Google Scholar] [CrossRef]
- Yezli, S.; Wilder-Smith, A.; Bin Saeed, A.A. Carriage of Neisseria meningitidis in the Hajj and Umrah mass gatherings. Int. J. Infect. Dis. 2016, 47, 65–70. [Google Scholar] [CrossRef]
- Wilder-Smith, A. Meningococcal vaccine in travelers. Curr. Opin. Infect. Dis. 2007, 20, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Moore, P.S.; Reeves, M.W.; Schwartz, B.; Gellin, B.G.; Broome, C.V. Intercontinental spread of an epidemic group A Neisseria meningitidis strain. Lancet 1989, 2, 260–263. [Google Scholar] [CrossRef]
- Yezli, S.; Assiri, A.M.; Alhakeem, R.F.; Turkistani, A.M.; Alotaibi, B. Meningococcal disease during the Hajj and Umrah mass gatherings. Int. J. Infect. Dis. 2016, 47, 60–64. [Google Scholar] [CrossRef] [Green Version]
- Badahdah, A.M.; Rashid, H.; Khatami, A.; Booy, R. Meningococcal disease burden and transmission in crowded settings and mass gatherings other than Hajj/Umrah: A systematic review. Vaccine 2018, 36, 4593–4602. [Google Scholar] [CrossRef]
- Memish, Z.; Al Hakeem, R.; Al Neel, O.; Danis, K.; Jasir, A.; Eibach, D. Laboratory-confirmed invasive meningococcal disease: Effect of the Hajj vaccination policy, Saudi Arabia, 1995 to 2011. Eurosurveillance 2013, 18, 20581. [Google Scholar] [CrossRef]
- World Health Organization. Health conditions for travellers to Saudi Arabia for the pilgrimage to Mecca (Hajj). Wkly. Epidemiol. Rec. 2016, 91, 331–335. [Google Scholar]
- Memish, Z.A.; Yezli, S.; Almasri, M.; Assiri, A.; Turkestani, A.; Findlow, H.; Bai, X.; Borrow, R. Meningococcal serogroup A, C, W, and Y serum bactericidal antibody profiles in Hajj pilgrims. Int. J. Infect. Dis. 2014, 28, 171–175. [Google Scholar] [CrossRef] [Green Version]
- Memish, Z.A.; Assiri, A.; Almasri, M.; Alhakeem, R.F.; Turkestani, A.; Al Rabeeah, A.A.; Al-Tawfiq, J.A.; Alzahrani, A.; Azhar, E.; Makhdoom, H.Q.; et al. Prevalence of MERS-CoV nasal carriage and compliance with the Saudi health recommendations among pilgrims attending the 2013 Hajj. J. Infect. Dis. 2014, 210, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- El Bashir, H.; Rashid, H.; Memish, Z.A.; Shafi, S. Umra Research, G. Meningococcal vaccine coverage in Hajj pilgrims. Lancet 2007, 369, 1343. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Memish, Z.A. Mass gatherings and infectious diseases: Prevention, detection, and control. Infect. Dis. Clin. N. Am. 2012, 26, 725–737. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, A.S.; Wiley, K.E.; Tashani, M.; Willaby, H.W.; Heywood, A.E.; BinDhim, N.F.; Booy, R.; Rashid, H. Exploring barriers to and facilitators of preventive measures against infectious diseases among Australian Hajj pilgrims: Cross-sectional studies before and after Hajj. Int. J. Infect. Dis. 2016, 47, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Bateman, C. Haj threat creates huge fraud potential. S Afr. Med. J. 2002, 92, 178–179. [Google Scholar] [PubMed]
- Rahman, J.; Thu, M.; Arshad, N.; Van der Putten, M. Mass Gatherings and Public Health: Case Studies from the Hajj to Mecca. Ann. Glob. Health 2017, 83, 386–393. [Google Scholar] [CrossRef] [Green Version]
- Madani, T.A.; Ghabrah, T.M. Meningococcal, influenza virus, and hepatitis B virus vaccination coverage level among health care workers in Hajj. BMC Infect. Dis. 2007, 7, 80. [Google Scholar] [CrossRef]
- Memish, Z.A.; Assiri, A.M.; Alshehri, M.; Hussain, R.; Alomar, I. The prevalance of respiratory viruses among healthcare workers serving pilgrims in Makkah during the 2009 influenza A (H1N1) pandemic. Travel Med. Infect. Dis. 2012, 10, 18–24. [Google Scholar] [CrossRef]
- AlQuliti, K.W.; Tajaddin, W.A.; Habeeb, H.A.; As-Saedi, E.S.; Sheerah, S.A.; Al-Ayoubi, R.M.; Bukhary, Z.A. Meningococcal immunization among emergency room health care workers in Almadinah Almunawwarah, Saudi Arabia. J. Taibah Univ. Med. Sci. 2015, 10, 175–180. [Google Scholar] [CrossRef] [Green Version]
- Badahdah, A.M.; Alfelali, M.; Alqahtani, A.S.; Alsharif, S.; Barasheed, O.; Rashid, H. Mandatory meningococcal vaccine, and other recommended immunisations: Uptake, barriers, and facilitators among health care workers and trainees at Hajj. World J. Clin. Cases 2018, 6, 1128–1135. [Google Scholar] [CrossRef]
- Saudi Arabian General Authority for Statistics. Hajj Census. Available online: https://www.stats.gov.sa/en/28 (accessed on 25 August 2019).
- Alfelali, M.; Barasheed, O.; Badahdah, A.M.; Bokhary, H.; Azeem, M.I.; Habeebullah, T.; Bakarman, M.; Asghar, A.; Booy, R.; Rashid, H. Influenza vaccination among Saudi Hajj pilgrims: Revealing the uptake and vaccination barriers. Vaccine 2018, 36, 2112–2118. [Google Scholar] [CrossRef] [PubMed]
- Barasheed, O.; Rashid, H.; Heron, L.; Ridda, I.; Haworth, E.; Nguyen-Van-Tam, J.; Dwyer, D.E.; Booy, R. Influenza vaccination among Australian Hajj pilgrims: Uptake, attitudes, and barriers. J. Travel Med. 2014, 21, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, A.S.; Bondagji, D.M.; Alshehari, A.A.; Basyouni, M.H.; Alhawassi, T.M.; BinDhim, N.F.; Rashid, H. Vaccinations against respiratory infections in Arabian Gulf countries: Barriers and motivators. World J. Clin. Cases 2017, 5, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Al-Otaibi, B.M.; El-Saed, A.; Balkhy, H.H. Influenza vaccination among healthcare workers at a tertiary care hospital in Saudi Arabia: Facing challenges. Ann. Thorac. Med. 2010, 5, 120–121. [Google Scholar] [PubMed]
- Keles, H.; Sonder, G.J.; van den Hoek, A. Predictors for the uptake of recommended vaccinations in Mecca travelers who visited the Public Health Service Amsterdam for mandatory meningitis vaccination. J. Travel Med. 2011, 18, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Schlagenhauf, P.; Chen, L.H.; Wilson, M.E.; Freedman, D.O.; Tcheng, D.; Schwartz, E.; Pandey, P.; Weber, R.; Nadal, D.; Berger, C.; et al. Sex and gender differences in travel-associated disease. Clin. Infect. Dis. 2010, 50, 826–832. [Google Scholar] [CrossRef]
- Memish, Z.A.; Assiri, A.M.; Hussain, R.; Alomar, I.; Stephens, G. Detection of respiratory viruses among pilgrims in Saudi Arabia during the time of a declared influenza A(H1N1) pandemic. J. Travel Med. 2012, 19, 15–21. [Google Scholar] [CrossRef]
- Maiden, M.C.; Ibarz-Pavon, A.B.; Urwin, R.; Gray, S.J.; Andrews, N.J.; Clarke, S.C.; Walker, A.M.; Evans, M.R.; Kroll, J.S.; Neal, K.R.; et al. Impact of meningococcal serogroup C conjugate vaccines on carriage and herd immunity. J. Infect. Dis. 2008, 197, 737–743. [Google Scholar] [CrossRef]
- Read, R.C.; Baxter, D.; Chadwick, D.R.; Faust, S.N.; Finn, A.; Gordon, S.B.; Heath, P.T.; Lewis, D.J.M.; Pollard, A.J.; Turner, D.P.J.; et al. Effect of a quadrivalent meningococcal ACWY glycoconjugate or a serogroup B meningococcal vaccine on meningococcal carriage: An observer-blind, phase 3 randomised clinical trial. Lancet 2014, 384, 2123–2131. [Google Scholar] [CrossRef]
- Yezli, S. The threat of meningococcal disease during the Hajj and Umrah mass gatherings: A comprehensive review. Travel Med. Infect. Dis. 2018, 24, 51–58. [Google Scholar] [CrossRef]
- Peterson, M.E.; Mile, R.; Li, Y.; Nair, H.; Kyaw, M.H. Meningococcal carriage in high-risk settings: A systematic review. Int. J. Infect. Dis. 2018, 73, 109–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alborzi, A.; Oskoee, S.; Pourabbas, B.; Alborzi, S.; Astaneh, B.; Gooya, M.M.; Kaviani, M.J. Meningococcal carrier rate before and after hajj pilgrimage: Effect of single dose ciprofloxacin on carriage. East. Mediterr. Health J. 2008, 14, 277–282. [Google Scholar] [PubMed]
- Dellicour, S.; Greenwood, B. Systematic review: Impact of meningococcal vaccination on pharyngeal carriage of meningococci. Trop. Med. Int. Health 2007, 12, 1409–1421. [Google Scholar] [CrossRef] [PubMed]
- Borrow, R.; Alarcon, P.; Carlos, J.; Caugant, D.A.; Christensen, H.; Debbag, R.; de Wals, P.; Echániz-Aviles, G.; Findlow, J.; Head, C.; et al. The Global Meningococcal Initiative: Global epidemiology, the impact of vaccines on meningococcal disease and the importance of herd protection. Expert Rev. Vaccines 2017, 16, 313–328. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Measure | When | Age Criteria | Target Group |
|---|---|---|---|
| MenACWY polysaccharide vaccine | Within last 3 years, but ≥ 10 days before arrival | Any individual > 2 years | a. Visitors to Saudi Arabia for Umra *, Hajj, or seasonal work ** b. Residents of Saudi Arabia as follows: - Residents of Makkah and Madina at the time of Hajj - Residents of all other provinces undertaking the Hajj ** - Hajj workers *** |
| MenACWY conjugate vaccine | Within last 5 years, but ≥ 10 days before arrival | ||
| Chemoprophylaxis (ciprofloxacin, 1 tablet, 500 mg) | Upon arrival (at port of entry) | Any individual > 2 years (excluding pregnant women) | Visitors from African meningitis belt countries for Umra *, Hajj, or seasonal work ** |
| Characteristics | All n/N * (%) | Domestic Pilgrims n/N * (%) | Overseas Pilgrims n/N * (%) | p-Value |
|---|---|---|---|---|
| Number of participants | 509** | 416/489 (85.1) | 73/489 (14.9) | |
| Age in years | ||||
| Mean (SD) | 36 (± 12.6) | 34.7 (± 12) | 42 (± 13.4) | < 0.001 *** |
| Range (Median) | 13–82 (33.8) | 13–82 (32.6) | 21–69 (38.9) | |
| Gender | ||||
| Male:female | 6:1 | 7.5:1 | 3:1 | 0.03 *** |
| Country of residence | ||||
| Saudi Arabia | 398/499 (79.8) | 398/412 (96.6) | 0 | |
| Pakistan | 33/499 (6.6) | 0 | 30/73 (41.1) | |
| South Africa | 28/499 (5.6) | 0 | 28/73 (38.4) | |
| Egypt | 11/499 (2.2) | 7/412 (1.7) ¶ | 0 | |
| Malawi | 6/499 (1.2) | 0 | 6/73 (8.2) | |
| Zambia | 5/499 (1) | 0 | 5/73 (6.8) | |
| Other | 18/499 (3.6) | 7/412 (1.7) ¶ | 4/73 (5.5) | |
| Highest qualification | ||||
| No formal education | 4/499 (0.8) | 2/411 (0.5) | 1/70 (1.4) | |
| School certificate ǂ | 43/499 (8.6) | 34/411 (8.2) | 4/70 (5.7) | |
| High school certificate § | 124/499 (24.8) | 100/411 (24.3) | 21/70 (30) | |
| Diploma | 58/499 (11.6) | 39/411 (9.5) | 12/70 (17.1) | |
| University undergraduate degree | 215/499 (43.1) | 184/411 (44.8) | 30/70 (42.9) | |
| University postgraduate degree | 55/499 (11) | 52/411 (12.7) | 2/70 (2.9) | |
| Employed | ||||
| No | 168/501 (33.5) | 134/412 (32.5) | 25/69 (36.2) | 0.61 |
| Yes | 333/501 (66.5) | 278/412 (67.5) | 44/69 (63.8) | |
| Hajj attendance | ||||
| First time | 285/500 (57) | 212/409 (51.8) | 60/71 (84.5) | < 0.001 *** |
| > 1 time previously | 215/500 (43) | 197/409 (48.2) | 11/71 (15.5) | |
| Characteristics | Overall Meningococcal Vaccine Uptake | Meningococcal Vaccine Uptake among Domestic Pilgrims | ||||
|---|---|---|---|---|---|---|
| n/N * (%) | OR ** (95% CI) | p | n/N * (%) | OR ** (95% CI) | p | |
| All | ||||||
| All participants ¶ | 389/476 (81.7) | 321/397 (80.9) | ||||
| Gender | ||||||
| Male | 322/380 (84.7) | 1.0 (ref) | 270/326 (82.8) | 1.0 (ref) | ||
| Female | 53/58 (91.4) | 1.9 (0.7–4.98) | 0.18 | 39/43 (90.7) | 2 (0.7–5.9) | 0.19 |
| Origin | ||||||
| Domestic | 321/382 (84) | 1.0 (ref) | ||||
| Overseas | 58/58 (100) | n.a | <0.001 § | |||
| Province of residence | ||||||
| Makkah Province | 59/80 (73.8) | 1.0 (ref) | ||||
| Other | 207/235 (88.1) | 2.6 (1.4–5) | < 0.01 § | |||
| Hajj attendance | ||||||
| First time | 208/246 (84.6) | 1.0 (ref) | 158/193 (81.9) | 1.0 (ref) | ||
| ≥ 1 time previously | 174/199 (87.4) | 1.3 (0.7–2.2) | 0.39 | 158/183 (86.3) | 1.4 (0.8–2.4) | 0.24 |
| Tertiary qualification | ||||||
| No | 122/150 (81.3) | 1.0 (ref) | 99/125 (79.2) | 1.0 (ref) | ||
| Yes | 262/297 (88.2) | 1.7 (1.0–2.5) | 0.048 § | 220/254 (86.6) | 1.7 (0.97–2.98) | 0.06 |
| Employed | ||||||
| No | 113/144 (78.5) | 1.0 (ref) | 92/121 (76) | 1.0 (ref) | ||
| Yes | 269/302 (89.1) | 2.2 (1.3–3.8) | 0.03§ | 226/258 (87.6) | 2.2 (1.3–3.9) | < 0.01 § |
| Received pre-Hajj health advice | ||||||
| No | 64/89 (71.9) | 1.0 (ref) | 54/78 (69.2) | 1.0 (ref) | ||
| Yes | 322/360 (89.4) | 3.3 (1.9–5.9) | < 0.001 § | 264/300 (88) | 3.3 (1.8–5.9) | < 0.001 § |
| Characteristics | Proportion of Participants Who Paid for the Vaccine | |||
|---|---|---|---|---|
| n/N * (%) | OR (95% CI) | p | ||
| All | ||||
| All participants ¶ | 55/364 (15.1) | |||
| Gender | ||||
| Male | 38/302 (12.6) | 1.0 (ref) | ||
| Female | 16/49 (32.7) | 3.4 (1.7–6.7) | < 0.001 § | |
| Origin | ||||
| Domestic | 30/307 (9.8) | 1.0 (ref) | ||
| Overseas | 23/48 (47.9) | 8.5 (4.3–16.7) | < 0.001 § | |
| Pakistan | 17/17 (100) | |||
| South Africa | 3/20 (15) | |||
| Other | 9/27 (33.3) | |||
| Hajj attendance | ||||
| ≥ 1 time previously | 13/165 (7.9) | 1.0 (ref) | ||
| First time | 41/193 (21.2) | 3.2 (1.6–6.1) | < 0.001 § | |
| Tertiary qualification | ||||
| Yes | 31/246 (12.6) | 1.0 (ref) | ||
| No | 22/112 (19.6) | 1.7 (0.9–3.1) | 0.09 | |
| Employed | ||||
| Yes | 32/246 (13) | 1.0 (ref) | ||
| No | 21/108 (19.4) | 1.6 (0.9–3) | 0.12 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badahdah, A.-M.; Alghabban, F.; Falemban, W.; Albishri, A.; Rani Banik, G.; Alhawassi, T.; Abuelizz, H.; Bakarman, M.A.; Khatami, A.; Booy, R.; et al. Meningococcal Vaccine for Hajj Pilgrims: Compliance, Predictors, and Barriers. Trop. Med. Infect. Dis. 2019, 4, 127. https://doi.org/10.3390/tropicalmed4040127
Badahdah A-M, Alghabban F, Falemban W, Albishri A, Rani Banik G, Alhawassi T, Abuelizz H, Bakarman MA, Khatami A, Booy R, et al. Meningococcal Vaccine for Hajj Pilgrims: Compliance, Predictors, and Barriers. Tropical Medicine and Infectious Disease. 2019; 4(4):127. https://doi.org/10.3390/tropicalmed4040127
Chicago/Turabian StyleBadahdah, Al-Mamoon, Fatimah Alghabban, Wajd Falemban, Abdullah Albishri, Gouri Rani Banik, Tariq Alhawassi, Hatem Abuelizz, Marwan A. Bakarman, Ameneh Khatami, Robert Booy, and et al. 2019. "Meningococcal Vaccine for Hajj Pilgrims: Compliance, Predictors, and Barriers" Tropical Medicine and Infectious Disease 4, no. 4: 127. https://doi.org/10.3390/tropicalmed4040127