Hemophagocytic Lymphohistiocytosis Associated with Scrub Typhus: Systematic Review and Comparison between Pediatric and Adult Cases

Abstract
:1. Introduction
2. Methods
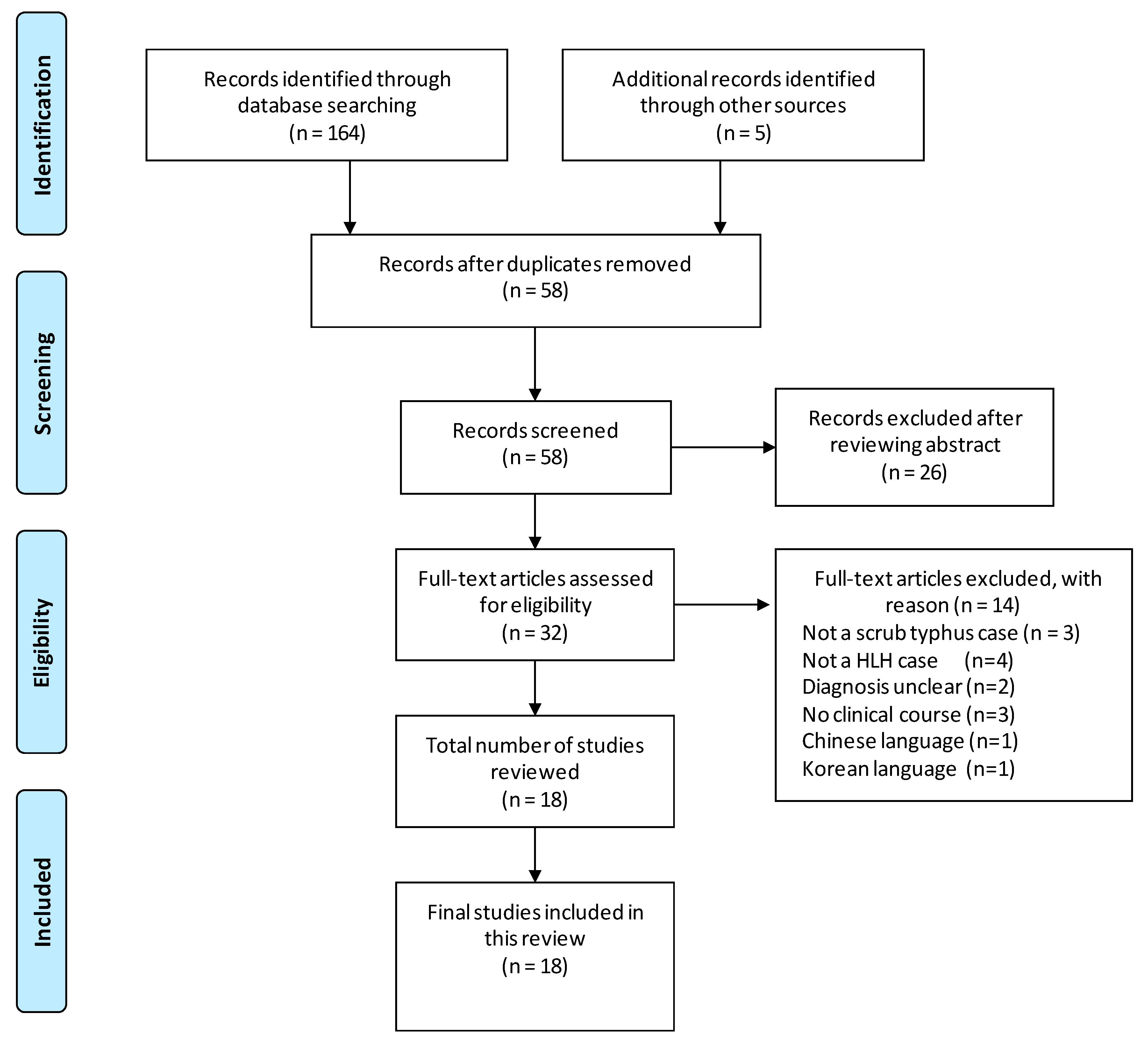
2.1. Search Strategy and Study Selection
2.2. Data Extraction
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Diagnosis of Scrub Typhus and HLH
3.2. Clinical Findings of HLH Associated with Scrub Typhus
3.3. Laboratory Findings of HLH Associated with Scrub Typhus
3.4. Treatment of HLH Associated with Scrub Typhus
4. Discussion
5. Conclusions
Conflicts of Interest
References
- Jeong, Y.J.; Kim, S.; Wook, Y.D.; Lee, J.W.; Kim, K.I.; Lee, S.H. Scrub typhus: Clinical, pathologic, and imaging findings. Radiographics 2007, 27, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Saah, A.J. Orientia tsutsugamushi (scrub typhus). In Principles and Practice of Infectious Disease, 5th ed.; Mandell, G.L., Bennett, J.E., Dolin, R., Eds.; Churchill Livingstone: Philadelphia, PA, USA; Tokyo, Japan, 2000; pp. 2056–2057. ISBN 044307593X. [Google Scholar]
- Allen, A.C.; Spitz, S. A comparative study of the pathology of scrub typhus (tsutsugamushi disease) and other rickettsial diseases. Am. J. Pathol. 1945, 21, 603–681. [Google Scholar] [PubMed]
- Kim, S.J.; Chung, I.K.; Chung, I.S.; Song, D.H.; Park, S.H.; Kim, H.S.; Lee, M.H. The clinical significance of upper gastrointestinal endoscopy in gastrointestinal vasculitis related to scrub typhus. Endoscopy 2000, 32, 950–955. [Google Scholar] [CrossRef] [PubMed]
- Seong, S.Y.; Choi, M.S.; Kim, I.S. Orientia tsutsugamushi infection: Overview and immune responses. Microbes Infect. 2001, 3, 11–21. [Google Scholar] [CrossRef]
- Strickman, D.; Smith, C.D.; Corcoran, K.D.; Ngampochjana, M.; Watcharapichat, P.; Phulsuksombati, D.; Tanskul, P.; Dasch, G.A.; Kelly, D.J. Pathology of Rickettsia tsutsugamushi infection in Bandicota savilei, a natural host in Thailand. Am. J. Trop. Med. Hyg. 1994, 51, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Chung, K.M.; Kim, E.S.; Kwak, Y.G.; Moon, C.; Lee, C.S. Dynamics of clinical symptoms in patients with scrub typhus. Jpn. J. Infect. Dis. 2013, 66, 155–157. [Google Scholar] [CrossRef] [PubMed]
- Naoi, T.; Shimazaki, H.; Sawada, M. The rapid effectiveness of minocycline against scrub typhus meningoencephalitis. Intern. Med. 2016, 55, 805–809. [Google Scholar] [CrossRef] [PubMed]
- Koh, G.C.; Maude, R.J.; Paris, D.H.; Newton, P.N.; Blacksell, S.D. Diagnosis of scrub typhus. Am. J. Trop. Med. Hyg. 2010, 82, 368–370. [Google Scholar] [CrossRef] [PubMed]
- Henter, J.I.; Horne, A.; Aricó, M.; Egeler, R.M.; Filipovich, A.H.; Imashuku, S.; Ladisch, S.; McClain, K.; Webb, D.; Winiarski, J.; et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr. Blood Cancer 2007, 48, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Casals, M.; Brito-Zerón, P.; López-Guillermo, A.; Khamashta, M.A.; Bosch, X. Adult haemophagocytic syndrome. Lancet 2014, 383, 1503–1516. [Google Scholar] [CrossRef]
- Lilic, D.; Cant, A.J.; Abinun, M.; Calvert, J.E.; Spickett, G.P. Cytokine production differs in children and adults. Pediatr. Res. 1997, 42, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Takizawa, H.; Hiroshima, K.; Uruma, T.; Enokihara, H.; Okuyama, A. A case of new type scrub typhus (tsutsugamushi disease) presenting with acute respiratory failure and hemophagocytic syndrome. Nihon Kyobu Shikkan Gakkai Zasshi 1992, 30, 447–452. [Google Scholar] [PubMed]
- Iwasaki, H.; Hashimoto, K.; Takada, N.; Nakayama, T.; Ueda, T.; Nakamura, T. Fulminant Rickettsia tsutsugamushi infection associated with haemophagocytic syndrome. Lancet 1994, 343, 1236. [Google Scholar] [CrossRef]
- Chen, Y.C.; Chao, T.Y.; Chin, J.C. Scrub typhus-associated hemophagocytic syndrome. Infection 2000, 28, 178–179. [Google Scholar] [CrossRef] [PubMed]
- Wada, M.; Yamane, Y.; Tsumori, M.; Kato, Y. Tsutsugamushi disease-associated hemophagocytic syndrome. Rinsho Kenkyu 2001, 78, 1173–1176. [Google Scholar]
- Takami, A.; Yamauchi, H.; Asakura, H.; Ishiyama, K.; Nakao, S. Tsutsugamushi disease (scrub typhus)-associated hemophagocytic syndrome. Int. J. Hematol. 2002, 75, 337–338. [Google Scholar] [CrossRef] [PubMed]
- Miyakawa, K.; Ohsugi, K.; Kuriyama, C.; Sugahara, S.; Kikuchi, A.; Ohta, M. Tsutsugamushi disease with hemophagocytosis complicated by parvovirus B19 infection. Nippon Naika Gakkai Zashi 2006, 95, 2544–2546. [Google Scholar] [CrossRef]
- Premaratna, R.; Williams, H.S.; Chandrasena, T.G.; Rajapakse, R.P.; Kularatna, S.A.; de Silva, H.J. Unusual pancytopenia secondary to haemophagocytosis syndrome in rickettsioses. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 961–963. [Google Scholar] [CrossRef] [PubMed]
- Valsalan, R.; Kosaraju, K.; Sohanlal, T.; Kumar, P.S. Hemophagocytosis in scrub typhus. J. Postgrad. Med. 2010, 56, 301–302. [Google Scholar] [CrossRef] [PubMed]
- Gopal, G.K.; Anugrah, C.; Boorugu, H. Scrub typhus associated macrophage activation syndrome. Trop. Dr. 2010, 40, 249–250. [Google Scholar] [CrossRef] [PubMed]
- Jayakrishnan, M.P.; Veny, J.; Feroze, M. Rickettsial infection with hemophagocytosis. Trop. Dr. 2011, 41, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Han, D.K.; Baek, H.J.; Shin, M.G.; Kim, J.W.; Kook, H.; Hwang, T.J. Scrub typhus-associated severe hemophagocytic lymphohistiocytosis with encephalomyelitis leading to permanent sequelae: A case report and review of the literature. J. Pediatr. Hematol. Oncol. 2012, 34, 531–533. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J.; Yoo, I.H.; Lee, J.W.; Chung, N.G.; Cho, B.; Kim, H.K.; Kang, J.H. Life-threatening scrub typhus with hemophagocytosis and acute respiratory distress syndrome in an infant. J. Trop. Pediatr. 2013, 59, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Shi, Z.Y. A case report of scrub typhus-associated hemophagocytic syndrome and a review of literature. Jpn. J. Infect. Dis. 2014, 67, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Diwan, A.G.; Shewale, R.; Iyer, S.; Nisal, A.; Agrawa, P. Triple trouble--macrophage activation syndrome in a case of severe leptospirosis and scrub typhus co-infection. J. Assoc. Physicians India 2014, 62, 58–61. [Google Scholar] [PubMed]
- Basheer, A.; Padhi, S.; Boopathy, V.; Mallick, S.; Nair, S.; Varghese, R.G.; Kanungo, R. Hemophagocytic lymphohistiocytosis: An unusual complication of Orientia tsutsugamushi disease (scrub typhus). Mediterr. J. Hematol. Infect. Dis. 2015, 7, e2015008. [Google Scholar] [CrossRef] [PubMed]
- Pazhaniyandi, S.; Lenin, R.; Sivathanu, S. Hemophagocytic lymphohistiocytosis with a leukemoid reaction in an infant with scrub typhus. J. Infect. Public Health 2015, 8, 626–629. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.H.; Xia, F.Q.; Van Poucke, S.; Zheng, M.H. Successful treatment of scrub typhus-associated hemophagocytic lymphohistiocytosis with chloramphenicol: Report of 3 pediatric cases and literature review. Medicine (Baltimore) 2016, 95, e2928. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Huang, L.; Fan, H.; Lu, G.; Xu, Y.; Wu, Z. Scrub typhus associated with hemophagocytic lymphohistiocytosis: A report of six pediatric patients. Exp. Ther. Med. 2016, 12, 2729–2734. [Google Scholar] [CrossRef] [PubMed]
- Imashuku, S.; Teramura, T.; Tauchi, H.; Ishida, Y.; Otoh, Y.; Sawada, M.; Tanaka, H.; Watanabe, A.; Tabata, Y.; Morimoto, A.; Hibi, S.; Henter, J.I. Longitudinal follow-up of patients with Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis. Haematologica 2004, 89, 183–188. [Google Scholar] [PubMed]
- Lu, G.; Xie, Z.D.; Shen, K.L.; Wu, R.H.; Jin, Y.K.; Yang, S.; Liu, C.Y. Clinical analysis and follow-up study of Epstein-Barr virus associated-hemophagocytic lymphohistiocytosis in childhood. Zhonghua Er Ke Za Zhi 2010, 48, 121–126. [Google Scholar] [PubMed]
- Brastianos, P.K.; Swanson, J.W.; Torbenson, M.; Sperati, J.; Karakousis, P.C. Tuberculosis-associated haemophagocytic syndrome. Lancet Infect. Dis. 2006, 6, 447–454. [Google Scholar] [CrossRef]
- Otrock, Z.K.; Eby, C.S. Clinical characteristics, prognostic factors, and outcomes of adult patients with hemophagocytic lymphohistiocytosis. Am. J. Hematol. 2015, 90, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Hwang, J.H.; Lee, H.B.; Kwon, K.S. Risk factors leading to fatal outcome in scrub typhus patients. Am. J. Trop. Med. Hyg. 2009, 81, 484–488. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, M.; Hagiwara, T.; Kishimoto, T.; Shiga, S.; Yoshida, Y.; Furuya, Y.; Kaiho, I.; Ito, T.; Nemoto, H.; Yamamoto, N.; et al. Scrub typhus in Japan: Epidemiology and clinical features of cases reported in 1998. Am. J. Trop. Med. Hyg. 2002, 67, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kim, S.J.; Youn, S.K.; Park, K.; Gwack, J. Epidemiology of scrub typhus and the eschars patterns in South Korea from 2008 to 2012. Jpn. J. Infect. Dis. 2014, 67, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Sonthayanon, P.; Chierakul, W.; Wuthiekanun, V.; Phimda, K.; Pukrittayakamee, S.; Day, N.P.; Peacock, S.J. Association of high Orientia tsutsugamushi DNA loads with disease of greater severity in adults with scrub typhus. J. Clin. Microbiol. 2009, 47, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Varghese, G.M.; Abraham, O.C.; Mathai, D.; Thomas, K.; Aaron, R.; Kavitha, M.L.; Mathai, E. Scrub typhus among hospitalised patients with febrile illness in South India: Magnitude and clinical predictors. J. Infect. 2006, 52, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Thompson, B.T.; Chambers, R.C.; Liu, K.D. Acute respiratory distress syndrome. N. Engl. J. Med. 2017, 377, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.S.; Zimmerman, J.J.; Martin, T.R. Mechanisms of acute respiratory distress syndrome in children and adults: a review and suggestions for future research. Pediatr. Crit. Care Med. 2013, 14, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Misra, U.K.; Kalita, J.; Mani, V.E. Neurological manifestations of scrub typhus. J. Neurol. Neurosurg. Psychiatry 2015, 86, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Settle, E.B.; Pinkerton, H.; Corbett, A.J. A pathologic study of tsutsugamushi disease (scrub typhus) with notes on clinicopathologic correlation. J. Lab. Clin. Med. 1945, 30, 639–661. [Google Scholar]
- Hwang, K.; Jang, H.N.; Lee, T.W.; Cho, H.S.; Bae, E.; Chang, S.H.; Park, D.J. Incidence, risk factors and clinical outcomes of acute kidney injury associated with scrub typhus: A retrospective study of 510 consecutive patients in South Korea (2001-2013). BMJ Open 2017, 7, e013882. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Yadav, A.K.; Iyengar, S.; Bhalla, A.; Sharma, N.; Aggarwal, R.; Jain, S.; Jha, V. Scrub typhus is an under-recognized cause of acute febrile illness with acute kidney injury in India. PLoS Negl. Trop. Dis. 2014, 8, e2605. [Google Scholar] [CrossRef] [PubMed]
- Murai, K.; Okayama, A.; Horinouchi, H.; Oshikawa, T.; Tachibana, N.; Tsubouchi, H. Eradication of Rickettsia tsutsugamushi from patients’ blood by chemotherapy, as assessed by the polymerase chain reaction. Am. J. Trop. Med. Hyg. 1995, 52, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Tai, K.; Iwasaki, H.; Ikegaya, S.; Ueda, T. Minocycline modulates cytokine and chemokine production in lipopolysaccharide-stimulated THP-1 monocytic cells by inhibiting IκB kinase α/β phosphorylation. Transl. Res. 2013, 161, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Chung, D.R.; Lee, Y.S.; Lee, S.S. Kinetics of inflammatory cytokines in patients with scrub typhus receiving doxycycline treatment. J. Infect. 2008, 56, 44–50. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Year (Reference) | Case No. | Age/Sex | Country | Eschar Location | Diagnostic Test for Scrub Typhus | HPS Findings in BM | HLH Criteria 2004 | Outcome |
|---|---|---|---|---|---|---|---|---|
| 1992 [13] | 1 | 47/male | Japan | ND | IFA; Gilliam | + | ND | survived/cured |
| 1994 [14] | 2 | 53/female | Japan | back | IFA; Gilliam | + | ND | survived/cured |
| 2000 [15] | 3 | 21/male | Taiwan | ND | Weil–Felix; OX-K | + | ND | survived/cured |
| 2001 [16] | 4 | 53/female | Japan | left thigh | IFA; Karp | + | ND | survived/cured |
| 2002 [17] | 5 | 75/female | Japan | left buttock | IFA; Gilliam | + | ND | survived/cured |
| 6 | 69/female | Japan | left leg | IFA; Gilliam | + | ND | survived/cured | |
| 2006 [18] | 7 | 74/female | Japan | external genitalia | IFA; Karp, Kato, Gilliam | + | ND | survived/cured |
| 2009 [19] | 8 | 58/female | Sri Lanka | perineum | IgG IFA | + | ND | survived/cured |
| 2010 [20] | 9 | 22/male | India | not detected | Weil–Felix; OX-K, IgM ELISA | + | ND | survived/cured |
| 2010 [21] | 10 | 35/male | India | posterior chest wall | IgM ELISA | + | ND | survived/cured |
| 11 | 61/male | India | ND | IgM ELISA | + | ND | survived/cured | |
| 12 | 23/male | India | ND | IgM ELISA | + | ND | survived/cured | |
| 2011 [22] | 13 | 5/female | India | hypogastrium | Weil–Felix; OX-K, IgM | + | criteria not met | survived/cured |
| 2012 [23] | 14 | 9/female | South Korea | scalp | IgM IFA | + | criteria is met | survived with sequela |
| 2013 [24] | 15 | 8 months/male | South Korea | right inguinal area | IgM IHA | ND | criteria is met | survived/cured |
| 2014 [25] | 16 | 34/female | Taiwan | not detected | Weil–Felix; OX-K, IgM, PCR | + | criteria is met | died |
| 2014 [26] | 17 | 40/female | India | ND | Weil–Felix; OX-K | + | criteria is met | survived/cured |
| 2015 [27] | 18 | 19/female | India | not detected | IgM ELISA | + | criteria is met | survived/cured |
| 19 | 64/male | India | not detected | IgM ELISA | + | criteria is met | survived/cured | |
| 20 | 45/male | India | left groin | IgM ELISA | + | criteria is met | survived/cured | |
| 2015 [28] | 21 | 2 months/male | India | not detected | IgM ELISA | not observed | criteria is met | survived/cured |
| 2016 [29] | 22 | 6/male | China | left shoulder | Weil–Felix; OX-K | + | criteria is met | survived/cured |
| 23 | 4/female | China | right opisthotic area | Weil–Felix; OX-K | + | criteria is met | survived/cured | |
| 24 | 3/female | China | left forearm | Weil–Felix; OX-K | + | criteria is met | survived/cured | |
| 2016 [30] | 25 | 8 months/male | China | + (location not described) | Weil–Felix and/or IgM IFA | + | criteria is met | died |
| 26 | 1/female | China | + (location not described) | Weil–Felix and/or IgM IFA | + | criteria is met | survived/cured | |
| 27 | 7/male | China | + (location not described) | Weil–Felix and/or IgM IFA | + | criteria is met | survived/cured | |
| 28 | 7/female | China | + (location not described) | Weil–Felix and/or IgM IFA | + | criteria is met | survived/cured | |
| 29 | 11/male | China | + (location not described) | Weil–Felix and/or IgM IFA | + | criteria is met | survived/cured | |
| 30 | 7/male | China | + (location not described) | Weil–Felix and/or IgM IFA | + | criteria is met | survived/cured |
| Case No. | Age/Sex | Illness Days Prior to Admission | Illness Days Prior to Antibiotics | Illness Days Prior to Additional Treatment | Days to Confirm HLH | Treatment | Fever Subsided after Initiation Antibiotics | |
|---|---|---|---|---|---|---|---|---|
| Antibiotics | Additional treatment | |||||||
| 1 | 47/male | 11 days | 13 days | 12 days | 11 days | minocycline | PSL | within 24 h |
| 2 | 53/female | ND | ND | not treated | ND | minocycline | within 72 h | |
| 3 | 21/male | 14 days | ND | not treated | ND | doxycycline | within 24 h | |
| 4 | 53/female | 8 days | 8 days | not treated | 8 days | minocycline | within 72 h | |
| 5 | 75/female | ND | ND | ND | ND | doxycycline | PSL | within 72 h |
| 6 | 69/female | 7 days | ND | not treated | ND | minocycline | ND | |
| 7 | 74/female | 4 days | 7 day | not treated | ND | minocycline | within 24 h | |
| 8 | 58/female | 10 days | 24 days | not treated | ND | doxycycline | within 72 h | |
| 9 | 22/male | 10 days | 12 days | not treated | ND | doxycycline | within 72 h | |
| 10 | 35/male | 10 days | ND | not treated | ND | doxycycline | within 96 h | |
| 11 | 61/male | 20 days | ND | not treated | ND | doxycycline | within 72 h | |
| 12 | 23/male | 5 days | ND | not treated | ND | doxycycline | within 48 h | |
| 13 | 5/female | 6 days | 7 days | not treated | ND | doxycycline | within 48 h | |
| 14 | 9/female | 7 days | 18 days | 9 days | 9 days | (roxithromycin) | DEX, cyclosporine, etoposide | after 96 h |
| doxycycline | intrathecal methotrexate | |||||||
| 15 | 8 months/male | 10 days | 10 days | ND | ND | clarithromycin | DEX, etoposide | within 96 h |
| 16 | 34/female | 7 days | 7 days | not treated | ND | minocycline | (died) | |
| 17 | 40/female | 10 days | ND | ND | ND | doxycycline | mPSL | ND |
| 18 | 19/female | ND | ND | ND | ND | doxycycline | corticosteroid, etoposide | ND |
| 19 | 64/male | ND | ND | ND | ND | doxycycline | ND | |
| 20 | 45/male | ND | ND | ND | ND | doxycycline | ND | |
| 21 | 2 months/male | 5 days | 9 days | 9 days | 9 days | doxycycline | IVIG | within 24 h |
| 22 | 6/male | 7 days | 7 days | not treated | ND | chloramphenicol | within 24 h | |
| 23 | 4/female | 9 days | 9 days | not treated | ND | chloramphenicol | within 48 h | |
| 24 | 3/female | 8 days | 8 days | not treated | ND | chloramphenicol | within 24 h | |
| 25 | 8 months/male | 9 days | ND | ND | ND | azithromycin | IVIG/mPSL | (died) |
| 26 | 1/female | 4 days | ND | ND | ND | azithromycin | IVIG/mPSL | ND |
| 27 | 7/male | 12 days | ND | ND | ND | doxycycline | IVIG/mPSL | ND |
| 28 | 7/female | 9 days | ND | ND | ND | doxycycline | IVIG/mPSL | ND |
| 29 | 11/male | 7 days | ND | ND | ND | doxycycline | IVIG | ND |
| 30 | 7/male | 7 days | ND | ND | ND | doxycycline | IVIG/mPSL | ND |
| The diagnosis of HLH can be established if any one of two given factors is fulfilled: |
| 1. A molecular diagnosis consistent with HLH |
| 2. Diagnostic criteria for HLH are fulfilled (5 or more of 8 criteria below)* |
| Fever |
| Splenomegaly |
| Cytopenias (affecting ≥2 of 3 lineages in the peripheral blood) |
| Hemoglobin <90 g/L (in infants <4 weeks old; hemoglobin <100 g/L) |
| Platelets <100 × 109/L |
| Neutrophils <1.0 × 109/L |
| Hypertriglyceridemia and/or hypofibrinogenemia: fasting |
| Hypertriglyceridemia ≥3.0 mmol/L (i.e., ≥265 mg/dl), fibrinogen ≤1.5 g/L |
| Hemophagocytosis in the bone marrow, spleen, or lymph nodes |
| Low or absent natural killer cell activity (according to the local laboratory reference) |
| Ferritin ≥500 µg/L |
| Soluble CD25 (i.e., sIL2r) ≥2400 U/mL |
| Pediatric Group (n = 13) | Adult Group (n = 17) | p-value | |
|---|---|---|---|
| Age range/median age | 2 months–11 years/5.0 years | 19–74 years/47.0 years | |
| Female | 6/13 (46.2%) | 9/17 (52.9%) | 0.712 |
| Mortality | 1/13 (7.7%) | 1/17 (5.9%) | 0.844 |
| Respiratory system | |||
| ARDS | 7/13 (53.8%) | 4/17 (23.5%) | 0.132 |
| Pleural effusion | 0/13 (0%) | 1/17 (5.9%) | 0.567 |
| Pulmonary hemorrhage | 1/13 (7.7%) | 0/17 (0%) | 0.433 |
| Bronchitis | 1/13 (7.7%) | 0/17 (0%) | 0.433 |
| Invasive ventilator use | 7/13 (53.8%) | 5/17 (29.4%) | 0.175 |
| Central nervous system | |||
| Seizure | 3/13 (23.1%) | 1/17 (5.9%) | 0.290 |
| Consciousness disturbance | 0/13 (0%) | 1/17 (5.9%) | 0.567 |
| Intracranial hemorrhage | 1/13 (7.7%) | 1/17 (5.9%) | 1.000 |
| Altered sensorium | 1/13 (7.7%) | 0/17 (0%) | 0.433 |
| Altered mental status | 1/13 (7.7%) | 0/17 (0%) | 0.433 |
| Meningitis | 1/13 (7.7%) | 0/17 (0%) | 0.433 |
| Encephalomyelitis | 1/13 (7.7%) | 0/17 (0%) | 0.433 |
| Gastrointestinal system | |||
| Gall bladder distension | 0/13 (0%) | 1/17 (5.9%) | 0.567 |
| Abdominal pain | 0/13 (0%) | 2/17 (11.8%) | 0.492 |
| Other complication | |||
| Fever | 13/13 (100%) | 17/17 (100%) | |
| Skin rash | 9/13 (69.2%) | 6/17 (35.3%) | 0.065 |
| Eschar | 12/13 (92.3%) | 8/17 (47.1%) | 0.017 |
| Splenomegaly ± hepatomegaly | 11/13 (84.6%) | 14/17 (82.4%) | 1.000 |
| Liver dysfunction | 13/13 (100%) | 15/17 (88.2%) | 0.492 |
| Lymphadenopathy | 5/13 (38.5%) | 8/17 (47.1%) | 0.638 |
| Acute kidney injury | 0/13 (0%) | 7/17 (41.2%) | 0.010 |
| Pedal edema | 0/13 (0%) | 1/17 (5.9%) | 0.567 |
| Tonsillar swelling | 0/13 (0%) | 2/17 (11.8%) | 0.492 |
| Myalgia | 0/13 (0%) | 2/17 (11.8%) | 0.492 |
| Leukemoid reaction | 1/13 (7.7%) | 0/17 (0%) | 0.433 |
| Hydrocele | 1/13 (7.7%) | 0/17 (0%) | 0.433 |
| Arthralgia | 0/13 (0%) | 1/17 (5.9%) | 0.567 |
| Pediatric Group (0–11 years) | Adult Group (≥19 years) | p-value | |
|---|---|---|---|
| Hematological | |||
| Hemoglobin <90 g/L | 10/13 (76.9%) | 10/15 (66.7%) | 0.686 |
| Platelets <100 × 109/L | 12/13 (92.3%) | 14/17 (82.4%) | 0.613 |
| Neutrophils <1.0 × 109/L | 0/4 (0%) | 6/12 (50%) | 0.234 |
| Coagulation | |||
| Fibrinogen ≤1.5 g/L | 9/12 (75%) | 1/5 (20%) | 0.101 |
| Biochemical features | |||
| Ferritin ≥500 µg/L | 13/13 (100%) | 11/13 (84.6%) | 0.480 |
| Triglycerides ≥265 mg/dl | 9/11 (81.8%) | 4/9 (44.4%) | 0.160 |
| Soluble CD25 (i.e., sil2r) ≥2400 U/ml | not examined | 2/2 (100%) | |
| Low or absent natural killer cell activity | 3/4 (75%) | not examined | |
| AST or ALT ≥50 IU/L | 12/12 (100%) | 13/17 (76.5%) | 0.121 |
| Creatinine ≥1.0 mg/dl | 0/3 (0%) | 5/10 (50%) | 0.231 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naoi, T.; Morita, M.; Kawakami, T.; Fujimoto, S. Hemophagocytic Lymphohistiocytosis Associated with Scrub Typhus: Systematic Review and Comparison between Pediatric and Adult Cases. Trop. Med. Infect. Dis. 2018, 3, 19. https://doi.org/10.3390/tropicalmed3010019
Naoi T, Morita M, Kawakami T, Fujimoto S. Hemophagocytic Lymphohistiocytosis Associated with Scrub Typhus: Systematic Review and Comparison between Pediatric and Adult Cases. Tropical Medicine and Infectious Disease. 2018; 3(1):19. https://doi.org/10.3390/tropicalmed3010019
Chicago/Turabian StyleNaoi, Tameto, Mitsuya Morita, Tadataka Kawakami, and Shigeru Fujimoto. 2018. "Hemophagocytic Lymphohistiocytosis Associated with Scrub Typhus: Systematic Review and Comparison between Pediatric and Adult Cases" Tropical Medicine and Infectious Disease 3, no. 1: 19. https://doi.org/10.3390/tropicalmed3010019
APA StyleNaoi, T., Morita, M., Kawakami, T., & Fujimoto, S. (2018). Hemophagocytic Lymphohistiocytosis Associated with Scrub Typhus: Systematic Review and Comparison between Pediatric and Adult Cases. Tropical Medicine and Infectious Disease, 3(1), 19. https://doi.org/10.3390/tropicalmed3010019