The As and Bs of HIV and Hepatitis Co-Infection


Abstract
1. Introduction
2. HAV and HIV Co-Infection
2.1. Epidemiology of HAV and HIV Co-Infection
2.2. Clinical Manifestations of HAV Co-Infection among People with HIV
2.3. HAV Vaccination among People with HIV Infection
3. HBV and HIV Co-Infection
3.1. Epidemiology of HBV and HIV Co-Infection
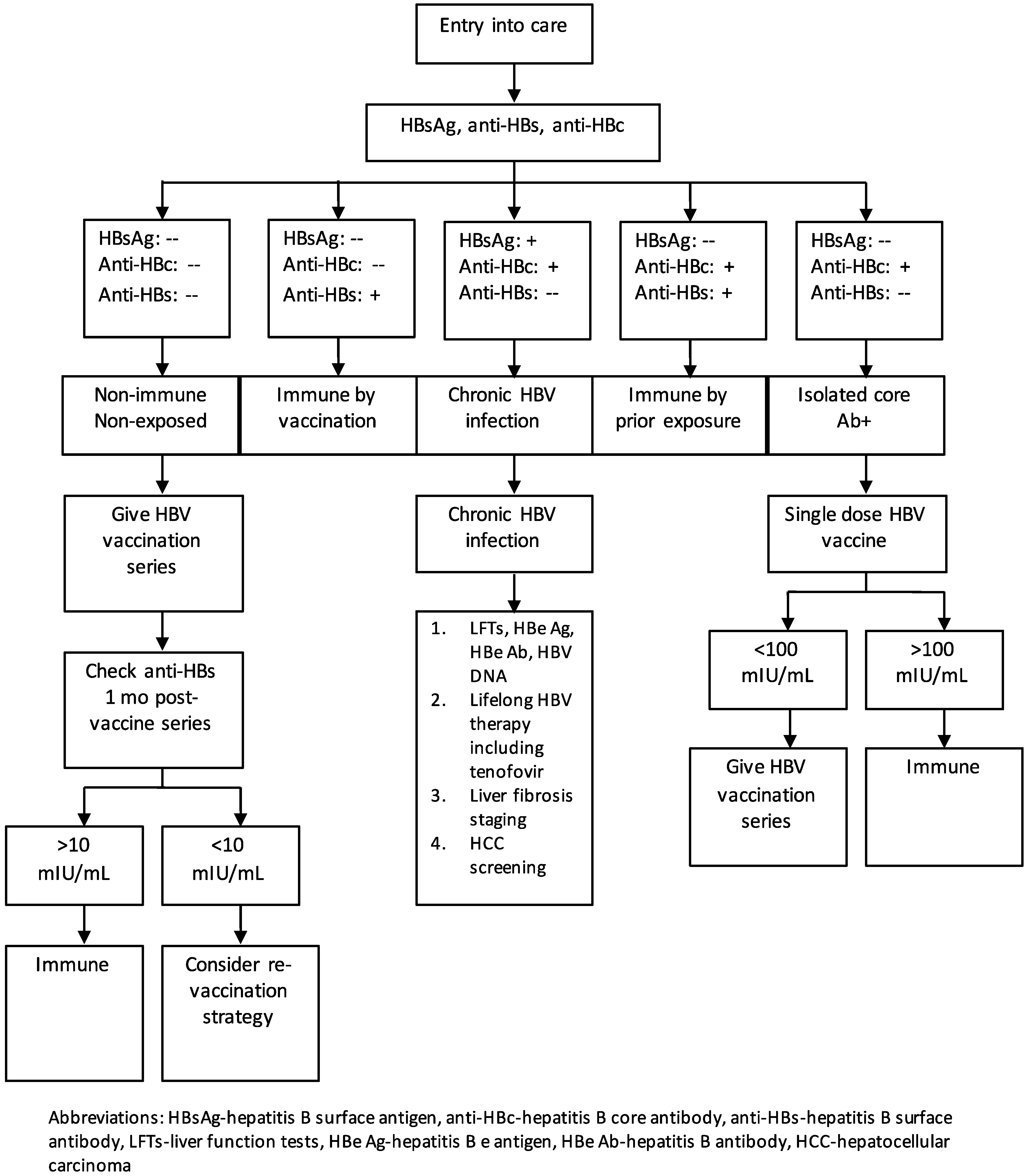
3.2. Staging Patients with HBV/HIV Co-Infection
3.3. Treatment of HBV/HIV Co-Infection
3.4. HBV Vaccination among People with HIV Infection
3.5. New HBV Treatment and Cure Strategies
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lin, K.Y.; Chen, G.J.; Lee, Y.L.; Huang, Y.C.; Cheng, A.; Sun, H.Y.; Chang, S.Y.; Liu, C.E.; Hung, C.C. Hepatitis A virus infection and hepatitis A vaccination in human immunodeficiency virus-positive patients: A review. World J. Gastroenterol. 2017, 23, 3589–3606. [Google Scholar] [CrossRef]
- Spada, E.; Genovese, D.; Tosti, M.E.; Mariano, A.; Cuccuini, M.; Proietti, L.; Giuli, C.D.; Lavagna, A.; Crapa, G.E.; Morace, G.; et al. An outbreak of hepatitis A virus infection with a high case-fatality rate among injecting drug users. J. Hepatol. 2005, 43, 958–964. [Google Scholar] [CrossRef]
- Foster, M.; Ramachandran, S.; Myatt, K.; Donovan, D.; Bohm, S.; Fiedler, J.; Barbeau, B.; Collins, J.; Thoroughman, D.; McDonald, E.; et al. Hepatitis A Virus Outbreaks Associated with Drug Use and Homelessness—California, Kentucky, Michigan, and Utah, 2017. Morb. Mortal. Wkly. Rep. 2018, 67, 1208–1210. [Google Scholar] [CrossRef]
- Lin, K.Y.; Hsieh, S.M.; Sun, H.Y.; Lo, Y.C.; Sheng, W.H.; Chuang, Y.C.; Cheng, A.; Pan, S.C.; Chen, G.J.; Hung, C.C.; et al. Serologic responses and effectiveness of hepatitis A vaccination among human immunodeficiency virus-positive individuals during the outbreak of acute hepatitis A. Hepatology 2018, 68, 22–31. [Google Scholar] [CrossRef]
- Kourkounti, S.; Papaizos, V.; Leuow, K.; Kordosis, T.; Antoniou, C. Hepatitis A vaccination and immunological parameters in HIV-infected patients. Viral. Immunol. 2013, 26, 357–363. [Google Scholar] [CrossRef]
- Centers for Disease Control Hepatitis A Questions and Answers for Health Professionals. Available online: https://www.cdc.gov/hepatitis/hav/havfaq.htm (accessed on 15 February 2019).
- Rossati, A.; Bargiacchi, O.; Kroumova, V.; Nebbiolo, C.; Tacca, M.G.; Pratillo, S.; Garavelli, P.L. Outbreak of severe Hepatitis A in Eastern Piedmont, Italy. Infez Med. 2017, 25, 344–346. [Google Scholar]
- Charre, C.; Ramière, C.; Roque-Afonso, A.M.; Chidiac, C.; Zoulim, F.; Godinot, M.; Koffi, J.; Scholtès, C.; Livrozet, J.M.; HAV Lyon Study Group; et al. Hepatitis A outbreak in HIV-infected MSM and in PrEP-using MSM despite a high level of immunity, Lyon, France, January to June 2017. Eurosurveillance 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- Lanini, S.; Minosse, C.; Vairo, F.; Garbuglia, A.; Di Bari, V.; Agresta, A.; Rezza, G.; Puro, V.; Pendenza, A.; Loffredo, M.R.; et al. A large ongoing outbreak of hepatitis A predominantly affecting young males in Lazio, Italy; August 2016—March 2017. PLoS ONE 2017, 12, e0185428. [Google Scholar] [CrossRef] [PubMed]
- Gozlan, Y.; Bar-Or, I.; Rakovsky, A.; Savion, M.; Amitai, Z.; Sheffer, R.; Ceder, N.; Anis, E.; Grotto, I.; Mendelson, E.; et al. Ongoing hepatitis A among men who have sex with men (MSM) linked to outbreaks in Europe in Tel Aviv area, Israel, December 2016–June 2017. Euro Surveill 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- Comelli, A.; Izzo, I.; Casari, S.; Spinetti, A.; Bergamasco, A.; Castelli, F. Hepatitis A outbreak in men who have sex with men (MSM) in Brescia (Northern Italy), July 2016–July 2017. Infez Med. 2018, 26, 46–51. [Google Scholar] [PubMed]
- Rivas, V.; Barrera, A.; Pino, K.; Núñez, R.; Caceres, C.J.; Lopez-Lastra, M.; Soza, A. Hepatitis A outbreak since November 2016 affecting men who have sex with men (MSM) in Chile connected to the current outbreak in MSM in Europe, situation up to October 2017. Eurosurveillance 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Tajes, S.; Perpiñán, E.; Caballol, B.; Lens, S.; Mariño, Z.; Costa, J.; Vilella, A.; Pérez-Del-Pulgar, S.; Forns, X.; Koutsoudakis, G. Hepatitis A outbreak in Barcelona among men who have sex with men (MSM), January–June 2017: A hospital perspective. Liver Int. 2018, 38, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Lemon, S.M. Type A viral hepatitis. New developments in an old disease. N. Engl. J. Med. 1985, 313, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Koff, R.S. Clinical manifestations and diagnosis of hepatitis A virus infection. Vaccine 1992, 10 (Suppl. 1), S15–S17. [Google Scholar] [CrossRef]
- Ajmera, V.; Xia, G.; Vaughan, G.; Forbi, J.C.; Ganova-Raeva, L.M.; Khudyakov, Y.; Opio, C.K.; Taylor, R.; Restrepo, R.; Munoz, S.; et al. What factors determine the severity of hepatitis A-related acute liver failure? J. Viral. Hepat. 2011, 18, e167–e174. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.M.; Park, S.J.; Kim, J.S.; Jang, J.H.; Lee, S.H.; Kim, J.W.; Park, Y.M.; Hwang, S.G.; Rim, K.S.; Kang, S.K.; et al. Atypical manifestations of hepatitis A infection: A prospective, multicenter study in Korea. J. Med. Virol. 2010, 82, 1318–1326. [Google Scholar] [CrossRef] [PubMed]
- Ida, S.; Tachikawa, N.; Nakajima, A.; Daikoku, M.; Yano, M.; Kikuchi, Y.; Yasuoka, A.; Kimura, S.; Oka, S. Influence of human immunodeficiency virus type 1 infection on acute hepatitis A virus infection. Clin. Infect. Dis. 2002, 34, 379–385. [Google Scholar] [CrossRef]
- Lee, Y.L.; Chen, G.J.; Chen, N.Y.; Liou, B.H.; Wang, N.C.; Lee, Y.T.; Yang, C.J.; Huang, Y.S.; Tang, H.J.; Huang, S.S.; et al. Less Severe but Prolonged Course of Acute Hepatitis A in Human Immunodeficiency Virus (HIV)-Infected Patients Compared with HIV-Uninfected Patients During an Outbreak: A Multicenter Observational Study. Clin. Infect. Dis. 2018, 67, 1595–1602. [Google Scholar] [CrossRef]
- Kim, D.K.; Riley, L.E.; Harriman, K.H.; Hunter, P.; Bridges, C.B. Advisory Committee on Immunization Practices Recommended Immunization Schedule for Adults Aged 19 Years or Older—United States, 2017. Morb. Mortal. Wkly. Rep. 2017, 66, 136–138. [Google Scholar] [CrossRef] [PubMed]
- British HIV Association Guidelines. Available online: https://www.bhiva.org/guidelines (accessed on 15 February 2019).
- European AIDS Clinical Society Guidelines. Available online: http://www.eacsociety.org/guidelines/eacs-guidelines/eacs-guidelines.html (accessed on 15 February 2019).
- Nelson, N.P.; Link-Gelles, R.; Hofmeister, M.G.; Romero, J.R.; Moore, K.L.; Ward, J.W.; Schillie, S.F. Update: Recommendations of the Advisory Committee on Immunization Practices for Use of Hepatitis A Vaccine for Postexposure Prophylaxis and for Preexposure Prophylaxis for International Travel. Morb. Mortal. Wkly. Rep. 2018, 67, 1216–1220. [Google Scholar] [CrossRef]
- Department of Health and Human Services (DHHS) Guidelines. Available online: https://aidsinfo.nih.gov/guidelines/html/1/adult-and-adolescent-arv/0 (accessed on 15 February 2019).
- WHO Guidelines. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-a (accessed on 15 February 2019).
- Sun, H.Y.; Sheng, W.H.; Tsai, M.S.; Lee, K.Y.; Chang, S.Y.; Hung, C.C. Hepatitis B virus coinfection in human immunodeficiency virus-infected patients: A review. World J. Gastroenterol. 2014, 20, 14598–14614. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.P.; Crane, M.; Audsley, J.; Avihingsanon, A.; Sasadeusz, J.; Lewin, S.R. HIV-hepatitis B virus coinfection: Epidemiology, pathogenesis, and treatment. AIDS 2017, 31, 2035–2052. [Google Scholar] [CrossRef] [PubMed]
- Phung, B.C.; Sogni, P.; Launay, O. Hepatitis B and human immunodeficiency virus co-infection. World J. Gastroenterol. 2014, 20, 17360–17367. [Google Scholar] [CrossRef]
- Zhou, K.; Terrault, N. Management of hepatitis B in special populations. Best Pr. Res. Clin. Gastroenterol. 2017, 31, 311–320. [Google Scholar] [CrossRef]
- Soriano, V.; Labarga, P.; de Mendoza, C.; Peña, J.M.; Fernández-Montero, J.V.; Benítez, L.; Esposito, I.; Barreiro, P. Emerging challenges in managing hepatitis B in HIV patients. Curr. HIV/Aids Rep. 2015, 12, 344–352. [Google Scholar] [CrossRef]
- Hyer, R.; McGuire, D.K.; Xing, B.; Jackson, S.; Janssen, R. Safety of a two-dose investigational hepatitis B vaccine, HBsAg-1018, using a toll-like receptor 9 agonist adjuvant in adults. Vaccine 2018, 36, 2604–2611. [Google Scholar] [CrossRef]
- Jackson, S.; Lentino, J.; Kopp, J.; Murray, L.; Ellison, W.; Rhee, M.; Shockey, G.; Akella, L.; Erby, K.; Heyward, W.L.; et al. Immunogenicity of a two-dose investigational hepatitis B vaccine, HBsAg-1018, using a toll-like receptor 9 agonist adjuvant compared with a licensed hepatitis B vaccine in adults. Vaccine 2018, 36, 668–674. [Google Scholar] [CrossRef]
- Mena, G.; García-Basteiro, A.L.; Bayas, J.M. Hepatitis B and A vaccination in HIV-infected adults: A review. Hum. Vaccin Immunother. 2015, 11, 2582–2598. [Google Scholar] [CrossRef]
- Launay, O.; van der Vliet, D.; Rosenberg, A.R.; Michel, M.L.; Piroth, L.; Rey, D.; Colin de Verdière, N.; Slama, L.; Martin, K.; Lortholary, O.; et al. Safety and immunogenicity of 4 intramuscular double doses and 4 intradermal low doses vs standard hepatitis B vaccine regimen in adults with HIV-1: A randomized controlled trial. JAMA 2011, 305, 1432–1440. [Google Scholar] [CrossRef] [PubMed]
- Chaiklang, K.; Wipasa, J.; Chaiwarith, R.; Praparattanapan, J.; Supparatpinyo, K. Comparison of immunogenicity and safety of four doses and four double doses vs. standard doses of hepatitis B vaccination in HIV-infected adults: A randomized, controlled trial. PLoS ONE 2013, 8, e80409. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Prada, M.; Rodríguez-Fonseca, O.D.; Brandy-García, A.M.; Alonso-Penanes, P.; Huerta-González, I.; Fernández-Noval, F. Use of hepatitis B AS04C adjuvanted vaccine in HIV patients. Rev. Esp. Quim. 2018, 31, 105–109. [Google Scholar]
- Heyward, W.L.; Kyle, M.; Blumenau, J.; Davis, M.; Reisinger, K.; Kabongo, M.L.; Bennett, S.; Janssen, R.S.; Namini, H.; Martin, J.T. Immunogenicity and safety of an investigational hepatitis B vaccine with a Toll-like receptor 9 agonist adjuvant (HBsAg-1018) compared to a licensed hepatitis B vaccine in healthy adults 40–70 years of age. Vaccine 2013, 31, 5300–5305. [Google Scholar] [CrossRef] [PubMed]
- Janssen, R.S.; Mangoo-Karim, R.; Pergola, P.E.; Girndt, M.; Namini, H.; Rahman, S.; Bennett, S.R.; Heyward, W.L.; Martin, J.T. Immunogenicity and safety of an investigational hepatitis B vaccine with a toll-like receptor 9 agonist adjuvant (HBsAg-1018) compared with a licensed hepatitis B vaccine in patients with chronic kidney disease. Vaccine 2013, 31, 5306–5313. [Google Scholar] [CrossRef]
- Arends, J.E.; Lieveld, F.I.; Ahmad, S.; Ustianowski, A. New Viral and Immunological Targets for Hepatitis B Treatment and Cure: A Review. Infect. Dis. 2017, 6, 461–476. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Brand | Dose(s) | Schedule |
|---|---|---|
| Recombivax HB | 10 mcg rHBsAg, 40 mcg rHBsAg | 0, 1, and 6 months |
| Energix-B | 20 mcg rHBsAg | 0, 1, and 6 months |
| Twinrix | 20 mcg rHBsAg + inactivated HAV vaccine | 0, 1, and 6 months |
| Heplisav-B | 20 mcg rHBsAg + TLR9 agonist | 0 and 1 month |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wooten, D.; Karris, M.Y. The As and Bs of HIV and Hepatitis Co-Infection. Trop. Med. Infect. Dis. 2019, 4, 55. https://doi.org/10.3390/tropicalmed4020055
Wooten D, Karris MY. The As and Bs of HIV and Hepatitis Co-Infection. Tropical Medicine and Infectious Disease. 2019; 4(2):55. https://doi.org/10.3390/tropicalmed4020055
Chicago/Turabian StyleWooten, Darcy, and Maile Y. Karris. 2019. "The As and Bs of HIV and Hepatitis Co-Infection" Tropical Medicine and Infectious Disease 4, no. 2: 55. https://doi.org/10.3390/tropicalmed4020055
APA StyleWooten, D., & Karris, M. Y. (2019). The As and Bs of HIV and Hepatitis Co-Infection. Tropical Medicine and Infectious Disease, 4(2), 55. https://doi.org/10.3390/tropicalmed4020055