

The Factors Influencing the Incidence, Persistence, and Severity of Symptoms After SARS-CoV-2 Infection in Chinese Adults: A Case–Control Study

 , , ,
, , ,
Abstract
1. Introduction
2. Method
2.1. Data Sources
2.2. Study Participants
2.3. Study Design
2.4. Statistical Analyses
3. Results
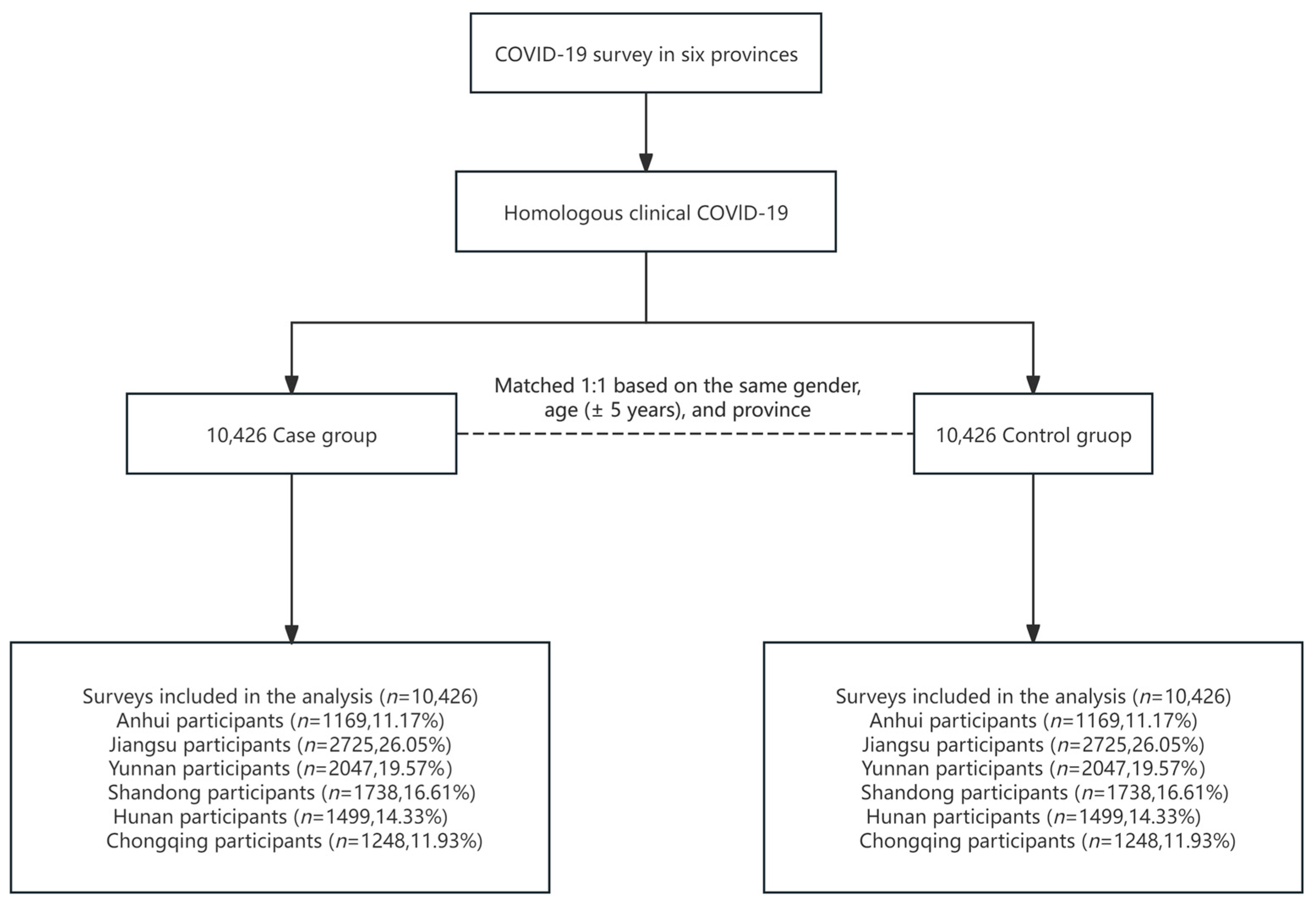
3.1. Description of Study Population
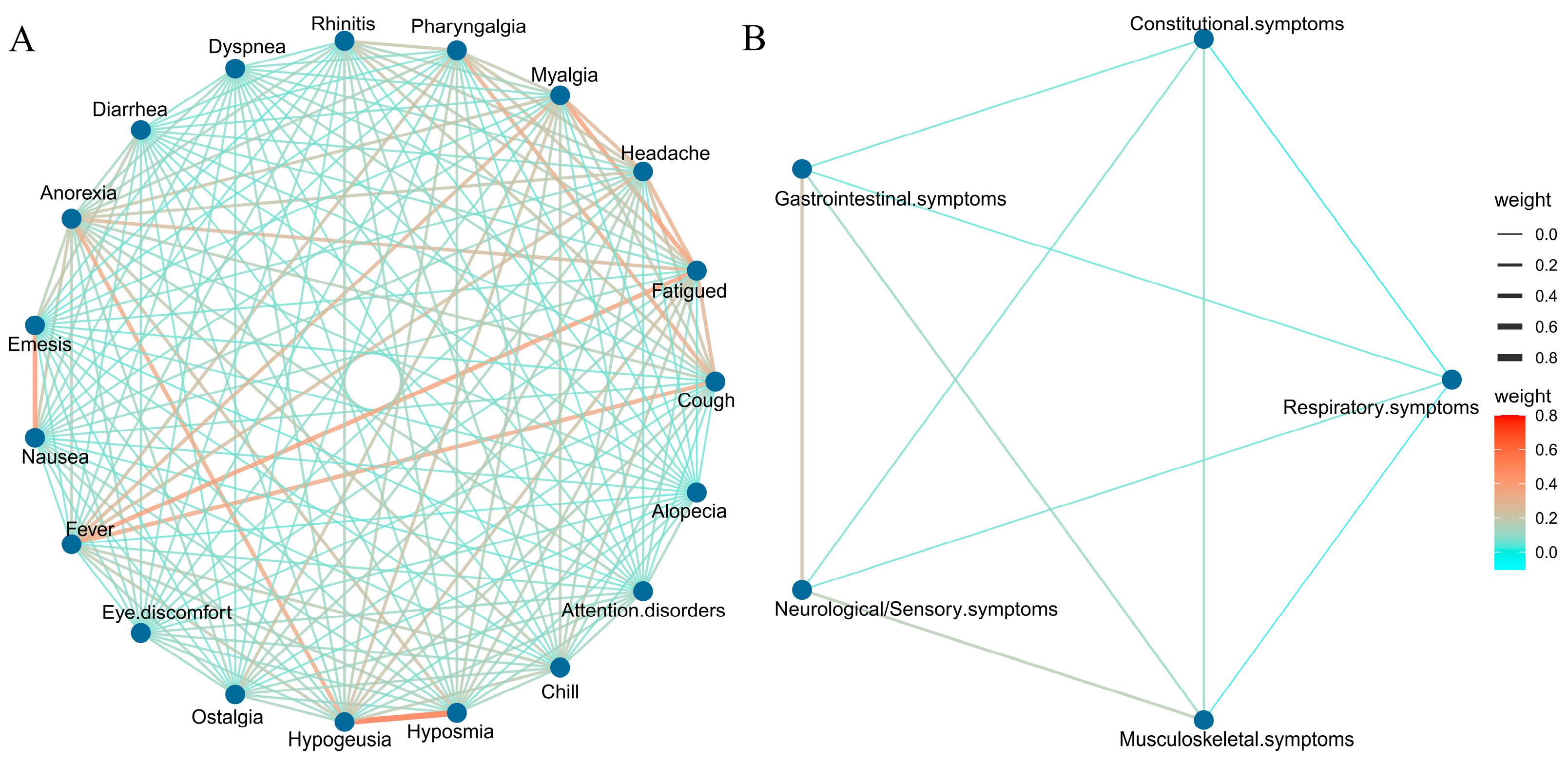
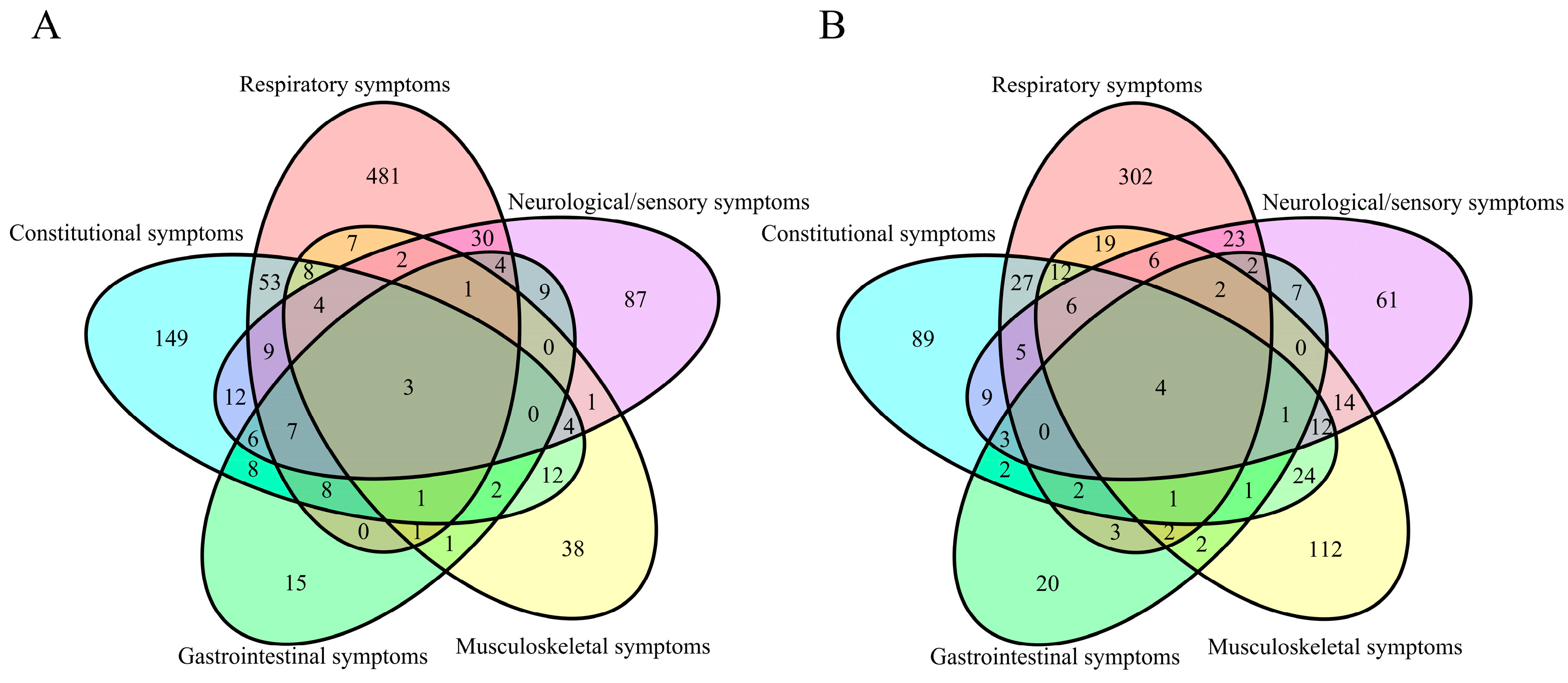
3.2. COVID-19 Symptoms
3.3. Factors Associated with the Incidence of COVID-19
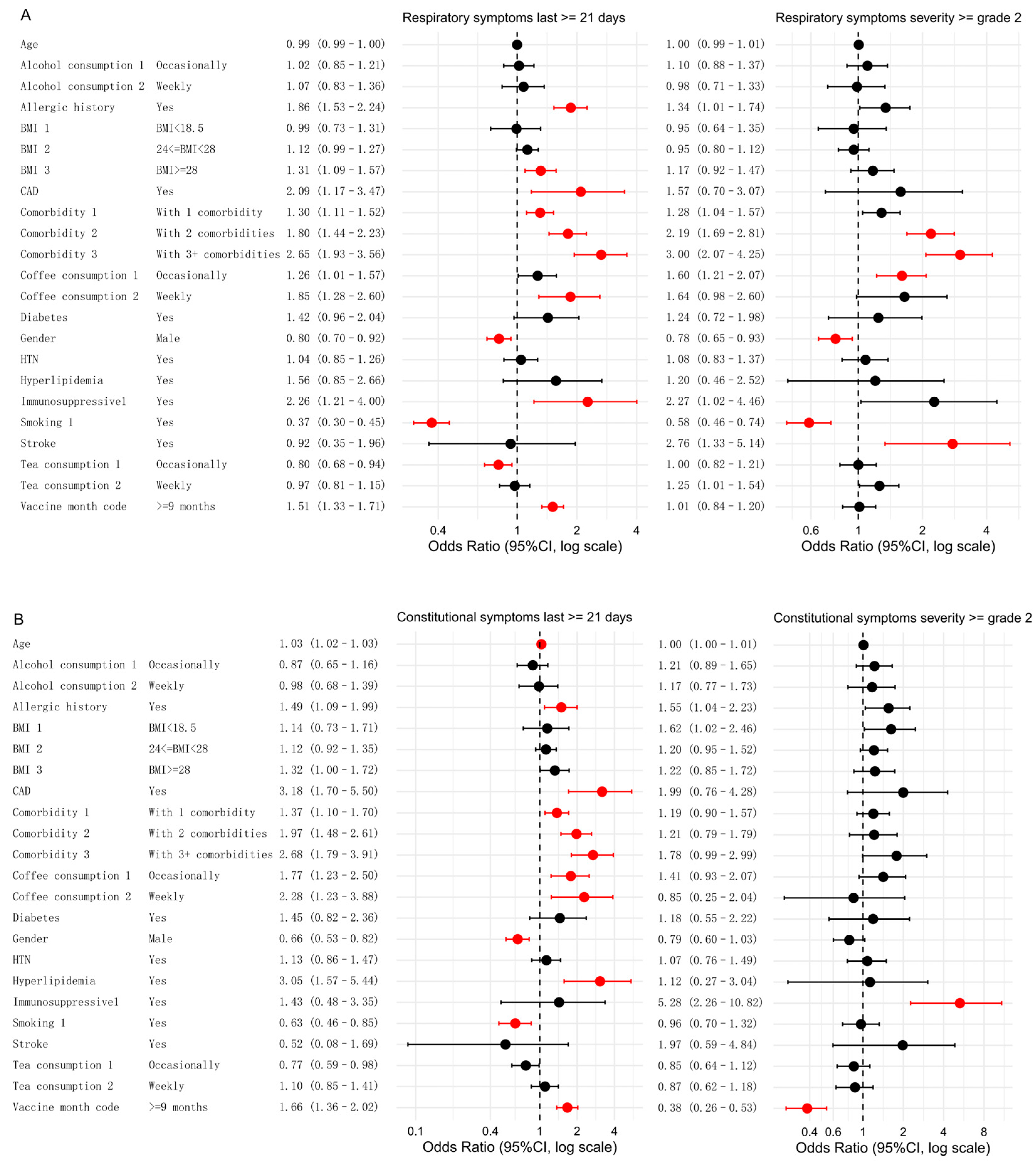
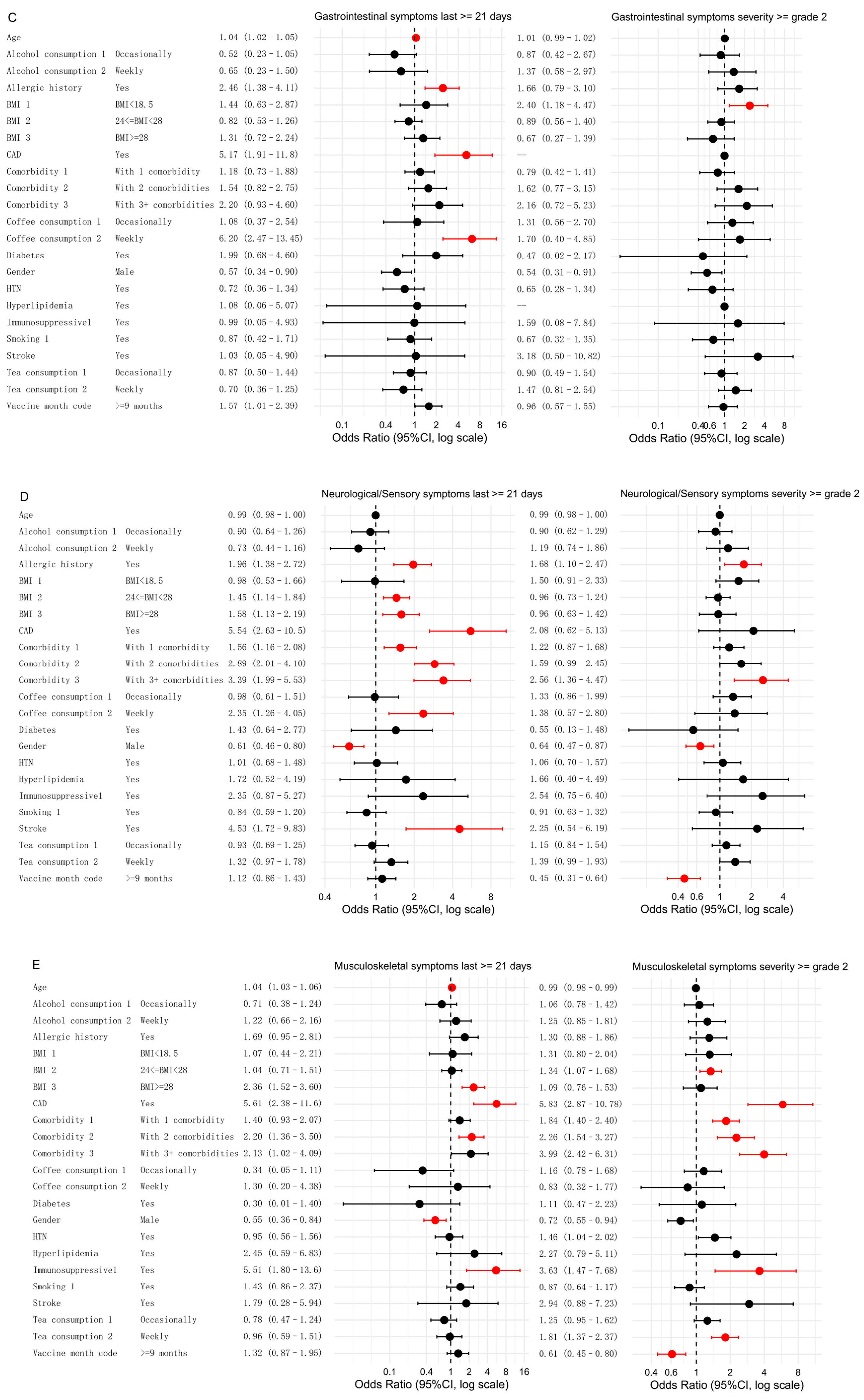
3.4. Factors Associated with Symptom Categories
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade Classification |
|---|
| COVID-19 symptoms |
| Cough |
| Grade 1: Mild symptoms; require over-the-counter medication |
| Grade 2: Require prescription medication; affect instrumental activities of daily living * |
| Grade 3: Severe symptoms; limited self-care ability |
| Fatigue |
| Grade 1: Fatigue, relieved after resting |
| Grade 2: Fatigue, not relieved after resting |
| Grade 3: Fatigue, not relieved after resting; affects personal daily activities |
| Headache |
| Grade 1: Mild headache |
| Grade 2: Moderate headache; affects instrumental activities of daily living * |
| Grade 3: Severe headache; limited self-care ability |
| Myalgia |
| Grade 1: Mild pain |
| Grade 2: Moderate pain; affects instrumental activities of daily living * |
| Grade 3: Severe pain; affects personal daily activities |
| Pharyngalgia |
| Grade 1: Mild throat pain; rough sound |
| Grade 2: Moderate throat pain; requires analgesics |
| Grade 3: Moderate throat pain; requires analgesics |
| Rhinitis (nasal obstruction/itching/runny nose/sneezing) |
| Grade 1: Mild symptoms; no intervention needed |
| Grade 2: Moderate symptoms; medical intervention required |
| Grade 3: With bloody nasal secretions or nosebleeds |
| Dyspnea |
| Grade 1: Shortness of breath with moderate activities |
| Grade 2: Shortness of breath with minimal activity |
| Grade 3: Shortness of breath at rest; limited self-care ability |
| Grade 4: Life-threatening; requires urgent intervention |
| Grade 5: Death |
| Nausea |
| Grade 1: Decreased appetite without changes in diet habits |
| Grade 2: Reduced oral intake without significant weight loss, dehydration, or malnutrition |
| Grade 3: Inadequate oral intake of energy and fluids; requires nasogastric, parenteral nutrition, or hospitalization |
| Vomiting |
| Grade 1: 1–2 episodes within 24 h (5 min intervals) |
| Grade 2: 3–5 episodes within 24 h (5 min intervals) |
| Grade 3: ≥6 episodes within 24 h (5 min intervals) |
| Grade 4: Life-threatening; requires urgent treatment |
| Grade 5: Death |
| Diarrhea |
| Grade 1: Less than four bowel movements per day compared to baseline; slight increase in stoma output |
| Grade 2: 4–6 bowel movements per day compared to baseline; intravenous hydration <24 h; moderate increase in stoma output |
| Grade 3: ≥7 bowel movements per day compared to baseline; fecal incontinence; requires inpatient treatment; severe increase in stoma output; affects instrumental activities of daily living |
| Grade 4: Life-threatening; requires urgent treatment |
| Grade 5: Death |
| Anorexia |
| Grade 1: Reduced appetite without changes in diet habits |
| Grade 2: Altered diet but without weight loss or malnutrition; oral nutritional supplementation required |
| Grade 3: Altered diet but without weight loss or malnutrition; oral nutritional supplementation required |
| Grade 4: Life-threatening; requires urgent treatment |
| Grade 5: Death |
| Ophthalmalgia/Redness and Swelling/Conjunctivitis/Eye discomfort |
| Grade 1: Mild pain |
| Grade 2: Moderate pain; affects instrumental activities of daily living * |
| Grade 3: Severe pain; affects personal daily activities |
| Ostalgia |
| Grade 1: Mild pain |
| Grade 2: Moderate pain; affects instrumental activities of daily living * |
| Grade 3: Severe pain; affects personal daily activities |
| Hyposmia |
| Grade 1: Altered sense of smell but does not affect normal diet habits |
| Grade 2: Altered taste affecting normal diet habits (e.g., oral supplements); toxic or uncomfortable taste; loss of taste |
| Chills |
| Grade 1: Mild sensation of cold; shivering; teeth chattering |
| Grade 2: Moderate full-body shivering; requires anesthesia |
| Grade 3: Severe or delayed response or lack of response to anesthesia. |
| Attention disorders |
| Grade 1: Mild inability to concentrate or decreased level of concentration |
| Grade 2: Moderate impairment of concentration; affects instrumental activities of daily living |
| Grade 3: Severe impairment of concentration or severely reduced level of concentration; inability to perform self-care |
| Alopecia |
| Grade 1: Less than 50% hair loss, no difference in appearance from a distance, but noticeable up close. Requires a change in hairstyle to conceal hair loss but does not require a wig or hairpiece |
| Grade 2: Greater than 50% hair loss, significantly noticeable symptoms, requires a wig or hairpiece, psychological impact |
| Others |
| Grade 1: Mild; asymptomatic or mild symptoms; only clinically or diagnostically discovered; no treatment required |
| Grade 2: Moderate; minimal, localized, or non-invasive treatment indications; impact on age-related instrumental activities of daily living |
| Grade 3: Severe or of significant medical importance but not immediately life-threatening; hospitalization or extension of hospitalization indications; disability; impact on self-care activities ** |
Appendix B. Method 1
- Demographic Characteristics
- Study Number: _____
- Place of Residence (Specify to the Village/Town):
- _______Province_______City_______District/County_______Town/Village/Street
- Height (cm)______
- Weight (kg)______
- Lifestyle
- Have you consumed alcohol in the past year__(1) Never/Rarely (2) Occasionally (3) Only during specific times (e.g., summer) (4) 1–3 times a month (5) ≥1 time a week [if choose 5, proceed to question 1.1; otherwise, skip to question 2]1.1 How many days a week have you consumed alcohol in the past year__(1) 1–2 days a week (2) 3–5 days a week (3) daily or nearly daily
- Have you smoked in the past year__(1) Never/Rarely (2) Occasionally (3) Only during specific times (e.g., holidays) (4) 1–3 times a month (5) ≥1 time a week [if choose 5, proceed to question 2.1; otherwise, skip to question 3]2.1 How many days a week have you smoked in the past year__(1) 1–2 days a week (2) 3–5 days a week (3) daily or nearly daily
- Have you consumed tea regularly in the past year__(1) Never/Rarely (2) Occasionally (3) Only during specific times (e.g., summer) (4) 1–3 times a month (5) ≥1 time a week [if choose 5, proceed to question 3.1; otherwise, skip to question 4]3.1 How many days a week have you consumed tea in the past year__(1) 1–2 days a week (2) 3–5 days a week (3) daily or nearly daily
- Have you consumed coffee regularly in the past year__(1) Never/Rarely (2) Occasionally (3) Only during specific times (e.g., summer) (4) 1–3 times a month (5) ≥1 time a week [if choose 5, proceed to question 4.1; otherwise, skip to question 5]4.1 How many days a week have you consumed coffee in the past year__(1) 1–2 days a week (2) 3–5 days a week (3) daily or nearly daily
- Medical History
- Do you have any of the following chronic diseases? (Select all that apply)(1) hypertension (2) diabetes (3) hyperlipidemia (4) coronary atherosclerotic heart disease (5) stroke (including ischemic and hemorrhagic) (6) tumors (7) chronic bronchitis (8) chronic kidney disease (9) HIV/AIDS (10) others__ (11) none
- Do you have a history of allergies or allergic reactions in the past__(1) Yes (2) No
- Have you received immunosuppressive treatment in the past six months (including allergy treatment, cytotoxic therapy, or the use of corticosteroid medications) __(1) Yes, the name of the medication is__ (2) No
- COVID-19 infection information
- Did you have a COVID-19 infection before 1 November 2022?(1) Yes (2) No
- Have you had a positive nucleic acid test result since 1 November 2022?(1) Yes, the first positive sample date was__ (2) No (3) Not done
- Have you had a positive antigen rapid test result since 1 November 2022?(1) Yes, the first positive sample date was __ (2) No (3) Not done
- Do you have any typical symptoms of COVID-19 infection? [If choose ‘Do not have typical symptoms,’ end the questionnaire.](1) Have typical symptoms (2) Do not have typical symptoms
- Since November 2022, the date of COVID-19 onset (first appearance of typical symptoms of COVID-19, such as fever, cough, fatigue, headache, muscle pain, sore throat, rhinitis, dyspnea, nausea/diarrhea/anorexia) was __
- What symptoms of infection have you experienced? (Multiple choices, if any, please fill in the highest grade)
- (1)
- Fever, or the highest body temperature is __ (degrees) (please fill in a value between 37.3–45.0 or “unknown”), duration (days) __
- (2)
- Cough, highest grade__, duration (days) __Grade classification: Grade 1: Mild symptoms; require over-the-counter medication; Grade 2: Require prescription medication; affect instrumental activities of daily living *;Grade 3: Severe symptoms; limited self-care ability.
- (3)
- Fatigue, highest grade__, duration (days) __Grade classification: Grade 1: Fatigue, relieved after resting; Grade 2: Fatigue, not relieved after resting; Grade 3: Fatigue, not relieved after resting; affects personal daily activities.
- (4)
- Headache, highest grade__, duration (days)__Grade classification: Grade 1: Mild headache; Grade 2: Moderate headache; affects instrumental activities of daily living*; Grade 3: Severe headache; limited self-care ability.
- (5)
- Muscle pain, highest grade__, duration (days)__Grade classification: Grade 1: Mild pain; Grade 2: Moderate pain; affects instrumental activities of daily living *; Grade 3: Severe pain; affects personal daily activities.
- (6)
- Sore throat, highest grade__, duration (days)__Grade classification: Grade 1: Mild throat pain; hoarseness; Grade 2: Moderate throat pain; requires analgesics; Grade 3: Severe throat pain; requires endoscopy.
- (7)
- Rhinitis (nasal obstruction/itching/runny nose/sneezing), highest grade__, duration (days)__Grade classification: Grade 1: Mild symptoms; no intervention needed; Grade 2: Moderate symptoms; medical intervention required; Grade 3: With bloody nasal secretions or nosebleeds.
- (8)
- Dyspnea, highest grade__, duration (days)__Grade classification: Grade 1: Shortness of breath with moderate activities; Grade 2: Shortness of breath with minimal activity; affects instrumental activities of daily living *; Grade 3: Shortness of breath at rest; limited self-care ability; Grade 4: Life-threatening; requires urgent intervention; Grade 5: Death.
- (9)
- Nausea, highest grade__, duration (days)__Grade classification: Grade 1: Decreased appetite without changes in diet habits; Grade 2: Reduced oral intake without significant weight loss, dehydration, or malnutrition; Grade 3: Inadequate oral intake of energy and fluids; requires nasogastric, parenteral nutrition, or hospitalization.
- (10)
- Vomiting, highest grade__, duration (days)__Grade classification: Grade 1: 1–2 episodes within 24 h (5-min intervals); Grade 2: 3–5 episodes within 24 h (5-min intervals); Grade 3: ≥6 episodes within 24 h (5-min intervals); Grade 4: Life-threatening; requires urgent treatment; Grade 5: Death.
- (11)
- Diarrhea, highest grade__, duration (days)__Grade classification: Grade 1: Less than 4 bowel movements per day compared to baseline; slight increase in stoma output; Grade 2: 4–6 bowel movements per day compared to baseline; intravenous hydration <24 h; moderate increase in stoma output; Grade 3: ≥7 bowel movements per day compared to baseline; fecal incontinence; requires inpatient treatment; severe increase in stoma output; affects instrumental activities of daily living; Grade 4: Life-threatening; requires urgent treatment; Grade 5: Death.
- (12)
- Anorexia, highest grade__, duration (days)__Grade classification: Grade 1: Reduced appetite without changes in diet habits; Grade 2: Altered diet but without weight loss or malnutrition; oral nutritional supplementation required; Grade 3: Marked weight loss or malnutrition symptoms (e.g., insufficient oral calorie intake); requires nasogastric or parenteral nutrition; Grade 4: Life-threatening; requires urgent treatment; Grade 5: Death.
- (13)
- Ophthalmalgia/Redness and Swelling/Conjunctivitis/Eye discomfort, highest grade__, duration (days)__Grade classification: Grade 1: Mild pain; Grade 2: Moderate pain; affects instrumental activities of daily living *; Grade 3: Severe pain; affects personal daily activities.
- (14)
- Bone pain, highest grade__, duration (days)__Grade classification: Grade 1: Mild pain; Grade 2: Moderate pain; affects instrumental activities of daily living *; Grade 3: Severe pain; affects personal daily activities.
- (15)
- Hyposmia, highest grade__, duration (days)__Grade classification: Grade 1: Altered sense of smell but does not affect normal diet habits; Grade 2: Altered sense of smell affecting normal diet habits (e.g., oral supplements); toxic or uncomfortable odor; loss of smell.
- (16)
- Hypogeusia, highest grade__, duration (days)__Grade classification: Grade 1: Altered taste but does not affect normal diet habits; Grade 2: Altered taste affecting normal diet habits (e.g., oral supplements); toxic or uncomfortable taste; loss of taste.
- (17)
- Chills, highest grade__, duration (days)__Grade classification: Grade 1: Mild sensation of cold; shivering; teeth chattering; Grade 2: Moderate full-body shivering; requires anesthesia; Grade 3: Severe or delayed response or lack of response to anesthesia.
- (18)
- Concentration disorders, highest grade__, duration (days)__Grade classification: Grade 1: Mild inability to concentrate or decreased level of concentration; Grade 2: Moderate impairment of concentration; affects instrumental activities of daily living; Grade 3: Severe impairment of concentration or severely reduced level of concentration; inability to perform self-care.
- (19)
- Hair loss, highest grade__, duration (days)__Grade classification: Grade 1: Less than 50% hair loss, no difference in appearance from a distance, but noticeable up close. Requires a change in hairstyle to conceal hair loss but does not require a wig or hairpiece; Grade 2: Greater than 50% hair loss, significantly noticeable symptoms, requires a wig or hairpiece, psychological impact.
- (20)
- Others__, highest grade__, duration (days)__Grade classification: Grade 1: Mild; asymptomatic or mild symptoms; only clinically or diagnostically discovered; no treatment required; Grade 2: Moderate; minimal, localized, or non-invasive treatment indications; impact on age-related instrumental activities of daily living; Grade 3: Severe or of significant medical importance but not immediately life-threatening; hospitalization or extension of hospitalization indications; disability; impact on self-care activities; Grade 4: Life-threatening, requiring urgent treatment; Grade 5: Death.
- 7.
- Has the symptoms of COVID-19 completely disappeared? [if no, proceed to question 9](1) Yes (2) No
- 8.
- Date when COVID-19 symptoms completely disappeared or tested negative: ____
- 9.
- Did you have any possible exposure to a confirmed or suspected COVID-19 case or a history of being in a location with potential exposure before the onset of typical symptoms (e.g., staying in a hospital or visiting crowded places)?(1) Yes (2) No
- 10.
- Have you sought medical care at an outpatient clinic due to a COVID-19 infection?(1) Yes (2) No
- 11.
- Have you been hospitalized due to a COVID-19 infection? [if no, proceed to question 13)(1) Yes (2) No
- 12.
- Did you receive any of the following treatments during the hospitalization?(1) Hospital treatment without oxygen supplementation(2) Hospital treatment with oxygen supplementation(3) Hospital treatment with high-flow oxygen therapy(4) Hospital treatment involving intubation and mechanical ventilation(5) Hospital treatment involving mechanical ventilation and external organ support, such as ECMO therapy
- 13.
- Did you take medication for the treatment of COVID-19__ [if no, proceed to question 15](1) Yes (2) No
- 14.
- Do you know the name of the medications you took?(1) Name of medications taken:Medication for COVID-19—Name 1: _____Duration of medication (days): _____Medication for COVID-19—Name 2: _____Duration of medication (days): _____Medication for COVID-19—Name 3: _____Duration of medication (days): _____Medication for COVID-19—Name 4: _____Duration of medication (days): _____Medication for COVID-19—Name 5: _____Duration of medication (days): _____Medication for COVID-19—Name 6: _____Duration of medication (days): _____Medication for COVID-19—Name 7: _____Duration of medication (days): _____Medication for COVID-19—Name 8: _____Duration of medication (days): _____Medication for COVID-19—Name 9: _____Duration of medication (days): _____Medication for COVID-19—Name 10: _____Duration of medication (days): _____
- 15.
- Severity of COVID-19 infection: __(1) Mild: Symptomatic patients meeting the case definition for COVID-19 without evidence of viral pneumonia or hypoxia.(2) Moderate: Adolescent or adult with clinical signs of pneumonia (fever, cough, dyspnoea, fast breathing) but no signs of severe pneumonia (including SpO2 ≥ 90% on room air).(3) Severe: Adolescent or adult with clinical signs of pneumonia (fever, cough, dyspnoea) plus one of the following: respiratory rate > 30 breaths/min, severe respiratory distress, or SpO2 < 90% on room air.(4) Critical: Acute respiratory distress syndrome (ARDS); or Sepsis; or Septic shock; or Acute thrombosis.
- 16.
- Did you experience a recurrence of COVID-19?(1) Yes, recurrence started on _____ and ended on ______.(2) No
- 17.
- Did you have any housemate (family members or door roommates, etc.) when infected with COVID-19 [if no, proceed to end](1) Yes (2) No
- 18.
- Infections status among housemates (family members or dorm roommates, etc.)
- Housemate 1
- ① Age (in years) ____
- ② Gender____ (1) Male (2) Female
- ③ COVID-19 vaccination status____ (1) Yes (2) No
- ④ Did they infect with COVID-19 (with typical symptoms, or positive nucleic acid test, or positive antigen rapid test) ____ (1) Yes (2) No
- Housemate 2
- ① Age (in years) ____
- ② Gender____ (1) Male (2) Female
- ③ COVID-19 vaccination status____ (1) Yes (2) No
- ④ Did they infect with COVID-19 (with typical symptoms, or positive nucleic acid test, or positive antigen rapid test) ____ (1) Yes (2) No
- Housemate 3
- ① Age (in years) ____
- ② Gender____ (1) Male (2) Female
- ③ COVID-19 vaccination status____ (1) Yes (2) No
- ④ Did they infect with COVID-19 (with typical symptoms, or positive nucleic acid test, or positive antigen rapid test) ____ (1) Yes (2) No
- Housemate 4
- ① Age (in years) ____
- ② Gender____ (1) Male (2) Female
- ③ COVID-19 vaccination status____ (1) Yes (2) No
- ④ Did they infect with COVID-19 (with typical symptoms, or positive nucleic acid test, or positive antigen rapid test) ____ (1) Yes (2) No
- Housemate 5
- ① Age (in years) ____
- ② Gender____ (1) Male (2) Female
- ③ COVID-19 vaccination status____ (1) Yes (2) No
- ④ Did they infect with COVID-19 (with typical symptoms, or positive nucleic acid test, or positive antigen rapid test) ____ (1) Yes (2) No
Appendix C
References
- Schumacher, A.E.; Kyu, H.H.; Aali, A.; Abbafati, C.; Abbas, J.; Abbasgholizadeh, R.; Abbasi, M.A.; Abbasian, M.; ElHafeez, S.A.; Abdelmasseh, M.; et al. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950–2021, and the impact of the COVID-19 pandemic: A comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 1989–2056. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Knight, M.; A’cOurt, C.; Buxton, M.; Husain, L. Management of post-acute COVID-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]
- Marra, A.R.; Kobayashi, T.; Callado, G.Y.; Pardo, I.; Gutfreund, M.C.; Hsieh, M.K.; Lin, V.; Alsuhaibani, M.; Hasegawa, S.; Tholany, J.; et al. The effectiveness of COVID-19 vaccine in the prevention of post-COVID conditions: A systematic literature review and meta-analysis of the latest research. Antimicrob. Steward. Healthc. Epidemiol. 2023, 3, e168. [Google Scholar] [CrossRef] [PubMed]
- de Gier, B.; Huiberts, A.J.; Hoeve, C.E.; Hartog, G.D.; van Werkhoven, H.; van Binnendijk, R.; Hahné, S.J.M.; de Melker, H.E.; Hof, S.v.D.; Knol, M.J. Effects of COVID-19 vaccination and previous infection on Omicron SARS-CoV-2 infection and relation with serology. Nat. Commun. 2023, 14, 4793. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [CrossRef]
- Qin, S.; Zhang, Y.; Li, Y.; Huang, L.; Yang, T.; Si, J.; Wang, L.; Zhao, X.; Ma, X.; Gao, G.F. Long COVID facts and findings: A large-scale online survey in 74,075 Chinese participants. Lancet Reg. Health-West. Pac. 2024, 52, 101218. [Google Scholar] [CrossRef]
- Tsampasian, V.; Elghazaly, H.; Chattopadhyay, R.; Debski, M.; Naing, T.K.P.; Garg, P.; Clark, A.; Ntatsaki, E.; Vassiliou, V.S. Risk Factors Associated With Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2023, 183, 566–580. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Gavrilov, D.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; et al. Coronavirus (COVID-19) Vaccinations. 2020. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 6 March 2025).
- Jia, S.; Yin, Z.; Pan, H.; Wang, F.; Liu, X.; Wang, Q.; Zhang, L.; Tang, J.; Yang, H.; Du, J.; et al. Relative effectiveness of a heterologous booster dose with adenovirus type 5 vectored COVID-19 vaccine versus three doses of inactivated COVID-19 vaccine in adults during a nationwide outbreak of omicron predominance, in China: A retrospective, individually matched cohort-control study. Emerg. Microbes Infect. 2024, 13, 2332660. [Google Scholar] [CrossRef]
- Ballering, A.V.; van Zon, S.K.R.; Hartman, T.C.O.; Rosmalen, J.G.M. Persistence of somatic symptoms after COVID-19 in the Netherlands: An observational cohort study. Lancet 2022, 400, 452–461. [Google Scholar] [CrossRef]
- COVID-19 Clinical and Surveillance Data-9 December 2022 to 23 January 2023, China. Chinese Center for Disease Control and Prevention. Available online: https://en.chinacdc.cn/news/latest/202301/W020230126558725888448.pdf (accessed on 13 March 2025).
- Richard, S.A.; Pollett, S.D.; Fries, A.C.; Berjohn, C.M.; Maves, R.C.; Lalani, T.; Smith, A.G.; Mody, R.M.; Ganesan, A.; Colombo, R.E.; et al. Persistent COVID-19 Symptoms at 6 Months After Onset and the Role of Vaccination Before or After SARS-CoV-2 Infection. JAMA Netw. Open 2023, 6, e2251360. [Google Scholar] [CrossRef]
- Arnold, D.T.; Milne, A.; Samms, E.; Stadon, L.; Maskell, N.A.; Hamilton, F.W. Symptoms After COVID-19 Vaccination in Patients with Persistent Symptoms After Acute Infection: A Case Series. Ann. Intern. Med. 2021, 174, 1334–1336. [Google Scholar] [CrossRef] [PubMed]
- Solomon, M.D.; Escobar, G.J.; Lu, Y.; Schlessinger, D.; Steinman, J.B.; Steinman, L.; Lee, C.; Liu, V.X. Risk of severe COVID-19 infection among adults with prior exposure to children. Proc. Natl. Acad. Sci. USA 2022, 119, e2204141119. [Google Scholar] [CrossRef]
- Azambuja, P.; Bastos, L.S.; Batista-Da-Silva, A.A.; Ramos, G.V.; Kurtz, P.; Dias, C.M.; da Silva, E.P.; Arouca, L.E.; Soares, J.; Sejvar, J.J.; et al. Prevalence, risk factors, and impact of long COVID in a socially vulnerable community in Brazil: A prospective cohort study. Lancet Reg. Health Am. 2024, 37, 100839. [Google Scholar] [CrossRef]
- Ren, J.; Pang, W.; Luo, Y.; Cheng, D.; Qiu, K.; Rao, Y.; Zheng, Y.; Dong, Y.; Peng, J.; Hu, Y.; et al. Impact of Allergic Rhinitis and Asthma on COVID-19 Infection, Hospitalization, and Mortality. J. Allergy Clin. Immunol. Pract. 2022, 10, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Ou, S.; Huang, Z.; Lan, M.; Ye, J.; Chen, J.; Guo, H.; Xiao, J.; Zhuang, S.; Wu, J.; Yang, C.; et al. The duration and breadth of antibody responses to 3-dose of inactivated COVID-19 vaccinations in healthy blood donors: An observational study. Front. Immunol. 2022, 13, 1027924. [Google Scholar] [CrossRef] [PubMed]
- Storozhuk, M.; Lee, S.; Lee, J.I.; Park, J. Green Tea Consumption and the COVID-19 Omicron Pandemic Era: Pharmacology and Epidemiology. Life 2023, 13, 852. [Google Scholar] [CrossRef]
- Islam, Z.; Yamamoto, S.; Mizoue, T.; Konishi, M.; Ohmagari, N. Coffee and Green Tea Consumption With the Risk of COVID-19 Among the Vaccine Recipients in Japan: A Prospective Study. J. Epidemiol. 2024, 34, 444–452. [Google Scholar] [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- van Zyl-Smit, R.N.; Richards, G.; Leone, F.T. Tobacco smoking and COVID-19 infection. Lancet Respir. Med. 2020, 8, 664–665. [Google Scholar] [CrossRef]
- Velazquez-Salinas, L.; Verdugo-Rodriguez, A.; Rodriguez, L.L.; Borca, M.V. The Role of Interleukin 6 During Viral Infections. Front. Microbiol. 2019, 10, 1057. [Google Scholar] [CrossRef]
- Zampelas, A.; Panagiotakos, D.B.; Pitsavos, C.; Chrysohoou, C.; Stefanadis, C. Associations between coffee consumption and inflammatory markers in healthy persons: The ATTICA study. Am. J. Clin. Nutr. 2004, 80, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Sezer, Z.; Pavel, S.T.I.; Inal, A.; Yetiskin, H.; Kaplan, B.; Uygut, M.A.; Aslan, A.F.; Bayram, A.; Mazicioglu, M.; Unuvar, G.K.; et al. Long-Term Immunogenicity and Safety of a Homologous Third Dose Booster Vaccination with TURKOVAC: Phase 2 Clinical Study Findings with 32-Week Post-Booster Follow-Up. Vaccines 2024, 12, 140. [Google Scholar] [CrossRef]
- Tarke, A.; Coelho, C.H.; Zhang, Z.; Dan, J.M.; Yu, E.D.; Methot, N.; Bloom, N.I.; Goodwin, B.; Phillips, E.; Mallal, S.; et al. SARS-CoV-2 vaccination induces immunological T cell memory able to cross-recognize variants from Alpha to Omicron. Cell 2022, 185, 847–859.e11. [Google Scholar] [CrossRef]
- Zhang, Z.; Mateus, J.; Coelho, C.H.; Dan, J.M.; Moderbacher, C.R.; Gálvez, R.I.; Cortes, F.H.; Grifoni, A.; Tarke, A.; Chang, J.; et al. Humoral and cellular immune memory to four COVID-19 vaccines. Cell 2022, 185, 2434–2451.e17. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Baraff, A.; Fox, A.; Shahoumian, T.; Hickok, A.; O’hAre, A.M.; Bohnert, A.S.B.; Boyko, E.J.; Maciejewski, M.L.; Bowling, C.B.; et al. Rates and factors associated with documentation of diagnostic codes for long COVID in the National Veterans Affairs Health Care System. JAMA Netw. Open 2022, 5, e2224359. [Google Scholar] [CrossRef] [PubMed]
- Kostev, K.; Smith, L.; Koyanagi, A.; Jacob, L. Prevalence of and factors associated with post-coronavirus disease 2019 (COVID-19) condition in the 12 months after the diagnosis of COVID-19 in adults followed in general practices in Germany. Open Forum Infect. Dis. 2022, 9, ofac333. [Google Scholar] [CrossRef]
- Pazukhina, E.; Andreeva, M.; Spiridonova, E.; Bobkova, P.; Shikhaleva, A.; El-Taravi, Y.; Rumyantsev, M.; Gamirova, A.; Bairashevskaia, A.; Petrova, P.; et al. Prevalence and risk factors of post-COVID-19 condition in adults and children at 6 and 12 months after hospital discharge: A prospective, cohort study in Moscow (StopCOVID). BMC Med. 2022, 20, 244. [Google Scholar] [CrossRef] [PubMed]
- Baruch, J.; Zahra, C.; Cardona, T.; Melillo, T. National long COVID impact and risk factors. Public Health 2022, 213, 177–180. [Google Scholar] [CrossRef]
- Dias, M.B.; Medeiros, A.P.V.; de Melo, S.S.; Fonseca, C.S.; Jacob-Filho, W.; Avelino-Silva, T.J.; Aliberti, M.J.R.; for the CO-FRAIL Study Group. The long and winding road of COVID-19 in survivors of hospitalisation: Symptoms trajectory and predictors of long COVID. J. Intern. Med. 2023, 293, 264–268. [Google Scholar] [CrossRef]
- Chudzik, M.; Babicki, M.; Kapusta, J.; Kałuzińska-Kołat, Ż.; Kołat, D.; Jankowski, P.; Mastalerz-Migas, A. Long-COVID clinical features and risk factors: A retrospective analysis of Patients from the STOP-COVID registry of the PoLoCOV Study. Viruses 2022, 14, 1755. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Guijarro, C.; Torres-Macho, J.; Velasco-Arribas, M.; Plaza-Canteli, S.; Hernández-Barrera, V.; Arias-Navalón, J.A. Diabetes and the risk of long-term post-COVID symptoms. Diabetes 2021, 70, 2917–2921. [Google Scholar] [CrossRef] [PubMed]
| Control Group (n = 10,462, %) | Case Group (n = 10,462, %) | p | |
|---|---|---|---|
| Age group (year) | |||
| 18–29 | 608 (5.83) | 608 (5.83) | 0.990 |
| 30–39 | 1285 (12.32) | 1285 (12.32) | |
| 40–49 | 1505 (14.44) | 1548 (14.85) | |
| 50–59 | 2480 (23.79) | 2469 (23.68) | |
| 60–69 | 2601 (24.95) | 2563 (24.58) | |
| ≥70 | 1947 (18.68) | 1953 (18.73) | |
| Mean age, years | 55.28 ± 14.92 | 55.20 ± 14.90 | 0.690 |
| Sex | |||
| Male | 6686 (64.13) | 6686 (64.13) | 1.000 |
| Mean BMI, kg/m2 | 23.72 ± 3.52 | 23.88 ± 3.39 | <0.001 |
| BMI, kg/m2 | |||
| ≥18.5 and <24 | 5282 (52.03) | 5024 (49.16) | <0.001 |
| <18.5 | 444 (4.37) | 383 (3.75) | |
| ≥24 and <28 | 3468 (34.16) | 3742 (36.61) | |
| ≥28 | 958 (9.44) | 1071 (10.48) | |
| Interval from last dose vaccination to 1 November 2022 (days) | 252.00 (247.00, 256.00) | 252.00 (247.00, 257.00) | 0.760 |
| Interval from last dose vaccination to 1 November 2022 (months) | |||
| 5–8 months | 8831 (84.70) | 8509 (81.61) | <0.001 |
| ≥9 months | 1595 (15.30) | 1917 (18.39) | |
| Smoking | |||
| No | 6424 (61.62) | 7148 (68.56) | <0.001 |
| Yes | 4002 (38.38) | 3278 (31.44) | |
| Alcohol consumption | |||
| Never/hardly ever | 6522 (62.56) | 6686 (64.13) | <0.001 |
| Weekly | 2198 (21.08) | 2365 (22.68) | |
| Occasionally | 1706 (16.36) | 1375 (13.19) | |
| Tea consumption | |||
| Never/hardly ever | 6327 (60.68) | 5888 (56.47) | <0.001 |
| Weekly | 2072 (19.87) | 2374 (22.77) | |
| Occasionally | 2027 (19.44) | 2164 (20.76) | |
| Coffee consumption | |||
| Never/hardly ever | 9874 (94.71) | 9726 (93.29) | <0.001 |
| Weekly | 480 (4.60) | 594 (5.70) | |
| Occasionally | 72 (0.69) | 106 (1.02) | |
| Allergic history | 377 (3.62) | 554 (5.31) | <0.001 |
| Immunological therapy history | 24 (0.23) | 44 (0.42) | 0.020 |
| Types of comorbidities | |||
| No | 7813 (74.94) | 7145 (68.53) | <0.001 |
| Only hypertension | 1300 (12.47) | 1507 (14.45) | |
| Only diabetes | 48 (0.46) | 77 (0.74) | |
| Only stroke | 239 (2.29) | 259 (2.48) | |
| Only hyperlipemia | 78 (0.75) | 95 (0.91) | |
| Only coronary heart disease | 63 (0.60) | 68 (0.65) | |
| Number of comorbidities | |||
| No | 7813 (74.94) | 7145 (68.53) | <0.001 |
| One comorbidity | 1985 (19.04) | 2333 (22.38) | |
| Two comorbidities | 484 (4.64) | 697 (6.69) | |
| Three or more comorbidities | 144 (1.38) | 251 (2.41) |
| Symptoms | Total (n = 10,462) | Symptoms Lasting ≥ 21 Days (n = 963, 9%) | Symptoms Severity ≥ Grade 2 (n = 773, 7%) |
|---|---|---|---|
| Respiratory symptoms | 7470 (71.40) | 600 (62.31) | 416 (53.82) |
| cough | 6100 (58.30) | 566 (58.77) | 259 (33.51) |
| pharyngalgia | 3311 (31.65) | 41 (4.25) | 142 (18.37) |
| rhinitis | 1953 (18.67) | 36 (3.73) | 56 (7.25) |
| dyspnea | 332 (3.17) | 49 (5.09) | 42 (5.43) |
| Constitutional symptoms | 9284 (88.74) | 282 (29.28) | 198 (25.61) |
| fatigue | 6662 (63.68) | 279 (28.97) | 197 (25.49) |
| chill | 1384 (13.23) | 14 (1.45) | 2 (0.26) |
| fever | 7114 (68.00) | 1 (0.10) | - |
| Neurological and sensory symptoms | 4218 (40.32) | 176 (18.28) | 155 (20.05) |
| headache | 3092 (29.55) | 36 (3.74) | 94 (12.16) |
| hypogeusia | 1618 (15.47) | 92 (9.55) | 51 (6.60) |
| hyposmia | 802 (7.67) | 59 (6.12) | 25 (3.23) |
| eye discomfort | 151 (1.44) | 10 (1.04) | 5 (0.65) |
| attention disorders | 143 (1.37) | 23 (2.39) | 4 (0.52) |
| alopecia | 50 (0.48) | 16 (1.66) | 0 (0.00) |
| Musculoskeletal symptoms | 4674 (44.68) | 82 (8.52) | 218 (28.21) |
| myalgia | 4374 (41.81) | 68 (7.06) | 186 (24.06) |
| ostalgia | 886 (8.47) | 26 (2.70) | 74 (9.57) |
| Gastrointestinal symptoms | 2148 (20.53) | 64 (6.65) | 52 (6.73) |
| anorexia | 1853 (17.71) | 60 (6.23) | 35 (4.53) |
| diarrhea | 255 (2.43) | 4 (0.42) | 10 (1.29) |
| emesis | 219 (2.09) | 1 (0.10) | 9 (1.16) |
| nausea | 270 (2.58) | 6 (0.62) | 2 (0.26) |
| Characteristic | OR (95% CI) | p | FDR |
|---|---|---|---|
| BMI, kg/m2 | |||
| 18.5 ≤ BMI < 24 | 1.00 (Reference) | ||
| BMI < 18.5 | 0.92 (0.80~1.06) | 0.269 | 0.283 |
| 24 ≤ BMI < 28 | 1.08 (1.02~1.15) | 0.008 | 0.013 |
| BMI ≥ 28 | 1.07 (0.97~1.18) | 0.150 | 0.164 |
| Smoking | |||
| No | 1.00 (Reference) | ||
| Yes | 0.69 (0.64~0.74) | <0.001 | <0.001 |
| Alcohol consumption | |||
| Never/hardly ever | 1.00 (Reference) | ||
| Occasionally | 1.15 (1.07~1.24) | <0.001 | <0.001 |
| ≥1/week | 0.90 (0.82~0.98) | 0.021 | 0.032 |
| Tea consumption | |||
| Never/hardly ever | 1.00 (Reference) | ||
| Occasionally | 1.33 (1.24~1.43) | <0.001 | <0.001 |
| ≥1/week | 1.29 (1.20~1.39) | <0.001 | <0.001 |
| Coffee consumption | |||
| Never/hardly ever | 1.00 (Reference) | ||
| Occasionally | 1.19 (1.05~1.35) | 0.006 | 0.011 |
| ≥1/week | 1.41 (1.04~1.93) | 0.024 | 0.035 |
| Types of comorbidities | |||
| None | 1.00 (Reference) | ||
| Hypertension | 1.27 (1.17~1.38) | <0.001 | <0.001 |
| Hyperlipemia | 1.70 (1.18~2.46) | 0.004 | 0.009 |
| Diabetes | 1.17 (0.98~1.40) | 0.080 | 0.100 |
| Coronary heart disease | 1.32 (0.97~1.79) | 0.070 | 0.093 |
| Stroke | 1.19 (0.84~1.69) | 0.310 | 0.310 |
| Number of comorbidities | |||
| None | 1.00 (Reference) | ||
| One comorbidity | 1.29 (1.20~1.38) | <0.001 | <0.001 |
| Two comorbidities | 1.57 (1.39~1.77) | <0.001 | <0.001 |
| Three or more comorbidities | 1.85 (1.50~2.28) | <0.001 | <0.001 |
| Allergic history | |||
| No | 1.00 (Reference) | ||
| Yes | 1.37 (1.20~1.57) | <0.001 | <0.001 |
| Immunosuppressive | |||
| No | 1.00 (Reference) | ||
| Yes | 1.48 (0.89~2.49) | 0.130 | 0.153 |
| Interval from last dose vaccination to 1 November 2022 (months) | |||
| 5–8 months | 1.00 (Reference) | ||
| ≥9 months | 1.28 (1.19~1.38) | <0.001 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.; Qi, R.; Jia, S.; Peng, Z.; Pan, H.; Xu, M.; Liu, Y.; Liu, X.; Wang, Q.; Zhang, L.; et al. The Factors Influencing the Incidence, Persistence, and Severity of Symptoms After SARS-CoV-2 Infection in Chinese Adults: A Case–Control Study. Trop. Med. Infect. Dis. 2025, 10, 185. https://doi.org/10.3390/tropicalmed10070185
Wang W, Qi R, Jia S, Peng Z, Pan H, Xu M, Liu Y, Liu X, Wang Q, Zhang L, et al. The Factors Influencing the Incidence, Persistence, and Severity of Symptoms After SARS-CoV-2 Infection in Chinese Adults: A Case–Control Study. Tropical Medicine and Infectious Disease. 2025; 10(7):185. https://doi.org/10.3390/tropicalmed10070185
Chicago/Turabian StyleWang, Weixiao, Runjie Qi, Siyue Jia, Zhihang Peng, Hongxing Pan, Ming Xu, Yuanbao Liu, Xiaoqiang Liu, Qing Wang, Li Zhang, and et al. 2025. "The Factors Influencing the Incidence, Persistence, and Severity of Symptoms After SARS-CoV-2 Infection in Chinese Adults: A Case–Control Study" Tropical Medicine and Infectious Disease 10, no. 7: 185. https://doi.org/10.3390/tropicalmed10070185
APA StyleWang, W., Qi, R., Jia, S., Peng, Z., Pan, H., Xu, M., Liu, Y., Liu, X., Wang, Q., Zhang, L., Tang, J., Yang, H., Jin, P., Li, S., & Li, J. (2025). The Factors Influencing the Incidence, Persistence, and Severity of Symptoms After SARS-CoV-2 Infection in Chinese Adults: A Case–Control Study. Tropical Medicine and Infectious Disease, 10(7), 185. https://doi.org/10.3390/tropicalmed10070185